


Many therapeutic clinical trials have proposed using a measure of metabolic change to assess therapeutic response rather than relying on conventional anatomic measurements of changes in tumor size on CT or MRI. PET assessment of changes in 18F-FDG uptake by tumors is gaining acceptance as such a measure.
Despite the increasing use of 18F-FDG PET as a biomarker for predicting therapeutic response, there are no widely accepted standardized protocols for using 18F-FDG PET as a tool for assessing response to therapy, nor are there validated criteria for judging response using 18F-FDG PET. The European PET community, working with the European Organization for Research and Treatment of Cancer, initiated a project to begin defining response criteria for PET and published their preliminary consensus recommendations in 1999 (1). The European Organization for Research and Treatment of Cancer continues to accumulate data in order to more carefully assess the role of 18F-FDG PET in measuring therapeutic response.
18F-FDG PET has become a common imaging modality in oncology, primarily as a result of the widespread availability of PET instruments, an accumulation of clinical data, and the gradual expansion of oncology indications that Medicare will reimburse. With this increasing clinical experience, it is becoming clear that 18F-FDG PET may have an important role as a surrogate endpoint for assessing the clinical efficacy of novel oncologic therapies. At the same time, it has become equally clear that the potential of 18F-FDG PET as such a tool will not be achieved unless standard protocols are developed so that data can be accumulated and compared across multiple clinical sites. Today, the methods of obtaining 18F-FDG PET scans and assessing 18F-FDG metabolism and uptake vary.
To provide such guidance and to help standardize the acquisition and interpretation of 18F-FDG PET images in clinical trials sponsored by the National Cancer Institute (NCI), the Cancer Imaging Program of the NCI convened a workshop on January 10−11, 2005, in Washington, DC, at which the current status of 18F-FDG PET technology and clinical experience—both in diagnosis and in monitoring therapeutic response—was reviewed. The participants focused on patient preparation, image acquisition, image reconstruction, quantitative and semiquantitative image analysis, quality assurance, reproducibility, and other parameters important in 18F-FDG PET studies before and after a therapeutic intervention. Their discussions were based on the existing medical literature and on their own expertise.
This document represents the outcome of those deliberations. We intend that it serve as the recommended set of procedures for the acquisition and analysis of 18F-FDG PET scans of patients participating in NCI-sponsored diagnostic and therapeutic clinical trials. We hope that these guidelines will help bring about a future in which 18F-FDG PET can provide an early metabolic assessment of therapeutic response.
IMAGE ANALYSIS AND UPTAKE QUANTIFICATION
18F-FDG is a marker of metabolic activity in a variety of tissues and tumors (2). Most malignant tissues have increased 18F-FDG uptake associated with an increased rate of glycolysis and of glucose transport. Warburg first described this fundamental aberration of malignant cells in the 1930s (3), and more recently, several groups have described the specific cellular mechanisms associated with glucose uptake in malignant tissue (4–6). The increase in 18F-FDG uptake noted in malignant tissue is related in a complex manner to the proliferative activity of malignant tissue and to the number of viable tumor cells (7–9). For these reasons, investigators have postulated that alterations and changes in 18F-FDG uptake after treatment of cancer should reflect the cellular response to the treatment, likely including effects such as changes in the number of viable tumor cells and altered cellular proliferation. However, a complex mix of different cellular processes determines the rate of glucose metabolism. The precise mechanism by which alterations in these cellular processes with cancer treatment lead to changes in 18F-FDG uptake is incompletely understood and may be different for different tumor types and different treatments.
Numerous approaches have been used to assess 18F-FDG uptake in malignant tissue. There are 3 broad categories: visual interpretation and estimation of relative uptake, assessment of uptake over a defined time using semiquantitative methods, and assessment of uptake from the time of injection to a defined endpoint using kinetic analysis. Table 1 provides an overview of the various methods of assessing tumor 18F-FDG uptake and their advantages and disadvantages. Each method has been shown to have clinical utility but has been applied rigorously in only a few trials assessing response to therapy.
Methods of Assessing 18F-FDG Uptake (1)
Visual assessment, the easiest method, is subjective and not suitable for clinical trials in which a more objective quantitative measure is desirable, barring the uncommon occurrence of a complete response to therapy. Visual assessment is based on a comparison of 18F-FDG uptake in tumor with 18F-FDG uptake in surrounding tissue, either of which may show the effects of a therapeutic intervention on subsequent scans.
A major issue in monitoring tumor response by determining 18F-FDG uptake is that the uptake depends on the time of measurement. An important aspect of oncologic 18F-FDG PET is whole-body imaging, because it assesses the entire body for malignant disease. However, whole-body imaging complicates semiquantitative and quantitative techniques because various parts of the body are imaged at different times after the injection of 18F-FDG. In reality, whole-body images are a composite of static images obtained sequentially beginning at some defined time after the injection of 18F-FDG. The static images are typically obtained over a defined period and often are corrected for attenuation using a separate transmission scan. When used to assess the response of tumors to therapy, whole-body 18F-FDG PET must be attenuation corrected to allow for accurate kinetic analysis or semiquantitative measurement.
The standardized uptake value (SUV) is the semiquantitative method most commonly used to determine 18F-FDG uptake in attenuation-corrected PET images. With this technique, the tumor 18F-FDG concentration is normalized to the amount of injected activity and total volume of distribution. Numerous indices have been used to represent the volume of distribution, such as body weight, lean body mass, and body surface area (10). Another variable incorporated into the SUV equation is normalization for the serum glucose concentration. When corrected only for body weight, SUV does not take into account the relatively lower 18F-FDG accumulation in fatty tissues (11). Normalization to body surface area or lean body mass potentially reduces the effect of weight loss (which may occur during therapy) on subsequent SUV determinations. Lean body mass may be the better method because of the availability of sex-specific corrections (12).
Full kinetic modeling has been used infrequently for the evaluation of malignancy in clinical practice because of the complexity of such an approach, including patient compliance issues and the requirement for arterial blood sampling or dynamic imaging of a blood-pool structure to obtain a precise input function (13). The advantages of a full kinetic quantitative analysis, however, are that it yields an absolute rate for 18F-FDG metabolism, is independent of imaging time, and provides insight into various components of glucose metabolism such as transport and phosphorylation. Early in the development of PET, absolute quantitative techniques were commonly used for the brain because a dynamic image set of the nonmoving brain could be obtained easily. Even in this context, however, the technique was not widespread as a clinical tool because of its complexity, the time involved, and the need for arterial blood sampling (14). A tremendous amount of research has gone into defining the specific rate constants, lumped constant, and other parameters of 18F-FDG quantitation in brain tissue (15). A critical component in determining the absolute metabolic rate for glucose from 18F-FDG studies is the lumped constant, because it reflects the difference between the affinities of 18F-FDG and glucose for transport and subsequent phosphorylation (16). Some studies have suggested that the lumped constant varies considerably in tumors, leading many investigators to describe the 18F-FDG metabolic rate instead of the glucose metabolic rate in 18F-FDG PET studies of tumors.
Other techniques were eventually developed to determine parameters of interest in studies of neurologic disorders, including graphical or Patlak analysis for irreversibly trapped tracers (17,18). Because 18F-FDG is an irreversibly trapped metabolic tracer, the influx rate constant can be determined from a graphical approach without the nonlinear optimization inherent in the full kinetic approach. As in kinetic analysis, however, graphical analysis requires dynamic scanning and determination of the blood time–activity curve, possibly by arterial blood sampling. This technique has been extrapolated from brain imaging and used in tumor imaging when a tumor is evaluated over a defined period. Whole-body imaging is difficult with this technique because dynamic tissue time–activity data are required for each specific location or tumor (19). The potential value in absolute quantitative PET studies is the ability to determine metabolic rate and the greater robustness of the approach to variations that may affect semiquantitative studies, such as the time from injection to scanning.
In the full kinetic approach, the study reflects transport and phosphorylation of 18F-FDG in both normal and malignant tissues. It is obvious that these approaches, both absolute quantitation with dynamic imaging and Patlak analysis, will be burdensome and difficult to implement routinely in patients with cancer or, indeed, in large phase II and phase III clinical trials. One advantage of 18F-FDG PET is the ability to easily image whole-body distribution of the tracer and look for new metastatic lesions. This advantage would be compromised with the full kinetic and Patlak approaches, which require monitoring of arterial 18F-FDG plasma concentration and, consequently, can be difficult for patients and PET center personnel. To avoid placing an arterial catheter to obtain the arterial input function, investigators have used various surrogate approaches, including dynamic scanning over the heart or a major artery. In addition, techniques have been developed for arterializing venous blood. However, these are fraught with technical difficulties, particularly in patients with poor venous access, as is typical in patients with cancer. Several “simplified kinetic” methods have been proposed and represent a compromise between full kinetic analysis and simple static imaging (20–22). These methods might prove useful in monitoring changes in 18F-FDG metabolism with therapy but, to date, have not been widely tested.
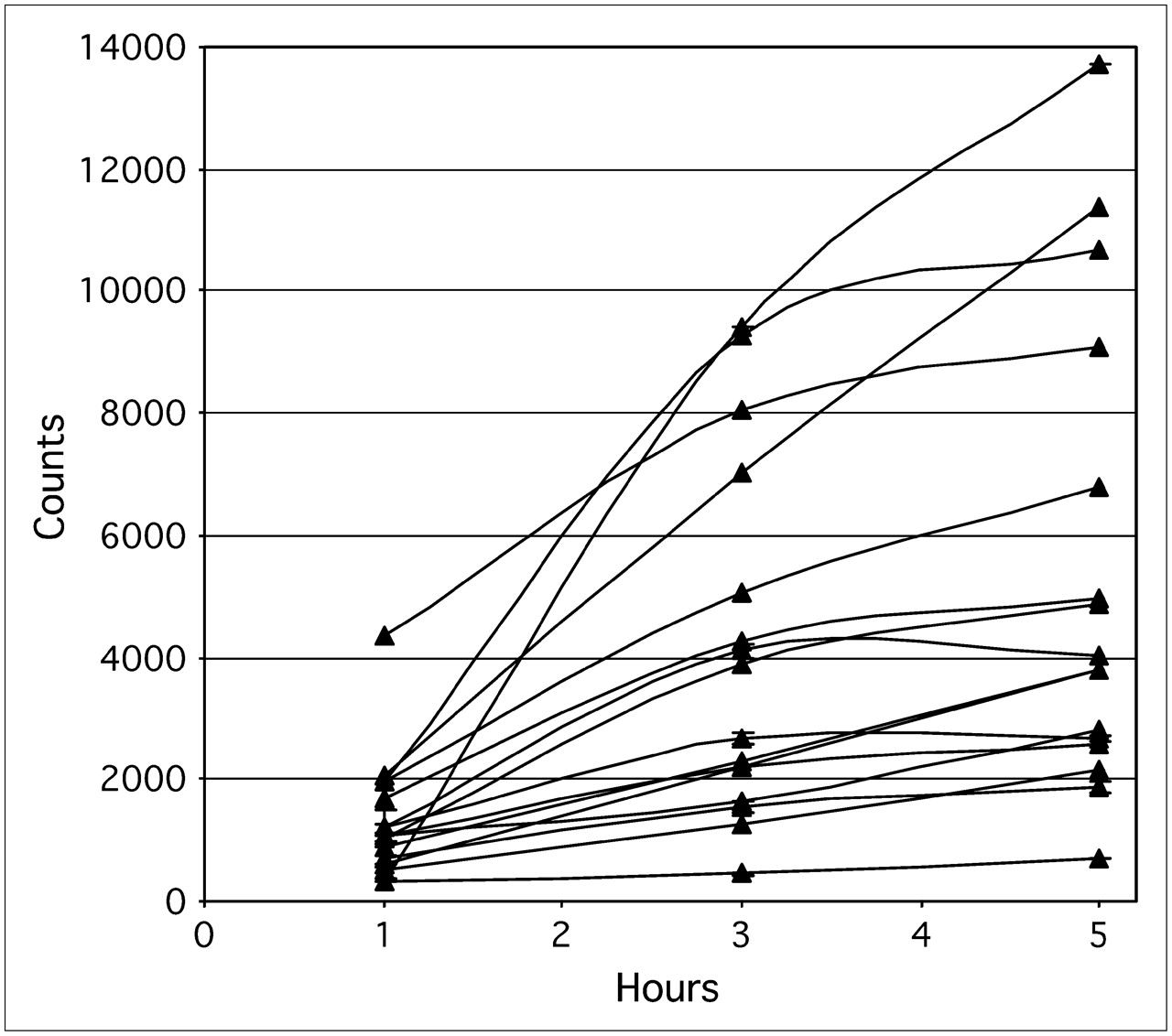
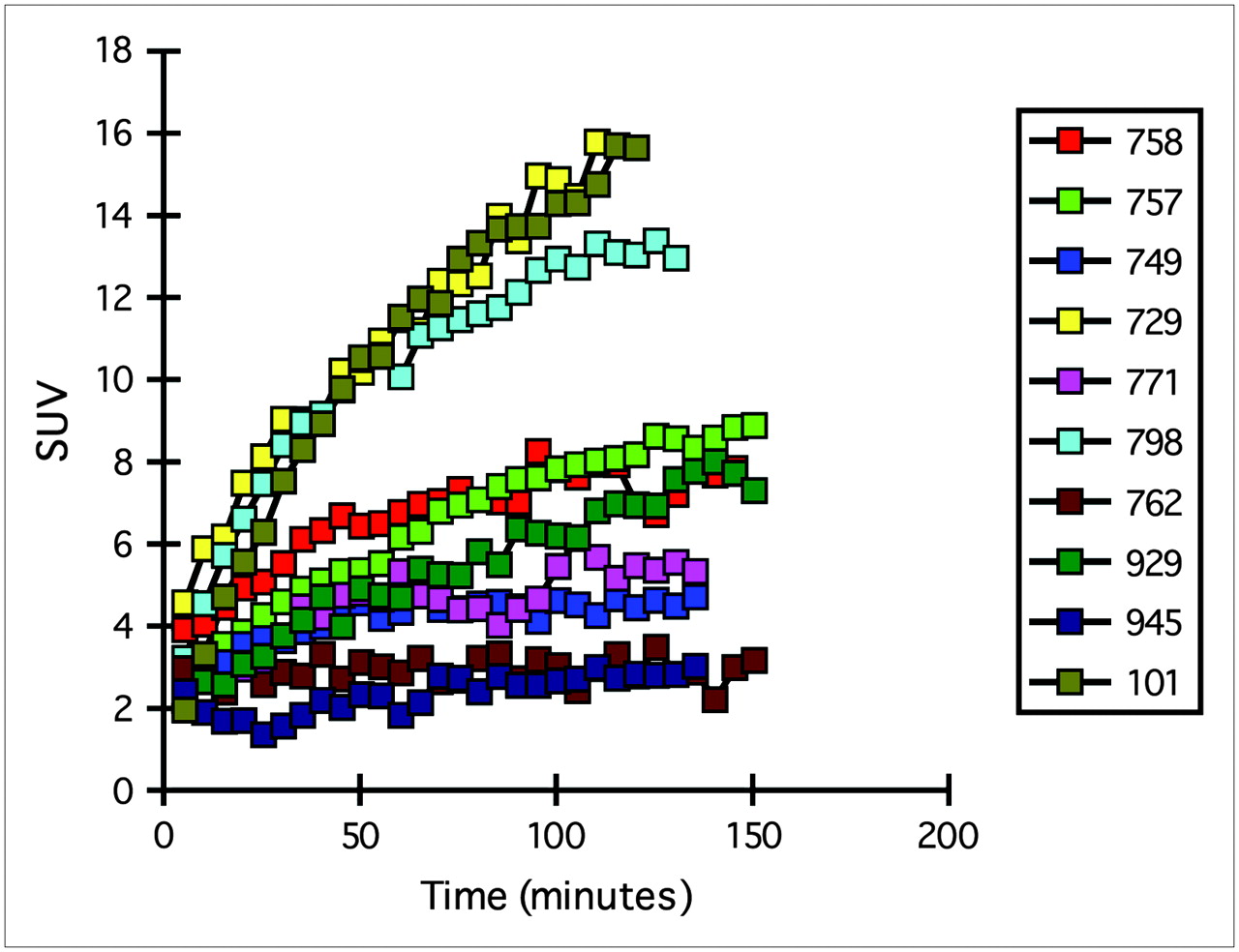
A major difficulty with whole-body 18F-FDG PET is that the patient may have numerous lesions, including both the primary tumor and metastatic lesions, spread throughout the body. 18F-FDG uptake into both primary and metastatic tumors, as well as into other body tissues, is a dynamic process that peaks and plateaus at various time points dependent on the tumor tissue kinetics for 18F-FDG uptake, the method by which the patient is prepared for the study, and other unknown variables. Therefore, it is extremely important that in serial examinations the target lesion or lesions be imaged at exactly the same time after injection of the tracer. An 18F-FDG uptake period of at least 60 min is generally considered most appropriate for patients with malignancy, and this period was used in most of the published clinical studies. However, uptake in the tumors of some patients evaluated with dynamic imaging may not peak or plateau until 90 or 120 min, or longer, after tracer injection. Therefore, in a given patient, image acquisitions should commence at exactly the same time after injection of 18F-FDG and the sequences should be of exactly the same time and length to ensure that each component static image of the whole-body image is obtained similarly. Figures 1 and 2 show the tissue time–activity relationships of various lesions and the resultant variability in SUV determination as a function of time. If uptake is still increasing, significant variability in SUV determination is possible unless the patient is imaged at the same time on all sequential studies used to assess response (23,24). Studies have shown that in metabolically active tumors, SUV can change significantly over the course of 10–15 min (25,26).

Tissue time–activity curves for 10 patients with solitary pulmonary nodules imaged over time with dynamic emission PET (23). Lesions were identified, ROI analysis performed, and SUV determined. 18F-FDG uptake plateaued at various times after injection. Reprinted with permission from the Society of Nuclear Medicine.
Tissue time–activity curves for 16 patients. Static PET was performed at 1, 3, and 5 h after injection of 18F-FDG, and activity in lesions was determined. 18F-FDG uptake plateaued at various times after injection and, in several lesions, was still increasing even at 5 h after injection. (Courtesy of Karen Kurdziel.)
Comparisons of various kinetic modeling and semiquantitative techniques show a good correlation between absolute quantitative metabolic rate and SUV normalized to body weight, lean body mass, or body surface area. Many members of the working group expressed a preference for normalizing to lean body mass, but existing data did not warrant a unanimous preference for normalizing to lean body mass over other parameters. Given the complexities of conducting kinetic analysis, the working group concluded that a reasonable approach for large phase II or III clinical trials would be semiquantitative analysis (i.e., measurement of SUV normalized to either lean body mass or body surface area). If there is a perceived need to obtain the absolute quantitative metabolic rate or more detailed information on 18F-FDG kinetics in a protocol evaluating therapeutic response (e.g., for new therapies that may affect tracer delivery to the tumor and limit uptake), this need could be more easily addressed in the setting of a single-institution phase I or early phase II study.
FACTORS AFFECTING UPTAKE DETERMINATION
Partial-Volume Effects
Partial-volume effects secondary to scanner resolution are an important technical factor. Most PET scanners have a reconstructed image resolution of approximately 5–10 mm. However, this may be altered depending on the filtering applied before, during, or after reconstruction and on the reconstruction and display matrix sizes (27). It has been amply demonstrated that measuring objects of less than 2 times the resolution of the scanner results in varying and possibly significant partial-volume effects. Unfortunately, partial-volume correction is often complicated and laborious. Nevertheless, partial-volume correction has been shown to improve the diagnostic accuracy of SUV measurements (28,29). This point is critical, because many therapeutic interventions reduce the size of the tumor. In the absence of partial-volume correction, 18F-FDG uptake in small tumors will be underestimated.
Scanner Quality Control
PET scanners should routinely be assessed for quantitative integrity and stability by being tested using various imaging protocols on a standard phantom. For SUV measurements, this assessment should include a comparison against a dose calibrator to ensure accuracy; that is, a comparison of the absolute activity measured, versus the measured injected, should be performed. This comparison is particularly important after software or hardware upgrades.
Region-of-Interest (ROI) Determination
Tumors are extremely heterogeneous and contain necrotic tissue, cystic components, and fibrous elements, as well as malignant tumor cells. This heterogeneity becomes a critical issue after therapy begins and the malignant or other components of the “tumor” mass change. Drawing of the ROI by hand or by edge-finding techniques is typical for defining the tumor boundaries. Both methods appear to work well as long as they are performed in the same, systematic manner on serial examinations. Threshold-determination or edge-finding algorithms are accurate and can be applied with less subjective interaction from the technician or physician determining the ROI. It should be obvious, however, that the same approach must be applied systematically and uniformly across all patients and across all sequential tumor measurements. Another factor that may confound ROI determination is the partial-volume effect already mentioned. Both the mean value within the ROI and the maximum value (reflecting the most metabolically active region) within the ROI may have clinical importance and should be reported.
Blood Glucose Level
The concentration of circulating glucose can significantly affect 18F-FDG uptake by tumors, and various groups have reported schemes for correcting the 18F-FDG SUV for the circulating plasma glucose concentration. The working group agreed that in patients with a plasma glucose concentration within the reference range, SUV determinations are not appreciably related to serum plasma glucose concentration (9,30). The working group also agreed that in patients with a high serum glucose concentration, the problems with administration of insulin would diminish the accuracy of SUV determination by altering the biodistribution of 18F-FDG, especially in insulin-sensitive tissue such as muscle, myocardium, fat, and gut. In such patients, the 18F-FDG PET study should be rescheduled, and adjustments to diet and medications be made if necessary, so that the fasting blood glucose concentration can be brought down to an acceptable range at the time of 18F-FDG injection, that is, 150−200 mg/dL or less. The working group also agreed that diabetic patients should not be excluded from clinical trials but that such patients should be scanned early in the morning before the first meal and that the doses of insulin and hypoglycemic medication should be titrated appropriately the night before and morning of the study. Before scheduling an 18F-FDG PET study, diabetic patients should test their ability to maintain reasonable plasma glucose levels after fasting, while avoiding insulin close to the time that 18F-FDG would be administered.
RECOMMENDATIONS OF WORKSHOP PANEL
These recommendations are summarized in Table 2.
Recommendations of Workshop Panel
Patient Preparation
Patient preparation is critical to the quality of 18F-FDG PET, both as a diagnostic test and as an assessment of therapeutic response. The following are recommendations to ensure consistency of data across institutions, as well as in the same patient in serial 18F-FDG PET studies:
Patients should avoid strenuous exercise for 24 h before the 18F-FDG PET study to minimize uptake of the radiotracer in muscles.
Patients should, as much as possible, be on a low-carbohydrate diet for 24 h before the study.
Patients should fast for a minimum of 4 h before receiving the injection of 18F-FDG. In general, patients should not eat anything after midnight if a study is planned for the following morning. For 18F-FDG PET studies performed in the afternoon, a light breakfast with minimal carbohydrate-containing foods is acceptable. However, patients should fast for at least 4 h after finishing that meal. While fasting, patients should consume at least two to three 355-mL (12-oz) glasses of water to ensure adequate hydration.
When patients arrive at the PET facility, their height and weight should be measured and recorded. Venous serum glucose should be measured to determine whether the concentration is within the reference range (<120 mg/dL for nondiabetic patients and 150−200 mg/dL for diabetic patients). Before injection of the 18F-FDG tracer, patients should be asked to urinate to minimize the possibility that they will need to move during the 18F-FDG uptake phase.
If the serum glucose concentration is greater than 200 mg/dL, the study should be rescheduled. The glucose concentration should be measured consistently and accurately across all patients, preferably by a credentialed clinical laboratory. Insulin should not be used to adjust the blood glucose at the time of the imaging procedure.
A medical history should be obtained from patients. Any history of previous treatment with radiation, chemotherapy, or other experimental therapeutics, and when these therapies were performed and completed, should be documented. In particular, the use of medications that may affect the uptake or biodistribution of 18F-FDG, such as marrow-stimulating cytokines or steroids, should be noted. These data are important in assessing the interval from the completion of a certain therapy to the time of the 18F-FDG PET study to ensure that all relevant confounding clinical issues are identified.
Adequate hydration is important in 18F-FDG PET to ensure excretion of 18F-FDG from background tissue. If possible, patients should drink 500 mL of water after injection and before scanning. Depending on the type of study performed and the area of clinical concern, a urinary (e.g., Foley) catheter may be required to ensure adequate visualization of pelvic structures. If the patient is to be catheterized for the imaging study, the bladder catheter should be placed before the 18F-FDG injection. In other instances (or in addition to Foley catheter placement), for specific imaging of the pelvis or kidney region, intravenous administration of a diuretic, such as furosemide, 20–40 mg, may be required. The diuretic should be administered approximately 10–15 min after injection of the 18F-FDG to allow time for the drug to clear 18F-FDG from the renal collecting system and for patients to void before being placed on the scanner. If there are no medical contraindications, patients requiring clearance of the urinary background activity should receive 250–500 mL of intravenous saline (not dextrose-containing solutions) during the 18F-FDG uptake period to ensure adequate hydration.
Patients should be placed in a comfortable position, either supine or semirecumbent, in a dimly lit, quiet room. The room should be kept warm to avoid shivering and other temperature effects that may increase muscular or fat uptake. A large-bore intravenous line (21 gauge or greater) should be placed in an arm or hand vein contralateral to any known site of disease.
The dose of 18F-FDG should be 5.18–7.77 MBq (0.14–0.21 mCi) per kilogram of body weight, with a typical range of 370–740 MBq (10–20 mCi). This amount may need to be adjusted for a 3-dimensional brain acquisition. The exact times at which the dose is calibrated and the injection given should be recorded to permit correction of the administered dose for radioactive decay. In addition, the dose remaining in the tubing or syringe, or that spilled during injection, should be recorded. The injection should be performed through an intravenous catheter using a slow infusion over 1–2 min.
The administration of a sedative, such as diazepam, is at the discretion of the clinician. A sedative can facilitate muscle relaxation and reduce 18F-FDG uptake in muscle and brown fat—particularly important for patients who are extremely anxious or for whom the area of interest is the head and neck. In patients with a history of or a suspicion of head and neck tumors, a benzodiazepine or similar sedative, if not medically contraindicated, should be administered orally or intravenously approximately 30 min before injection of the 18F-FDG to ensure a degree of relaxation of the neck muscles. The amount and timing of the sedative should be documented.
Whole-body imaging should begin 60 ± 10 min (mean ± SD) after injection.
Image Acquisition and Reconstruction
Because the specifications of PET cameras are variable and manufacturer specific, every attempt should be made to use the same scanner (ideally at the same center) or same scanner model for serial scanning of the same patient. Whole-body acquisition is important because it allows for sampling of all areas of interest and can assess whether new lesions have appeared and, thus, the possibility that disease has progressed. Whole-body acquisitions can be in either 2- or 3-dimensional mode with attenuation correction, but a consistent method should be chosen for all serial scanning of an individual patient throughout the clinical trial. The use of CT in combined PET/CT scanners is strongly encouraged to provide anatomic registration for PET data.
The whole-body acquisition should sample from the angle of the jaw to the level of the mid thigh. Because several target lesions may be identified on the initial 18F-FDG PET study or on anatomic imaging studies, it is critical that for a given patient, all subsequent 18F-FDG PET studies be performed identically to the first to ensure the quantitative integrity of the data and the validity of comparisons. For example, if the patient is scanned from the head to the thighs in the baseline scan, subsequent scans should also be started at the head and extend to the thighs. The parameters for the timing of both emission and transmission acquisitions vary from one patient to another depending on the size of the patient, the PET camera used, and the amount of 18F-FDG injected. Therefore, the timing of the acquisitions cannot be standardized. However, the times at which target lesions are imaged after 18F-FDG injection should be as close as possible to those used on the baseline or previous study. It is strongly encouraged that serial studies to evaluate therapeutic response be done in exactly the same way, at the same institution, on the same type of camera, and using the same dose, imaging times, acquisition parameters, and reconstruction parameters.
Patients with head and neck malignancies may require more extensive imaging of the head. Some patients (e.g., those with malignant melanoma or sarcoma) may require imaging of the lower extremities. Patients with brain tumors require imaging of the whole brain, typically using either 1 or 2 acquisitions and bed positions depending on the field of view of the PET camera.
PET Timing Relative to Prior Therapy
Insufficient data are available on the optimal interval from completion of therapy to imaging with 18F-FDG PET. Nevertheless, the working group recommends that the complete treatment history of the patient be documented, particularly the use of supportive therapies such as bone marrow expansion drugs and the recent use of corticosteroids. Pretreatment scanning is generally critical to assess subsequent response. The timing of posttreatment scanning depends on numerous variables, including correlative studies, whether a complete clinical response variable is under consideration, the expected responsiveness of the tumor type to the therapy being used, and the endpoints of the study.
Currently available information supports the recommendation that posttreatment imaging be performed 2 wk after the end of a specific chemotherapy cycle. The exact timing may depend on the frequency and duration of therapy. It is postulated that the transient and nondurable alterations in 18F-FDG uptake that may occur in tumors during the immediate-posttreatment period will be minimized using this approach. A specific understanding of the basic biology of the tumor from previous clinical and preclinical studies may help one determine the optimal posttreatment time point.
Data on the treatment interval after the completion of radiotherapy are less clear. Acute inflammatory changes with subsequent alterations in 18F-FDG uptake in both tumor and surrounding tissue have been documented (31). Newer radiation therapies such as γ-knife and focal high-dose radiation appear to enhance inflammatory reactions, and thus confound the interpretation of 18F-FDG PET scans, in patients studied within a short period after completing these therapies (32). Many investigators recommend a delay of 6−8 wk or longer after radiation therapy before performing the posttreatment 18F-FDG PET study (33). Although further study may be required to arrive at an appropriate interval for scanning after completion of radiation therapy, a longer wait clearly helps in distinguishing inflammatory response from viable residual tumor.
Image Analysis
The working group agreed that there is no single optimal method for analysis of 18F-FDG PET whole-body images in oncology but that there can be standardized protocols for use in a particular clinical trial. The working group recommended that phase I trials use either full or partial kinetic analysis, such as Patlak analysis, if deemed necessary, along with semiquantitative SUV analysis based on lean body mass and body surface area. The reason for recommending that SUVs be calculated on the basis of both lean body mass and body surface area is to develop a body of data to determine whether they are equivalent or whether one is better than the other. It is also critical that before a particular clinical trial begins, the method of ROI determination be agreed on and specified in the protocol.
Of obvious importance is that whole-body 18F-FDG PET provides information additional to that obtained from standard anatomic imaging studies such as CT or MRI. Therefore, it is also critical that the whole-body 18F-FDG PET study be interpreted carefully and reported as a clinical study would be reported to ensure that new lesions are identified. This care will be critical in the development of subsequent response criteria. SUV should be determined in order to assess the 18F-FDG uptake and define the response in target lesions of interest. Image reconstruction parameters depend on the PET scanner and other variables. Filters, image reconstruction techniques and parameters, and application of the attenuation map must be consistent across all scanning of a given patient. The exact timing of image acquisition for each target lesion is critical and must be kept constant on all subsequent studies of a given patient.
SUV should be determined for all target lesions and should be calculated consistently on the basis of either lean body mass or body surface area. No data indicate that one is superior to the other. Each clinical trial should set a protocol calling for all SUV calculations to be done the same way.
In addition, the SUV of a reference organ or tissue not involved in the neoplastic process should be measured after each scan to help ensure that SUV changes in tumors are related either to treatment response or to disease progression.
ROI Determination
Tumors can be of various sizes and of various heterogeneities. Accurate and reproducible determination of the ROI will be critical for determining SUV. With therapy, alterations in the pattern of heterogeneity and in 18F-FDG uptake may occur and must be considered when one is drawing or determining the ROI. On the pretreatment scan, the identified target lesion should be the most visible and easily defined lesion. The mean SUV of the region and the maximum pixel SUV should be determined and recorded.
No prescribed methodologies for determining regions of interest have been validated. Thresholding techniques or freehand drawing are typically used. No specific recommendations on either of these approaches can be made. The choice of method will depend on the technical support staff, expertise, and image-processing capabilities of an individual PET center. However, in each clinical trial, the same ROI technique should be specified (e.g., whether to include necrotic areas) and used in subsequent 18F-FDG PET studies to ensure quantitative consistency. Quantitative measurements of mean and maximum tumor ROI counts per pixel, calibrated as mBq/L (μCi/L), should be obtained with the scanner. The consensus of the working group was that maximum or “peak” approaches are the most robust and reproducible and that the maximum SUV and mean SUV of each tumor should be recorded. The panel strongly encouraged further cooperative studies, including work with camera manufacturers, to improve reproducibility and standardization between centers by developing more standard and automated methods of defining regions.
During the course of treatment, the extent and shape of an imaged tumor might change. Documentation of either an increase or a decrease in dimensions or a change in shape is recommended.
As discussed, partial-volume effects on determinations of 18F-FDG uptake may be significant. If a significant decrease in tumor size is evident from anatomic imaging studies (which are typically available throughout therapy), this information should be documented because subsequent analysis may require partial-volume corrections of the 18F-FDG PET data. Further data analysis and research are required to better define how the assessment of response can be adjusted to account for partial-volume effects, tumor heterogeneity, and other confounding variables.
CONCLUSION
18F-FDG PET has gained acceptance as a valuable clinical tool for detecting, staging, and managing disease. It is now clear that 18F-FDG PET can also be an important tool for assessing therapeutic efficacy in large, multicenter clinical trials, but only with the application of standard protocols. Currently, there is no one best methodology for obtaining or analyzing 18F-FDG PET scans, nor is there one agreed-on standard for judging the significance of a response seen on 18F-FDG PET. Enacting these recommendations to develop standard protocols for NCI-sponsored clinical trials should go a long way toward determining when and for what indications 18F-FDG PET can serve as a surrogate measure of therapeutic efficacy. The result should be shorter clinical trials and improved therapy for patients with cancer.
References
- Received for publication March 1, 2006.
- Accepted for publication March 10, 2006.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Principles of Tracer Kinetic Analysis in Oncology, Part II: Examples and Future Directions
- Whole-Body Parametric Imaging of 18F-FDG PET Using uEXPLORER with Reduced Scanning Time
- Performance of Digital PET Compared with High-Resolution Conventional PET in Patients with Cancer
- Does 2-FDG PET Accurately Reflect Quantitative In Vivo Glucose Utilization?
- Linsitinib (OSI-906) for the Treatment of Adult and Pediatric Wild-Type Gastrointestinal Stromal Tumors, a SARC Phase II Study
- First-in-Human Phase I Study to Evaluate the Brain-Penetrant PI3K/mTOR Inhibitor GDC-0084 in Patients with Progressive or Recurrent High-Grade Glioma
- Use of a Qualification Phantom for PET Brain Imaging in a Multicenter Consortium: A Collaboration Between the Pediatric Brain Tumor Consortium and the SNMMI Clinical Trials Network
- Prospective Study of Serial 18F-FDG PET and 18F-Fluoride PET to Predict Time to Skeletal-Related Events, Time to Progression, and Survival in Patients with Bone-Dominant Metastatic Breast Cancer
- Early prediction of lenvatinib treatment efficacy by using 18F-FDG PET/CT in patients with unresectable or advanced thyroid carcinoma that is refractory to radioiodine treatment: a protocol for a non-randomized single-arm multicenter observational study
- Linker engineering in anti-TAG-72 antibody fragments optimizes biophysical properties, serum half-life, and high-specificity tumor imaging
- Test-Retest Variability in Lesion SUV and Lesion SUR in 18F-FDG PET: An Analysis of Data from Two Prospective Multicenter Trials
- 89Zr-anti-{gamma}H2AX-TAT but not 18F-FDG Allows Early Monitoring of Response to Chemotherapy in a Mouse Model of Pancreatic Ductal Adenocarcinoma
- Qualification of National Cancer Institute-Designated Cancer Centers for Quantitative PET/CT Imaging in Clinical Trials
- Repeatability of SUV in Oncologic 18F-FDG PET
- Reliability of PET/CT Shape and Heterogeneity Features in Functional and Morphologic Components of Non-Small Cell Lung Cancer Tumors: A Repeatability Analysis in a Prospective Multicenter Cohort
- Getting the Most out of 18F-FDG PET Scans: The Predictive Value of 18F-FDG PET-Derived Blood Flow Estimates for Breast Cancer
- Accuracy and Precision of Partial-Volume Correction in Oncological PET/CT Studies
- Multicenter Clinical Trials Using 18F-FDG PET to Measure Early Response to Oncologic Therapy: Effects of Injection-to-Acquisition Time Variability on Required Sample Size
- Dose-Finding Quantitative 18F-FDG PET Imaging Study with the Oral Pan-AKT Inhibitor GSK2141795 in Patients with Gynecologic Malignancies
- Molecular Imaging to Plan Radiotherapy and Evaluate Its Efficacy
- Complexity of Response Evaluation During Primary Systemic Therapy of Breast Cancer: Scoring Systems and Beyond-Preliminary Results
- Phase II Study of Lapatinib in Combination With Trastuzumab in Patients With Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer: Clinical Outcomes and Predictive Value of Early [18F]Fluorodeoxyglucose Positron Emission Tomography Imaging (TBCRC 003)
- Repeatability of 18F-FDG PET/CT in Advanced Non-Small Cell Lung Cancer: Prospective Assessment in 2 Multicenter Trials
- 18F-FLT PET Evaluation of Radiation Response
- Summary of the UPICT Protocol for 18F-FDG PET/CT Imaging in Oncology Clinical Trials
- FDG PET-CT in follicular lymphoma: a case-based evidence review
- TBCRC 008: Early Change in 18F-FDG Uptake on PET Predicts Response to Preoperative Systemic Therapy in Human Epidermal Growth Factor Receptor 2-Negative Primary Operable Breast Cancer
- Quantitative PET/CT Scanner Performance Characterization Based Upon the Society of Nuclear Medicine and Molecular Imaging Clinical Trials Network Oncology Clinical Simulator Phantom
- Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group
- The predictive role of interim positron emission tomography for Hodgkin lymphoma treatment outcome is confirmed using the interpretation criteria of the Deauville five-point scale
- Sarcoma Mid-Therapy [F-18]Fluorodeoxyglucose Positron Emission Tomography (FDG PET) and Patient Outcome
- Early Predictive Value of Non-response to Docetaxel in Neoadjuvant Chemotherapy in Breast Cancer Using 18F-FDG-PET
- Impact of Different Standardized Uptake Value Measures on PET-Based Quantification of Treatment Response
- Interim 18F-FDG PET in Hodgkin Lymphoma: Would PET-Adapted Clinical Trials Lead to a Paradigm Shift?
- Comparison of EORTC Criteria and PERCIST for PET/CT Response Evaluation of Patients with Metastatic Colorectal Cancer Treated with Irinotecan and Cetuximab
- Reporting Guidance for Oncologic 18F-FDG PET/CT Imaging
- Differences in the Biologic Activity of 2 Novel MEK Inhibitors Revealed by 18F-FDG PET: Analysis of Imaging Data from 2 Phase I Trials
- Sepantronium Bromide (YM155) Enhances Response of Human B-Cell Non-Hodgkin Lymphoma to Rituximab
- Noise Considerations for PET Quantification Using Maximum and Peak Standardized Uptake Value
- 18F-FDG-PET/CT Imaging as an Early Survival Predictor in Patients with Primary High-Grade Soft Tissue Sarcomas Undergoing Neoadjuvant Therapy
- 18F-FDG PET as a Surrogate Biomarker in Non-Small Cell Lung Cancer Treated with Erlotinib: Newly Identified Lesions Are More Informative Than Standardized Uptake Value
- Assessment of Valvular Calcification and Inflammation by Positron Emission Tomography in Patients With Aortic Stenosis
- Mutatis Mutandis: Harmonize the Standard!
- Need for Standardization of 18F-FDG PET/CT for Treatment Response Assessments
- Imaging in Sarcoma
- 18F-FDG PET/CT for Monitoring Treatment Responses to the Epidermal Growth Factor Receptor Inhibitor Erlotinib
- Prevalence and Risk Factors of Carotid Vessel Wall Inflammation in Coronary Artery Disease Patients: FDG-PET and CT Imaging Study
- Practical Approach for Comparative Analysis of Multilesion Molecular Imaging Using a Semiautomated Program for PET/CT
- Positron Emission Tomography-Computed Tomography (PET-CT) After Induction Therapy Is Highly Predictive of Patient Outcome in Follicular Lymphoma: Analysis of PET-CT in a Subset of PRIMA Trial Participants
- FDG-PET as a Potential Tool for Selecting Patients with Advanced Non-Small Cell Lung Cancer Who May Be Spared Maintenance Therapy after First-Line Chemotherapy
- Changes in 18F-Fluorodeoxyglucose and 18F-Fluorodeoxythymidine Positron Emission Tomography Imaging in Patients with Non-Small Cell Lung Cancer Treated with Erlotinib
- Standardization of Quantitative Imaging: The Time Is Right, and 18F-FDG PET/CT Is a Good Place to Start
- Variations in Clinical PET/CT Operations: Results of an International Survey of Active PET/CT Users
- PET and PET/CT of the Neck Lymph Nodes Improves Risk Prediction in Patients with Squamous Cell Carcinoma of the Oral Cavity
- Variations in PET/CT Methodology for Oncologic Imaging at U.S. Academic Medical Centers: An Imaging Response Assessment Team Survey
- Monitoring Response to Antiangiogenic Therapy in Non-Small Cell Lung Cancer Using Imaging Markers Derived from PET and Dynamic Contrast-Enhanced MRI
- Phase II Study of Daily Sunitinib in FDG-PET-Positive, Iodine-Refractory Differentiated Thyroid Cancer and Metastatic Medullary Carcinoma of the Thyroid with Functional Imaging Correlation
- A functional dynamic scoring model to elucidate the significance of post-induction interim fluorine-18-fluorodeoxyglucose positron emission tomography findings in patients with Hodgkin's lymphoma
- Imaging Atherosclerotic Plaque Inflammation by Fluorodeoxyglucose With Positron Emission Tomography: Ready for Prime Time?
- Imaging in drug development: will it deliver on the promise of personalised medicine?
- SUVs: Always a Good Choice?
- Guidelines for the Development and Incorporation of Biomarker Studies in Early Clinical Trials of Novel Agents
- A Phase I Clinical Trial of CHT-25 a 131I-Labeled Chimeric Anti-CD25 Antibody Showing Efficacy in Patients with Refractory Lymphoma
- Phase I Biodistribution and Pharmacokinetic Study of Lewis Y-Targeting Immunoconjugate CMD-193 in Patients with Advanced Epithelial Cancers
- Frontiers of Biomedical Imaging Science 2009: Workshop Report and Research Opportunities
- Expert Opinions on Positron Emission Tomography and Computed Tomography Imaging in Lymphoma
- 18F-FDG PET/CT for Image-Guided and Intensity-Modulated Radiotherapy
- Repeatability of 18F-FDG PET in a Multicenter Phase I Study of Patients with Advanced Gastrointestinal Malignancies
- Chemotherapy Response Evaluation in Metastatic Colorectal Cancer with FDG PET/CT and CT Scans
- Qualification of PET Scanners for Use in Multicenter Cancer Clinical Trials: The American College of Radiology Imaging Network Experience
- Comparison of Imaging Protocols for 18F-FDG PET/CT in Overweight Patients: Optimizing Scan Duration Versus Administered Dose
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Monitoring Predominantly Cytostatic Treatment Response with 18F-FDG PET
- Role of 18F-FDG PET in Assessment of Response in Non-Small Cell Lung Cancer
- From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors
- Standards for PET Image Acquisition and Quantitative Data Analysis
- FDG-PET/CT Imaging Predicts Histopathologic Treatment Responses after the Initial Cycle of Neoadjuvant Chemotherapy in High-Grade Soft-Tissue Sarcomas
- Measuring Response with FDG-PET: Methodological Aspects
- Considerations for the Use of Imaging Tools for Phase II Treatment Trials in Oncology
- 18F-FDG PET/CT as an Indicator of Progression-Free and Overall Survival in Osteosarcoma
- Relationships Among Regional Arterial Inflammation, Calcification, Risk Factors, and Biomarkers: A Prospective Fluorodeoxyglucose Positron-Emission Tomography/Computed Tomography Imaging Study
- Standardization of Scanning for [18F]Fluorodeoxyglucose Positron Emission Tomography
- In Reply
- Imaging Surrogates of Tumor Response to Therapy: Anatomic and Functional Biomarkers
- Early Prediction of Response to Sunitinib After Imatinib Failure by 18F-Fluorodeoxyglucose Positron Emission Tomography in Patients With Gastrointestinal Stromal Tumor
- 18F-FDG PET and PET/CT in the Evaluation of Cancer Treatment Response
- Spatial Heterogeneity in Sarcoma 18F-FDG Uptake as a Predictor of Patient Outcome
- [18F]Fluorothymidine Positron Emission Tomography before and 7 Days after Gefitinib Treatment Predicts Response in Patients with Advanced Adenocarcinoma of the Lung
- Combined Assessment of Metabolic and Volumetric Changes for Assessment of Tumor Response in Patients with Soft-Tissue Sarcomas
- Tumor Metabolism and Blood Flow Changes by Positron Emission Tomography: Relation to Survival in Patients Treated With Neoadjuvant Chemotherapy for Locally Advanced Breast Cancer
- The role of clinical imaging in oncological drug development
- Analysis and Reproducibility of 3'-Deoxy-3'-[18F]Fluorothymidine Positron Emission Tomography Imaging in Patients with Non-Small Cell Lung Cancer
- Treatment Monitoring by 18F-FDG PET/CT in Patients with Sarcomas: Interobserver Variability of Quantitative Parameters in Treatment-Induced Changes in Histopathologically Responding and Nonresponding Tumors
- Atherosclerosis Inflammation Imaging with 18F-FDG PET: Carotid, Iliac, and Femoral Uptake Reproducibility, Quantification Methods, and Recommendations
- Molecular Imaging of Metastatic Potential
- Reduction of Glucose Metabolic Activity Is More Accurate than Change in Size at Predicting Histopathologic Response to Neoadjuvant Therapy in High-Grade Soft-Tissue Sarcomas
- The role of FDG-PET scans in patients with lymphoma
- Prospective Assessment of Discontinuation and Reinitiation of Erlotinib or Gefitinib in Patients with Acquired Resistance to Erlotinib or Gefitinib Followed by the Addition of Everolimus
- Early Prediction of Response to Chemotherapy and Survival in Malignant Pleural Mesothelioma Using a Novel Semiautomated 3-Dimensional Volume-Based Analysis of Serial 18F-FDG PET Scans