


Abstract
We prospectively evaluated the sensitivity and specificity of 18F-FDG PET in the detection of neck lymph node metastases in patients with oral cavity squamous cell carcinoma (OSCC). We also sought to evaluate whether pretreatment PET visual scores in the neck lymph nodes may improve risk stratification. Methods: We enrolled 473 OSCC patients (445 men and 28 women; mean age ± SD, 50.9 ± 11.7 y) without distant metastases. All participants underwent 18F-FDG PET within 2 wk before surgery and neck dissection. Histopathology was taken as the reference standard for neck lymph node status. The duration of follow-up was at least 24 mo in all surviving patients. Results: 18F-FDG PET correctly diagnosed 164 of 211 patients with neck metastases and 152 of 262 subjects without pathologic neck metastases, resulting in a patient-based sensitivity and specificity of 77.7% and 58.0%, respectively. In Cox models adjusting for age, sex, traditional risk factors, and treatment modality, PET results at the neck lymph nodes were significantly and independently associated with rates of neck control, distant metastasis, disease-free survival, disease-specific survival, and overall survival. Notably, the results of the c-statistics demonstrated that PET score improved the accuracy of risk prediction in terms of overall and disease-free survival rates. Conclusion: PET findings at the neck lymph nodes have limited sensitivity and specificity for primary staging of OSCC but improve risk stratification beyond that of traditional risk factors.
Head and neck carcinomas are the sixth most common malignancy reported worldwide, and oral cavity squamous cell carcinoma (OSCC) is the most frequent neoplasm in this region ( 1). The routine staging method for the preoperative detection of cervical lymph node metastases in OSCC patients consists of physical examination and CT/MRI. The presence and extent of neck lymph node metastases (pN+) significantly affect outcomes and potential treatment strategies in OSCC patients ( 2– 10). Despite the prognostic value of neck lymph node metastases, this factor does not fully explain the extent of variability in the clinical course ( 2– 10).
PET using the radiolabeled glucose analog 18F-FDG has great importance in lymph node imaging ( 11, 12). However, controversy still exists on its routine clinical use in cN0 OSCC patients because of the limited additional value of 18F-FDG PET ( 13). Unlike other anatomic imaging modalities, PET supplies a semiquantitative metabolic characterization of tissues that may help to predict tumor behavior. In 2 recent studies in nonselected patients with head and neck cancers, the sensitivity and specificity of 18F-FDG PET for identification of lymph node metastases on a neck level-by-level basis were higher than those of CT/MRI ( 14, 15). However, the accuracy of 18F-FDG PET neck staging in OSCC should be evaluated by comparing it against the gold standard of pathologic staging. Unfortunately, this issue has not been fully addressed in previous studies ( 14– 18). Although 18F-FDG PET may be more accurate for lymph node staging than anatomic imaging studies, this, by itself, may not affect patient management and the policy of neck dissection (ND). Therefore, the clinical implications of 18F-FDG PET for primary and nodal staging of patients with OSCC deserve further scrutiny.
18F-FDG PET has prognostic value in OSCC patients ( 13, 19, 20). Notably, 18F-FDG uptake in the primary tumor predicts overall survival in different cancers ( 21– 26), including OSCC ( 27). However, little has been reported about the prognostic significance of PET findings in the neck lymph nodes in patients with OSCC. The ability to identify patients who display a poor prognosis would be beneficial in at least 2 ways. First, identifying high-risk patients may reveal a survival benefit from postsurgical adjuvant therapies. Second, a better prognostic stratification may allow the identification of low-risk patients who can achieve adequate survival with less radical approaches. Numerous clinical features and pathologic characteristics have been studied in an attempt to improve risk stratification. These negative prognostic factors include extracapsular spread (ECS), close or positive margins, perineural invasion, level IV or V lymph node metastases, poor differentiation, tumor depth, and the number of metastatic neck lymph nodes ( 2– 10). However, the incorporation of functional information derived from PET has the potential to improve prognostic stratification and treatment planning for patients with OSCC. A large cohort of OSCC patients has been and continues to be enrolled in our hospital, allowing us to take advantage of the large sample sizes to demonstrate the potential impact of 18F-FDG PET/CT on various clinical endpoints.
The objective of this study was 2-fold. The first was to prospectively assess the sensitivity and specificity of 18F-FDG PET/CT for detecting neck lymph node metastases in patients with OSCC, with pathologic results as the reference standard. The second was to investigate whether pretreatment visual scores in the neck lymph nodes may improve risk stratification ( 28).
MATERIALS AND METHODS
Study Patients
Between August 2001 and May 2008, patients with a histologic diagnosis of OSCC, a previously untreated tumor scheduled for radical surgery with or without ND, and no other suspected distant metastatic lesions detected by imaging (including MRI/CT and 18F-FDG PET/CT) were eligible for the study. All patients expressed willingness to receive a CT- or ultrasound-guided biopsy or surgical exploration, if necessary. Patients with a previous diagnosis of other malignancies and refusal or inability to receive definitive treatment for the disease were excluded. Patients were also excluded if they had hyperglycemia (defined as a serum glucose level of more than 200 mg/dL) before the PET study, because such levels seem to affect the quality of the PET images adversely.
All participants underwent an extensive presurgical evaluation including 18F-FDG PET/CT within 2 wk before primary surgery (median, 2.0 d; mean ± SD, 3.0 ± 2.8 d; range, 1–14 d). This evaluation included a medical history and complete physical examination, flexible fiberoptic laryngopharyngoscopy, complete blood count and routine blood biochemistry, CT or MRI scans of the head and neck, chest radiographs, bone scan, and liver ultrasound. Primary staging was performed according to the 2002 criteria of the American Joint Committee on Cancer (AJCC) ( 29). The study was approved by the Institutional Review Board of the Chang Gung Memorial Hospital (96-0672B). All patients provided their written informed consent.
18F-FDG PET/CT
Patients were instructed to fast for 6 h before the PET study. 18F-FDG (370–444 MBq) was administered intravenously. Before April 2006, all patients (n = 280) underwent PET (ECAT EXACT HR+ PET camera; CTI). As of May 2006, all participants (n = 193) underwent PET/CT (Discovery ST; GE Healthcare), combining a PET component with a 16-slice spiral CT scanner. For PET/CT scans, oral contrast was administered to patients during the uptake time; no intravenous contrast material was administered for CT scans. Head to midthigh scans were obtained for all patients. Lower limb scanning was performed when indicated. PET and CT images were acquired consecutively, 50 min after the injection of 18F-FDG. CT data were used for low-noise attenuation correction of PET emission data and for fusion with attenuation-corrected PET images. PET images were reconstructed iteratively using an ordered-subset expectation maximization algorithm. PET, CT, and fused PET/CT images were available for review and were displayed in axial, coronal, and sagittal planes. PET data were displayed as noncorrected and attenuation-corrected images as well as in a rotating maximum-intensity projection.
All imaging results were reviewed prospectively by a combined team who had knowledge of the patients’ clinical history. Foci of increased 18F-FDG uptake were carefully recorded. Studies showing at least 1 area of increased 18F-FDG uptake with intensity higher than that of surrounding tissues, localized by hybrid images to an area that did not correspond to the physiologic biodistribution of the radiotracer, were defined as positive. Studies showing 18F-FDG activity only in areas of the physiologic tracer biodistribution or no sites of increased uptake were considered negative. Regions of interest were placed and measured over lesions visible on PET images, on simultaneously displayed axial, coronal, and sagittal tomograms. The regions of interest of lesions that were invisible on PET images were located using the corresponding CT images. The highest activity within a region of interest was measured, and the standardized uptake value (SUV) was determined as the highest activity concentration per injected dose per body weight (kg) after correction for radioactive decay. Two experienced nuclear medicine physicians and 1 radiologist interpreted 18F-FDG PET (PET/CT) images. Interpretation was based on visual evaluation, and decisions were reached by consensus. 18F-FDG uptake was graded visually on the following 5-point scale: 0, definitely benign; 1, probably benign; 2, equivocal; 3, probably malignant; and 4, definitely malignant ( 14, 16). This score was based on the intensity of focal 18F-FDG uptake, presence of corresponding lymph node on CT, and pattern of tracer distribution. In an effort to improve sensitivity, findings graded as 2, 3, or 4 were considered positive ( 30).
Surgery and Adjuvant Therapy
The primary tumors were excised with safety margins of 1 cm or greater (both peripheral and deep margins). Classic radical or modified NDs (levels I–V) were performed in patients with clinically positive lymph node disease. Supraomohyoid NDs (levels I–III) were performed in clinically node-negative patients. Postoperative radiotherapy (60–66 Gy) was performed on patients with pT4 tumors, positive lymph nodes, or close margins (≤4 mm). Concomitant chemoradiation with cisplatin (50 mg/m2) biweekly plus daily oral tegafur (800 mg) and leucovorin (60 mg) or cisplatin (30 mg/m2) weekly was administered to patients with ECS or multiple lymph node metastases ( 31, 32).
Data Analysis
All patients were followed for at least 24 mo after surgery or until death. Study participants were followed through May 2010 for 6 outcomes: local control, neck control, distant metastasis, disease-free survival, disease-specific survival, and overall survival. Cumulative survival plots according to the PET score in the neck lymph nodes were univariately evaluated by the Kaplan–Meier analysis (log-rank test). Because the Kaplan–Meier method cannot adjust for the effects of other factors, we used a series of multivariable proportional-hazards models to examine the association between the PET score in the neck lymph nodes and the study outcomes. We first confirmed that the proportional-hazards assumption was met. The hazard ratios for the PET score at the neck lymph node were estimated in a model adjusting for age, sex, and known prognostic factors (ECS, close or positive margins, perineural invasion, level IV or V lymph node metastasis, poor differentiation, tumor depth, at least 5 metastatic neck lymph nodes, and treatment modality) in OSCC patients. To evaluate the ability of the PET score to predict prognosis, we compared the c-statistics for the combination of 8 known clinical and pathologic prognostic factors (ECS, close or positive margins, perineural invasion, level IV or V lymph node metastasis, poor differentiation, tumor depth, presence of at least 5 metastatic neck lymph nodes, and treatment modality) with or without the PET score. In this analysis, we used disease-free and overall survival rates at 5 y as the outcome measures. Statistical calculations were performed with SPSS software (version 17.0; SPSS). The tests for the proportional-hazards assumption were performed with the survival package for R; the areas under the receiver operating characteristic (ROC) curves given by c-statistics were determined with the ROCR package for R (www.r-project.org). Two-sided P values less than 0.05 were considered statistically significant.
RESULTS
The baseline characteristics of the study participants are shown in Tables 1 and 2.
Clinicopathologic Characteristics of Study Participants
Tumor Subsites of Study Participants
Detection of Neck Metastases with PET
Of the 473 patients examined, 211 were diagnosed with pathologically positive lymph nodes whereas the remaining 262 were without neck metastases. In the entire study cohort, 179 patients had a preoperative PET-negative neck with no 18F-FDG uptake (visual score of 0), 20 had a faint tracer uptake, 49 a mild uptake, 79 a moderate uptake, and 146 an intense uptake (visual score of 4). 18F-FDG PET correctly diagnosed 164 of 211 patients with neck metastases and 152 of 262 patients without pathologic neck metastases, resulting in a sensitivity and specificity of 77.7% and 58.0%, respectively, on a patient-based analysis, using a cutoff of 2 for the 18F-FDG uptake score. Compared with subjects with a PET-negative neck, those with a PET-positive neck showed significant differences in clinical nodal status, ND, treatment modality, tumor depth, pathologic T and N status, pN2c status, ECS, bone marrow invasion, perineural invasion, and lymph invasion ( Tables 1 and 2).
The median SUVs were 2.3 (range, 1.4–4.0) for lesions with a score of 1, 2.6 (range, 1.4–4.4) for lesions with a score of 2, 3.5 (range, 2.1–7.9) for lesions with a score of 3, and 6.6 (range, 2.6–24.5) for lesions with a score of 4. When an SUV of 3.1 was used as the cutoff for positive PET results, the ROC analysis showed a patient-based sensitivity and specificity of 79.9% and 59.4%, respectively. The areas under the ROC curves, which represent overall diagnostic performance, did not differ significantly among the 2 analytic methods (visual, 0.81; SUV, 0.83). Therefore, only visual scores were considered for further analysis.
PET Findings and Pathologic Size of Neck Lymph Node Metastasis
The correlation of lymph node size and PET results in the 211 patients diagnosed with positive lymph nodes on histopathology is shown in Table 3. The size distribution of lymph node metastases showed significant differences according to PET results (χ2 = 57.73, P < 0.001).
Results of 18F-FDG PET and Pathologic Tumor Size in pN+ OSCC Patients
PET Findings and Clinical Course
Categorization of the entire patient population according to PET scores revealed a statistically significant trend toward higher event rates through increasing PET scores in terms of neck control ( Fig. 1A), distant metastasis ( Fig. 1B), disease-free survival ( Fig. 1C), disease-specific survival ( Fig. 1D), and overall survival rates ( Fig. 1E). We observed no association of PET scores with local control ( Fig. 1F).
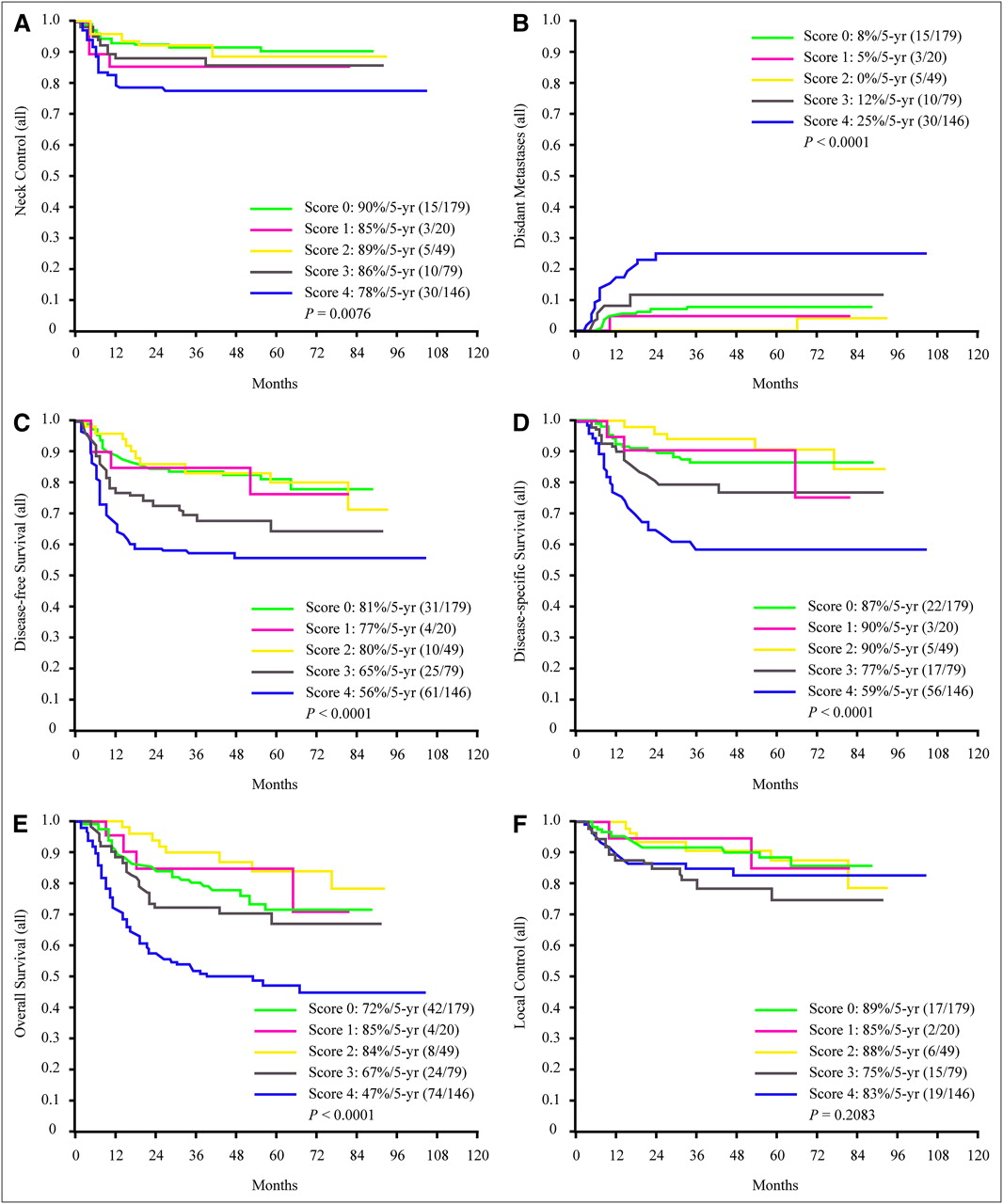
Kaplan–Meier curves for study outcomes, by PET scores in neck lymph nodes. Results are presented in terms of neck control (A), distant metastasis (B), disease-free survival (C), disease-specific survival (D), and overall survival rates (E). We observed no association of PET scores with local control (F).
Multivariable Analysis of Outcomes
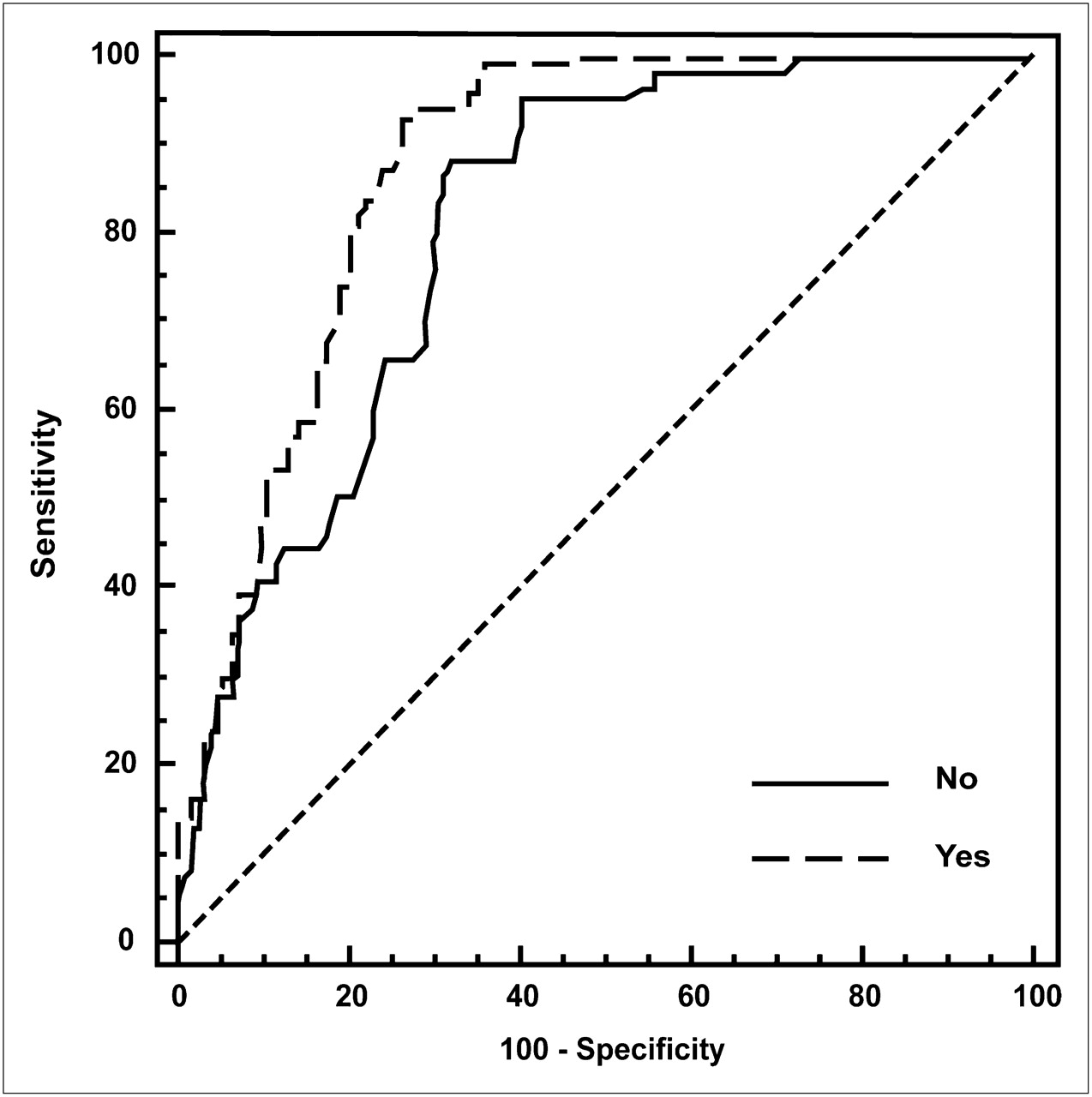
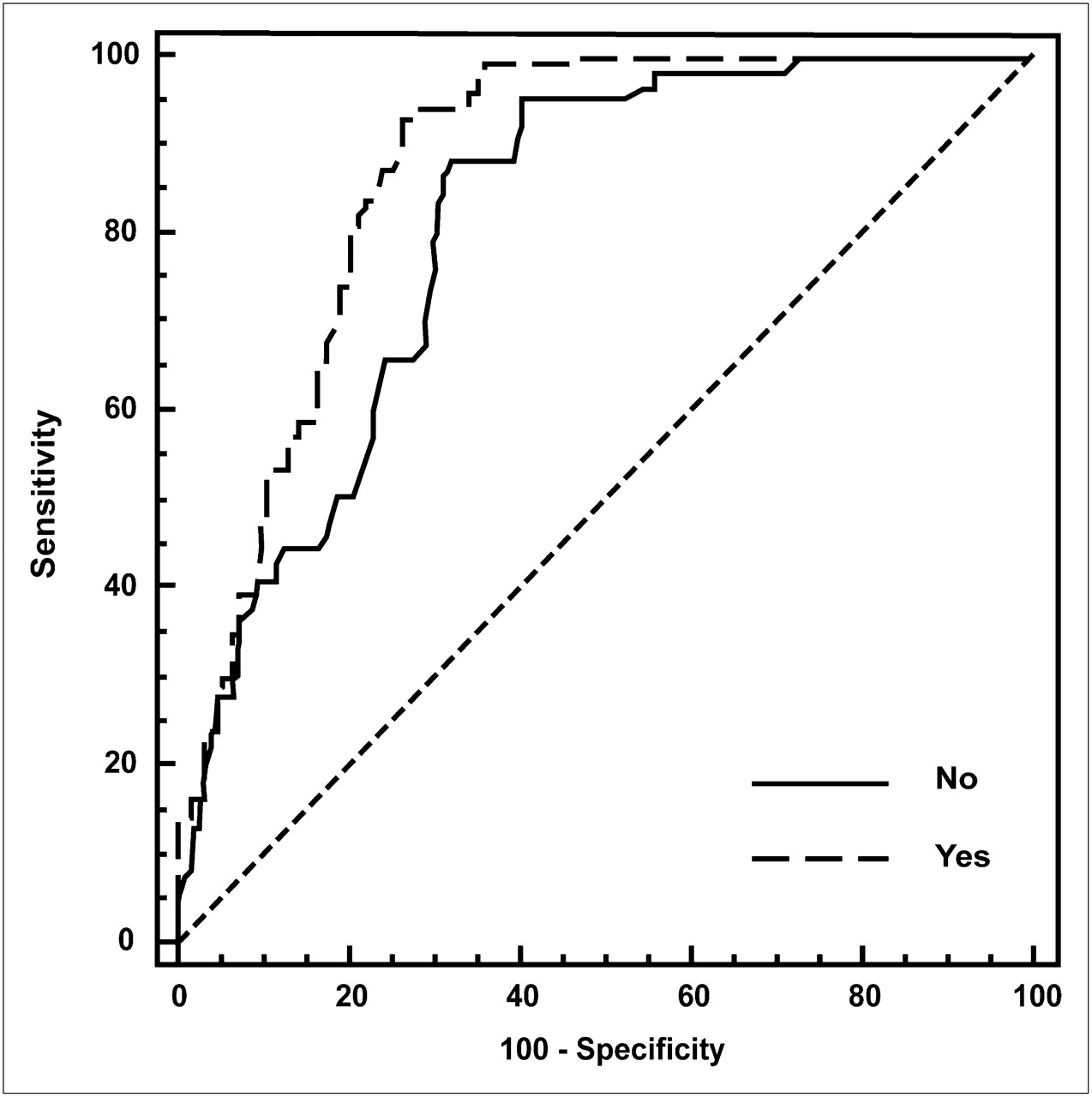
In Cox models adjusting for age, sex, known prognostic factors, and treatment modalities, a PET score of 2 or more in the neck lymph nodes was independently associated with rates of neck control (hazard ratio [HR], 1.36; 95% confidence interval [CI], 1.03–2.01; P < 0.05), distant metastasis (HR, 1.44; 95% CI, 1.13–2.42; P < 0.01), disease-free survival (HR, 1.58; 95% CI, 1.32–2.32; P < 0.01), disease-specific survival (HR, 1.39; 95% CI, 1.08–2.07; P < 0.05), and overall survival (HR, 1.65; 95% CI, 1.24–2.42; P < 0.01). We then determined the c-statistics for the model incorporating established risk factors (ECS, close or positive margins, perineural invasion, level IV or V lymph node metastasis, poor differentiation, tumor depth, presence of at least 5 metastatic neck lymph nodes, and treatment modality) with and without inclusion of the PET score, using disease-free and overall survival rates at 5 y as the outcome measures. The c-statistic for disease-free survival was 0.84 for the risk model without the PET score and 0.90 with the PET score at the neck lymph node (P < 0.01, Fig. 2). For overall survival, the c-statistic was 0.83 for the risk model without the PET score and 0.87 with the PET score (P < 0.05, Fig. 3).

ROC curves for disease-free survival rates. Curves are based on risk-prediction models incorporating established risk factors (extracapsular spread, close or positive margins, perineural invasion, level IV or V lymph node metastasis, poor differentiation, tumor depth, presence of at least 5 metastatic neck lymph nodes, and treatment modality) that either included PET score at neck lymph nodes (dotted line) or did not include PET score (solid line). c-statistic was 0.84 for risk model without PET score and 0.90 with PET score at neck lymph nodes (P < 0.01).
ROC curves for overall survival rates. Curves are based on risk-prediction models incorporating established risk factors (extracapsular spread, close or positive margins, perineural invasion, level IV or V lymph node metastasis, poor differentiation, tumor depth, presence of at least 5 metastatic neck lymph nodes, and treatment modality) that either included PET score at neck lymph nodes (dotted line) or did not include PET score (solid line). c-statistic was 0.83 for risk model without PET score and 0.87 with PET score (P < 0.05)
DISCUSSION
There are 2 principal findings in this study. First, we have shown that PET has suboptimal diagnostic sensitivity and specificity for primary staging of the neck in OSCC patients. However, we found that PET scores at the neck lymph node predicted clinical outcomes in a large group of OSCC patients in an endemic “betel quid chewing” (one of the carcinogens of OSCC) area. Importantly, the PET score improved the accuracy of risk prediction in terms of overall and disease-free survival rates, as assessed by the c-statistics.
Why might PET findings at the neck lymph nodes help predict outcomes even after accounting for established risk factors and in the absence of major diagnostic capacity for primary staging? Our results showed that PET could detect small amounts of macroscopic disease at the neck lymph nodes but did not have acceptable sensitivity in the detection of microscopic disease ( Table 3). Because of limited spatial resolution, PET appears insufficiently sensitive to identify microscopic neck lymph node metastases in OSCC patients. An alternative possibility is that neck lymph node metastasis from low-grade primary tumors may display relatively poor uptake of 18F-FDG, leading to a reduced sensitivity. However, an important strength of the use of PET is the ability to measure the intensity of metabolic activity ( 17, 27). When added to conventional prognostic factors, we found that the PET score at the neck lymph node did improve the ability to determine which patients will have a poor outcome for disease-free and overall survival and which will remain disease-free at follow-up. These results clearly suggest that PET at the neck lymph node could prove useful in risk stratification or targeting therapies in OSCC patients, even without major diagnostic implications during primary staging. Improvements in prognostic prediction with PET can stem from a variety of sources, including the metabolic discrimination between indolent and aggressive forms of cancers and the possibility of gaining molecular or functional information ( 17, 27). The significant improvement of prognostic stratification of PET in the neck lymph node basin highlights the need to use molecular imaging strategies that focus aggressive treatment strategies on OSCC patients most likely to benefit. In the future, one possible approach would be a 2-step strategy that first would identify OSCC patients at intermediate risk for the clinical outcomes at follow-up via traditional clinical and pathologic prognostic factors, and then further stratify prognosis based on PET findings at the neck lymph nodes. Additional research is required on the effectiveness of 2-step approaches that use improvement of prognostic stratification after consideration of PET findings at the neck lymph nodes. In addition, careful cost-effectiveness strategies should provide more information concerning the absolute degree of risk and costs to detect high-risk OSCC patients. Identifying OSCC patients at risk for adverse outcomes is a dynamic field, and newer molecular tests and imaging modalities are constantly being evaluated to improve our ability to assess risk more accurately so that the most appropriate follow-up and care can be provided.
Three main limitations of our study deserve mention. Our study sample was entirely of Taiwanese ancestry, and all subjects were living in a betel quid chewing area. This factor may limit the generalizability of our results. Second, in the interest of simplicity, we used a PET score based on the actual data for the purpose of analysis. The areas under the ROC curves, which represent overall diagnostic performance, did not differ significantly among the 2 analytic methods (visual, 0.81; SUV, 0.83). Third, the diagnostic performance of PET was estimated using only 18F-FDG as a tracer. Future studies should address the potential usefulness of other tracers such as 3′-deoxy-3′-18F-fluorothymidine (cell proliferation), O-(2-18F-fluoroethyl)-L-tyrosine (protein translation), 18F-fluoromisonidazole (hypoxia), 18F-arginine-glycine-aspartate (angiogenesis), or 18F-annexin (apoptosis) for nodal staging in OSCC patients.
CONCLUSION
PET findings at the neck lymph nodes showed a limited sensitivity and specificity for primary staging of OSCC patients. However, PET nodal findings have the capacity to improve prognostic stratification for clinical outcomes beyond standard clinical and pathologic risk factors, thus detecting a subgroup of patients with a substantially higher risk. The present study supports the claim that PET at the neck lymph nodes—even without major diagnostic implications for the purpose of primary staging—has clinical validity in the broad sense in OSCC patients without distant metastases. The use of improved prognostic models based on PET findings may also benefit OSCC patients when combined with appropriate risk reduction strategies.
Acknowledgments
This work was supported by grants NMRPG160031 and CMRPG370061 from the Chang Gung Memorial Hospital at Linko.
Footnotes
-
↵* Contributed equally to this work.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication August 18, 2010.
- Accepted for publication October 19, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Positive Clinical Impact of an Additional PET/CT Scan Before Adjuvant Radiotherapy or Concurrent Chemoradiotherapy in Patients with Advanced Oral Cavity Squamous Cell Carcinoma
- Oncologic PET/MRI, Part 1: Tumors of the Brain, Head and Neck, Chest, Abdomen, and Pelvis
- 18F-FDG Metabolic Tumor Volume and Total Glycolytic Activity of Oral Cavity and Oropharyngeal Squamous Cell Cancer: Adding Value to Clinical Staging