


Abstract
Molecular imaging plays a central role in the management of radiation oncology patients. Specific uses of imaging, particularly to plan radiotherapy and assess its efficacy, require an additional level of reproducibility and image quality beyond what is required for diagnostic imaging. Specific requirements include proper patient preparation, adequate technologist training, careful imaging protocol design, reliable scanner technology, reproducible software algorithms, and reliable data analysis methods. As uncertainty in target definition is arguably the greatest challenge facing radiation oncology, the greatest impact that molecular imaging can have may be in the reduction of interobserver variability in target volume delineation and in providing greater conformity between target volume boundaries and true tumor boundaries. Several automatic and semiautomatic contouring methods based on molecular imaging are available but still need sufficient validation to be widely adopted. Biologically conformal radiotherapy (dose painting) based on molecular imaging–assessed tumor heterogeneity is being investigated, but many challenges remain to fully exploring its potential. Molecular imaging also plays increasingly important roles in both early (during treatment) and late (after treatment) response assessment as both a predictive and a prognostic tool. Because of potentially confounding effects of radiation-induced inflammation, treatment response assessment requires careful interpretation. Although molecular imaging is already strongly embedded in radiotherapy, the path to widespread and all-inclusive use is still long. The lack of solid clinical evidence is the main impediment to broader use. Recommendations for practicing physicians are still rather scarce. 18F-FDG PET/CT remains the main molecular imaging modality in radiation oncology applications. Although other molecular imaging options (e.g., proliferation imaging) are becoming more common, their widespread use is limited by lack of tracer availability and inadequate reimbursement models. With the increasing presence of molecular imaging in radiation oncology, special emphasis should be placed on adequate training of radiation oncology personnel to understand the potential, and particularly the limitations, of quantitative molecular imaging applications. Similarly, radiologists and nuclear medicine specialists should be sensitized to the special need of the radiation oncologist in terms of quantification and reproducibility. Furthermore, strong collaboration between radiation oncology, nuclear medicine/radiology, and medical physics teams is necessary, as optimal and safe use of molecular imaging can be ensured only within appropriate interdisciplinary teams.
- PET/CT
- molecular imaging
- quantitative imaging
- radiation therapy
- target definition
- treatment response assessment
Molecular imaging plays a central role in the management of radiation oncology patients. Although most uses and applications of molecular imaging in radiation oncology do not significantly differ from those in general oncology (e.g., diagnostic applications), there are some specific imaging requirements and uses that warrant separate discussion and review, particularly for planning and assessment of radiotherapy (Fig. 1).
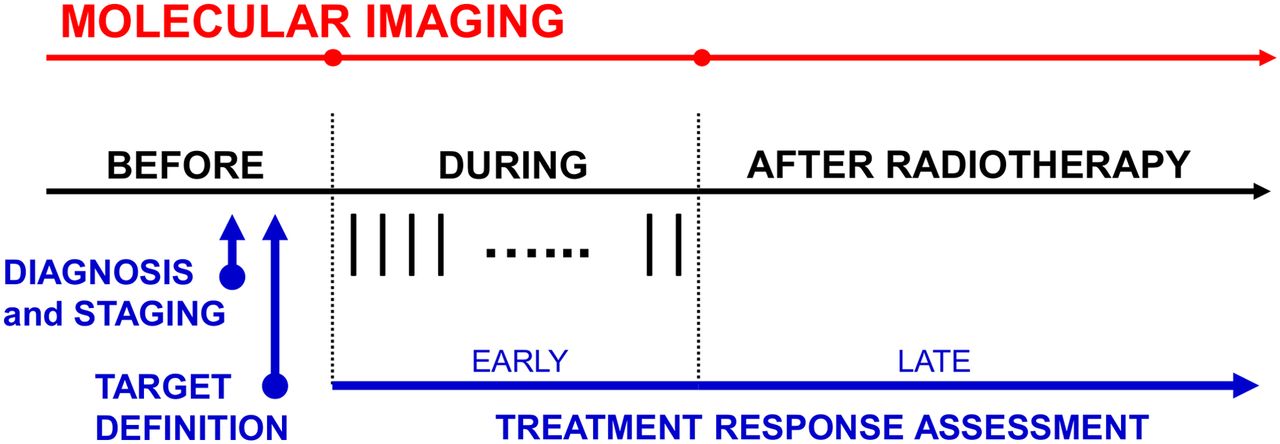
Use of molecular imaging in radiation oncology follows all steps of treatment process but with some specific challenges, particularly for defining treatment targets (e.g., requiring accurate spatial localization) and in treatment response assessment (e.g., requiring special attention to radiation-induced inflammation). Vertical bars during radiotherapy indicate individual treatment fractions.
Radiation therapy is a localized cancer treatment modality and, as such, requires accurate spatial localization of the tumor. Spatial localization has traditionally relied on anatomic imaging methods such as CT and MRI, but the added benefits of molecular imaging (e.g., increased sensitivity and specificity) make molecular imaging, and especially combined modalities such as PET/CT, particularly appealing. However, accurate spatial localization increases the complexity of the imaging procedure. For example, as patient (and tumor) position within the treatment system needs to be maintained during radiotherapy, the scanning position during molecular imaging procedures should be similarly maintained. These extra requirements increase the complexity of the process, not only to acquire molecular images but also to analyze them. With the recent interest in biologically conformal radiotherapy (dose painting), in which one would potentially target a spatially heterogeneous distribution of tumor resistance with variable levels of radiation dose, the requirements for molecular imaging quantification are further augmented.
18F-FDG PET/CT has been the main imaging modality of choice for treatment response assessment. However, because of radiation-induced inflammation, the time points for treatment response assessment need to be carefully selected. Because inflammatory processes initiated during radiation therapy can persist for months after the therapy ends, both late (after treatment) and particularly early (during treatment) response assessment based on 18F-FDG PET/CT requires complex interpretation. Solid tumors that are commonly treated with radiotherapy or chemoradiotherapy show variable resistance to therapy, ranging from very sensitive tumors (e.g., lymphoma, seminoma) to highly resistant tumors (e.g., melanoma and glioblastoma), with most squamous cell carcinomas and adenocarcinomas being in the intermediate zone. For resistant tumors, changes in tumor glucose metabolic activity may be small and occur only late during the course of radiotherapy. Fortunately, several alternative PET radiotracers and different modalities for molecular imaging exist, most notably 3ʹ-18F-fluoro-3ʹ-deoxy-l-thymidine (18F-FLT), a surrogate of tumor proliferation, and various MRI techniques, which are particularly applicable for assessment of brain tumors.
This article provides a comprehensive and contemporary overview of molecular imaging applications in radiation therapy, particularly for target definition and treatment response assessment. Specific quantitative imaging requirements for use in radiation therapy, and potential confounding artifacts that limit image interpretation, will be highlighted. Future perspectives for full exploration of molecular imaging, particularly for biologically conformal applications of radiotherapy, will be discussed.
QUANTITATIVE IMAGING FOR RADIATION THERAPY
Molecular images should be of high quality for effective application in radiotherapy target delineation and treatment response assessment. The quality of molecular images depends on a combination of multiple factors, including patient preparation, technologist training, imaging protocol design, scanner technology, software algorithms, and data analysis methods. Several guidelines are available that provide recommendations on imaging procedures for 18F-FDG (1,2), as well as for other PET radiotracers (3,4). Practice guidelines for certain functional MRI procedures have also been suggested by the American College of Radiology (5). Molecular imaging for radiation therapy applications, however, requires an additional level of reproducibility and image quality beyond what is required for diagnostic imaging. This section will discuss the general steps to acquiring high-quality molecular images for use in radiation therapy planning and treatment response evaluation, with the focus on PET/CT but also briefly discussing other molecular imaging modalities, such as MRI.
Image Acquisition
It is important that patients undergo similar preparations before imaging and before receipt of each fraction of radiation therapy. For example, for abdominal tumors, fasting before imaging and treatment increases the likelihood that the stomach and bowels are the same size during treatment planning as they will be for each treatment session. For 18F-FDG PET imaging, fasting also helps to keep blood glucose levels within acceptable ranges for imaging. Blood glucose levels should be checked before 18F-FDG injection, and the scan should be rescheduled if levels are outside a predetermined range (2).
Molecular imaging for radiation therapy planning requires equipment and procedures additional to those typically used for diagnostic imaging. Unlike diagnostic images, images for radiation therapy planning will eventually need to be coregistered with treatment-planning CT images. Reliable target delineation is contingent on the accuracy of registration between the functional image and the planning CT image. As such, molecular imaging acquisitions for radiation therapy planning need to follow principles similar to those recommended for planning CT (or simulation CT) acquisitions (6).
The patient should be positioned and immobilized during image acquisition in the same manner as during receipt of each fraction of therapy. Because flat-top couches are used for radiation therapy delivery to ensure repeatable positioning, a flat-top table should be placed on top of the patient table. Any immobilization devices, padding, or bolus material should be in place during the scan. For nuclear medicine, placement of positioning equipment outside the transaxial imaging field of view but within the scanner bore should be avoided, as it can lead to attenuation artifacts (7). Scanners with large bores are preferred to accommodate the extra equipment. Positioning for functional MRI can be more challenging, depending on the tumor site (8). For example, for head and neck cancer, personalized masks are often used to ensure reproducible positioning and immobilization, but these masks often do not fit inside standard head coils. Furthermore, MRI bores are often smaller than CT bores, potentially limiting the use of some positioning devices. In these cases, creative solutions may be necessary (9). In addition to the internal positioning lasers included with imaging systems, it is preferable to have mobile external lasers for patient marking/tattooing and positioning, similar to those used during CT simulation. The positioning of the lasers should be precise and maintained at a known spatial relationship to the image center, so that patients can be marked in a way that will ensure repeatable positioning at subsequent treatment sessions. The alignment of the external laser should be tested for accuracy; such quality assurance tests have been described by the American Association of Physicists in Medicine (AAPM) task group 66 (6).
For PET/CT imaging, there are different options for acquiring the CT component of the scan. Attenuation and scatter correction for PET image reconstruction can typically be performed using either low-dose CT or high-quality diagnostic CT. The preference is to acquire a single high-quality CT scan together with the PET scan, which can then be used for treatment planning. In this case, no additional image registration is needed to align the PET image and the planning CT image. Treatment-planning CT, however, is sometimes performed with intravenous contrast material. Unless corrected for, contrast-enhanced CT can cause the PET voxel values in regions of high contrast density to be increased when the scan is used for attenuation correction (10). In these cases (or when the planning CT scan has been acquired separately), an additional low-dose CT scan should be acquired together with the PET scan. This low-dose CT scan can be used for attenuation and scatter correction but is not suitable for treatment planning. If contrast-enhanced CT is to be performed during the PET/CT examination, it should occur after both the attenuation CT and the PET acquisitions. A promising alternative to PET/CT imaging, which will become more prevalent in the future, is PET/MRI, in which pseudo CT images are created and used for PET attenuation correction (11) and potentially also for radiotherapy planning (12). The challenge of pseudo CT generation is that the MRI intensity value of a single voxel cannot be uniquely mapped into the γ-ray attenuation coefficient. Although several methods to improve the accuracy of pseudo CT mapping (e.g., registered atlas CT) have been developed (11), these have yet to be thoroughly validated for use in radiation therapy planning.
Registration
When the planning CT image is not already registered to the functional images, the two image coordinate systems need to be aligned. Rigid registration algorithms rotate and translate two images to maximize the spatial similarity of their intensity values. Most modern image-analysis software packages include methods for performing rigid registration. For PET, the CT image from the PET/CT acquisition is typically registered to the planning CT image, and the resulting spatial transformation is then applied to the respective PET image. Voxel sizes for PET images are larger than CT voxel sizes and, depending on the software, may need to be up-sampled before PET can be used for target delineation. Unless nearest-neighbor resampling is used, this resampling step will alter the quantitative SUVs; therefore, quantitative image analysis for treatment response assessment should be performed before the PET image registration. For functional MRI, anatomic MRI sequences such as volumetric T1-weighted imaging should also be acquired during imaging so that MRI and CT images can be coregistered. Special software may be required to register anatomic MRI and CT images, as the imaging values for different tissues are inherently different between the two imaging modalities.
In many cases, patient positioning will not be identical in the molecular images and in the planning CT image. This issue can make rigid registration difficult and can occasionally cause algorithms to converge to strange solutions (results should always be checked). One option, if the software allows it, is to crop the template image, leaving only the regions of interest to be registered. Another option is to use deformable registration algorithms. Like rigid registration, deformable registration algorithms maximize the similarities between two images but allow for morphologic changes beyond rotation and translation. These algorithms ultimately warp the template image to match the reference image. There are several deformable registration algorithms, each with different similarity measures or regularization constraints. Because the resulting solution will differ depending on the algorithm used, an algorithm should not be arbitrarily chosen (13). Quality assurance processes for image registration have been proposed (14), and an upcoming report from task group 132 of the AAPM will further describe the proper use and quality assurance of image registration algorithms.
Motion
Patient motion during imaging causes the image to be blurred over the path of motion, elongating target volumes. Motion also affects image quantification, effectively reducing image intensity values (15). Certain motions, such as breathing, cannot be avoided during treatment and will affect imaging of the lungs, liver, esophagus, pancreas, breast, prostate, kidneys, and other organs. Lung motion amplitudes are case-dependent but usually range between 0 and 30 mm in the superior–inferior direction, with an average of around 10 mm (16).
The degree to which motion should be compensated for during imaging depends on the degree to which motion will be accounted for during treatment. In other words, motion management for imaging should be coupled to motion management strategies during radiation delivery. In the case of PET, the simplest strategy would be to apply no motion correction to PET images, as both PET imaging and radiation therapy delivery encompass all phases of respiratory motion. Likewise, slow CT imaging can be used to create a phase-averaged CT image (17). Not accounting for motion during planning and radiation therapy delivery, however, can result in an unnecessary dose to nearby healthy organs.
There are several methods to reduce or account for respiratory motion during imaging and radiation therapy delivery. A detailed description of these methods is beyond the scope of this review but has been published elsewhere (16). These methods include shallow or tidal breathing to limit motion amplitude, respiratory gating (16,18), and real-time tumor tracking (19,20). In any case, the type of image acquisition should be closely matched to the type of radiation treatment delivery (e.g., 4-dimensional [4D] PET/CT together with real-time radiation delivery tracking).
Uncertainties
Uncertainties in molecular imaging arise from technical factors (e.g., scanner calibration), physical factors (e.g., positron range), biologic factors (e.g., patient metabolism), and analytic factors (e.g., inconsistent image processing) (21,22). Some of these uncertainties can be controlled or minimized through careful study design and quality assurance procedures (Table 1 provides examples specific to 18F-FDG PET). Understanding the limitations and uncertainties of molecular imaging is necessary to its proper implementation in radiation oncology.
Uncertainties and Quality Control Measures for PET/CT in Radiation Therapy Planning
For PET imaging, one limitation is its spatial resolution. There are many factors that affect PET spatial resolution, but in general, PET-avid lesions with diameters less than 5–10 mm are unlikely to be discernible from background in a typical clinical PET image (23). Consequently, small lesions, some positive lymph nodes, sharp intratumor heterogeneities, and microscopic tumor extensions may not be resolved in a PET image. The limited spatial resolution of PET has implications for its use in target volume delineation and treatment response assessment.
Uncertainties in molecular image quantification will propagate into uncertainties in treatment response assessment. Quantitative imaging for treatment response assessment requires proper calibration of the scanner equipment (including the dose calibrator for nuclear medicine) at acceptance testing and during routine maintenance. A detailed quality assurance plan, including daily, quarterly, and annual calibrations, is necessary to ensure the reliability and consistency of the scanner equipment (24,25). For MRI, quality assurance procedures that minimize geometric distortion caused by gradient field nonlinearity or static field inhomogeneity are especially important. Even with properly calibrated equipment, however, biologic variability and statistical noise cause substantial uncertainties in molecular imaging. For example, test–retest studies with 18F-FDG PET imaging suggest that biologic and statistical uncertainties contribute to an overall uncertainty (coefficient of variation) in SUVmax of about 10%–15% (26,27). Even the position of a lesion relative to the detector array geometry can cause fluctuations in PET SUV for small lesions (28).
There are also uncertainties on how to best extract meaningful quantitative imaging biomarkers from molecular images. In PET, the semiquantitative SUV is easily calculated by normalizing the measured radioactivity concentration in an image voxel by the ratio of the patient’s injected activity to body weight—either total body weight or lean body mass. Both the SUVmean and the SUVmax of a region of interest are typically reported. However, depending on the application and radiotracer used, SUV may not represent a reliable measure of the biologic process of interest and can be very sensitive to the conditions of the acquisition, reconstruction, and analysis. In these cases, dynamic imaging with kinetic analysis may be necessary to understand the tracer kinetics and extract the most biologically relevant parameters. Dynamic scans are much more challenging to perform and analyze than static scans.
In MRI, similar challenges in image quantification exist. For example, it is becoming increasingly common for apparent diffusion coefficient (ADC) from diffusion-weighted (DW) MRI to be measured in clinical examinations, but standardized protocols for acquisition and analysis of DW MR images are lacking, especially across vendors (29). This lack of standardization also applies to perfusion MRI, which models and calculates kinetic parameters relating to blood flow. Standards for appropriate uses and analyses of quantitative imaging biomarkers, including proper characterization of their uncertainties, are being developed by the Quantitative Imaging Biomarkers Alliance (30).
Quantitative PET image values are highly sensitive to the algorithm used to reconstruct the images (31). With iterative reconstruction algorithms (which have become standard in clinical PET imaging) and a growing library of image correction methods (e.g., point-spread-function modeling), there are hundreds of possible combinations of reconstruction parameters. Furthermore, the optimal reconstruction method may depend on the region of interest (e.g., chest vs. brain). It is therefore incumbent on an institution’s nuclear medicine physicians, physicists, or technologists to determine the reconstruction method that optimizes image quality for a particular PET scanner. This generally involves scanning a PET image-quality phantom, exploring several different reconstructions, and finding the set of parameters that offers the best trade-off between spatial resolution and image noise. Furthermore, as different PET scanners can have substantial differences in image quality and quantitative accuracy, image reconstruction parameters can be tuned such that the different PET scanners involved in a multicenter study produce comparable image quality. This process of scanner harmonization can improve the statistical power of multicenter clinical trials investigating imaging biomarkers (32).
Overall, many uncertainties in molecular imaging and in its application to radiation oncology can be minimized using a detailed and unambiguous protocol for acquisition and image analysis. One such protocol is the 18F-FDG PET imaging protocol developed by the Uniform Protocols for Imaging in Clinical Trials working group (33). Strict adherence to protocols ensures that for baseline and follow-up imaging, identical procedures will be followed for patient preparation, patient immobilization, radiotracer or contrast injection, acquisition settings, image reconstruction/corrections, image processing, and image analysis. Minimizing these quantitative imaging uncertainties will allow for more precise quantification of treatment response (34).
MOLECULAR IMAGING FOR TARGET DEFINITION
Uncertainty in target definition is arguably the greatest challenge facing radiation oncology. Recent technologic advances in radiation delivery and dosimetry allow for precise and conformal delivery of dose to patients. Exactly where that dose should be delivered, on the other hand, is still not clear. The impact that uncertainty in target volume delineation has on patient dosimetry is almost an order of magnitude greater than the impact of tumor motion (16,35). Perhaps the greatest impact that molecular imaging can have in radiation oncology is in reducing interobserver variability in target volume delineation and in bringing about greater conformity between target volume boundaries and true tumor boundaries. An upcoming report from task group 211 of the AAPM will further describe the proper use of 18F-FDG PET/CT for target definition.
Manual Tumor Segmentation
Currently, the most common method for molecular imaging–based gross tumor volume delineation is manual segmentation. A prerequisite for all molecular imaging–based segmentation methods is an understanding of the normal biologic processes that will be measured in the images, so that normal tissue is not mistaken for diseased tissue during segmentation. Potential sources of false-positives and false-negatives should be well understood. For example, in the case of 18F-FDG PET, brown adipose tissue, granulous tissue, areas of inflammation, and muscle often have elevated levels of uptake and can be mistaken for tumor (1,36). PET images should be interpreted by nuclear medicine physicians and MR images by radiologists before being used for radiation therapy purposes so that, if necessary, previously unknown lesions can be detected and potential image artifacts can be identified.
After image registration, the molecular and the anatomic images should be fused by the visualization software (37). All available information should be used for defining the target volume. Manual segmentation methods, however, are known to suffer from inter- and intraobserver variability in target volume delineation. To reduce this variability, it is recommended that institutions develop a strict delineation protocol that describes exactly how the tumor should be visualized (e.g., window level and color settings) and details any other parameters that can affect the physician’s choice of contouring (38). Because of the significant inter- and intraobserver variability, manual segmentation is generally inferior to automatic and semiautomatic segmentation and as such is discouraged. However, it will take some time for the manual segmentation to be entirely replaced by automatic and semiautomatic segmentation tools, which still require more rigorous clinical validation.
If DW MRI is used for tumor segmentation, special attention should be paid to the potential for spatial distortions in the ADC maps. Studies have found that substantial geometric distortions can occur in DW MR images, even on the order of centimeters (39). Such distortions, both global and local, can also occur for other imaging sequences, including sequences used for perfusion MRI. If not accounted for, these distortions can substantially affect the accuracy of the target volume delineation.
Automatic and Semiautomatic Tumor Segmentation
Computer algorithms that automate tumor volume segmentation based on molecular images can improve workflow and reduce physician variability in target definition. In PET, the most common method for automatic segmentation is thresholding based on SUV. There are different ways by which thresholding can be performed. A threshold based on SUVmax is the most commonly used method and usually the most simple. The threshold value for 18F-FDG PET is often set at around 40% of SUVmax but varies from 20% to 50%. Other types of thresholding include using a fixed SUV threshold (e.g., SUV ≥ 2.5 (40)) or using a background-subtracted threshold (41). A clear disadvantage of thresholding is the uncertainty about which threshold is optimal, which can vary depending on the scanner hardware, reconstruction and acquisition parameters, presence of motion, tumor size, and patient biology (42). Furthermore, thresholding cannot distinguish normal uptake from disease, and results will need to be corrected manually, preferably by an experienced nuclear medicine physician.
Numerous advanced automatic and semiautomatic PET segmentation algorithms have been developed (43,44). Broadly, these can be categorized as iterative/adaptive methods, statistical modeling methods, machine learning–based methods, and image filter–based methods (e.g., using gradients or texture features). Currently, it remains unclear which methods perform best and how best to assess the performance of different algorithms. Various performance evaluation methods have been developed for testing segmentation algorithms (44,45). It is recommended that institutions thoroughly evaluate segmentation algorithms, including any tuning parameters, and benchmark their performance against both phantom and clinical images before clinical implementation. Even when automatic and semiautomatic tools are used, manual review of the contours is highly recommended.
For brain tumor segmentation, the utility of 18F-FDG PET is limited by high background levels of 18F-FDG uptake in healthy brain tissue. Other radiotracers have been shown to perform better in the identification and delineation of brain tumors. For example, the amino acid radiotracers O-(2-18F-fluoroethyl)-l-tyrosine and l-[methyl-11C]-methionine are taken up by cancer cells because of overexpression of amino acid transporters (46,47). 3,4-dihydroxy-6-18F-fluoro-l-phenylalanine (18F-DOPA) is another amino acid PET radiotracer that has produced promising results (48). MRI, however, remains the standard for delineation of most brain tumors. Other tumor sites may also benefit from the use of nonstandard PET radiotracers for target definition, such as 16α-18F-fluoro-17β-estradiol in breast cancer, and somatostatin-analogs DOTATOC and DOTATATE for neuroendocrine tumors.
Nodal Involvement
The ability of PET imaging to detect involved lymph nodes that appear benign on CT images has been demonstrated (49). However, its improvement over CT imaging for nodal detection is dependent on the tumor site. A series of review papers has been published on PET for radiation treatment planning for various tumor sites, including the brain (50), head and neck (51), lung (52), gastrointestinal tract (53), prostate (54), and cervix/endometrium (55). For some situations, such as mediastinal lymph node staging for lung cancer, the sensitivity of 18F-FDG PET/CT appears to be superior to CT alone at detecting involved lymph nodes (52). In others, such as colorectal cancer, PET does not perform as well (56). It remains to be seen whether PET/MRI scanners will improve nodal detection, particularly in some anatomic sites such as the abdomen.
Tumor Boosting
One appealing future application of molecular imaging in radiation therapy planning is in the delineation of biologic tumor subvolumes for dose escalation. This method has been termed biologically conformal radiation therapy, or dose painting (57). The rationale for dose painting comes from the fact that tumors are biologically heterogeneous in composition and often show nonuniform patterns of response to radiation therapy (58,59). Molecular imaging may be able to identify spatial patterns of radioresistance, which can be used to guide and shape the dose distribution. Indirect evidence of this principle comes from studies that have found molecular imaging biomarkers to correlate with patient outcome after radiation therapy (60,61). Possible biologic targets include tumor hypoxia (measured with PET hypoxia radiotracers or with dynamic contrast-enhanced [DCE] MRI), cellularity (measured with 18F-FDG PET or DW MRI), and others. Identifying effective and robust imaging-based targets for dose painting is currently an ongoing research problem (61,62). Dose painting can be applied either on a region-of-interest level (dose painting by contours) or on a voxel level (dose painting by numbers), in which each tumor voxel receives a unique dose prescription proportional to the voxel’s image intensity value (63). Studies have demonstrated the feasibility of creating and delivering dose-painting plans—both subvolume boosting and voxel-based dose painting—using existing clinical software and therapy systems (64).
Dose painting has yet to be validated as an effective treatment option, but clinical studies have begun to investigate the efficacy of dose painting. Studies have been performed on the brain using 18F-FDG (65) and O-(2-18F-fluoroethyl)-l-tyrosine PET (66), on head-and-neck tumors using 18F-FDG PET (67–69), on prostate tumors using 18F-fluorocholine PET (70), and on lung tumors using 18F-FDG PET (71). Further clinical studies are ongoing.
Normal-Tissue Sensitivity
The potential for using molecular imaging to discriminate radiosensitive tissue from radioresistant tissue in tumors may be equally valuable when applied to the surrounding normal tissue. Certain regions in an organ, particularly the lung, appear to be more sensitive to radiation therapy than other regions in the same organ. Or some regions may be more functional than other regions and therefore more important to spare. For example, in 18F-FDG PET imaging of the lungs, studies have found that regions of uptake before radiation therapy are more likely to experience radiation-induced toxicity after radiation therapy (72). Ventilation imaging may identity lung regions that are blocked—either by obstructive lung disease or by tumor burden—and may contribute less to overall lung function than healthy, functioning lung. Information on functional lung can be acquired through a variety of imaging methods. For MRI, hyperpolarized gases or gadolinium aerosol can be used in combination with serial imaging to produce 4D images of lung ventilation (73). Ventilation maps can also be derived from 4D CT imaging, in which voxel Hounsfield units correlate with the fraction of air in the voxel volume (74). In SPECT, 99mTc-labeled macroaggregated albumin can also be used to create 3D ventilation maps (75). The feasibility of incorporating lung ventilation maps into treatment planning for conformal avoidance has been demonstrated (76). Although promising, the clinical benefit of using functional lung images for conformal avoidance has yet to be validated.
Overall, there are many potential uses of molecular imaging in target definition for radiation therapy. The various methods by which molecular imaging can be used for target definition and their respective degrees of complexity are outlined in Table 2. Considering the extensive ongoing clinical research and continuous technologic advances, it is likely that the methods presently considered to be advanced will soon become routine practice.
Methods to Incorporate Molecular Images into Radiation Therapy Planning and Their Respective Degrees of Complexity
MOLECULAR IMAGING FOR TREATMENT RESPONSE ASSESSMENT
In radiation oncology, the time point at which treatment response is assessed will depend on the purpose of the assessment (Fig. 1). Early assessment—during the course of radiotherapy—serves as an early predictor of treatment outcome and potentially allows the therapy to be adapted in order to maximize its benefit. Late assessment—after the radiotherapy has been completed—serves as a late predictor of treatment outcome in order to guide patient care after radiotherapy. Anatomic changes visible on CT or MRI, which have traditionally been used to assess treatment response, typically occur slowly over the course of weeks and months after the therapy (77), whereas with molecular imaging treatment response can potentially be assessed much earlier.
The potential of using changes in SUV on 18F-FDG PET to assess treatment response earlier was recognized by the European Organization for Research and Treatment of Cancer in its recommendations (78). Later, frameworks for PET-based therapy response evaluation were drafted by the National Cancer Institute (79) and Wahl et al., ultimately resulting in the PET Response Criteria in Solid Tumors (PERCIST) (80). Initially, 18F-FDG PET–based therapy response assessment was used for only chemotherapy. A limitation of 18F-FDG PET–based therapy response assessment in radiation oncology is the high 18F-FDG avidity of normal tissue surrounding the tumor because of inflammation, which builds up late during or early after the completion of radiotherapy. In contrast to inflammatory changes in normal tissue, metabolic activity in tumors decreases progressively during radiotherapy, leading to a relatively narrow window of opportunity to extract information from molecular imaging—when there are still enough viable tumor cells but before the surrounding inflammatory changes start to dominate (typically within the first 2–3 wk).
The problem of inflammatory changes in normal tissue during and after radiotherapy, which hinders early 18F-FDG PET/CT–based assessment of radiotherapy response, is obviously 18F-FDG–specific. Other types of molecular imaging techniques, such as PET/CT with other radiotracers (e.g., 18F-FLT) or various MRI techniques, typically avoid this problem. However, 18F-FDG PET/CT is by far the most established molecular imaging technique, as is evident from their being no similar response assessment guidelines established yet for other types of molecular imaging techniques.
Prognostic Role of Molecular Imaging in Radiation Therapy
High clinical availability and wide applicability are why 18F-FDG PET/CT is most commonly investigated as a prognostic and predictive imaging biomarker in radiation oncology. Relative changes in 18F-FDG SUVs are commonly investigated for being representative of clinical response, as suggested in the guidelines of the European Organization for Research and Treatment of Cancer and the National Cancer Institute, as well as PERCIST, for the measurement of treatment response (78–80). These guidelines also provide criteria for classifying patients into various response categories (complete response, partial response, stable disease, progressive disease). The response thresholds have not been generally validated in larger clinical trials and therefore serve mostly as recommended guidelines for standardized reporting. In addition, 18F-FDG PET/CT–based therapy response assessment requires proper selection and control of some factors that are highly important for therapy response assessment. One of them is the timing of sequential 18F-FDG PET/CT imaging for response assessment. Because of the dynamic nature of inflammatory and tumor-response processes, the timing of imaging relative to the treatment schedule has a profound effect on how early it is possible to assess treatment response. Some key studies representing the current evidence for various tumor types are highlighted as follows.
Lung Cancer
In lung cancer, clinical outcome has been correlated with the metabolic tumor response rate assessed after the end of radiotherapy. For example, overall survival at 9 mo in 102 patients with non–small cell lung cancer (NSCLC) of various stages has been correlated with the metabolic tumor response rate assessed 70 d after the end of radiotherapy (81). Furthermore, various small clinical studies have demonstrated that 18F-FDG PET/CT imaging during the course of radiotherapy can predict late metabolic response or clinical outcome in NSCLC patients (82,83). Timing in sequential 18F-FDG PET imaging for early response assessment is extremely important, as has been clearly demonstrated by van Baardwijk et al., who have shown that 18F-FDG PET SUVmax in nonresponding NSCLC patients increased in the first week of radiotherapy and then decreased in the second week of radiotherapy and after radiotherapy (84). In contrast, changes in SUVmax for responding patients were negligible during radiotherapy and notably negative after radiotherapy. 18F-FDG uptake and functional volume for both primary tumors and lymph nodes in NSCLC generally decrease during the course of radiotherapy, roughly linearly with time or dose, suggesting that 18F-FDG PET/CT images can be acquired during radiotherapy without artifacts that hamper image interpretation and quantification (85).
Head and Neck Cancer
In head and neck cancer, the first initiative to assess response after radiotherapy with 18F-FDG PET/CT dates back almost 3 decades (86). Currently, 18F-FDG PET/CT is widely accepted for assessing response after radiotherapy or chemoradiotherapy, with imaging typically performed 3–6 mo after completion of radiotherapy (87–89). Reports on using 18F-FDG for early response assessment during radiotherapy or chemoradiotherapy are much less frequent than reports on late 18F-FDG PET/CT–based response assessment. Generally, reports on early assessment agree that 18F-FDG PET/CT during chemoradiotherapy may help differentiate responders from nonresponders, but these results are not yet reliable enough to replace posttherapy 18F-FDG PET/CT evaluation (90).
Rectal Cancer
In rectal cancer, the most common therapy for early and locally advanced stages is radical surgery, which is usually preceded by preoperative radiotherapy or chemoradiotherapy. The surgical approach depends heavily on assessing the success of preoperative chemoradiotherapy. It has been shown that pathologic response to preoperative chemoradiotherapy can be reliably evaluated by 18F-FDG PET/CT during chemoradiotherapy (91). Similarly, when 18F-FDG PET/CT is performed early, between 1 and 2 wk after the onset of preoperative chemoradiotherapy, it has been shown to be highly accurate in predicting response in patients with locally advanced rectal cancer (92). In addition, posttherapeutic response assessment with 18F-FDG PET has also been thoroughly studied (93).
Esophageal Cancer
Late response assessment with 18F-FDG PET/CT during neoadjuvant treatment is suggested to be a significant prognostic predictor of disease-free and overall survival in locally advanced esophageal and esophagogastric junction cancer (94). Early response assessment with 18F-FDG PET/CT is not considered a reliable prognostic predictor in esophageal cancer (95).
Cervical Cancer
In locally advanced cervical cancer, the generally accepted method of response assessment is 18F-FDG PET/CT 3 mo after the completion of concurrent chemoradiotherapy; reliable long-term prognostic information can be obtained (96). Despite the high predictive value of 18F-FDG PET/CT–based response assessment, relapses remain problematic. Therefore, other disease characteristics such as bulky tumors (>5 cm), high stage (>IIB), or pelvic or paraaortic lymph node metastasis can be used to direct more aggressive treatment or adjuvant chemotherapy regimens (97). In cervical cancer, apart from being used for posttherapeutic response assessment, 18F-FDG PET/CT has been investigated for monitoring of response during radiotherapy. Despite some promising results, future clinical trials are warranted (98).
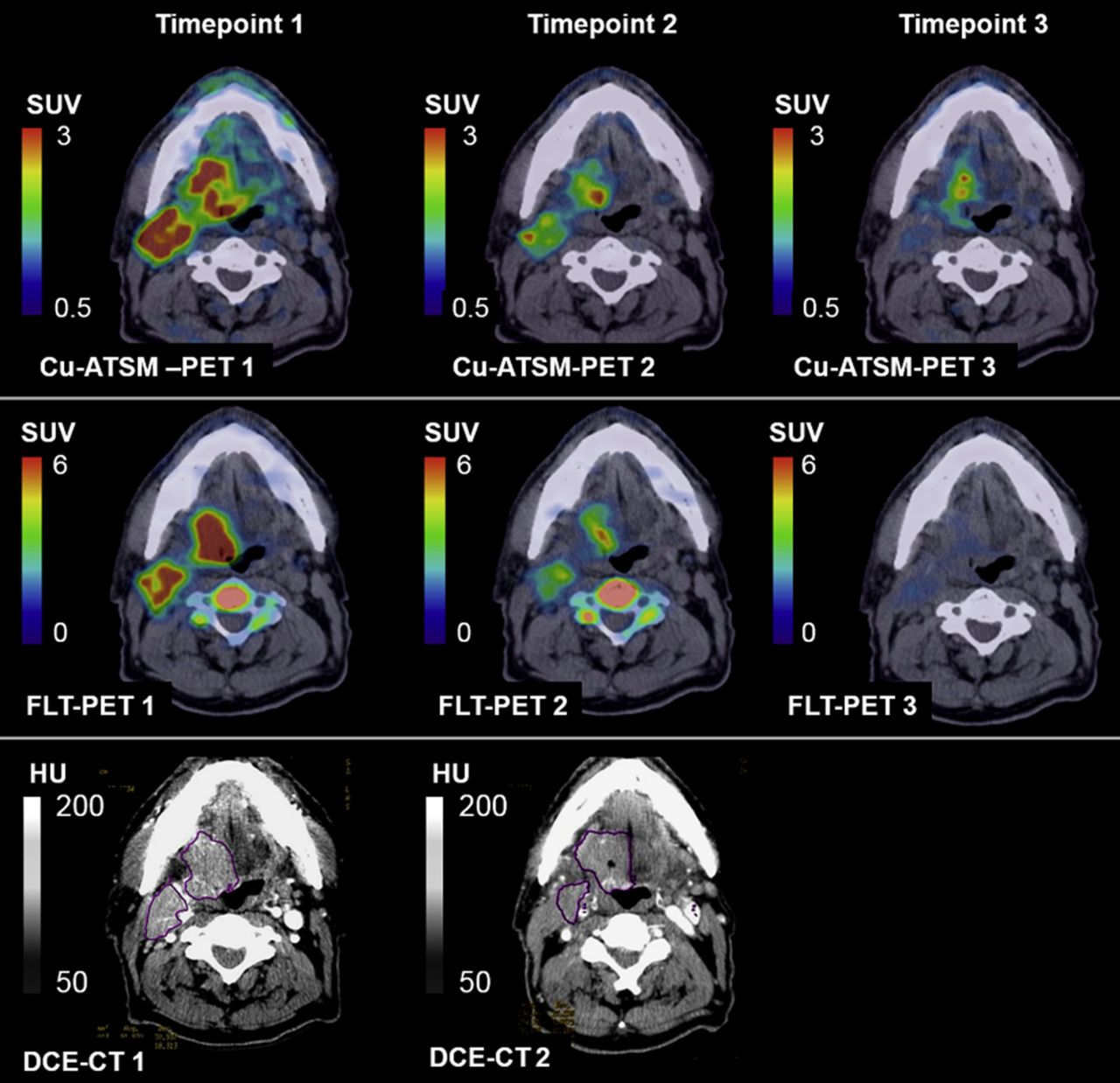
Although some limitations of 18F-FDG PET/CT–based therapy response assessment in radiation oncology can be overcome by careful design and implementation of imaging protocols, the inherent limitation caused by radiation-induced inflammation makes interpretation of treatment-response results difficult. To overcome this limitation, the focus of PET imaging is shifting to more tumor-specific characteristics (e.g., cellular proliferation, hypoxia, angiogenesis, and apoptosis). Currently, the most established of these is imaging of cellular proliferation using 18F-FLT PET, a surrogate of cellular proliferation. The characteristics of 18F-FLT make it suitable for static PET imaging, with a reasonable uptake period and dynamic PET imaging that can be subsequently analyzed for kinetics (99,100). The potential of 18F-FLT PET/CT for early assessment of chemotherapy has been demonstrated in a variety of cancers (101–103). In the context of radiotherapy, 18F-FLT PET/CT first proved its sensitivity to ionizing radiation in preclinical tumor models (104,105). After promising results from 18F-FLT PET/CT–based assessments of radiation response in these models, an increasing number of studies have shown that decreased 18F-FLT uptake early (as early as 5 d/10 Gy) in the course of radiotherapy or chemoradiotherapy is a strong indicator of long-term outcome in a large-animal preclinical model (106) and humans (107–110) (Fig. 2). Although the data on 18F-FLT PET/CT response assessment in radiation therapy are still emerging, its potential is indisputable, and it should be considered an alternative to 18F-FDG PET/CT. One alternative PET surrogate marker of cellular proliferation is 11C- and 18F-choline, which appears relatively sensitive for detecting recurring prostate cancer (111). Another is l-[methyl-11C]-methionine, which may be useful for late response evaluation in brain cancer (112).

Multimodality multitracer molecular images of 61Cu-diacetyl-bis(N4-methylthiosemicarbazone) (Cu-ATSM) PET, 18F-fluorothymidine (FLT) PET, and DCE CT in patient before bevacizumab monotherapy (time point 1), after 3 wk of bevacizumab (time point 2), and after 1–2 wk of chemoradiation therapy (time point 3), indicating potential of molecular imaging to assess complex radiation treatment regimens. (Reprinted with permission of (116).)
Apart from cellular proliferation imaging, hypoxia is another tumor-specific characteristic that has been successfully imaged and used for radiotherapy response assessment in clinical studies. Although tumor hypoxia is widely recognized as a negative prognostic factor in radiation oncology, hypoxic tumor subvolumes often change during radiotherapy (113,114). Treatment outcome may correlate more with hypoxia assessed during radiotherapy than before radiotherapy (115) (Fig. 2 (116)).
Similar to PET-based radiotherapy response assessment, SPECT imaging with 99mTc-HL91 radiotracer allows for detection of tumor hypoxia and has significant predictive power for tumor response and patient survival (117). SPECT imaging with the 99mTc-hydrazinonicotinamide-rh-annexin V radiotracer also allows for evaluating apoptosis in tumors. Apoptotic SPECT imaging has shown radiation dose–dependent uptake in the parotid glands within 2 d after the first course of chemoradiotherapy (6–8 Gy) in head and neck cancer patients; such uptake was indicative of early apoptosis during radiotherapy (118).
In addition to nuclear medicine molecular imaging techniques, MR-based molecular imaging has long been investigated for early radiotherapy response assessment. Research has focused primarily on DCE and DW MRI. For example, increased perfusion early during the course of radiotherapy (within the first 2 wk) assessed with DCE MRI has been shown to be a strong predictor of tumor regression and local control in cervical cancer treated with conventional radiotherapy (119). Also, pretherapy DCE MRI perfusion, permeability, or blood volume measurements have been associated with radiation treatment response in rectal cancers (120) and brain cancers (121). Water diffusion in the tissue can be assessed with DW MRI through the ADCs. Low ADCs measured before radiotherapy have been shown to be associated with response to radiotherapy for brain lesions (122), cervical cancer (123), and head and neck cancer (124). Similarly, increases in ADCs measured during radiotherapy in patients with brain (122), cervical (123), liver (125), rectal (126), and head and neck cancer (124) have been shown to be associated with a favorable outcome. Obstacles toward more successful use of DCE or DW MRI for treatment response assessment includes the unknown optimal timing of DCE MRI (which is most likely disease-dependent (127)), and the lack of reproducibility in ADCs between vendors and institutions (128).
Spatially Resolved Treatment Response Evaluation
Solid cancers have intrinsic spatial heterogeneity in biologic characteristics, which limits the efficacy of point measurements such as biopsy-based molecular assays or point measures derived from PET images (e.g., SUVmax). Methods to incorporate spatial heterogeneities into treatment response assessment are an active area of research. An obvious approach to incorporate the intratumoral heterogeneity into treatment response would be to evaluate spatial therapeutic response. Therapeutic response can be evaluated at a voxel level as absolute change in the PET values (129,130) or as relative change from the baseline image (131). Evaluation of relative changes on a voxel level is unreliable for tumor subvolumes with a very low baseline PET value, for which relative changes may be high despite both baseline and posttherapy PET image values within the background range. Evaluation of absolute change in PET values on a voxel level (129,130) might be less sensitive to cases of very low baseline PET values. An evaluation of the therapeutic response on a voxel level is also strongly affected by the selection of registration algorithm (131).
Intratumoral heterogeneity can also be incorporated into treatment response assessment by the extraction of various textural features from molecular images (popularly termed radiomics). These features are subsequently used for therapy response assessment instead of or in addition to point SUV measures (i.e., SUVpeak and SUVmax) or overall SUV measures (i.e., SUVmean and SUVtotal). Although the use of texture analysis in molecular imaging is still in its infancy, some successful applications in radiation oncology have already been published. Various textural features that were extracted from pretreatment 18F-FDG PET images have been correlated to treatment outcome in breast, cervix, esophageal, head and neck, and lung cancer tumors (132). Changes in textural features of 18F-FDG PET images during and after chemoradiotherapy have also been significantly correlated to time to progression and survival in rectal cancer patients (133).
A common technical limitation of all approaches for incorporating intratumoral heterogeneity into treatment response assessment is the influence of image acquisition and reconstruction parameters on image heterogeneity measures. Image acquisition and reconstruction intrinsically implement some smoothing and possibly other distortions of the data, in comparison to the real data, the degree of which depends on the imaging hardware and software, and also on the acquisition and reconstruction settings. Therefore, sequential imaging for voxel-based treatment response assessment and for extraction of imaging features would have to be performed on the same scanner with the same acquisition and reconstruction settings. Alternatively, different scanners could produce comparable results if they were carefully harmonized. However, interchangeability of textural features from different but carefully harmonized PET/CT scanners has yet to be proved.
Adaptation
The main goal of early molecular-imaging response assessment during radiation therapy is to allow therapy to be modified to improve the clinical outcome—the so-called biologically adaptive radiotherapy. The radiation is adapted during therapy to match corresponding changes in tumor physiology as derived from molecular imaging. Modeling studies have demonstrated potential for significant improvement of clinical outcome using biologically adaptive radiotherapy (134), whereas the clinical evidence has yet to be provided.
Although 18F-FDG PET/CT is the molecular imaging technique with the highest clinical acceptance and availability (68,135), treatment adaption based on 18F-FDG PET/CT is hampered by the inflammatory signal after radiotherapy. The potential use of 18F-FDG PET/CT for adaptive tumor dose escalation or normal-tissue sparing has been investigated in patients with NSCLC (135) and even coupled with dose painting in patients with head and neck cancer (68). Both studies found significant changes in target volumes based on mid-therapy 18F-FDG PET/CT images, warranting replanning of the treatment target.
In addition to 18F-FDG PET, more specific (e.g., cellular proliferation, hypoxia) imaging biomarkers can be used for radiotherapy adaption. As a rapid decrease in 18F-FLT uptake has been demonstrated as early as 5 d/10 Gy in the course of radiotherapy (107–110), early radiotherapy adaption based on 18F-FLT PET/CT imaging appears particularly attractive. The clinical utility of early radiotherapy adaption based on 18F-FLT PET/CT has yet to be demonstrated.
Normal-Tissue Response Evaluation
The main application of molecular imaging for normal-tissue response evaluation is the detection of radiation-induced injuries to these tissues. Monitoring induction, resolution, and mitigation of radiation-induced toxicity is essential in the development of clinically successful strategies to preserve normal tissues. Molecular imaging can be particularly useful to study and monitor these changes.
Lung Cancer
In lung cancer, normal-tissue response assessment has focused mainly on detection of radiation-induced lung toxicity and inflammation. The mainstay of imaging for detection of radiation-induced lung toxicity remains SPECT perfusion and ventilation for evaluating pulmonary function (75,136–138). 18F-FDG PET and DCE MRI have also been investigated for imaging radiation-induced lung toxicity (137,138). The functional relationship between posttherapy 18F-FDG uptake and radiation dose has been measured and shown to correlate with the clinical symptoms of radiation pneumonitis after thoracic radiotherapy (139). The intensity of posttherapy 18F-FDG uptake was related to the severity of radiation pneumonitis using a simple visual scoring system (140). Similarly, increased 18F-FDG uptake in normal lung was associated with the subsequent development of clinical radiation-induced lung toxicity early during radiotherapy (141).
Head and Neck Cancer
In head and neck cancer, xerostomia is the most common major normal-tissue complication after radiation therapy. Decreased parotid uptake of 18F-FDG on postradiotherapy PET/CT images has been associated with early parotid toxicity as defined by posttreatment salivary output and xerostomia scores. Interestingly, pretreatment 18F-FDG PET/CT in conjunction with the radiation dose distribution can predict changes in parotid 18F-FDG uptake, which can potentially be exploited to guide function-sparing treatment planning (142). Besides being studied with 18F-FDG PET, salivary gland function has been studied with l-[methyl-11C]-methionine PET, 99mTc-pertechnetate SPECT, and functional MRI (138).
Esophageal Cancer
In esophageal cancer, research has focused primarily on assessing the myocardium for radiation-induced damage. Focally increased 18F-FDG uptake in the basal myocardium after radiotherapy has been hypothesized to be related to radiation-induced myocardial damage. Therefore, cardiac function and other symptoms should be followed carefully in patients with elevated 18F-FDG uptake in the myocardium (143).
Cervical Cancer
In cervical cancer, pelvic bone marrow irradiation during radiotherapy causes hematologic toxicity, which can be more severe in the case of concomitant chemotherapy. Generally, bone marrow activity can be measured by several imaging modalities, such as CT, MRI, and PET. Imaging with 18F-FDG PET or 18F-FLT PET has been shown to help differentiate active from nonactive bone marrow in cervical cancer patients who have undergone chemoradiotherapy (144,145).
Brain Tumors
In brain tumors, distinguishing tumor growth from radiation-induced injury is often challenging, as both are often visible on posttherapy molecular images. 18F-FDG and 18F-FLT PET imaging have shown promise in the differentiation of recurrent glioma from radiation necrosis through both quantitative and visual image assessment (146). Similarly, 18F-FDG PET/CT and dynamic susceptibility-weighted contrast-enhanced perfusion MRI have demonstrated the ability to differentiate tumor growth from radiation injury (147). 18F-DOPA PET has also been shown to effectively differentiate recurrent or progressive brain metastases from late or delayed radiation injury (148). In addition, radiation-induced brain injury can be assessed with various other MRI techniques (136).
Liver Cancer
In liver cancer, the liver is the most important organ at risk; information on the spatial distribution of liver function is therefore highly valuable for assessing radiation-induced liver toxicity. DCE CT is the current mainstay of liver function spatial assessment; MRI and PET/CT have been studied but to only a limited extent (138).
Several specific challenges in molecular imaging of normal-tissue effects remain. For example, radiation therapy is often combined with chemotherapy and molecularly targeted therapies, with normal-tissue toxicity resulting either from each modality separately or through a synergistic effect of combined therapies. Furthermore, potential inhibition of the inflammatory effects with antiinflammatory compounds (e.g., inhibitors of nuclear factor κB and interleukin-1 signaling) may significantly affect management of radiation-induced toxicity. Much work still needs to be done in the development of relevant molecular imaging agents to effectively probe these processes and fully explore the potential that molecular imaging offers.
IMPEDIMENTS TO BROADER USE
Overall, molecular imaging has many potential uses in assessing response to radiation therapy and in evaluating radiation-induced injury. Various initiatives to use molecular imaging for early response assessment, treatment adaption, late response assessment, and normal-tissue response evaluation in radiation oncology are outlined in Table 3. In the context of the increasing trend toward personalization of therapies, it is likely that some of the methods presented here as research initiatives will soon become clinical practice.
Selected References on Early Response Assessment and Treatment Adaption, Late Response Assessment, and Normal-Tissue Response Evaluation
Molecular imaging is already strongly embedded in radiotherapy; however, the path to widespread and inclusive use in all steps of the radiation treatment process, particularly in planning and evaluation, is still long. In addition to the lack of insurance coverage for scans, the lack of solid clinical evidence is a major impediment to broader use. Recommendations for practicing physicians are still scarce. Of particular note are the National Comprehensive Cancer Network (NCCN) evidence-based guidelines for treating various cancers (www.nccn.org). The NCCN guidelines specific to the use of 18F-FDG PET/CT imaging have recently been summarized by the PET Use Task Force of the Society of Nuclear Medicine and Molecular Imaging and can be found on its website (http://snmmi.files.cms-plus.com/FileDownloads/Centers/NCCNPracticeGuidelinesII.pdf). Table 4 summarizes the NCCN recommendations for PET/CT applications specific to radiation therapy, not including PET/CT applications in diagnosis and staging. As the clinical evidence from multiple clinical trials and clinical practice becomes available for different disease sites and applications, one can expect that this list will grow rapidly. Similar guidelines, some of which are more specific to a particular treatment process or procedures (e.g., use of 18F-FDG PET/CT for tumor delineation) are emerging from the key professional organizations, such as the Society of Nuclear Medicine and Molecular Imaging, European Association of Nuclear Medicine, AAPM, American Association of Therapeutic Radiation Oncology, European Society for Therapeutic Radiation Oncology, and International Committee for Radiation Units.
NCCN Recommendations on Use of 18F-FDG PET/CT for Target Definition and Treatment Response Evaluation in Radiotherapy
CONCLUSION
Clearly, the use of molecular imaging in radiation oncology is continuing to grow. With increasing presence, special emphasis should be put on adequate training of radiation oncology personnel to understand the potential, and particularly the limitations, of quantitative molecular imaging applications. Furthermore, strong collaboration between radiation oncology, nuclear medicine/radiology, and medical physics teams is necessary, as optimal and safe use of molecular imaging can be ensured only within appropriate interdisciplinary teams.
Footnotes
Published online Sep. 17, 2015.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) how to acquire high-quality molecular images for use in radiation therapy; (2) how molecular imaging can be used to plan radiotherapy and evaluate treatment efficacy; and (3) the limitations and challenges to widespread use of molecular imaging in radiation oncology.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through November 2018.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.
- 109.
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- Received for publication August 2, 2015.
- Accepted for publication September 8, 2015.





{kind=link}
{kind=link}