


Abstract
Hodgkin lymphoma (HL) is a curable disease with currently available chemotherapy regimens. Major late morbidities can potentially be avoided in most limited-stage HL patients if the treatment can be adapted to the patient’s early response profile. The therapy efficacy can also be increased early during therapy in nonresponding HL patients with the addition of involved-field radiation therapy or a switch to an escalated therapy protocol, particularly in advanced-stage or unfavorable-risk patients. 18F-FDG PET is a well-established surrogate for tumor chemosensitivity early during therapy. The ongoing PET-adaptive clinical trials are testing the hypothesis that a decision can reliably be made on escalating or deescalating therapy based on interim PET results. Discussed in this review is the integral role of interim 18F-FDG PET in HL, challenges, critical issues to improve its accuracy, and the observations from completed interim PET studies and ongoing PET-adaptive clinical trials.
Ever since its introduction to the diagnostic armamentarium, 18F-FDG PET, integrated with CT, has rapidly evolved to become an essential diagnostic tool in Hodgkin lymphoma (HL) staging, restaging, and response evaluation. Consequently, PET/CT is now considered an integral part of HL management. Nevertheless, the clinical value of interim response assessment during therapy remains to be confirmed by the results of ongoing prospective trials. The capability of a test to individualize treatment, either for escalation or deescalation of standard therapy, largely depends on its predictive power base on a priori definition of treatment response as well as improvement in patient outcomes. Thus, the impact of a PET-adapted treatment strategy will be confirmed only after the outcome data prove the benefit of an effective therapeutic intervention over the standard approach. In this regard, the results of ongoing PET-adapted HL trials will play a major role in allowing PET/CT to claim a crucial role in individualizing HL treatment. However, until these results become available, treatment changes based on interim PET/CT results should be limited to clinical trial settings.
This review will summarize the results of recent literature reporting the predictive value of interim PET in HL patients undergoing first-line therapy, as well as PET-adapted ongoing clinical studies in both early-stage and advanced-stage HL populations. In addition, the requirements for a standardized approach including both PET protocol and interim interpretation rules are reviewed.
CURRENT NEEDS AND TRENDS IN MANAGEMENT OF HL
Unfulfilled Needs for Better Management of HL
HL is a highly chemosensitive disease, with a remarkable remission rate of higher than 75% in patients undergoing standard ABVD treatment (doxorubicin, bleomycin, vinblastine, and dacarbazine) (1). Despite excellent survival rates achieved by most HL patients, 10%–15% of early-stage and 20%–30% of advanced-stage patients ultimately succumb to progression because of chemoresistant or refractory disease (2). Consequently, the optimal first-line treatment for both early- and advanced-stage disease remains controversial, with an unfulfilled need for a highly accurate means to determine tumor chemosensitivity and to predict the completeness of therapy response and patient outcome. It would be ideal to stratify patients into risk groups at baseline or early during treatment so that, in the unfavorable-risk category, the ineffective standard treatment can be escalated to achieve a durable remission or cure and, in the favorable-risk category, therapy can be deescalated to minimize adverse effects. A successful strategy should balance high cure rates with a low likelihood of treatment-related complications. Despite significant efforts to improve on existing risk-stratifying systems, a robust prognostic and predictive means is yet to be discovered to individualize therapy. The widely used international prognostic score (IPS) is applicable only to those patients with advanced-stage disease (3). Additionally, the prognostic systems developed for early-stage HL by the European Organization for Research and Treatment of Cancer and Groupe d’Etude des Lymphomes de l’Adulte (EORTC/GELA) and by the German Hodgkin Study Group (GHSG) and the National Comprehensive Cancer Network are not based on a comprehensive multivariate analysis (4–6). Particularly, with the availability of various effective treatment regimens, there is a growing need for accurate prognostic surrogate markers to guide risk-adapted strategies to improve patient outcome by counterbalancing risk with benefit. 18F-FDG PET/CT was proven to be a good surrogate for interim assessment of tumor chemosensitivity (7–13), even proving to be a more accurate prognosticator than the IPS (4–12), with a wide range of sensitivities and specificities of 43%–100% and 67%–100%, respectively (14).
Current Clinical Management Trends
Most patients with limited-stage disease—that is, almost a third of patients diagnosed with HL (15)—can be cured. Thus, the current trend in this population is to optimize the efficacy of treatment with the least toxicity. The realization of significant long-term chemotherapy- and radiotherapy-related adverse effects, including second neoplasms (25-y actuarial risk of death, 13.5%), cardiovascular disease (6.9%), and infertility (60%–91% with escalated therapy depending on the number of treatment courses) (16–19), paved the way to clinical trials with less intensive treatment protocols. The interest in decreasing first-line therapy in limited-stage favorable HL (nonbulky, stage I–IIA) has further grown in light of prior reports of acceptable overall survivals, without compromised overall survivals, using abbreviated therapies (20,21). In a recent randomized reduced-treatment-intensity trial on patients with early-stage, favorable HL, treatment with 2 cycles of ABVD followed by 20 Gy of involved-field radiation therapy (IFRT) was as effective as, and less toxic than, 4 cycles of ABVD with 30 Gy of IFRT (20). Contrasting with these results, in current practice many centers have adopted a strategy of delivering IFRT to all patients with apparently PET-positive lesions regardless of the degree of uptake largely due to the assumption that these patients are more effectively treated with a potentially non–cross-resistant modality. However, since the significance of a positive interim PET result in early-stage HL is still debated, mainly because of the low specificity and positive predictive value (PPV) of PET-2 results (PET after 2 cycles of standard therapy), many centers continue to consider chemoradiation the standard treatment in this patient subset, with 2–4 courses of ABVD followed by IFRT. However, the enthusiasm to promote intensified treatments for such patients should be tempered by the awareness of significantly increased toxicity and the paucity of data to prove a survival benefit. Accordingly, the use of intensified strategies is currently being investigated. In the ongoing PET-directed clinical trials exploiting the excellent negative predictive value (NPV) of PET/CT imaging, the main objective is to avoid unwarranted therapy-induced sequelae but yet to maintain the treatment efficacy. Thus, therapy optimization presently includes elimination of radiation and abbreviation of therapy cycles in a subgroup selected with a PET-directed approach.
In patients with advanced-stage or unfavorable limited-stage HL, however, the management approach has shifted toward early therapy intensification to overcome chemotherapy resistance and afford a long-term survival. The ongoing prospective interim PET–adapted trials will probably answer the questions centered on whether a PET-adapted approach will allow clinicians to lower the intensity of both chemotherapy and radiotherapy schedules with sufficient safety margins and the effectiveness of escalation protocols. However, it is important to realize that until long-term survival and toxicity data are available from adaptive trials, the ideal management of HL will remain uncertain.
WHAT WE KNOW ABOUT INTERIM PET IMAGING
Continued Challenges
A range of issues remains unsettled to definitively establish the role of interim 18F-FDG PET/CT imaging as a surrogate for therapy response. It is worthwhile to highlight important variables to consider while reviewing the design and results of recent PET-adapted HL trials. Oncologists frequently confront the dilemma of managing potentially false-positive interim PET findings in light of the fact that approximately 30% of patients with no residual viable disease will have false-positive results (7,8).
Minimal Residual Uptake.
After 2 cycles of standard therapy, a negative interim PET result is obtained in approximately 75% of HL patients. In the remaining 25% of patients, interim PET will vary from definitively positive to minimally positive, but the latter group usually will not exceed 10%–15% of the patients (7–9,11). Notably, minimal residual uptake in HL is usually caused by the inflammatory component of the tumor mass. Consequently, interpreting the minimal residual uptake as negative would be clinically more appropriate to minimize false-positive results for residual disease (7,11,22,23).
Early (Limited) Stage With or Without a Bulky Mass.
The high false-positive rates associated with PET/CT imaging in limited-stage HL can be attributed to disease curability and high efficacy of combination chemoradiation treatment, regardless of the results of interim PET (1). However, the presence of a bulky mass could negatively influence the specificity and PPV of end-treatment (8) and of interim PET scans in this group of patients. In the EORTC H10 study, investigating the prognostic role of interim PET in early-stage HL, the PET-2 positive rates were 13% and 23% in early favorable and early unfavorable (mostly bulky mediastinal mass) subgroups, respectively (24). Similarly, in a large cohort of early-stage HL treated with standard therapy, the PPV of PET-2 in bulky and nonbulky patients was 47% and 71%, respectively (25). The higher false-positive rates in bulky HL lesions could be based on a more pronounced inflammatory process within the tumor bulk, but tumor bulk is also an adverse prognostic factor for recurrence (4–6). Although histopathologic confirmation is the gold standard, this method does not solve the issue of sampling errors and also indicates whether a positive finding points to a less curable disease. In addition, a biopsy during therapy is likely to be negative or inconclusive even if the disease is present.
Sites of Residual Disease on Interim PET.
Needless to say, anatomic sites of residual HL after several courses of treatment are generally confined to the disease sites detected at initial staging. One different scenario might be in the case of progressive disease, for which there may be new disease sites in addition to original sites of involvement. Otherwise, it is reasonable to think that any new site of uptake is more likely to reflect an infectious or inflammatory process, particularly in the lungs. It is also possible that new sites of uptake in the vasculature are based on venous thrombosis, which may be relatively frequent in this patient population. An interim analysis of the prospective multicenter Gruppo Italiano Terapie Innovative nei Linfomi (GITIL)/Fondazione Italiana Linfomi (FIL) HD0607 PET response–adapted therapy trial in advanced-stage HL, using the Deauville 5-point scoring system (5PS), found that the most frequently positive site after 2 cycles of standard ABVD therapy is the mediastinum, followed by superficial nodes, abdominal nodes, lung nodules, and the spleen (26). All reported sites of persistent residual uptake were at the original disease sites seen at baseline staging. No case of 18F-FDG uptake at a new site of disease was found.
Timing of 18F-FDG PET Imaging.
Interim PET should be scheduled at least 2 wk, and preferably 3 wk, after the initiation of therapy (22,23) or 4–5 d before the start of the subsequent therapy cycle. This approach is recommended to improve the PPV by minimizing false-positive findings introduced by the inflammatory response, which was proven in a mouse model to peak between 10 and 15 d after therapy administration (22). Not surprisingly, the timing of 18F-FDG PET studies after completion of therapy is more flexible, but a 3-wk window after the end of therapy should be observed to allow time for inflammation to subside (27). The interval between radiation therapy and 18F-FDG PET imaging should not be less than 6–8 wk.
Although the existing data strongly support the use of interim PET after 2 cycles of treatment in HL, there is no established optimal timing with regard to therapy cycles. If and when a paradigm shift toward a tailored approach is established, performing PET after 2 cycles seems reasonable. There is also evidence that PET after 1 cycle has a high NPV with respect to progression-free survival (PFS) (10).
PET/CT Interpretation Criteria
The uncertainties associated with “minimal residual uptake” impelled the initiatives for standardizing PET interpretation criteria. To increase the specificity of PET readings, the definition of a positive interim PET result has evolved from any uptake above the background level to uptake intensity equaling that of the mediastinal blood pool (23) and, more recently, exceeding that of the liver (28–30).
The first standardization initiative was proposed in 2007 by the imaging subcommittee of the International Harmonization Project (IHP) in Lymphoma which provided criteria for a positive 18F-FDG PET scan after completion of therapy (Fig. 1) (23,31). According to these criteria, uptake greater than that in the mediastinal blood pool in residual masses larger than 2 cm is considered positive for residual lymphoma. Because of partial-volume effects, uptake greater than that in the background in lymph nodes smaller than 2 cm is positive for lymphoma. These criteria were based on a retrospective study of 54 patients with diffuse large B-cell lymphoma treated with an anthracycline-based regimen (32). 18F-FDG PET results enhanced the ability to discern the difference in PFS between patients attaining a complete remission (CR) and partial remission (PR) and have made the CR/unconfirmed response category obsolete. Of note, the CR/unconfirmed term was coined for residual masses of unknown significance, which usually represent residual scar tissue and may never fully regress to normal size. The IHP recommended that the mediastinal blood pool be used as an internal reference for lesions of 2.0 cm or larger (Fig. 1) (23,31) to discriminate a positive finding from a negative one. However, for lesions smaller than 2 cm, background uptake remained the reference irrespective of the lesion location. For interim PET readings, a higher cutoff may be used given that these scans measure chemosensitivity rather than response and it has been proven that the prognosis of the group with minimal residual uptake is similar to that of PET-negative patients at interim PET evaluation (7–9). As a result of the rationale provided by the IHP initiative, 18F-FDG PET was integrated into the International Workshop Criteria for response classification of lymphoma (31,32). However, further validation of the IHP criteria is necessary in prospective settings with a large number of patients. It is important to realize that the use of IHP criteria for interim PET scans is considered inappropriate because interim PET is intended to measure chemosensitivity rather than final therapy response at the time of evaluation. Allowing for a low threshold such as mediastinal blood pool may lead to a significant number of false-positive results (33). The other limitation of these criteria is the inclusion of a size measurement to determine whether a higher threshold than the background can be used as a reference. Obviously, low-dose unenhanced CT may not yield accurate measurements, particularly in the abdomen. With the increasing use of interim PET scans, Hutchings and Gallamini advocated the use of the mediastinal blood pool without size measurements of the residual mass (7–9,12). However, particularly in early-stage HL, despite the excellent NPV, the high rate of false-positive findings associated with interim PET scans (30%–70%) has raised concerns about its clinical utility (7–9,11). Moreover, for an interim PET interpretation, the scoring system should be more adaptive depending on the treatment intention. A high PPV using a higher cutoff, that is, liver uptake, may be preferred for therapy intensification to avoid overtreatment and unnecessary toxicity, whereas a high NPV using a lower cutoff, that is, mediastinal blood pool, can be the objective of lowering the intensity of therapy to minimize undertreatment and attendant relapses. More recently, to better address these concerns, at a consensus meeting in Deauville the 5PS system was proposed to allow for a continuous reading scheme suitable for different positivity thresholds to adjust for the intended treatment endpoints (Table 1 and Fig. 2) (28–30) and to minimize false-positive results by using a higher threshold applying liver uptake as the reference site. The reproducibility of Deauville 5PS has recently been confirmed in an international validation study in a retrospective cohort of 260 advanced-stage HL patients imaged after 2 ABVD cycles, with no treatment change based on PET-2 results (34,35). The sensitivity, specificity, NPV, and PPV were 73%, 94%, 94%, and 73%, respectively. After a mean follow-up of 27.2 mo, the 3-year failure-free survival was 28% and 95% for PET-2–positive and PET-2–negative patients, respectively (P < 0.0001). The binary concordance between paired reviewers was high (Cohen κ = 0.84) (34).

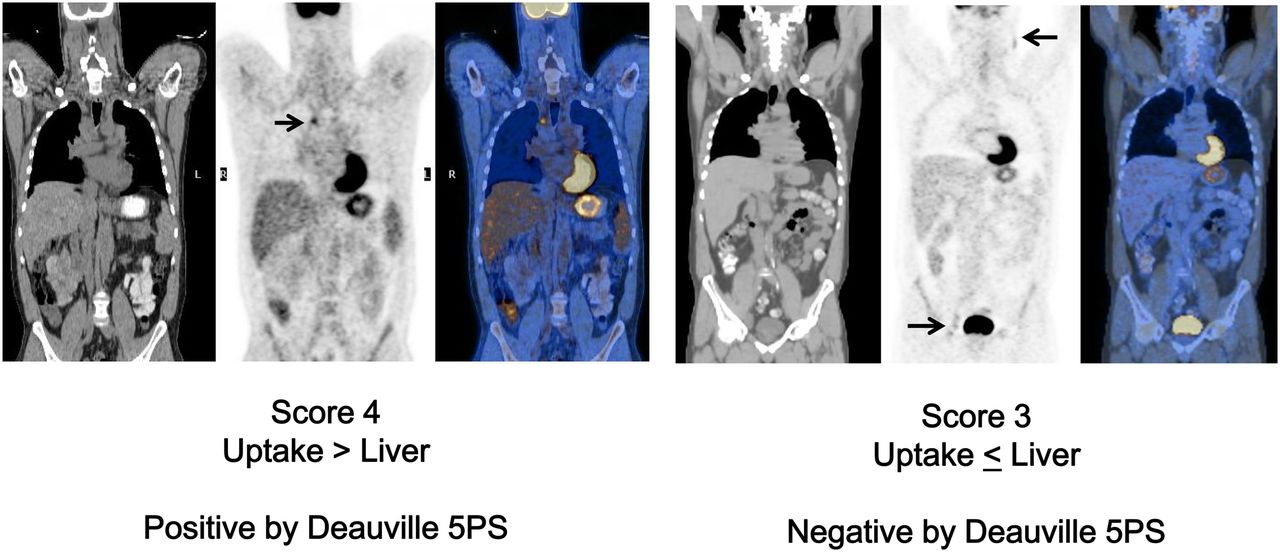
(Left) Coronal CT, PET, and PET/CT images of 29-y-old patient with stage II HL, referred for PET/CT for evaluation of response after 2 cycles of standard therapy. Right paratracheal lymph node shows 18F-FDG uptake moderately higher than that in liver (arrow), interpreted as positive according to Deauville 5PS and qualifying as score 4 by criteria for positive PET scan. (Right) Coronal CT, PET, and PET/CT images of 35-y-old patient with stage III HL, referred for PET/CT for evaluation of response after 2 cycles of standard therapy. Left cervical and right external iliac lymph nodes (arrows) show mildly increased 18F-FDG uptake equaling that in liver, interpreted as negative according to Deauville 5PS and qualifying as score 3 by criteria for negative PET scan. Cutoff for positive interim PET scan can be adjusted to mediastinal blood pool or liver uptake depending on primary objective of study.

(Top) Axial CT, PET, and PET/CT images of 41-y-old patient with stage II HL, referred for PET/CT for evaluation of response after 2 cycles of standard therapy. Left axillary lymph node measuring 2 cm (arrow) demonstrates increased 18F-FDG uptake equaling that in liver (bottom), interpreted as negative according to Deauville 5PS and qualifying as score 3 by the criteria for a negative PET scan. If IHP criteria were used for interpretation, this level of uptake would be interpreted as positive as it exceeds that in the mediastinal blood pool, but IHP criteria were proposed for end-treatment PET and not for interim PET.
Deauville 5PS for Interim PET Evaluation
One should also take the companion CT findings into consideration to clarify the resolution of lymph node or organ involvement, which may not be apparent on the 18F-FDG PET imaging, particularly for disease in the neck and abdomen, the sites where physiologic uptake by normal structures may hinder interpretation without well-defined anatomic markers. In a recent prospective study of 88 patients with stage I–II, nonbulky HL, IHP and Deauville 5PS criteria and percentage decrease in the sum of the products of the perpendicular diameters after 2 cycles were correlated with PFS (36). After a median follow-up of 3.3 y, in a univariate analysis, PET-2 predicted PFS better than percentage decrease in the sum of the products of the perpendicular diameters, and in an analysis combining PET and diagnostic CT, in the PET-2–positive group, a negative diagnostic result on corresponding CT decreased the false-positive PET results, thus increasing the predictive value for PFS by 27%–35%. However, some confidence intervals were large because of small sample sizes. In conclusion, the combined analysis of PET-2 with diagnostic CT suggested a better predictive value for PFS than can be obtained with either test alone. Further studies are under way to confirm these findings.
Future Directions for PET Response Evaluation
Disease bulk at staging is a well-recognized adverse prognostic factor, particularly in early-stage HL (37). Several methods can be used to measure disease bulk, including the mediastinal-to-thoracic ratio and the maximum size of the largest mass. However, there is still no validated or established methodology to evaluate PET-based metabolic tumor volume or total lesion glycolysis to determine disease burden for the whole body using sophisticated software systems (38–40). Notably, like any quantitative analysis, these methodologies require strict adherence to protocols for all imaging periods because metabolic activity measurements depend on multiple variables including interval after injection, blood glucose level, body weight, and technical PET parameters. Preliminary data that are available for patients with HL (40) suggest a better role for Deauville 5PS for interim analysis. The jury is out on future studies to define a widely accepted semiquantitative approach for HL.
WHAT WE LEARNED FROM PUBLISHED 18F-FDG PET STUDIES ON HL
Limited-Stage HL
The discussions for optimizing treatment intensity in limited-stage HL patients focus on the sparing use of consolidative radiotherapy and abbreviation of chemotherapy cycles.
Observational Studies.
Most of the early series reporting on the potential value of interim PET as a response predictor included mixed-HL patient subsets whose risks of relapse were significantly divergent (7–9,11–13). In a subgroup analysis of early-stage HL, Hutchings et al. reported a PPV for interim PET after 2–3 cycles of ABVD chemotherapy of only 30% whereas the NPV was maintained at 95%. In this group, the 2-y PFS in the interim PET–negative and PET–positive patients were 97%–100% and 70%–80%, respectively (7,8). Notably, these results are in stark contrast to those published for advanced-stage HL patients, among whom most of those who were interim PET–positive relapsed within 2 y of completing therapy (9,14).
More recently, the best predictive value for interim PET imaging was reported by Zinzani et al. in a retrospective study (n = 304) on a subgroup of 147 stage I–IIA HL patients treated with standard therapy followed by IFRT (13). Using interpretation criteria similar to those suggested by IHP in lymphoma (23,31), Zinzani et al. found that 97.6% of patients with a negative PET-2 result were in continuous complete remission (CCR) (median follow-up, 45 mo) whereas only 21% of PET-2–positive patients had a CCR (median follow-up, 28 mo). The 9-y PFS for PET-2–negative and PET-2–positive patients were 95% and 31%, respectively (P = 0.0000). However, the retrospective design, inclusion of all early-stage patients regardless of tumor bulk (which is an adverse risk factor), and differences in percentage of patients treated with combined chemoradiotherapy might account for the differences between the results of this series and the others.
In a prospective study of 88 patients with stage I–II, nonbulky HL treated with a nonstandard regimen—doxorubicin, vinblastine, and gemcitabine—using IHP criteria, the 2-y PFS was 88% and 54% for PET-2–negative and –positive groups, respectively (P = 0.0009) (36,41). Similar results were obtained with Deauville 5PS for interim PET reporting (85% vs. 50%). Although the PPV (50%) was relatively better, the NPV (86%) appeared inferior to previously published early-stage HL data (95%–100%) (7,8,11,13), probably because of the lower CR rate achieved with the doxorubicin, vinblastine, and gemcitabine regimen (81%) than with standard ABVD therapy (94%) and the disparate patient risk factors.
In another prospective study, of 104 mixed-stage HL patients (early stage, n = 43) treated with ABVD (100%) and IFRT (79%), and using interpretation criteria similar to those of the IHP, a negative interim PET-2 result was highly predictive of treatment success regardless of stage or IPS risk category (42). In the early-stage group, the PPV and NPV of PET for treatment failure were 44% and 94%, respectively. In the early-stage subset, the 3-y event-free survival for PET-2–positive and PET-2–negative patients was 90% and 50%, respectively (P = 0.002). However, the investigators’ decision to use IPS nondiscriminately across all stages rather than restricting it to advanced-stage patients was the most significant limitation of this study. Moreover, stage IIB and early-stage unfavorable patient groups were evaluated in the same category as those with favorable early-stage disease.
In contrast to the prior supporting results, Barnes et al. failed to show a difference in PFS between interim PET–positive and –negative groups (87% vs. 91%; P = 0.57) in a retrospective analysis of 96 patients with nonbulky limited-stage HL treated with ABVD, 56% of whom received IFRT (43). By contrast, the end-chemotherapy PET result was predictive of outcome, with a PFS of 94% for PET-negative versus 54% for PET-positive patients (P < 0.0001). This study, however, had several limitations; it was retrospective, PET was performed at variable intervals after 2–4 therapy cycles, and the PET reading scheme was not compatible with the prior studies using a 5PS based on the likelihood of residual disease determined by the reviewing physician without a standard internal reference. Notably, even end-therapy PET–positive patients fared well, with a 4-y overall survival of 84%, highlighting the efficacy of available salvage therapies for relapsing low-risk patients. These results were similar to those obtained by Filippi et al. (44) in a recently reported retrospective cohort of 80 stage IA–IIA patients. Despite the preponderance of poor-risk early-stage patients (59% vs. 41%), the percentage of PET-positive patients (defined as having a Deauville score ≥ 3) was only 13.1%. The 3-y PFS and overall survival were, respectively, 97% and 98.4% for interim PET–negative and 100% and 100% for interim PET–positive patients (P = 0.63). The retrospective nature of the study, the possible overtreatment of some of the patients, and the low percentage of positive interim PET results could partly explain these results.
Sher et al., in a retrospective cohort of 73 patients (n = 50, stage I–IIA) treated with ABVD and IFRT regardless of PET response during or after ABVD, investigated the failure-free outcomes of patients with and without postchemotherapy PET positivity (45). For the study objectives, available reports were used without central reinterpretation of images. Among 46 patients who underwent interim PET, treatment failed in only 20% (n = 4) of those with a positive PET result (n = 20), with a 2-y failure-free survival of 85%, in the context of consolidative IFRT. The 2-y failure-free survival rates were 95% and 96% for patients who were, respectively, interim PET–positive/end PET–negative and interim PET–negative/end PET–negative, and these rates were significantly superior to that of patients who were end PET–positive (P = 0.01). The 2-y failure-free survival was 92% and 69% for patients who had residual 18F-FDG avidity after ABVD and consolidative IFRT, indicating that persistent lymphoma can be cured by sterilizing this PET-positive disease.
PET-Adapted Clinical Trials.
In a prospective study, 90 early- and advanced-stage HL patients were treated with a therapeutic strategy adapted to pretherapy prognostic factors and to interim PET and contrast-enhanced CT obtained after 4 courses of ABVD therapy (PET-4) (33). A positive PET result was defined as residual uptake above the local background level. In the early favorable HL group (n = 26), PET-4–negative patients with no progressive disease on CT or patients with CR on CT regardless of PET findings received only IFRT. In the early unfavorable HL and stage III–IV subsets (n = 44), patients with the same PET-4 findings received 4 more cycles of ABVD. The remaining 28 patients with positive PET-4 results and no CR on CT underwent autologous stem cell transplantation. Overall, 96% of patients achieved a CR and only 10.5% relapsed during a median follow-up of 49 mo. Treatment failed in only 12% of PET-4–negative patients, whereas 19.5% of PET-4–positive (n = 31) patients progressed or relapsed. The NPV and PPV for predicting 2-y PFS using the initial criteria were 95% and 16%, respectively (P < 0.0001). When the Deauville 5PS was applied, PPV increased from 19% to 45%, with no impact on the NPV. Notably, the low PPV for PFS was the consequence of therapy intensification, a strategy known to decrease the predictive power of PET in interim PET–positive patients. This study confirms the high NPV of interim PET for treatment outcome in HL, whereas PPV, although improved with the Deauville 5PS, proved not valuable in patients in whom treatment was intensified on the basis of a positive interim PET result (33). Limitations, however, include the lack of a definitive stage categorization according to PET results and a relatively late period for performing interim PET, thus rendering the results incomparable with those of other trials.
In conclusion, despite the nonuniformity of treatment regimens and patient risk groups and the nonstandardized PET interpretation criteria, these interim PET results point toward a considerably high NPV and a moderate but variable PPV in predicting treatment outcome. However, the limited number of disease-related events in the low-risk-category patients and the high likelihood of nonspecific inflammatory processes, particularly in those with bulky disease, contribute to false-positive PET results. Moreover, a PET-response–adapted strategy is used, if clinicians are to exploit the high NPV of interim PET to omit radiotherapy in the PET-negative group, the benefits of omission of consolidative radiation therapy should be weighed against the risk of disease relapse and the salvageability of the individual patient.
Advanced-Stage HL
Early interim 18F-FDG PET has been widely accepted as a prognostic tool for ABVD-treated advanced-stage or early-stage patients with unfavorable risk factors (7–9,11–14). Consequently, it is suggested that an adaptive therapy strategy based on interim PET results might distinguish high-risk patients who would benefit from escalated treatment regimens from low-risk patients whose treatment cycles could be abbreviated to minimize long-term adverse effects.
Observational Studies.
Most of the interim PET data published thus far have reported results during standard ABVD treatment.
In a multicenter prospective trial of 260 patients newly diagnosed with HL (stage IIA [70 with adverse prognostic factors] and stages IIB–IVB [190 with advanced disease]), all but 11 patients were treated with ABVD therapy followed by consolidative radiotherapy in the case of a bulky presentation or a residual tumor mass (12). Patients with minimal residual uptake (greater than that of the mediastinal blood pool) were considered PET-negative for the analysis. After a median follow-up of 2.2 y (range, 0.32–5.18 y), 205 patients were in CCR and 2 patients were in PR. Forty-three patients progressed during therapy or immediately afterward, whereas 10 patients relapsed. The 2-y PFS was 12.8% for patients with positive PET-2 results and 95.0% for patients with negative PET-2 results (P < 0.0001). In a univariate analysis, the treatment outcome was significantly associated with PET-2 (P < 0.0001), stage IV (P < 0.0001), leukocytosis (P < 0.0001), lymphopenia (P < 0.001), IPS as a continuous variable (P < 0.0001), extranodal involvement (P < 0.0001), and bulky disease (P = 0.012). In multivariate analyses, only PET-2 was found to be significant (P < 0.0001), overshadowing the prognostic value of IPS.
In a retrospective study of 304 newly diagnosed ABVD-treated HL patients of all stages (advanced, n = 157), a positive PET-2 result was associated with a 24.5% CCR, whereas 92% of PET-2–negative patients achieved a CCR after a median follow-up of 31 mo (13). In the advanced-stage group, only 26.4% of patients with a positive PET-2 result achieved a CCR, versus 88.6% of those with a negative PET-2 result. Despite a large sample size, this study was limited by its retrospective design, by its long accrual time spanning over 12 y, and by interpretation criteria that differed from those of other studies. In a prospective cohort of 104 HL patients of all stages (advanced stage, n = 61), Cerci et al. reported a 3-y event-free survival of 55% and 94% for PET-2–positive and –negative patients, respectively (P < 0.001) (42). In the advanced-stage group, the 3-y event-free survival rates for PET-2–positive and PET-2–negative patients were 90% and 50%, respectively (P = 0.002), and the PPV and NPV of PET-2 for treatment failure were 57% and 90%, respectively. However, as alluded to in the previous section, IPS categories were used for both early- and advanced-stage patients; thus, the superiority of interim PET over conventional prognostic criteria for the early-stage group (4–6) was not proven.
In a retrospective analysis of prospectively acquired multicenter data, the therapy design for a cohort of 160 early-stage unfavorable or advanced-stage HL patients was such that all PET-2–positive patients after 2 ABVD courses were allocated to receive BEACOPP therapy (4× escalated + 4× baseline), whereas in the PET-2–negative arm, patients continued on ABVD (total of 6 cycles) with consolidation IFRT (46). After a median follow-up of 34 mo, 95% of patients were alive; 65% of PET-2–positive patients achieved a CCR after intensified therapy, versus 90.5% of PET-2–negative patients. After a central review of PET-2 data using Deauville criteria, the failure-free survival was 95% in the PET-2–negative group and 62% in the PET-2–positive group (P < 0.0001). By multivariate analysis, PET-2 was the only prognostic factor associated with failure-free survival (P = 0.001). With the limitation of a retrospective appraisal of the results, these findings suggest that in advanced-stage HL patients treated with ABVD—along with early intensification with bleomycin, etoposide, adriamycin, cyclophosphamide, vincristine, procarbazine, and prednisone (BEACOPP) in a small subset that was PET-2–positive—the treatment outcome is similar to that obtained with this regimen from disease onset. These results could be achieved for the entire cohort while sparing undue toxicity from more aggressive chemotherapy in 80% of patients.
PET-Adapted Clinical Trials.
The efficacy of BEACOPP regimen intensification in PET-2–positive patients with advanced-stage HL during ABVD therapy is currently being tested in several multicenter clinical trials whose results are pending (Table 2). Four studies have reported the results of a PET-adapted strategy in this population (33,47–49).
Design of Interim PET–Adapted Clinical Trials in HL
In the HD15 trial from the GHSG, a subset of 69 patients who had newly diagnosed clinical stage III, IV, or IIB HL with a large mediastinal mass or extranodal disease were treated with either 8 (n = 35) or 6 (n = 24) cycles of escalated BEACOPP or with 8 cycles of BEACOPP14 (n = 10), and interim PET after 4 cycles proved to have quite a high NPV for PFS (47). Similar to the IHP criteria, 18F-FDG uptake above the level of the mediastinal blood pool was considered PET-positive. Only 1 patient relapsed when PET-4 was negative (n = 51) (NPV = 98%). In the PET-4–positive group (n = 18), only 4 progressed or relapsed within 1 y (PPV, 22%). The 4-y PFS for PET-4–negative and PET-4–positive patients was 96% and 78%, respectively (P = 0.016). The low PPV was likely due to a low, conservative threshold for PET positivity; a late time point for the interim PET scan (after the fourth cycle), when most patients could be already considered cured; the absence of a baseline PET scan as a reference for interim PET reporting; and the high efficacy of the escalated BEACOPP regimen, possibly rescuing the few patients with a positive interim PET result.
In the previously cited study by Le Roux et al., a limited cohort of 54 patients with early unfavorable or advanced-stage HL was treated with a PET-adapted strategy after 4 ABVD courses (refer to the “Limited-Stage HL” section) (33). Only 6 of 31 patients with a positive PET-4 result (19.3%) and 7 of 59 with a negative PET-4 result (12%) had a treatment failure, resulting in a high NPV (96%) but a rather low PPV (16%). Limitations of this study included the combined criteria based on both CT and PET results, the relatively late timing of PET during therapy, and the incomparability of the criteria used for interim PET interpretation. The fact that the PPV of PET cannot be determined in a treatment escalation setting would negate the predictive value of PET positivity.
In advanced-stage HL, an adaptive treatment based on a response-adapted (interim PET) and risk-adapted (high vs. low IPS) therapeutic strategy was prospectively tested by the Haifa group in a cohort of 124 advanced-stage HL patients (48). Patients with an IPS score of 0–2 and those with a score of at least 3 were treated with 2 cycles of baseline and escalated BEACOPP, respectively. A subsequent interim 67Ga or PET scan determined the therapy arms either with continuation of the escalated BEACOPP (test-positive) regimen or deescalation to baseline BEACOPP (test-negative). With a median follow-up of 89 mo, the 10-y PFS and overall survival in the entire cohort were 87% and 88%, respectively, yielding similar PFS and overall survival in both arms. Ten-year PFS was 83% in patients with a positive interim PET result, compared with 93% for those with a negative interim result (not statistically significant). As in the trial reported by le Roux et al., the PPV was substantially low (17%) based on an escalation strategy (33). The results of this study suggested that in patients with adverse prognostic factors, 6 cycles of tailored BEACOPP appears beneficial, with a high 10-y PFS, an acceptable incidence of secondary leukemia (1%), and preserved fertility in most female patients.
In a similar study by Avigdor et al., 45 newly diagnosed HL patients with stage IIB–IVB and an IPS of at least 3 were treated with 2 courses of escalated BEACOPP (49). Both interim PET and a contrast-enhanced CT scan determined the response and treatment arms; patients in CR or PR (according to IHP criteria) underwent deescalation with ABVD × 4; patients with less than PR were rescued with autologous stem cell transplantation. CR was defined as a negative PET result with a residual mass of any size. After therapy, the patients were allowed to receive IFRT to bulky masses. Of 44 patients who were in CR or PR, 70% showed a negative and 30% a positive interim PET result. In patients with a PET-2–negative and –positive result, 97% and 69% achieved a CR, respectively. PET-2 predicted the outcome in 75% of patients (33/44); PPV and NPV were 45% and 87%, respectively. After a median follow-up of 48 mo, 97.7% of patients were alive and 2 had died of progressive disease. The 4-y PFS for PET-2–negative and –positive patients was 87% and 53%, respectively (P < 0.01). The weakness of this study was its low power and the combined use of PET and CT to guide treatment, as well as the exclusion of patients who had less than PR, making the results incomparable with other studies.
In conclusion, 2 different strategies, one starting with a less intensive regimen (ABVD) and another with a more efficacious regimen (escalated BEACOPP), adopted opposite decisions based on interim PET results, escalating or deescalating treatment while maintaining the original therapy for PET-negative and PET-positive patients, respectively. The slightly higher NPV of interim PET after BEACOPP than after ABVD points toward a safer deescalation after BEACOPP. However, the risk of overtreatment remains higher in BEACOPP-treated patients.
RECENT PET-ADAPTED MULTICENTER CLINICAL TRIALS
Early-Stage HL
It has yet to be proven with outcome data whether a PET-adapted strategy can modernize management by individualizing therapy in the HL population (50,51). This personalized treatment approach is proposed with a 2-fold objective: first, to reduce treatment intensity in patients with a negative interim PET result in order to minimize chemotherapy- or radiotherapy-induced morbidity, and second, to increase the cure rate in the high-risk population using escalation strategies aiming at better disease control. In this respect, a reliable means of predicting therapy response early during therapy can potentially segregate the favorable-risk population, who could be cured with either conventional therapy or abbreviated courses of less toxic regimens, from the unfavorable-risk population, for whom an early switch to an intensified treatment strategy leading to a survival benefit would be preferable. Multiple trials have been run (52–65) to explore the feasibility of treatment deescalation in both limited-stage and advanced-stage HL patients with a negative interim PET result (Tables 2 and 3) and to address the therapy escalation approach in advanced-stage and unfavorable-risk HL patients who have a positive interim PET result. The PET interpretation criteria used in these trials were somewhat heterogeneous (Table 2).
Current Data on Interim PET–Adapted Clinical Trials in HL
Three recent prospective PET-adapted clinical trials on early-stage HL—by a collaboration of EORTC and GELA, as well as the German and British lymphoma groups (52–54)—have explored the possibility of omitting radiotherapy in patients with a negative interim PET result. Following is a summary of all ongoing studies on early-stage HL (Tables 2 and 3).
Nonbulky Favorable Stage I–II Subset.
Various designs have been applied to both the interim PET–positive and interim PET–negative arms; when interim PET is negative after 2 courses (52,57,58) or 3 courses (50), patients complete treatment with 4 more cycles of ABVD (54), 2 more cycles of ABVD (48,53,54), or only IFRT (50) or will undergo no further therapy (53,54,65). When interim PET is positive, patients receive either 2 cycles of escalated BEACOPP (52,61) followed by either involved-node radiation therapy (INRT) (48) or IFRT (53), 2 more cycles of ABVD (49,65) followed by INRT (58), or 1 more cycle of ABVD (total of 4 cycles) with IFRT (54) (Tables 2 and 3).
Bulky Unfavorable Subset.
When the interim PET result is negative, patients receive 1 or 2 more cycles of ABVD (EORTC/GELA) (54) or a full course of ABVD (total of 6 cycles) without IFRT (55) or with INRT (56). When the interim PET result is positive, patients receive 2 cycles of escalated BEACOPP (52) or 4 cycles of escalated BEACOPP with IFRT (55) or INRT (52,56) (Tables 2 and 3). Interestingly, 2 U.S. collaborative groups, Cancer and Leukemia Group B and Eastern Cooperative Oncology Group (55,56), are conducting 2 similar trials on early-stage bulky HL in which interim PET–positive patients after 2 cycles of ABVD are treated with escalated BEACOPP × 4 followed by IFRT. The former trial is designed to omit INRT to the PET-2–negative group (55) and the latter to deliver the conventional combination of ABVD + INRT to PET-negative patients (57).
The first interim analysis of the EORTC/GELA H10 study of early-stage supradiaphragmatic HL inclusive of favorable and unfavorable risk categories reported on 894 of 1,097 (stage II: 84% and 61% unfavorable) recruited patients (24). In this trial, the experimental arm consists of ABVD × 2 followed by interim PET: if negative, patients receive 2 additional cycles of ABVD and no INRT; if positive, patients receive escalated BEACOPP × 2 followed by 30 Gy of INRT. In the unfavorable group after ABVD × 2, if PET-2 negative, patients receive 4 additional cycles of ABVD and no INRT; if PET-2 positive, patients receive escalated BEACOPP × 2 with 30 Gy of INRT. IHP criteria were used for interpretation, with good agreement among readers (κ = 0.63). PET-2 was positive in 14% and 24% in the favorable and unfavorable categories, respectively. A PET-adapted treatment strategy was thus proven feasible in a large intergroup trial.
The preliminary results of the U.K. RAPID trial on nonbulky stage IA/IIA HL in 571 patients have been reported (66). In this trial, all patients receive ABVD × 3 and are restaged with an interim PET scan. Patients with a negative PET result after 3 courses of treatment (Deauville score, 1–2) are allocated to IFRT or no further treatment. Patients with a positive result after 3 courses (Deauville score, 3–5) are treated with a single further ABVD cycle followed by IFRT. In the interim report, 74.6% of patients had a negative result after 3 courses. After a median of 34.1 mo, 389 of 420 (92.6%) were alive and progression-free; 24 (5.7%) had progressed, and 6 (1.4%) had died, yielding a combined 3-y PFS of 92.2% and overall survival of 98.2%. In this study, given the effectiveness of salvage therapy at the time of relapse, randomizing to observation versus IFRT is powered around the proposition that a PFS that is 7% inferior is acceptable if radiation can be avoided. The results of the H10 and RAPID trials (52,53), despite different median follow-up times, different time points for interim PET scans, and different conclusions (1 trial stopped prematurely because of a futility analysis and the other reached the endpoint), share almost identical trial designs and endpoints.
It is hoped that the ongoing trials will determine the effectiveness of these deescalation and escalation strategies for HL patients in their respective stages and risk categories (Tables 2 and 3).
Advanced-Stage HL
Although the choice of optimal first-line therapy for advanced-stage HL continues to be controversial, ABVD and escalated BEACOPP are the 2 commonly applied chemotherapy regimens. The former regimen, in association with consolidation IFRT, achieves disease control in about 80% of patients, with relatively few side-effects (1,67). Although the latter choice has superior efficacy, with more than 90% of patients enjoying long-term disease control, this control is at the cost of an increased rate of toxicity and long-term adverse effects (68). Tables 2 and 3 summarize the recent PET-adapted clinical trials in advanced HL. Several of these trials were designed to test the cost-to-benefit ratio of the 2 disparate strategies using interim PET as a surrogate for chemosensitivity, the first strategy being initiating first-line therapy with the most efficacious regimen (escalated BEACOPP) and deescalating treatment in patients with a negative interim PET result, to overcome chemoresistance early during treatment, and the second strategy being starting with standard ABVD treatment and escalating to BEACOPP only in those patients who can benefit from an intensified treatment. The first strategy is currently being tested in the GHSG HD18 clinical trial: patients with advanced-stage HL are treated frontline with escalated BEACOPP × 2 followed by interim PET (60). Patients with a negative PET-2 result are allocated to continue with escalated BEACOPP × 4 (standard arm) or to deescalation with escalated BEACOPP × 2 (experimental arm). Patients with a positive PET-2 result are allocated to escalated BEACOPP × 4 (standard arm) or intensification with escalated BEACOPP × 4 supplemented by rituximab (experimental arm). The interim analysis was reported for 240 patients (29). Ninety-eight patients (41%) were PET-2–positive, and 142 (59%) were PET-2–negative; these numbers were updated in Table 3 after a personal communication with the primary investigator. The interpretation scheme for interim PET is similar to those of the Deauville 5PS, but the researchers chose a conservative cutoff (between scores 2 and 3) to minimize false-negative results and avoid undertreatment, as the main objective was treatment deescalation. This choice could explain the high percentage of PET-2–positive scans. There are 2 other trials at the time of this writing, both starting treatment with an escalated BEACOPP regimen and deescalating treatment in the case of a PET-2–negative result or randomization in the experimental arm: the results of interim analyses are pending (58,59). The second strategy is the principal endpoint of 4 currently running prospective international studies using a similar strategy: initiation with 2 courses of ABVD followed by interim PET: PET-2–positive patients are treated with BEACOPP (either BEACOPP14 or escalated BEACOPP), whereas PET-2–negative patients continue on an ABVD regimen (61–63). Other therapy randomizations are embedded in some of these trials. For example, in the RATHL trial, interim PET–negative patients are allocated to receive either ABVD or AVD with no consolidation IFRT (62); in the GITIL HD0607 study, patients with a positive interim PET result are switched to escalated BEACOPP (4 cycles) followed by baseline BEACOPP (4 cycles). Patients with a negative interim PET result were kept on ABVD for a total of 6 cycles and then allocated to receive IFRT or no further treatment (61).
Finally, the fourth ongoing study from FIL, HD0801, is exploring the role of autologous stem cell transplantation in interim PET–positive patients after 2 courses of ABVD (64). In this study, patients with a PET-2–positive result after 2 ABVD courses are allocated to escalated BEACOPP + baseline BEACOPP (4 + 4 courses) versus escalated BEACOPP + baseline BEACOPP (4 + 4 courses) + rituximab, 375 mg/m2 every 21 d. PET-2–negative patients continue with 4 courses of ABVD with or without consolidation IFRT.
The only study whose preliminary results have been presented is the GITIL HD0607study (26). A total of 485 stage IIB–IVB patients were enrolled and treated with ABVD. An interim PET scan after 2 courses was performed. Data on treatment efficacy were available for 221 patients with a median follow-up of 777 d: 32 (17%) had a positive interim PET result and 189 (83%) had a negative interim PET result; 23 of 32 in the PET-positive arm and 178 of 189 in the PET-negative arm are in CCR. The 2-y failure-free survival for the entire cohort, the interim PET–negative group, and the interim PET–positive group was 94.8%, 96.98%, and 82.6%, respectively.
Lastly, the concerns that surround the cost effectiveness of an individualized treatment approach based on a surrogate marker used early during therapy have been addressed by several studies (69,70).
CONCLUSION
There is growing interest in modifying the intensity of first-line therapy for HL in light of prior preliminary reports stressing the safety of treatment deescalation and the higher efficacy of treatment intensification. Despite the fact that the existing interim PET/CT data lent credence to the development of large PET-adaptive clinical trials, interim PET scanning is still considered investigational. Thus, until its clinical benefit is confirmed, its use should be restricted to clinical trials. There are many questions that beg for an answer: how reliable and economically sensible is interim PET as a surrogate for chemosensitivity to individualize therapy? In the case of a negative interim PET result, what should be the most rational therapy change? Is chemotherapy alone with no radiotherapy adequate to cure early-stage HL? In patients without a complete metabolic response after 2 cycles of ABVD, what is the survival benefit from an escalated treatment approach? The long-term follow-up data of these trials will probably resolve the dilemma by answering crucial questions on the judicious use of consolidative radiotherapy, the number of therapy cycles, and the need for escalated treatment protocols.
Footnotes
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the rationale behind the design of PET-adaptive studies either in a deescalation or an escalation setting; (2) the limitations of 18F-FDG PET/CT interpretation criteria proposed for end-therapy and interim-therapy response evaluation; and (3) the challenges involved in the use of interim PET as a surrogate for therapy response.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, participants can access this activity through the SNMMI Web site (http://www.snmmi.org/ce_online) through July 2016.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 27, 2013.
- Accepted for publication May 30, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- US Intergroup Trial of Response-Adapted Therapy for Stage III to IV Hodgkin Lymphoma Using Early Interim Fluorodeoxyglucose-Positron Emission Tomography Imaging: Southwest Oncology Group S0816
- Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group
- Assessment of Tumor Size Reduction Improves Outcome Prediction of Positron Emission Tomography/Computed Tomography After Chemotherapy in Advanced-Stage Hodgkin Lymphoma
- Molecular Imaging Biomarkers for Oncology Clinical Trials