


Abstract
Recently, the thymidine analog 3′-deoxy-3′-18F-fluorothymidine (FLT) was suggested for imaging tumoral proliferation. In this prospective study, we examined whether 18F-FLT better determines proliferative activity in newly diagnosed lung nodules than does 18F-FDG. Methods: Twenty-six patients with pulmonary nodules on chest CT were examined with PET and the tracers 18F-FDG and 18F-FLT. Tumoral uptake was determined by calculation of standardized uptake value (SUV). Within 2 wk, patients underwent resective surgery or had core biopsy. Proliferative activity was estimated by counting nuclei stained with the Ki-67–specific monoclonal antibody MIB-1 per total number of nuclei in representative tissue specimens. The correlation between the percentage of proliferating cells and the SUVs for 18F-FLT and 18F-FDG was determined using linear regression analysis. Results: Eighteen patients had malignant tumors (13 with non–small cell lung cancer [NSCLC], 1 with small cell lung cancer, and 4 with pulmonary metastases from extrapulmonary tumors); 8 had benign lesions. In all visible lesions, mean 18F-FDG uptake was 4.1 (median, 4.4; SD, 3.0; range, 1.0–10.6), and mean 18F-FLT uptake was 1.8 (median, 1.2; SD, 2.0; range, 0.8–6.4). Statistical analysis revealed a significantly higher uptake of 18F-FDG than of 18F-FLT (Mann–Whitney U test, P < 0.05). 18F-FLT SUV correlated better with proliferation index (P < 0.0001; r = 0.92) than did 18F-FDG SUV (P < 0.001; r = 0.59). With the exception of 1 carcinoma in situ, all malignant tumors showed increased 18F-FDG PET uptake. 18F-FLT PET was false-negative in the carcinoma in situ, in another NSCLC with a low proliferation index, and in a patient with lung metastases from colorectal cancer. Increased 18F-FLT uptake was related exclusively to malignant tumors. By contrast, 18F-FDG PET was false-positive in 4 of 8 patients with benign lesions. Conclusion: 18F-FLT uptake correlates better with proliferation of lung tumors than does uptake of 18F-FDG and might be more useful as a selective biomarker for tumor proliferation.
PET using the glucose analog 18F-FDG enables noninvasive tissue characterization based on metabolic differences between benign and malignant tumors. Several studies have found 18F-FDG PET to have a high sensitivity for staging lung cancer (1–3). However, 18F-FDG uptake is not tumor specific, and false-positive findings can occur in inflammatory lesions (4). Therefore, many efforts have been made to develop more selective tracers. In contrast to 18F-FDG uptake values, proliferative activity as measured by Ki-67 immunostaining has been shown to be a specific sign of malignant tumors (5). Furthermore, immunohistochemical studies using various biomarkers for proliferation showed significantly decreased survival in patients with highly proliferating tumors (6). In clinical studies, 18F-FDG uptake correlated with proliferative activity (7,8) and survival in non–small cell lung cancer (NSCLC) (9,10).
11C-Thymidine was the first radiotracer for noninvasive imaging of tumor proliferation (11). The short half-life of 11C and rapid metabolism of 11C-thymidine in vivo make the radiotracer less suitable for routine use. Hence, the thymidine analog 3′-deoxy-3′-18F-fluorothymidine (FLT) was recently introduced as a stable proliferation marker with a suitable nuclide half-life (12). 18F-FLT is phosphorylated to 3′-fluorothymidine monophosphate by thymidine kinase 1 and reflects thymidine kinase 1 activity in A549 lung cancer cells (13). In a first clinical study, our group demonstrated proliferation-dependent 18F-FLT uptake in NSCLC (14).
We devised a prospective study to evaluate whether PET with the novel tracer 18F-FLT better determines tumoral proliferation and better differentiates benign from malignant lung tumors than does PET with 18F-FDG.
MATERIALS AND METHODS
Patients
This prospective study included 26 patients (17 men, 9 women) with a mean age of 62 ± 9.9 y (range, 37–77 y; Table 1). PET with both tracers, 18F-FDG and 18F-FLT, was planned for 30 consecutive patients. Four patients had to be excluded from the study because only 18F-FDG or 18F-FLT PET was performed. Patients were selected when pulmonary nodules on CT scans strongly suggested a malignant tumor. Sixteen patients underwent resective surgery up to 14 d after 18F-FLT and 18F-FDG PET. In the other 10 patients, core-biopsy specimens were used for histopathologic evaluation. All patients gave written consent to participate in this study, which was approved by the local ethical committee.
Patient Characteristics, Tumoral Tracer Uptake, and Proliferation Fraction (Ki-67 Index)
Eighteen patients had malignant tumors. Histopathologic examination revealed NSCLC in 13 patients; small cell lung cancer in 1 patient; and pulmonary metastases from colorectal cancer, renal cell carcinoma, or osteosarcoma in 4 patients. Eight patients had benign tumors (1 case of bronchopulmonary chondroma; 3 of bronchiolitis; 1 of tuberculoma; 1 of focal fibrosis; and 2 of undefined tumors, for which malignancy was excluded by the clinical course).
Immunostaining and Morphometric Analysis
The detailed protocol for immunostaining was published elsewhere (5). Briefly, formalin-fixed and paraffin-embedded sections (5 μm) of resected specimens and biopsy samples were dewaxed, rehydrated, and microwaved in 0.01 mol/L citrate buffer for 30 min. For immunostaining, the monoclonal murine antibody MIB-1 (Dianova), specific for human nuclear antigen Ki-67, was used in a 1:500 dilution. Sections were lightly counterstained with hematoxylin. As a positive control for proliferating cells, sections of human lymph node tissue were used. The primary antibody was omitted on sections used as negative controls. Histopathologic slides were examined by a pathologist who was unaware of the patients’ clinical data.
An area with high cellularity was chosen for the evaluation of MIB-1 immunostaining. All epithelial cells with nuclear staining of any intensity were defined as positive. Proliferative activity was described as the percentage of MIB-1–stained nuclei per total number of nuclei in the sample. With light microscopy, 600 nuclei per slide and 3 slides per case were evaluated for Ki-67 expression to minimize tissue-sampling error. Representative images of each slide were transferred to the computer frame by a video camera using the computer-assisted imaging system OPTIMAS 6.2 (Media Cybernetics, Inc.).
18F-FLT Synthesis and PET Imaging
In accord with the method of Machulla et al. (15), benzoyl-protected anhydrothymidine was used for 18F-FLT synthesis. Radiosynthesis was performed in a PET tracer synthesizer from nuclear interface. After nucleophilic introduction of 18F-fluoride accompanied by an anhydro-ring opening, the benzylated intermediate was cleaved using 1% NaOH solution. 18F-FLT was purified via preparative high-performance liquid chromatography.
18F-FLT and 18F-FDG PET examinations were performed on consecutive days within 2 wk before resective surgery or core biopsy. PET was performed using a high-resolution full-ring scanner (ECAT EXACT or ECAT HR+; Siemens/CTI), which produces 47 or 63 contiguous slices per bed position. Axial field of view is 15.5 cm per bed position. Five bed positions were measured for each patient, covering a total field of view of 77.5 cm. The emission scan included the thorax and abdomen for all patients. Patients fasted for at least 6 h before undergoing PET. Static emission scans were obtained 45 min after injection of 265–370 MBq of 18F-FLT (mean, 334 MBq) or 345–550 MBq of 18F-FDG (mean, 391 MBq). The acquisition time was 10 min per bed position. Four-minute transmission scans with a 68Ge/68Ga ring source were obtained for attenuation correction after tracer application. Images were reconstructed using an iterative reconstruction algorithm described by Schmidlin (16).
All images were evaluated by 2 experienced nuclear medicine physicians. For calculation of standardized uptake value (SUV), circular regions of interest were drawn containing the area with focally increased pulmonary 18F-FLT and 18F-FDG uptake (lesional diameter at spiral CT, 4–48 mm).
Data Analysis
Data are presented as mean, median, range, and SD. The amount of Ki-67–positive cells and the SUVs for 18F-FDG and 18F-FLT were compared using linear regression analysis. Differences were considered statistically significant at P < 0.05. 18F-FDG and 18F-FLT uptakes were compared using the Mann–Whitney U test.
RESULTS
18F-FDG PET
All malignant lesions except 1 carcinoma in situ (NSCLC, patient 13) showed focally increased and easily detectable 18F-FDG uptake (Table 1). The mean 18F-FDG SUV in all visible lesions was 4.1 (median, 4.4; SD, 3.0; range, 1.0–10.6). The mean maximum 18F-FDG uptake was 6.9 (median, 7.0; SD, 5.8; range, 1.4–22.7).
The mean 18F-FDG SUV in the 13 patients with NSCLC was 5.6 (median, 5.5; SD, 2.6; range, 1.0–10.6; Fig. 1), and the mean maximum 18F-FDG SUV was 9.7 (median, 10.1; SD, 5.5; range, 1.4–22.7). Four of the 8 patients with benign lesions presented with focal 18F-FDG uptake. The reviewers visually interpreted 2 of 8 nodules as malignant. Histopathologic examination revealed unifocal tuberculoma in one patient (patient 21; mean 18F-FDG SUV, 1.1; maximum 18F-FDG SUV, 1.8; Fig. 2) and focal bronchiolitis in another patient (patient 19; mean 18F-FDG SUV, 6.9; maximum 18F-FDG SUV, 10.3). Inflammatory lesions were suspected in the other 2 patients. Tissue sampling was not performed because clinical follow-up at 3 mo indicated benign lesions (a 1 × 2 cm nodule disappeared on CT performed at the 3-mo follow-up examination, and a 2 × 3 cm nodule decreased to 1 × 1 cm). Mean 18F-FDG SUVs in these lesions were 2.2 and 3.0, respectively, and maximum 18F-FDG SUVs were 2.9 and 4.3, respectively.

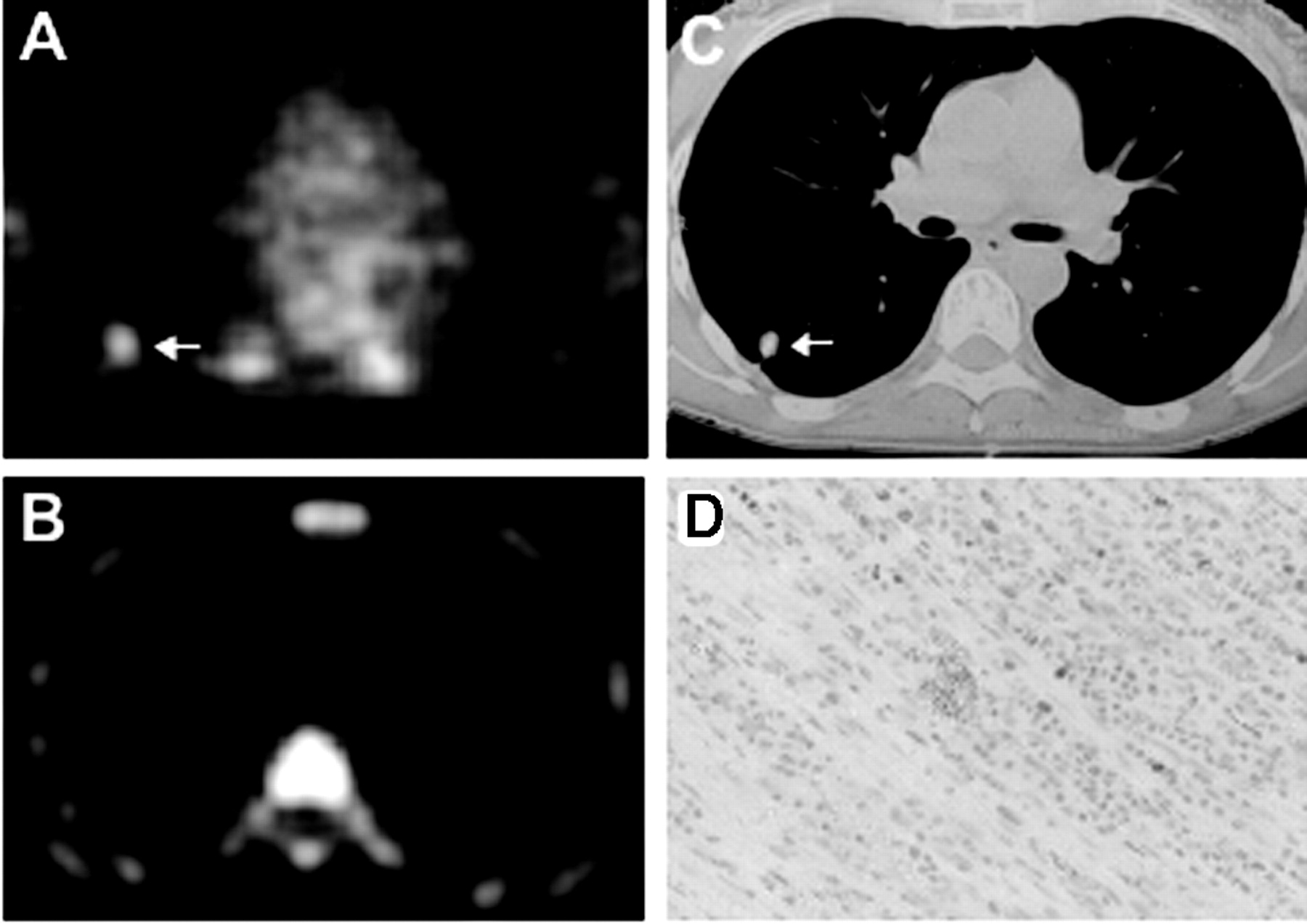
Patient 5, with NSCLC in left upper lobe. (A) Transaxial 18F-FLT PET scan demonstrates high 18F-FLT uptake (arrow) in tumor margin. 18F-FLT uptake in vertebral column, scapula, and ribs represents proliferating bone marrow. (B and C) Corresponding 18F-FDG PET and CT scans show high 18F-FDG uptake in tumor margin and primary lung tumor. (D) On Ki-67 immunohistochemistry, Ki-67–positive nuclei (brown) demonstrate high proliferation rate of 54%, and hematoxylin background staining reveals Ki-67–negative nuclei (blue).

Patient 21, with history of colorectal cancer and suggestive nodule in right middle lobe, for which histopathology revealed solitary tuberculoma. (A) Transaxial 18F-FDG PET scan demonstrates moderate 18F-FDG uptake (arrow) in tumor. (B) No focal tracer accumulation is seen in corresponding 18F-FLT PET scan. (C) Corresponding CT scan shows pulmonary nodule in right middle lobe. (D) On Ki-67 immunohistochemistry, 5% of nuclei show immunoreactivity to Ki-67 antigen.
18F-FLT PET
The mean 18F-FLT SUV in all visible lesions was 1.8 (median, 1.2; SD, 2.0; range, 0.8–6.4; Table 1), and the mean maximum 18F-FLT SUV was 2.7 (median, 1.6; SD, 3.1; range, 1.3–10.4). Mean 18F-FLT SUV in NSCLC was 3.2 (median, 3.1; SD, 2.0; range, 0.8–6.4), and the mean maximum 18F-FLT SUV was 4.7 (median, 5.2; SD, 3.1; range, 1.0–10.4). Increased 18F-FLT uptake within a nodule was identified in 11 of 13 patients with histologically confirmed NSCLC (Fig. 1). Patient 6, with highly differentiated NSCLC and a low proliferation fraction, and patient 13, with a carcinoma in situ, had no visible 18F-FLT uptake.
In pulmonary metastases, the mean 18F-FLT SUV was 1.1 (median, 1.3; SD, 0.8; range, 0.8–2.1), and the mean maximum 18F-FLT SUV was 1.6 (median, 1.9; SD, 1.3; range, 1.0–3.4). In the 1 patient with pulmonary metastases from colorectal cancer (patient 15), the metastases showed no 18F-FLT uptake (Fig. 3). Another patient, with small cell lung cancer (patient 14), showed weak but easily detectable 18F-FLT uptake (mean 18F-FLT SUV, 1.7). No benign tumors showed focal 18F-FLT uptake. Hence, SUV was not determined for these tumors.

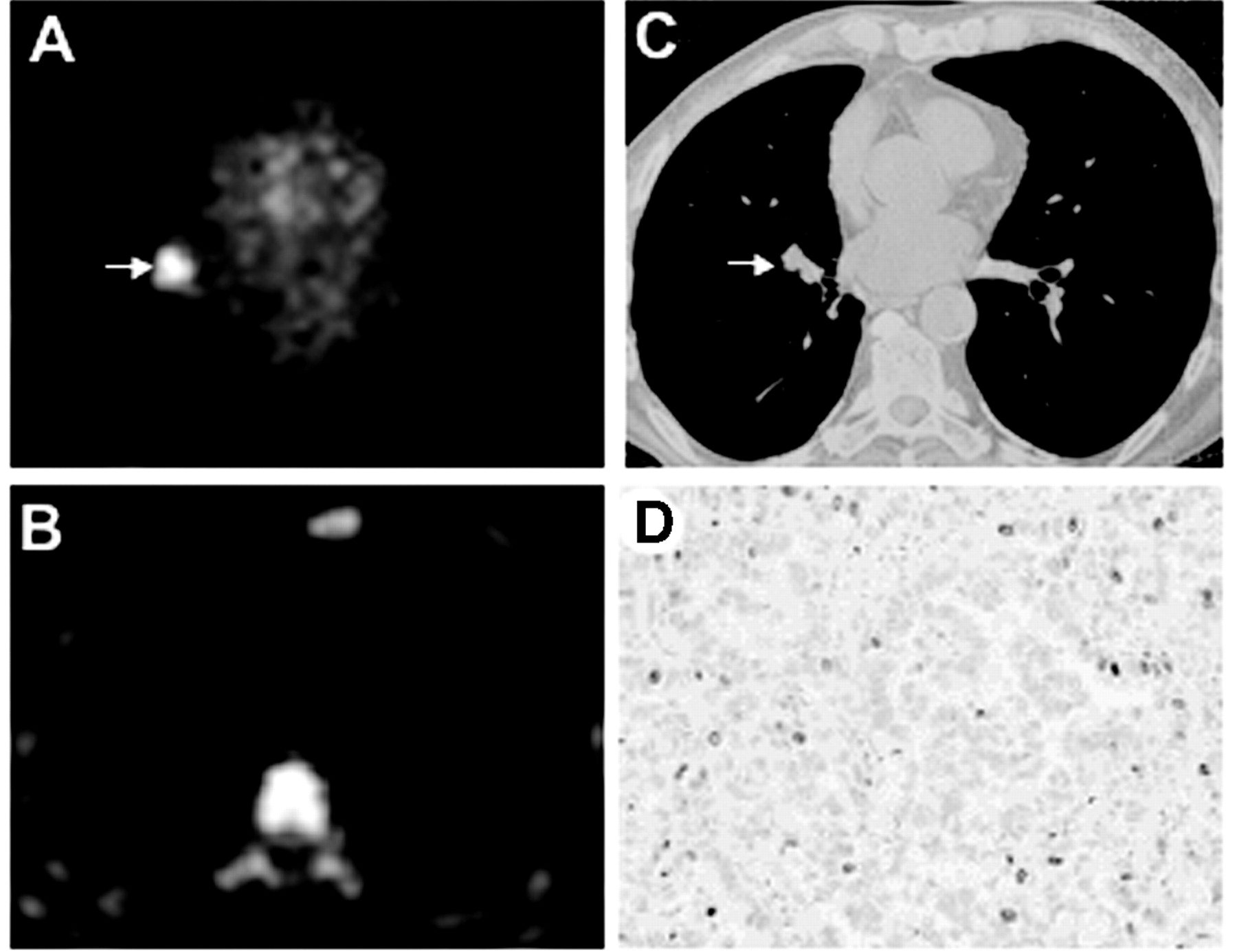
Patient 15, with pulmonary metastases from colorectal cancer. (A) Transaxial 18F-FDG PET scan demonstrates high 18F-FDG uptake (B) in metastatic nodule in right middle lobe. (B) 18F-FLT PET scan shows no tumoral 18F-FLT accumulation. (C) Corresponding CT scan shows pulmonary nodule in right middle lobe. (D) On Ki-67 immunohistochemistry, 12% of nuclei exhibit immunoreactivity to Ki-67–specific antibody MIB-1, indicating low proliferative activity.
In all pulmonary lesions, mean and maximum 18F-FLT uptake was lower than the respective 18F-FDG uptake. Mean 18F-FLT SUV was significantly lower than the respective 18F-FDG SUV (Mann–Whitney U test, P < 0.05). The mean maximum SUVs of 18F-FDG were also significantly higher (P < 0.0001).
Ki-67 Immunohistochemistry
Regional lymph nodes serving as a positive control showed an intense nuclear staining with Ki-67 antibody. In control sections, for which the primary antibody was omitted, no positive nuclear staining was visible.
All malignant tissue specimens contained Ki-67–positive cells. Stained nuclei belonged mainly to epithelial cells, and a very small portion belonged to inflammatory cells. Ki-67 positivity ranged from 1% to 70% of sampled epithelial nucleus profiles (median, 35%). The mean fraction of Ki-67–positive nuclei was 33% (SD, 6.5%). In 6 cases, more than 40% of nuclei showed immunoreactivity for Ki-67 antigen. In NSCLC, the mean proliferation fraction was 37.8% (median, 40%; SD, 19.1%; range, 10%–70%). In pulmonary metastases, the mean proliferative fraction was lower (11.5%; median, 11%; SD, 9%; range, 1%–23%).
Ki-67–positive cells were present in only 1 specimen with benign disease (patient 21, with tuberculoma; Ki-67 index, 5%). Seven benign tissue specimens showed no immunoreactivity to Ki-67 antigen. The range for Ki-67–positive cells was 0%–5%. Ki-67–positive nuclei belonged mainly to inflammatory cells rather than to epithelial cells. The mean of Ki-67–positive cells in benign lesions was 1% (SD, 1.4).
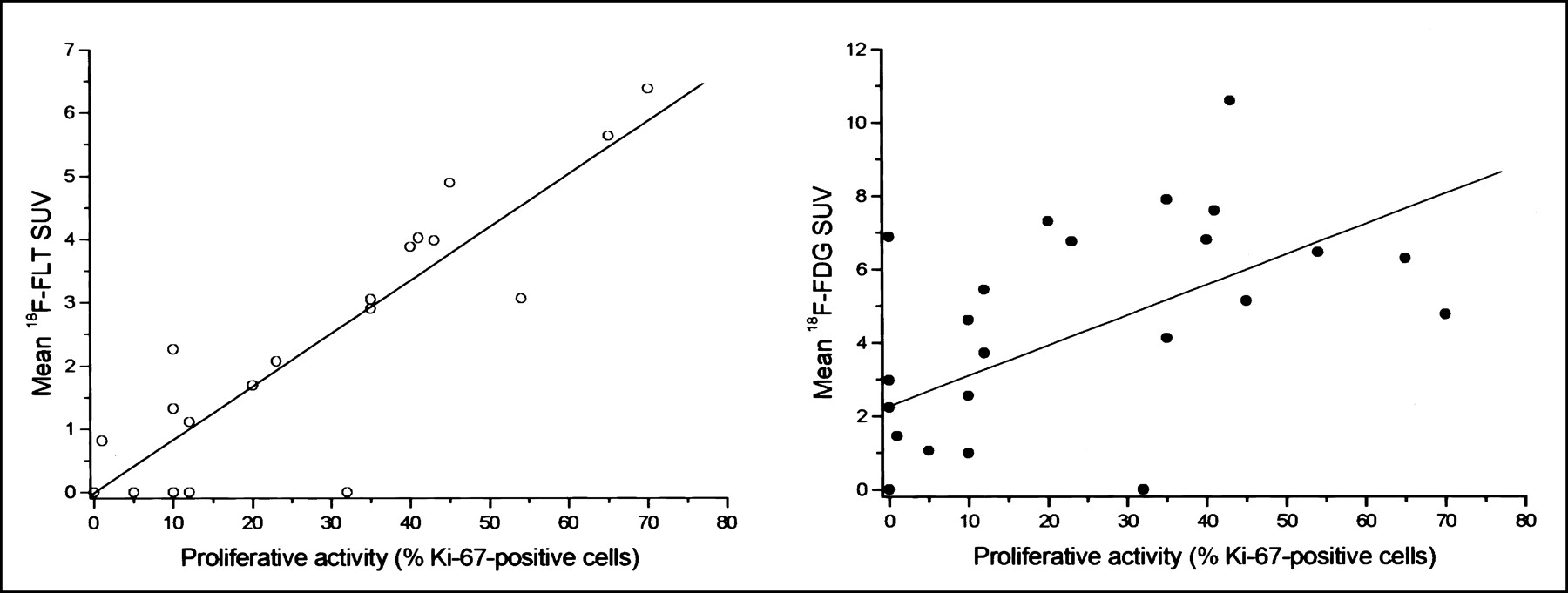
In all lung tumors, linear regression analysis indicated a highly significant correlation between 18F-FLT SUV and Ki-67 index (P < 0.0001; r = 0.92; Fig. 4). Between Ki-67 and 18F-FDG SUV, statistical analysis also revealed a significant correlation (P < 0.001; Fig. 4) but a weak correlation coefficient (r = 0.59).

Linear regression analysis of mean tumoral SUVs of 18F-FLT and 18F-FDG and proliferation fraction (percentage of Ki-67–positive tumor cells). Mean 18F-FLT SUV: significant correlation for P < 0.0001, r = 0.92. Mean 18F-FDG SUV: significant correlation for P < 0.001, r = 0.59.
DISCUSSION
This is the first clinical study comparing the correlation between 18F-FDG uptake and proliferation rate and the correlation between 18F-FLT and proliferation rate for unclear lung lesions. Compared with conventional imaging modalities, 18F-FDG PET has been reported to offer the highest sensitivity for staging lung cancer (17,18). In agreement with these findings, 18F-FDG uptake was increased in all malignant tumors except 1 carcinoma in situ (in patient 13) in our series.
Despite high sensitivity, false-positive findings can occur with 18F-FDG PET, especially in inflammatory lesions (4). Concordantly, focal 18F-FDG uptake was present in 4 of our study patients with inflammatory or other benign lesions (1 case of bronchiolitis, 1 of tuberculoma, and 2 of undefined benign lung tumors). The relatively high number of false-positive findings in the present series is related to patient selection. Other studies with more patients found specificities averaging 78% for 18F-FDG PET in detecting lung cancer (3). Recently, unspecific 18F-FDG uptake has been reported in inflammatory cells such as macrophages (19). Furthermore, many other factors have been reported to influence 18F-FDG uptake, such as upregulation of glucose transporter 1 receptors (20,21), number of viable tumor cells (22), microvessel density, or hexokinase expression (23). In pancreatic cancer, we previously demonstrated that proliferation was a specific sign for malignancy (5) and clearly differentiated benign from malignant tumors. Therefore, a marker specific for proliferation could reduce false-positive PET findings.
A significant correlation between 18F-FDG uptake and proliferative activity was also found for breast cancer (24) and NSCLC (7). However, the low correlation coefficient (r = 0.41–0.73) indicated that 18F-FDG uptake reflects proliferation only in part. In agreement with these findings, the correlation coefficient was as low as 0.59 (r2 = 0.35) in our study. That means that only 35% of 18F-FDG uptake in lung tumors can be explained by proliferative activity.
Various nucleoside analogs have been assessed for imaging proliferation (25–27), but 18F-FLT is probably the best approach so far. 18F-FLT turned out to be stable in vivo (12) and accumulates in lung cancer cells in a proliferation-dependent manner (13). Furthermore, thymidine kinase 1 was revealed as the key enzyme responsible for intracellular trapping of 18F-FLT (28). However, the detailed uptake mechanism is still unknown, and the influence of other factors, such as expression of nucleoside transporters, remains to be determined.
For patients with pulmonary nodules, our data show a highly significant correlation between tumoral 18F-FLT uptake and proliferative activity as indicated by Ki-67 immunostaining. The correlation coefficient was 0.92 (r2 = 0.85). In contrast to the lower correlation coefficient observed for 18F-FDG, 85% of tracer uptake can be explained by proliferative activity. In agreement with this finding, no 18F-FLT uptake was visible in nonproliferating tumors. 18F-FLT PET may therefore be used for the differentiation of benign from malignant lung tumors.
However, 2 patients with NSCLC (1 case of carcinoma in situ and 1 of large cell carcinoma with low proliferative activity), and another patient with pulmonary metastases from colorectal cancer with a proliferation rate of 12%, showed no 18F-FLT uptake but clear uptake of 18F-FDG. Compared with 18F-FDG, 18F-FLT seems less sensitive for staging disease in patients with malignant lung tumors. Further studies with larger patient populations are needed to determine the diagnostic accuracy of 18F-FLT PET in detecting malignant tumors.
Several studies have reported that 18F-FDG PET can be used to assess therapeutic response in various tumors (29–33). A first in vitro study demonstrated that 18F-FLT uptake in esophageal cancer cells was modified early after incubation with various cytotoxic drugs (34). Hence, 18F-FLT may be an alternative for therapeutic monitoring. However, for evaluation of 18F-FLT as a marker for therapy response, large clinical trials are needed.
CONCLUSION
18F-FLT correlates significantly better with the proliferative activity of lung tumors than does 18F-FDG. 18F-FLT may therefore be the superior PET tracer for assessment of therapy response and outcome. Because of 3 false-negative findings in our preliminary study, 18F-FLT PET may be less adequate than 18F-FDG for primary staging in patients with known lung cancer but may be more accurate for differentiation of unclear lung lesions.
Footnotes
Received Nov. 27, 2002; revision accepted Feb. 19, 2003.
For correspondence or reprints contact: Andreas K. Buck, MD, Department of Nuclear Medicine, University of Ulm, Robert-Koch-Strasse 8, D-89081 Ulm, Germany.
E-mail: andreas.buck{at}medizin.uni-ulm.de
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FLT PET/CT Adds Value to 18F-FDG PET/CT for Diagnosing Relapse After Definitive Radiotherapy in Patients with Lung Cancer: Results of a Prospective Clinical Trial
- Parametric Method Performance for Dynamic 3'-Deoxy-3'-18F-Fluorothymidine PET/CT in Epidermal Growth Factor Receptor-Mutated Non-Small Cell Lung Carcinoma Patients Before and During Therapy
- Single-Cell Characterization of 18F-FLT Uptake with Radioluminescence Microscopy
- Molecular Imaging to Plan Radiotherapy and Evaluate Its Efficacy
- Lower Respiratory Tract Infection of the Ferret by 2009 H1N1 Pandemic Influenza A Virus Triggers Biphasic, Systemic, and Local Recruitment of Neutrophils
- Predictive Value of Early-Stage Uptake of 3'-Deoxy-3'-18F-Fluorothymidine in Cancer Cells Treated with Charged Particle Irradiation
- Differential 18F-FDG and 18F-FLT Uptake on Serial PET/CT Imaging Before and During Definitive Chemoradiation for Non-Small Cell Lung Cancer
- Impact of Different Standardized Uptake Value Measures on PET-Based Quantification of Treatment Response
- PET Imaging of Proliferation with Pyrimidines
- FLT-PET Is Superior to FDG-PET for Very Early Response Prediction in NPM-ALK-Positive Lymphoma Treated with Targeted Therapy
- Tumor Microenvironment-Dependent 18F-FDG, 18F-Fluorothymidine, and 18F-Misonidazole Uptake: A Pilot Study in Mouse Models of Human Non-Small Cell Lung Cancer
- PET Imaging of Tumor Growth: Not as Easy as It Looks
- 4'-[Methyl-11C]-Thiothymidine PET/CT for Proliferation Imaging in Non-Small Cell Lung Cancer
- Impact of the Definition of Peak Standardized Uptake Value on Quantification of Treatment Response
- Pharmacodynamic Study Using FLT PET/CT in Patients with Renal Cell Cancer and Other Solid Malignancies Treated with Sunitinib Malate
- [18F]-3'Deoxy-3'-Fluorothymidine Positron Emission Tomography and Breast Cancer Response to Docetaxel
- Quantitative Analysis of Response to Treatment with Erlotinib in Advanced Non-Small Cell Lung Cancer Using 18F-FDG and 3'-Deoxy-3'-18F-Fluorothymidine PET
- Early Prediction of Nonprogression in Advanced Non-Small-Cell Lung Cancer Treated With Erlotinib By Using [18F]Fluorodeoxyglucose and [18F]Fluorothymidine Positron Emission Tomography
- Postchemotherapy Residual Masses in Nonseminomatous Germ Cell Tumor Patients: 18F-FLT PET Is Unlikely to Identify Mature Teratoma, but Imaging of {alpha}v{beta}3 Integrin Expression Could
- Predictive Value of Initial 18F-FLT Uptake in Patients with Aggressive Non-Hodgkin Lymphoma Receiving R-CHOP Treatment
- The future of imaging: developing the tools for monitoring response to therapy in oncology: the 2009 Sir James MacKenzie Davidson Memorial lecture
- Biodistribution and Uptake of 3'-Deoxy-3'-Fluorothymidine in ENT1-Knockout Mice and in an ENT1-Knockdown Tumor Model
- Different Modes of Transport for 3H-Thymidine, 3H-FLT, and 3H-FMAU in Proliferating and Nonproliferating Human Tumor Cells
- Monitoring Tumor Response to Therapy with 18F-FLT PET
- PET/CT with 18F-FLT: Does It Improve the Therapeutic Management of Metastatic Germ Cell Tumors?
- PET/CT with 18F-FLT Is Unlikely to Cause Significant Hepatorenal or Hematologic Toxicity
- Imaging of Proliferation in Hepatocellular Carcinoma with the In Vivo Marker 18F-Fluorothymidine
- 18F-FDG and 18F-FLT Uptake Early After Cyclophosphamide and mTOR Inhibition in an Experimental Lymphoma Model
- [18F]Fluorothymidine Positron Emission Tomography before and 7 Days after Gefitinib Treatment Predicts Response in Patients with Advanced Adenocarcinoma of the Lung
- Noninvasive imaging of cell proliferation following mitogenic extracellular kinase inhibition by PD0325901
- In Vivo Characterization of Proliferation for Discriminating Cancer from Pancreatic Pseudotumors
- Imaging of Cell Proliferation: Status and Prospects
- Imaging Bone and Soft Tissue Tumors with the Proliferation Marker [18F]Fluorodeoxythymidine
- Glioma Proliferation as Assessed by 3'-Fluoro-3'-Deoxy-L-Thymidine Positron Emission Tomography in Patients with Newly Diagnosed High-Grade Glioma
- A Multicenter Clinical Trial on the Diagnostic Value of Dual-Tracer PET/CT in Pulmonary Lesions Using 3'-Deoxy-3'-18F-Fluorothymidine and 18F-FDG
- Imaging Gastric Cancer with PET and the Radiotracers 18F-FLT and 18F-FDG: A Comparative Analysis
- Predicting Treatment Response of Malignant Gliomas to Bevacizumab and Irinotecan by Imaging Proliferation With [18F] Fluorothymidine Positron Emission Tomography: A Pilot Study
- Clinical Applications of PET in Brain Tumors
- Early Response Assessment Using 3'-Deoxy-3'-[18F]Fluorothymidine-Positron Emission Tomography in High-Grade Non-Hodgkin's Lymphoma
- Nuclear Imaging Probes: from Bench to Bedside
- 18F-FLT PET Does Not Discriminate Between Reactive and Metastatic Lymph Nodes in Primary Head and Neck Cancer Patients
- In vivo Biological Activity of the Histone Deacetylase Inhibitor LAQ824 Is detectable with 3'-Deoxy-3'-[18F]Fluorothymidine Positron Emission Tomography
- Early Detection of Chemoradioresponse in Esophageal Carcinoma by 3'-Deoxy-3'-3H-Fluorothymidine Using Preclinical Tumor Models
- Quantification of Cellular Proliferation in Tumor and Normal Tissues of Patients with Breast Cancer by [18F]Fluorothymidine-Positron Emission Tomography Imaging: Evaluation of Analytical Methods
- Potential of PET in oncology and radiotherapy
- Role of Positron Emission Tomography in Lymphoma
- Imaging Proliferation in Brain Tumors with 18F-FLT PET: Comparison with 18F-FDG
- Early Detection of Tumor Response to Chemotherapy by 3'-Deoxy-3'-[18F]Fluorothymidine Positron Emission Tomography: The Effect of Cisplatin on a Fibrosarcoma Tumor Model In vivo
- Comparison of 18F-FLT PET and 18F-FDG PET in Esophageal Cancer
- Kinetic Analysis of 3'-Deoxy-3'-Fluorothymidine PET Studies: Validation Studies in Patients with Lung Cancer
- Monitoring Antiproliferative Responses to Kinase Inhibitor Therapy in Mice with 3'-Deoxy-3'-18F-Fluorothymidine PET
- The Role of PET Scan in Diagnosis, Staging, and Management of Non-Small Cell Lung Cancer
- Is 18F-3'-Fluoro-3'-Deoxy-L-Thymidine Useful for the Staging and Restaging of Non-Small Cell Lung Cancer?
- Evaluation of 3'-Deoxy-3'-18F-Fluorothymidine for Monitoring Tumor Response to Radiotherapy and Photodynamic Therapy in Mice
- Current Concepts in Lymph Node Imaging
- Quantification of 18F-FDG Uptake in Non-Small Cell Lung Cancer: A Feasible Prognostic Marker?
- Oncological molecular imaging: nuclear medicine techniques
- PET Imaging with 18F-FLT and Thymidine Analogs: Promise and Pitfalls