


Abstract
Because 18F-FDG PET alone has only limited value in metastatic germ cell tumors (GCTs), we investigated the addition of 3′-deoxy-3′-18F-fluorothymidine (FLT) to 18F-FDG for early response monitoring and prediction of the histology of residual tumor masses in patients with metastatic GCT. Methods: Eleven patients with metastatic GCT were examined with both 18F-FDG PET/CT and 18F-FLT PET/CT before chemotherapy, after the first cycle of chemotherapy (early response), and 3 wk after completion of chemotherapy. In 1 patient with negative 18F-FLT PET/CT results before chemotherapy, no further 18F-FLT scanning was performed. PET images were analyzed visually and, using standardized uptake values (SUVs), semiquantitatively. The results were compared with the findings of CT and tumor marker levels and validated by histopathologic examination of resected residual masses, including Ki-67 immunostaining (7 patients), or by clinicoradiologic follow-up for at least 6 mo (4 patients). A responder was defined as a patient showing the presence of necrosis, a complete remission, or a marker-negative partial remission within a minimum progression-free interval of 6 mo. Early treatment response was judged according to the criteria of the European Organization for Research and Treatment of Cancer. Results: Before chemotherapy, reference lesions showed increased 18F-FDG uptake (mean SUV, 8.8; range, 2.9–15.0) in all patients and moderate 18F-FLT uptake (mean SUV, 3.7; range, 1.7–9.7) in 10 of 11 patients. After 1 cycle of chemotherapy, mean SUV decreased in responders and nonresponders by 64% and 60%, respectively, for 18F-FDG (P = 0.8) and by 58% and 48%, respectively, for 18F-FLT (P = 0.5). After the end of chemotherapy, mean SUV decreased in responders and nonresponders by 85% and 73%, respectively, for 18F-FDG (P = 0.1) and by 68% and 65%, respectively, for 18F-FLT (P = 0.8). The results of early and final PET were inconsistent in 6 of 11 patients for 18F-FDG and in 4 of 10 patients for 18F-FLT. Both patients with teratoma had false-negative results on both 18F-FDG and 18F-FLT. The sensitivity, specificity, positive predictive value, and negative predictive value for detection of viable tumor after 1 cycle of chemotherapy were 60%, 33%, 43%, and 50%, respectively, for 18F-FDG and 60%, 80%, 75%, and 67%, respectively, for 18F-FLT PET/CT. The respective values after the end of chemotherapy were 20%, 100%, 100%, and 60% for 18F-FDG and 0%, 100%, 0%, and 50% for 18F-FLT PET/CT. Conclusion: PET-negative residual masses after chemotherapy of metastatic GCT still require resection, since the low negative predictive value of 18F-FDG PET for viable tumor cannot be improved by application of 18F-FLT.
Through the application of cisplatin-based chemotherapy followed by secondary resection of residual masses, 70%−80% of patients with metastatic germ cell tumor (GCT) can be cured. Patients with poor-prognosis GCT according to the classification of the International Germ Cell Cancer Collaborative Group (1), however, have distinctly lower cure rates, with a 5-y overall survival of approximately only 48% after standard therapy (2). In an attempt to improve these results, high-dose chemotherapy with autologous stem cell support has been applied (3,4). A benefit was identified especially for those patients with an inadequate tumor marker decline after the first 2 cycles of conventional chemotherapy (4). These data underline the importance of a reliable assessment of early tumor response. The marker decline is the only tool of response evaluation that has been used to guide therapy. However, tumor markers are not always elevated. Furthermore, after chemotherapy, residual masses beyond 1 cm in diameter will be detectable in about 40% of the patients. These residues contain either necrosis or fibrosis but may also contain viable invasive GCT in mature teratomas (5). Resectioning of viable tumor is a means to eradicate residual tumor cells that could give rise to a relapse. Eliminating mature teratoma reduces the risk that either a growing-teratoma syndrome or a secondary GCT will develop. At the same time, resectioning of pure necrosis or fibrosis is probably of no benefit to the patient. To date, no diagnostic tool has been developed that reliably predicts the contents of the residual mass. Changes in GCT morphology documented by CT or MRI and the decline of tumor marker levels do not correctly differentiate between the different histologies (6). Because of its assessment of tumor biology, PET may offer additional diagnostic information for the prediction of therapy response and the classification of residual masses in patients with metastatic GCT (7). Up to now, 18F-FDG has been the only radiotracer used for imaging of GCT. Increased uptake of 18F-FDG is regarded as an indicator of viable tumor. However, 18F-FDG uptake is not specific for tumor; inflammatory and granulomatous tissues also show 18F-FDG accumulation (8). Several studies assessing the role of 18F-FDG PET in seminomas found a significant advantage of this modality over CT in evaluating postchemotherapy residues. However, the role of 18F-FDG PET in staging nonseminomatous residues is limited because 18F-FDG PET cannot differentiate mature teratoma from necrosis and fibrosis (6,7,9–12). In predicting early therapy response, 18F-FDG PET may have a role in poor-prognosis GCT patients, as has been addressed in a pilot study with 19 patients (13,14).
The thymidine analog 3′-deoxy-3′-18F-fluorothymidine (FLT) is a cell proliferation marker. The tracer is trapped within the cell after phosphorylation by thymidine kinase 1, the key enzyme in the salvage pathway of DNA synthesis (15,16). Therefore, the accumulation of 18F-FLT depends on the expression of thymidine kinase 1, which is closely associated with cell proliferation. Increased uptake of 18F-FLT has been shown in various tumors (17–21).
Because of the limitations of 18F-FDG PET in differentiating between viable tumor, teratoma, and necrosis or fibrosis, we performed 18F-FLT PET/CT in addition to 18F-FDG PET/CT in patients with advanced metastatic GCT. The aim was to compare the diagnostic efficacy of 18F-FLT PET/CT with that of 18F-FDG PET/CT for early response monitoring and prediction of residual viable tumor after chemotherapy of metastatic GCT.
MATERIALS AND METHODS
Patients
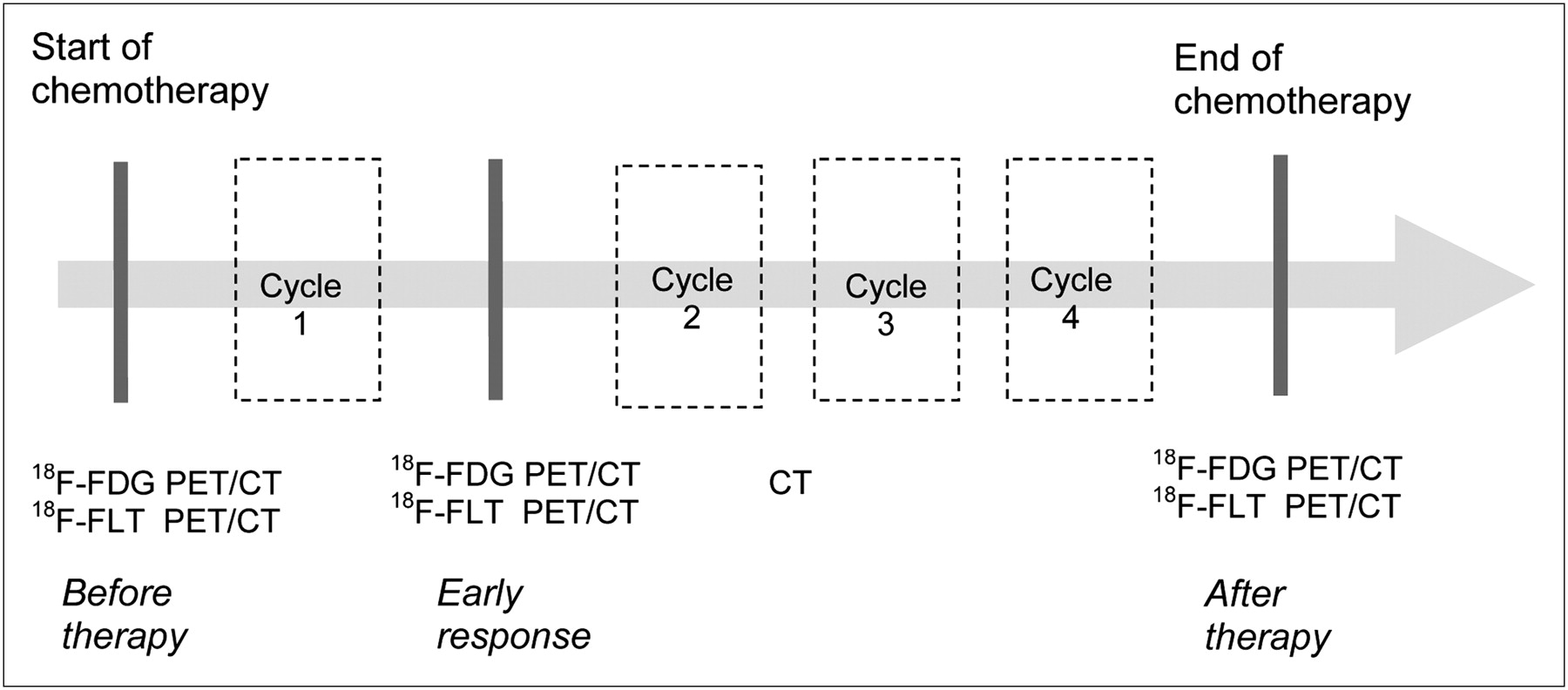
The PET/CT data of 11 consecutive treated men with a mean age of 38 y (range, 23–48 y) and histologically proven metastatic GCT (10 nonseminoma and 1 seminoma, all with gonadal primary) were analyzed. According to the classification of the International Germ Cell Cancer Collaborative Group, the group comprised 6 patients with poor-prognosis GCT, 4 with intermediate-prognosis GCT, and 1 with good-prognosis GCT. All but 2 patients presented with multiple metastatic sites: abdomen (n = 9), mediastinum (n = 6), lung (n = 5), liver (n = 2), bone (n = 2), and central nervous system (n = 1). In all patients, 18F-FLT PET/CT was performed 1–3 d after 18F-FDG PET/CT. In patients with increased tumor 18F-FLT uptake in the pretreatment scan, 18F-FLT PET/CT was repeated after the first cycle of chemotherapy (early response) and 3 wk after completion of chemotherapy (Fig. 1). According to local patient management standards, an additional interim staging by only CT took place after the second cycle. Routine staging also included evaluation of the tumor markers β-human chorionic gonadotropin, α-fetoprotein, and lactate dehydrogenase before each cycle and after completion of chemotherapy. Patients with poor-prognosis GCT received 4 cycles of sequential first-line high-dose chemotherapy plus autologous stem cell support. Patients with recurrent disease were treated with 3 cycles of standard-dose chemotherapy followed by 1 cycle of high-dose chemotherapy and stem cell support. Whenever technically feasible, all residual tumors were resected after completion of chemotherapy (22,23). Follow-up included CT and serum tumor markers every 3 mo after completion of therapy. The PET/CT examinations were performed according to our institutional guidelines, with all patients giving written informed consent. The study protocol was approved by the local Ethics Committee.
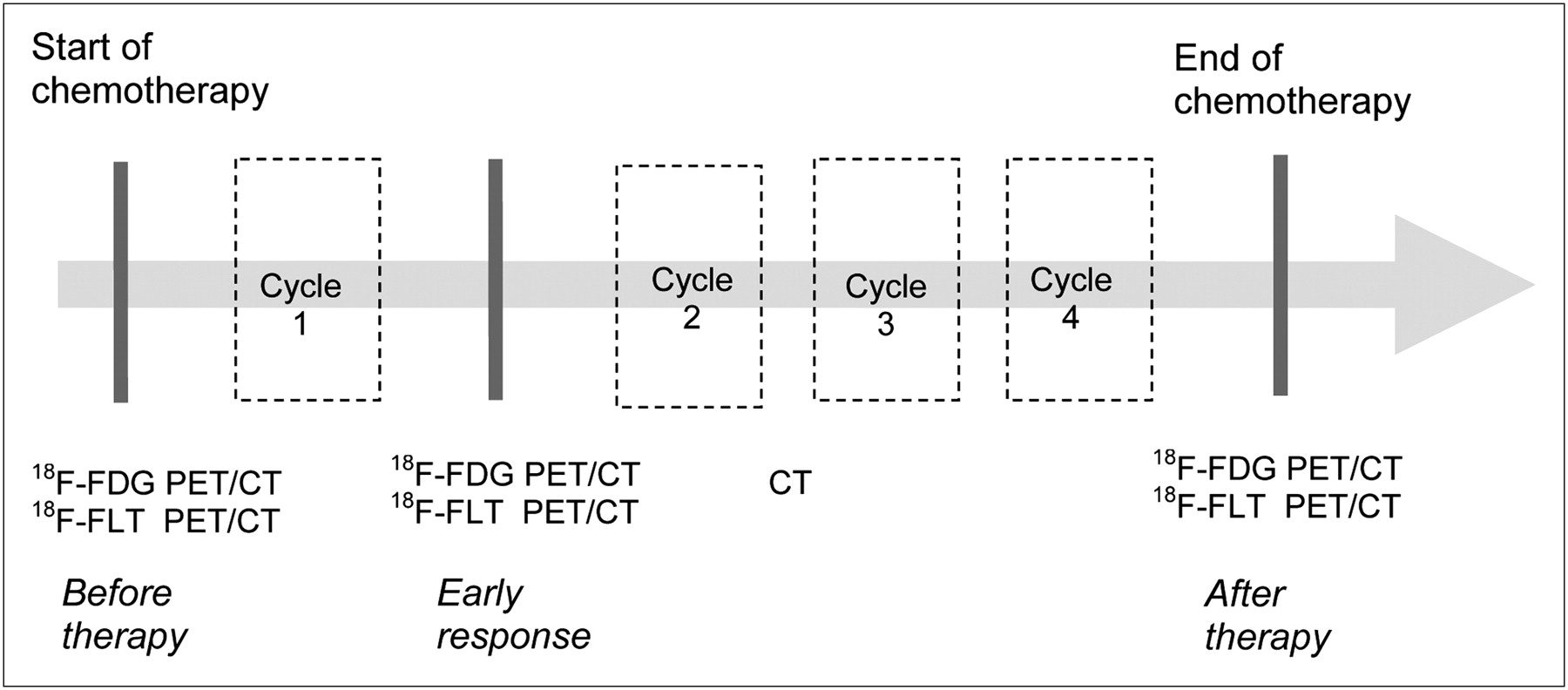
Schedule of 18F-FDG PET/CT and 18F-FLT PET/CT for response monitoring and evaluation of residual masses during and after chemotherapy in 11 patients with metastatic GCT.
PET/CT
The radiotracer 18F-FLT was synthesized at our radiopharmacy department as previously described (24). For 18F-FDG PET, all patients fasted at least 6 h before examination. The injected dose of 18F-FDG and 18F-FLT varied between 350 and 400 MBq according to patient weight. Blood glucose was measured before injection of 18F-FDG to ensure normal blood glucose levels below 120 mg/dL. During the 60-min uptake phase, the patients were given a negative oral contrast agent (1.0–1.5 L mannitol, 2%) for optimal bowel opacification.
In all patients, PET/CT was performed using the Hi-Rez Biograph 16 (Siemens Medical Solutions), consisting of a high-resolution 3-dimensional lutetium oxyorthosilicate PET scanner and a 16-row multidetector CT scanner. Emission data were acquired for 6–8 bed positions, typically covering the base of the skull to the upper thigh, with a 3-min acquisition per field of view. CT was operated at a peak voltage of 120 kV, tube current of 120–250 mAs, rotation time of 0.5 s, collimation of 0.75 mm (thorax) and 1.5 mm (abdomen), and table feed of 12 and 24 mm, respectively. All 18F-FDG PET/CT examinations before and after chemotherapy included single-phase contrast-enhanced CT with intravenous administration of 120 mL of iodinated contrast agent (Ultravist 370; Schering) to obtain diagnostic CT data. To reduce the radiation burden, all 18F-FLT studies and the 18F-FDG PET/CT study after the first cycle were performed without intravenous contrast and included an ultra low dose (30 mAs) CT scan only.
The CT data were used for attenuation correction of PET images. PET images were reconstructed using an iterative algorithm (ordered-subset expectation maximization: 2 iterations, 8 subsets). The reconstructed PET, CT, and fused images were displayed with commercially available software.
Image Analysis
The 18F-FDG and 18F-FLT PET/CT images were evaluated retrospectively, lesion by lesion, by 2 experienced nuclear medicine specialists and 2 experienced CT radiologists working in consensus. The readers were not aware of the histopathologic, clinical, or other imaging findings. Uptake of 18F-FDG and 18F-FLT in the metastatic lesions was evaluated visually and semiquantitatively. On PET images, any focal tracer uptake exceeding normal regional tracer accumulation was regarded as positive and indicative of viable tumor (carcinoma or teratoma), whereas lesions without 18F-FDG or 18F-FLT uptake were classified as negative and indicative of nonviable tumor tissue (necrosis or fibrosis). For semiquantitative analysis, 3-dimensional regions of interest were placed over the tumor semiautomatically using a dedicated software program, with a threshold of 50% of the maximum tracer uptake. According to the formula “standardized uptake value (SUV) = measured activity concentration (Bq/mL)/injected activity (Bq) per body volume (cm3),” the maximum SUV (SUVmax) and mean SUV (SUVmean) were calculated from each region of interest. SUVmean denotes the mean uptake averaged over all voxels in the tumor region of interest. In patients with multiple tumor sites, the lesion with the highest tracer uptake was selected as a reference lesion for the comparative analysis.
Ki-67 Immunohistochemistry
To evaluate the relationship between PET results and direct measurement of proliferation, Ki-67 immunohistochemical staining was performed on 7 tumor specimens obtained from patients who had undergone a surgical resection of residual masses. Formalin-fixed and paraffin-embedded tumor samples were sectioned and immunostained using the monoclonal anti–Ki-67 antibody (clone MIB-1, 1:400; Dako). The MIB-1 index was calculated as the ratio of the number of Ki-67–positive cells to the total number of cells.
Statistical Analysis
The PET findings were compared with histologic results or imaging follow-up. In patients who underwent resection, histopathologic results were used as the reference. A nonresponder was defined as a patient showing viable residual tumor and mature teratoma, a documented CT progression, or increasing tumor marker levels within a minimum follow-up period of 6 mo without resection of residual tumor masses. A responder was defined as a patient showing the presence of necrosis, a documented complete remission, or a marker-negative partial remission on CT within a minimum follow-up period of 6 mo without resection of residues. In cases of multiple resections, the most unfavorable histology was considered.
For early assessment of tumor response by PET, we used the preliminary criteria of the European Organization for Research and Treatment of Cancer (EORTC). According to these, a reduction of tumor 18F-FDG uptake (SUV) to a minimum of 10%−25% after 1 cycle of chemotherapy is considered to indicate metabolic response (25). Because there are no established response criteria for 18F-FLT, we used the same criteria for 18F-FLT as for 18F-FDG. Differences in SUVs between responder and nonresponder were evaluated using the 2-sided t test for independent probe samples. P values of less than 0.05 were considered statistically significant.
For both 18F-FDG PET/CT and 18F-FLT PET/CT, sensitivity, specificity, positive and negative prognostic predictive values, and accuracy were determined after 1 cycle and after completion of chemotherapy on a per-patient basis. If necrosis was found on histologic examination and the patient experienced progression-free survival, negative imaging findings were considered true-negative; if viable carcinoma and teratoma were found on histologic examination and relapse occurred within 6 mo, positive imaging finding were considered true-positive.
RESULTS
The 11 patients with advanced GCT underwent a total of 64 PET/CT examinations, including 33 with 18F-FDG and 31 with 18F-FLT. In a single patient with no distinct 18F-FLT tumor uptake on the pretreatment scan, no subsequent 18F-FLT examination was performed. The results of PET/CT were validated by histopathologic examination of resected residual masses in 7 patients and by clinicoradiologic follow-up in 4 patients. The median follow-up interval for patients without surgical resection of residual masses was 527 d (range, 206–1,337 d). Eight of 11 patients remained progression-free for at least 6 mo after treatment; in 5 of the 8 patients, histopathologic examination of the resected mass revealed necrosis (n = 3) or mature teratoma (n = 2). In the remaining 3 patients, clinical and imaging follow-up demonstrated no signs of relapse within a follow-up period of 1,337, 325, and 206 d. Three of 11 patients progressed between days 241 and 293 after completion of chemotherapy. In 2 of the 3 patients, histopathologic examination of resected residues revealed viable residual tumor confirmed by immunohistochemistry. If residual tumor was present, the proliferation index was determined by MIB-1 index. The third patient had no surgery. Details of patient characteristics, the PET/CT evaluation, and treatment results are listed in Table 1.
Patient Characteristics, PET/CT Findings, and Outcome
Pretreatment Analysis
In the patient-based analysis of pretreatment scans, all patients showed increased 18F-FDG uptake in the reference lesions, with a mean SUVmean and a mean SUVmax of 8.8 and 14.6, respectively (ranges, 2.9–15.0 and 5.1–23.7, respectively). In comparison to 18F-FDG, the 18F-FLT uptake was moderate, with a mean SUVmean and a mean SUVmax of 3.7 and 5.8, respectively (ranges, 1.7–9.7 and 4.6–11.4, respectively). A single patient was 18F-FLT–negative. Most reference lesions showed marked heterogeneous tracer uptake without any visible correlation between the uptake patterns of 18F-FDG and 18F-FLT in corresponding lesions (Figs. 2 and 3A–3C).

Changes in tumor uptake of 18F-FDG (A) and 18F-FLT (B) (SUVmean) after 1 cycle and after end of chemotherapy for responding and nonresponding patients with metastatic GCT.
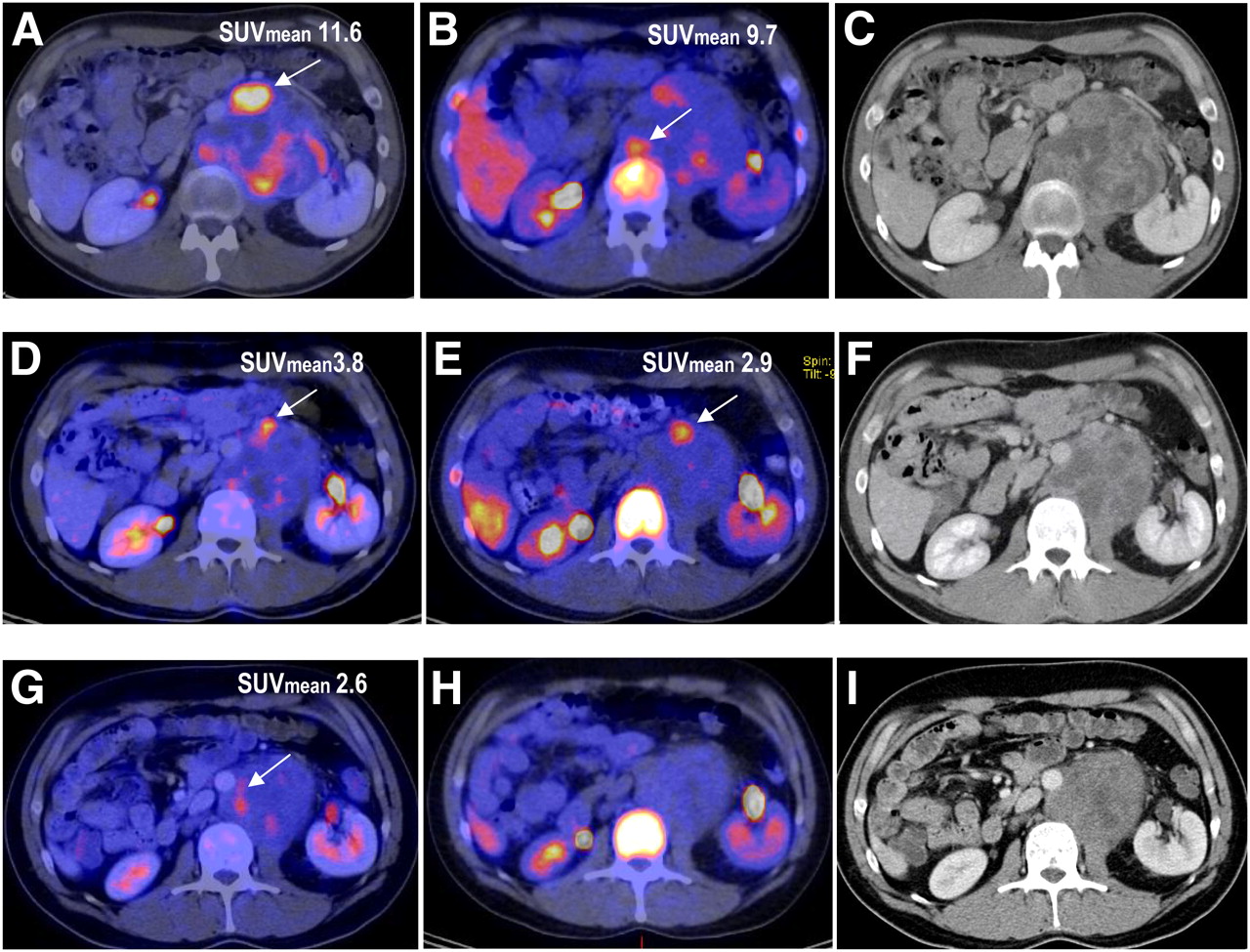
A 31-y-old man with advanced nonseminomatous GCT. (A–C) Before chemotherapy, 18F-FDG PET/CT (A) and 18F-FLT PET/CT (B) show focally increased heterogeneous tracer uptake by abdominal metastasis (arrows), and CT scan (C) shows heterogeneous mass with tumor and necroses. (D–F) After 1 cycle of chemotherapy (early response), tumor shows decreased uptake of 18F-FDG (D) and 18F-FLT (E) and foci of residual viability, and CT scan (F) shows only minor reduction of tumor size and necroses. (G–I) After completion of chemotherapy, tumor shows persistent slightly focally increased 18F-FDG uptake (G), suggestive of viable residual tumor, but normal 18F-FLT distribution (H), and CT scan (I) shows bulky residual mass of unknown viability. Histology of secondary resection revealed highly differentiated teratoma with yolk sac tumor (Fig. 4). Six months after completion of therapy, relapse occurred.
Early Response Monitoring
After 1 cycle of chemotherapy (early response), all patients showed a reduction of both 18F-FDG and 18F-FLT uptake in the reference lesions, indicating a metabolic tumor response according to the proposed EORTC criteria (Figs. 2 and 3D–3F). The mean SUVmean of 18F-FDG decreased from 8.8 at baseline to 2.8 (range, 1.2–6.4; ΔSUVmean, −62%; range, 14%−89%), and the mean SUVmean of 18F-FLT decreased from 3.7 at baseline to 1.7 (range, 0.7–2.9; ΔSUVmean, −52%; range, 14%−79%). There was basically no difference in the decrease of SUV between responders and nonresponders for 18F-FDG (ΔSUVmean, −64% vs. −60%; P = 0.8), and there was no significant difference for 18F-FLT (ΔSUVmean, −58% vs. −48%; P = 0.5).
Posttreatment Analysis
After completion of chemotherapy, the SUVs further decreased to a mean SUVmean of 1.5 for 18F-FDG (range, 1.0–2.6; ΔSUVmean, −80%, and range, 52%−92%) and a mean SUVmean of 1.1 (near background level) for 18F-FLT (range, 0.7–1.4; ΔSUVmean, −63%, and range, 53%−73%) (Figs. 2 and 3G–3I). After completion of chemotherapy, there was a tendency similar to that after 1 cycle, with hardly any difference in the decrease in SUV between responders and nonresponders for 18F-FDG (SUVmean, 85% vs. 73%; P = 0.1) or for 18F-FLT (SUVmean, 68% vs. 65%; P = 0.8), just a slight trend. No tumor showed an increase in 18F-FLT uptake at any time during or after therapy.
The results of early and final predictions of response were inconsistent in 6 of 11 patients on 18F-FDG PET and in 4 of 10 patients on 18F-FLT PET. In all 5 patients in whom viable tumor or teratoma was found on histologic examination of resected masses or who had early relapse during follow-up, the residual masses failed to show any 18F-FLT uptake. There was also no 18F-FDG uptake in 4 of these patients, resulting in a false-negative lesion classification. One patient with histologically proven viable tumor was correctly classified with 18F-FDG PET (Figs. 3G–3I and 4). The 2 patients with teratoma on histologic examination showed false-negative results on both 18F-FDG PET and 18F-FLT PET. All 6 patients with necrosis on histologic examination (n = 3) or progression-free follow-up (n = 3) were correctly classified as true-negative on both 18F-FDG PET and 18F-FLT PET. The sensitivity, specificity, accuracy, and positive and negative predictive values of 18F-FDG and 18F-FLT PET for prediction of response and classification of residual masses are summarized in Table 2.
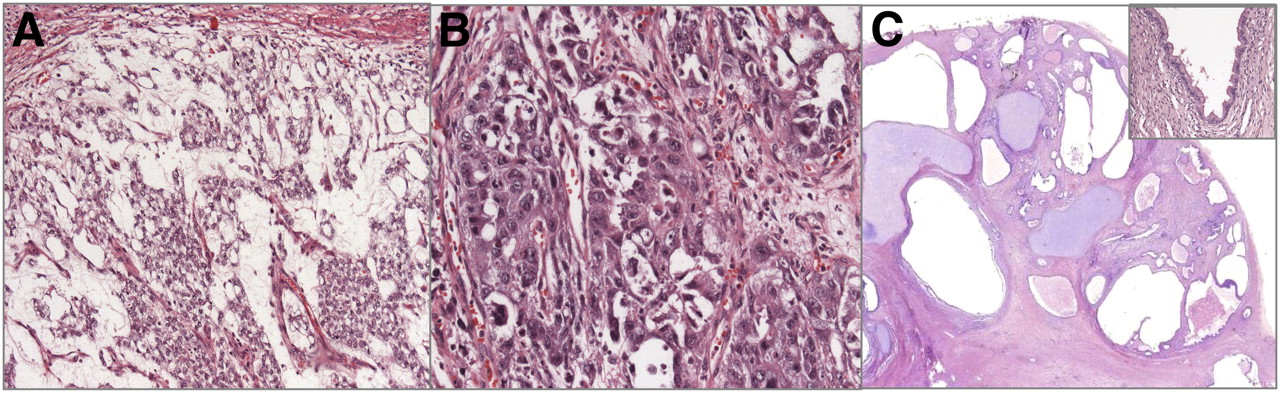
Histologic findings of mixed GCT (Fig. 3). (A) Yolk sac tumor before chemotherapy, with microvesicular growth pattern. Small cysts with thin walls are covered by flattened neoplastic epithelium. (Hematoxylin and eosin, ×200.) (B) Embryonal carcinoma before chemotherapy, with glandular and solid growth pattern. Cells of carcinoma show pleomorphic nuclei, numerous mitoses, and distinct cytoplasmatic borders with eosinophilic cytoplasm. (Hematoxylin and eosin, ×400.) (C) Resected retroperitoneal specimen after chemotherapy. Immature teratoma appears as multiple irregular cysts covered by intestinal, squamous, and bronchial epithelium (insert), in association with areas of pale basophilic cartilage, surrounded by immature mesenchymal spindle cell stroma. Minimal necrotic residues of yolk sac tumors are present, with no parts of embryonal carcinoma. (Hematoxylin and eosin, ×10.)
Diagnostic Value of 18F-FDG and 18F-FLT for Prediction of Response According to Histology and Follow-up
In the group of responding patients (necrosis on histologic examination and progression-free survival), the Response Evaluation Criteria in Solid Tumors showed 5 with marker-negative partial remission and 1 with complete remission on CT. In the group of nonresponders (viable carcinoma and teratoma on histologic examination and relapse within 6 mo), there were 2 patients with stable disease, 2 with marker-negative partial remission on CT, and 1 with marker-positive partial remission on CT.
Ki-67 Immunohistochemistry
The MIB-1 labeling index for the 7 resected tissue samples showed a wide variation, ranging from less than 1% for patients with necrosis on histology to 70% in 1 patient with viable residual lung metastases (Table 1). Analysis indicated no correlation between the MIB-1 index and 18F-FLT SUVmax (r = 0.12, P = 0.82) or Δ18F-FLT SUVmean after therapy (r = 0.13, P = 0.80). There was also no correlation between the MIB-1 index and 18F-FDG SUVmax (r = 0.30, P = 0.52) but a positive correlation between the MIB proliferation index and Δ18F-FDG SUVmean after therapy (r = 0.81, P = 0.025).
DISCUSSION
With cisplatin-based combination chemotherapy, most patients with metastatic GCT can be cured today. Because not all patients will benefit to the same degree from this treatment, it is important to identify nonresponding patients early in the course of chemotherapy to avoid the side effects and high costs of an ineffective therapy. In patients with an unfavorable tumor marker decline, intensification of treatment using high-dose chemotherapy regimens with autologous stem cell support may be beneficial (4). In other tumors, such as lymphoma and breast carcinoma, 18F-FDG PET has been found to be an accurate predictor of metabolic response after only 1 or 2 cycles of chemotherapy (26,27). In a previous study including patients with poor-prognosis GCT, we addressed this question and found that 18F-FDG PET was superior to CT and tumor marker decrease in predicting therapy response after chemotherapy, showing a high sensitivity but limited specificity (13). In the current investigation, all patients demonstrated a metabolic response on 18F-FDG and 18F-FLT PET according to EORTC criteria early after the first treatment cycle. However, when the early and final response assessments are compared on the basis of residual tumor histology or follow-up, the results are inconsistent for 18F-FDG and for 18F-FLT. In general, concerning the decrease of tumor uptake, there was no significant difference between responders and nonresponders for either tracer. However, in the 18F-FDG group, 4 of 11 patients showed false-positive results in the early evaluation that turned out to be necrosis on histologic examination or relapse-free survival on follow-up. False-positive results for 18F-FDG PET during or shortly after chemotherapy, mainly due to an inflammatory process, are a known phenomenon because 18F-FDG is not a tumor-specific agent (8). In contrast, 18F-FLT as a marker of cellular proliferation has proven in preclinical studies to be a more cancer-specific tracer with only low uptake in inflammatory tissue (28,29). The evaluation of our patients revealed that all but one who was negative before treatment showed a substantial reduction of 18F-FLT uptake during chemotherapy even early after the first cycle, but changes in 18F-FLT uptake did not correlate with final outcome. Correlation with the proliferation index determined by immunohistochemical staining with MIB-1 revealed no specific increase in residual tumors, compared with adjacent fibrosis and inflammation. In contrast to studies on lung tumors and colorectal cancer (17,21), we did not find a significant correlation between the Ki-67 index and either 18F-FLT uptake or 18F-FDG uptake in the present study. Only the decrease of 18F-FDG uptake has been found to correlate significantly with proliferation in these tumors. A reason for the lack of correlation between Ki-67 index and 18F-FLT or 18F-FDG uptake could be the inhomogeneous pathology of the disease itself. In fact, testicular cancer is a heterogeneous tumor, often mixed, and thus consisting of a variety of histologic layers (e.g., seminoma and nonseminoma parts, such as teratoma, teratocarcinoma, choriocarcinoma, yolk sac tumors, or polyembryoma), which also vary from one patient to another. The histologic layers differ in growth pattern, differentiation, and proliferation with regard to malignant and well-differentiated components. The problem will become more evident in the postchemotherapy assessment of such tumors with small residues of viable tumor in resected specimens, which are mainly scattered cells and small tubular structures, detected and classified by histologic examination only. These structures display a heterogeneous pattern of proliferative activity with foci of high mitotic activity and large areas of regression. Even here, proliferation can be matched in foam cells and lymphocytic follicles.
Another problem in the therapeutic management of metastasized GCT is that of residual masses remaining in 30%−40% of patients after completion of chemotherapy despite normalized tumor markers. The treatment of these residues remains difficult. To avoid unnecessary surgical resections (in cases of necrosis or fibrosis on histology), prediction of viability of these residual masses and differentiation between viable carcinoma, mature teratoma, and necrosis are important. So far, no diagnostic tool has been developed that reliably predicts the viability of residual masses. Established methods such as CT and serum tumor marker decline allow for an accuracy of 60%−70%, which is too low to avoid surgery. The results of our current study confirm the known limited role that has already been described for CT in classification of postchemotherapy residues (30–32). The authors of several investigations agree that 18F-FDG PET predicts viable residual tumor with high diagnostic accuracy, except in small residuals. However, 18F-FDG PET failed to differentiate mature teratoma from necrosis or fibrosis because both accumulate little or no 18F-FDG (7,9,11,33). Therefore 18F-FDG PET–negative residual tumors still require surgical resection. In our previous study, including 28 patients with mainly nonseminomatous poor-prognosis GCT, we confirmed the results of others demonstrating a high positive predictive value of 90% for 18F-FDG PET but a low sensitivity of 62% and a low negative predictive value of 48% (32). The high percentage of nonseminoma patients with a false-negative PET result in the present study is striking, too. There was no difference between the tracers. In all but 1 patient, the untreated metastases were characterized by a distinct uptake of 18F-FLT in the baseline examination. However, 18F-FLT PET failed to detect the viable residuals in some patients with viable carcinoma or mature teratoma in histology. With 18F-FDG PET, only 1 of those patients with an early relapse and residual malignancy on histology was correctly classified as positive. In contrast, the only seminoma patient was classified correctly as negative on both 18F-FDG and 18F-FLT in the early evaluation and in the final assessment after the end of therapy. Some investigators consider a teratomatous primary histology as the most important factor for the higher rate of false-negative 18F-FDG PET findings in nonseminomas (34). The low sensitivity of 18F-FLT for detection of viable residual tumor in our study may be related to the lower tissue uptake of 18F-FLT than of 18F-FDG in GCTs—a finding that has also been reported for several other tumors (17,19,21,29,35). It may be explained by a competition between 18F-FLT and endogenous thymidine for uptake transporter and phosphorylation by thymidine kinase 1 (36). Moreover, there are data demonstrating that 18F-FLT uptake and transport are determined not by thymidine kinase 1 activity alone but also by adenosine triphosphate levels (37,38). Therefore, the low 18F-FLT uptake in most of our patients may also have been caused by low adenosine triphosphate levels in the bulky GCT metastases. Another influencing factor may be the acquisition time, which was 60 min after injection in all our patients—probably not late enough for 18F-FLT. The poor correlation between the decrease of 18F-FLT during chemotherapy and the final response in our patients contrasts with the results of Pio et al. in breast cancer patients (39). This contrast may be related to the histopathologic differences in tumor type and chemotherapy regime, which may result in different relative contributions of the de novo and salvage pathways of DNA synthesis influencing 18F-FLT accumulation (18,19,29,40). Because of the lower tumor uptake, the usefulness of 18F-FLT for response monitoring in GCT seems to be a priori limited.
The small sample size of 11 patients in our pilot study including predominant nonseminomatous poor-prognosis GCT has to be regarded as a limitation. Any conclusions concerning the whole group of GCT patients, particularly those with less advanced clinical stages, can therefore be only limited. Another limitation is the method of validation, which was histology in only 7 of 11 of patients. In 4 patients the results were based largely on patient follow-up over at least 6 mo after the end of chemotherapy. However, because relapse or progression of GCT in high-risk patients can be expected soon after completion of therapy, our data seem valid even with this limitation.
CONCLUSION
Our results show that despite the lower incidence of false-positive results with 18F-FLT PET than with 18F-FDG PET, PET-negative residual masses after chemotherapy of metastatic nonseminomatous GCT still require resection, because the low negative predictive value of 18F-FDG PET cannot be improved by application of the proliferation marker 18F-FLT. 18F-FLT did not correlate with Ki-67 or response. Positive results on 18F-FDG PET after chemotherapy correlated strongly with the presence of viable tumor. For prediction of response after completion of chemotherapy, the final PET scan, whether performed using 18F-FDG or using 18F-FLT, cannot be replaced by early response evaluation.
Acknowledgments
We thank our technicians Henriette Heners, Agnetha Bürklin, Tina Brutschy, and Diana Feil for their helpful assistance in the acquisition of PET/CT data. We gratefully acknowledge the continuing support of our colleagues from the Radiopharmacy Department.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 6, 2009.
- Accepted for publication November 5, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Reporter nanoparticle that monitors its anticancer efficacy in real time
- PET Imaging of Proliferation with Pyrimidines
- Postchemotherapy Residual Masses in Nonseminomatous Germ Cell Tumor Patients: 18F-FLT PET Is Unlikely to Identify Mature Teratoma, but Imaging of {alpha}v{beta}3 Integrin Expression Could
- Can Evaluation of Targeted Therapy in Oncology Be Improved by Means of 18F-FLT?
- Monitoring Tumor Response to Therapy with 18F-FLT PET