


Abstract
In this pilot study, we evaluated 3′-deoxy-3′-18F-fluorothymidine (FLT) PET for the detection of gastric cancer and compared the diagnostic accuracy with that of 18F-FDG PET. Methods: Forty-five patients (31 male and 14 female) with histologically proven locally advanced gastric cancer underwent attenuation-corrected whole-body 18F-FLT PET and 18F-FDG PET/CT (low-dose CT). 18F-FLT emission images were acquired on a full-ring PET scanner 45 min after the injection of 270–340 MBq of 18F-FLT. 18F-FDG PET/CT was performed 60 min after the injection of 300–370 MBq of 18F-FDG. Mean standardized uptake values for 18F-FLT and 18F-FDG were calculated using circular ROIs (diameter, 1.5 cm) in the primary tumor manifestation site, in a reference segment of the liver, and in the bone marrow and were compared on a lesion-by-lesion basis. Results: According to the Lauren classification, 15 tumors (33%) were of the intestinal subtype and 30 (67%) of the nonintestinal subtype. 18F-FLT PET images showed high contrast for the primary tumor and proliferating bone marrow. In all patients (45/45), focal 18F-FLT uptake could be detected in the primary tumor. In contrast, 14 primary tumors were negative for 18F-FDG uptake, with lesional 18F-FDG uptake lower than or similar to background activity. The mean standardized uptake value for 18F-FLT in malignant primaries was 6.0 ± 2.5 (range, 2.4–12.7). In the subgroup of 18F-FDG–positive patients, the mean value for 18F-FDG was 8.4 ± 4.1 (range, 3.8/19.0), versus 6.8 ± 2.6 for 18F-FLT (Wilcoxon test: P = 0.03). Comparison of mean 18F-FLT and 18F-FDG uptake in tumors with signet ring cells revealed no statistically significant difference between the tracers (6.2 ± 2.1 for 18F-FLT vs. 6.4 ± 2.8 for 18F-FDG; Wilcoxon test: P = 0.94). Conclusion: The results of this study indicate that imaging gastric cancer with the proliferation marker 18F-FLT is feasible. 18F-FLT PET was more sensitive than 18F-FDG PET, especially in tumors frequently presenting without or with low 18F-FDG uptake, and may improve early evaluation of response to neoadjuvant treatment.
Imaging of gastric cancer with 18F-FDG PET is limited because of the relatively high number of primary tumors that are not avid for 18F-FDG (4%–53%), making primary staging and early evaluation of response to treatment impossible (1–5). Published sensitivities for 18F-FDG PET range from 47% to 96% (mean sensitivity, 77%; mean specificity, 99%) for the detection of gastric cancer and from 23% to 73% (mean sensitivity, 45%; mean specificity, 92%) for the detection of lymph node involvement (1–5). 18F-FDG uptake has been shown to be lower in cancers of the nonintestinal type, with signet ring cells, high mucinous content, and lower cellularity (3,6,7).
To increase sensitivity and specificity for gastric cancer, other tracers that complement the information provided by 18F-FDG are required. Increased proliferative activity has been shown to be potentially more specific for malignant tumors than are alterations of glucose metabolism (8). Therefore, measurement of tumor growth and DNA synthesis in vivo might be superior for imaging malignancies of the gastrointestinal tract. Recently, the pyrimidine analog 3′-deoxy-3′-18F-fluorothymidine (FLT) has been reported to be a stable PET tracer that accumulates in proliferating tissues and malignant tumors (9). 18F-FLT is a substrate for thymidine kinase 1, which is a key enzyme in the salvage pathway for the producing of thymidine monophosphate and has been assessed for its potential role in imaging thymidylate synthase inhibition (10–12). Several human studies recently demonstrated the feasibility of 18F-FLT PET for imaging gastrointestinal cancers (13–15).
In this pilot study, we investigated the feasibility of 18F-FLT PET, in comparison to 18F-FDG PET, for imaging locally advanced gastric cancer. Furthermore, we examined the correlation of 18F-FLT uptake with the histologic subtype and location of the tumor.
MATERIALS AND METHODS
Patient Population
Forty-five consecutive patients with an initial diagnosis of locally advanced gastric cancer and meeting the eligibility requirements (presence of biopsy-proven gastric cancer with or without clinical evidence of locoregional lymph node metastases and with a tumor stage of T3–4, Nx, M0, according to the TNM classification system) were included in this prospective study (31 men and 14 women; mean age, 61 ± 11 y; range, 36–78 y). Staging procedures included endoscopy, endoscopic ultrasound, and CT of the chest, abdomen, and pelvis in all patients and additional laparoscopy in some patients. Tumors were localized with endoscopy and—if available and detectable—CT. Patients with an Eastern Cooperative Oncology Group score of less than 1, uncontrolled bleeding from the tumor, gastric outlet syndrome, or an age of less than 18 y were excluded. Details of the study were explained by a physician, and written informed consent was obtained from all patients. The study protocol was approved by the local ethics committee of the Technische Universität München.
Histologic Classification
For histopathologic evaluation of the biopsy samples, the Lauren classification, tumor grading (microscopic growth type), and World Health Organization classification were applied. Tumor location was defined according to the findings on endoscopy and CT. In this study, a modified Lauren classification was used. This classification differentiates only between intestinal (gland formation) and nonintestinal tumors. This modification facilitates the classification based on biopsy and thereby decreases interobserver variability (7,16).
18F-FLT PET
18F-FLT was synthesized as previously described (17). Imaging was performed on a whole-body high-resolution PET scanner (ECAT HR+; Siemens/CTI). This scanner simultaneously acquires 47 contiguous slices with a slice thickness of 3.4 mm. The in-plane image resolution of transaxial images was approximately 8 mm in full width at half maximum, with an axial resolution of approximately 5 mm in full width at half maximum.
A dynamic 45-min acquisition began simultaneously with the injection of approximately 300 MBq of 18F-FLT (range, 270–340 MBq). Twelve 10-s frames, three 1-min frames, and eight 5-min frames were acquired. After the dynamic phase, static emission images were acquired covering the abdominal and pelvic area (2-dimensional mode, 4–5 bed positions, 8 min for each). Emission data were corrected for random coincidences, dead time, and attenuation and were reconstructed by filtered backprojection (Hanning filter with a cutoff frequency of 0.4 cycles per bin). The matrix size was 128 × 128 pixels, with a pixel size of 4.0 × 4.0 mm. The image pixel counts were calibrated to activity concentrations (Bq/mL) and decay-corrected using the time of tracer injection as the reference.
18F-FDG PET/CT
Patients underwent 18F-FDG PET/CT on a Biograph Sensation 16 scanner (Siemens Medical Solutions). The CT protocol included acquisition of a low-dose CT scan (26 mAs, 120 kV, 0.5 s per rotation, and 5-mm slice thickness) from the base of the skull to the mid thigh for attenuation correction, with use of diluted oral contrast material (sodium meglumine ioxithalamate, 300 mg), followed by the PET scan. All PET scans were acquired in 3-dimensional mode with an acquisition time of 3 min per bed position. Forty-seven contiguous slices were acquired per bed position, and the matrix size was 128 × 128, with a slice thickness of 3.4 mm. Images were reconstructed using attenuation-weighted ordered-subsets expectation maximization algorithm (4 iterations and 8 subsets) followed by a postreconstruction smoothing gaussian filter (5 mm in full width at half maximum). Patients fasted at least 6 h before the PET scan, and blood glucose levels were measured before administration of 18F-FDG. All measured values were less than 150 mg/dL. Static emission imaging was performed 60 min after intravenous injection of 300–370 MBq of 18F-FDG. Emission data were corrected for randoms, dead time, scatter, and attenuation, and the same reconstruction algorithm was applied as for the conventional PET data.
PET Data Analysis
All 18F-FLT PET scans were evaluated by 2 experienced nuclear medicine physicians who were unaware of the clinical data and the results of other imaging studies. Circular regions of interest (ROIs) with a diameter of 1.5 cm were placed in the area with the highest tumor activity as described earlier (18). Mean standardized uptake values (SUVs) were calculated from each ROI using the following formula: SUV = measured activity concentration (Bq/g) × body weight (g)/injected activity (Bq). ROIs were also placed in reference segments of the following organs: liver, bone marrow, and muscle. For definition of ROIs and data analysis, computer programs developed in the Interactive Data Language (IDL; Research Systems, Inc.) using the Clinical Application Programming Package (CAPP; Siemens/CTI, Inc.) (19).
18F-FDG PET/CT scans were semiquantitatively evaluated by circular ROIs (diameter, 1.5 cm) with the eSOFT software (Siemens Medical Solutions) and normalized for injected dose and the patient's body weight.
Statistical Analysis
Statistical analyses were performed using SPSS software (version 14.0; SPSS, Inc.). Quantitative values were expressed as mean ± SD, median, and range. Related metric measurements were compared using the Wilcoxon signed rank test and the Mann–Whitney U test in the case of 2 independent samples. The Fisher exact test was used for comparison of frequencies, and Spearman correlation coefficients were calculated to quantify bivariate correlations of measurement data. All analyses were 2-sided, and a P value of less than 0.05 was considered statistically significant.
RESULTS
Patients
The primary tumor was located in the proximal third of the stomach in 28 patients (62%), in the middle third in 9 patients (20%), and in the distal third in 8 patients (18%). According to the Lauren classification, 15 tumors (33%) were of the intestinal subtype and 30 (67%) of the nonintestinal subtype. Most tumors (78%) were poorly differentiated (grade 3 or 4 of 4). The endoscopic tumor category was cT3 in all included patients. Two tumors were cN0, and 43 were cN+. Histologic sections showed signet ring cells in 27 patients (60%) and mucinous content in 18 patients (40%).
Visual Interpretation of Gastric Cancer with 18F-FLT PET and 18F-FDG PET/CT
In the 45 patients undergoing an initial 18F-FLT PET scan, all tumors showed focal uptake of 18F-FLT, resulting in a sensitivity of 100%. Background activity was low for 18F-FLT, resulting in a high tumor-to-background contrast. In the 18F-FDG PET/CT scan, only 31 of 45 tumors could be detected visually, resulting in a sensitivity of 69% and a significantly lower detection rate than for 18F-FLT (P < 0.01) (Table 1). Uptake in the 18F-FDG–avid tumors was much higher than the physiologically variable uptake in the gastric wall.
Sensitivity and Uptake of 18F-FLT and 18F-FDG in Gastric Cancer
Semiquantitative Evaluation of 18F-FLT Uptake and Biodistribution
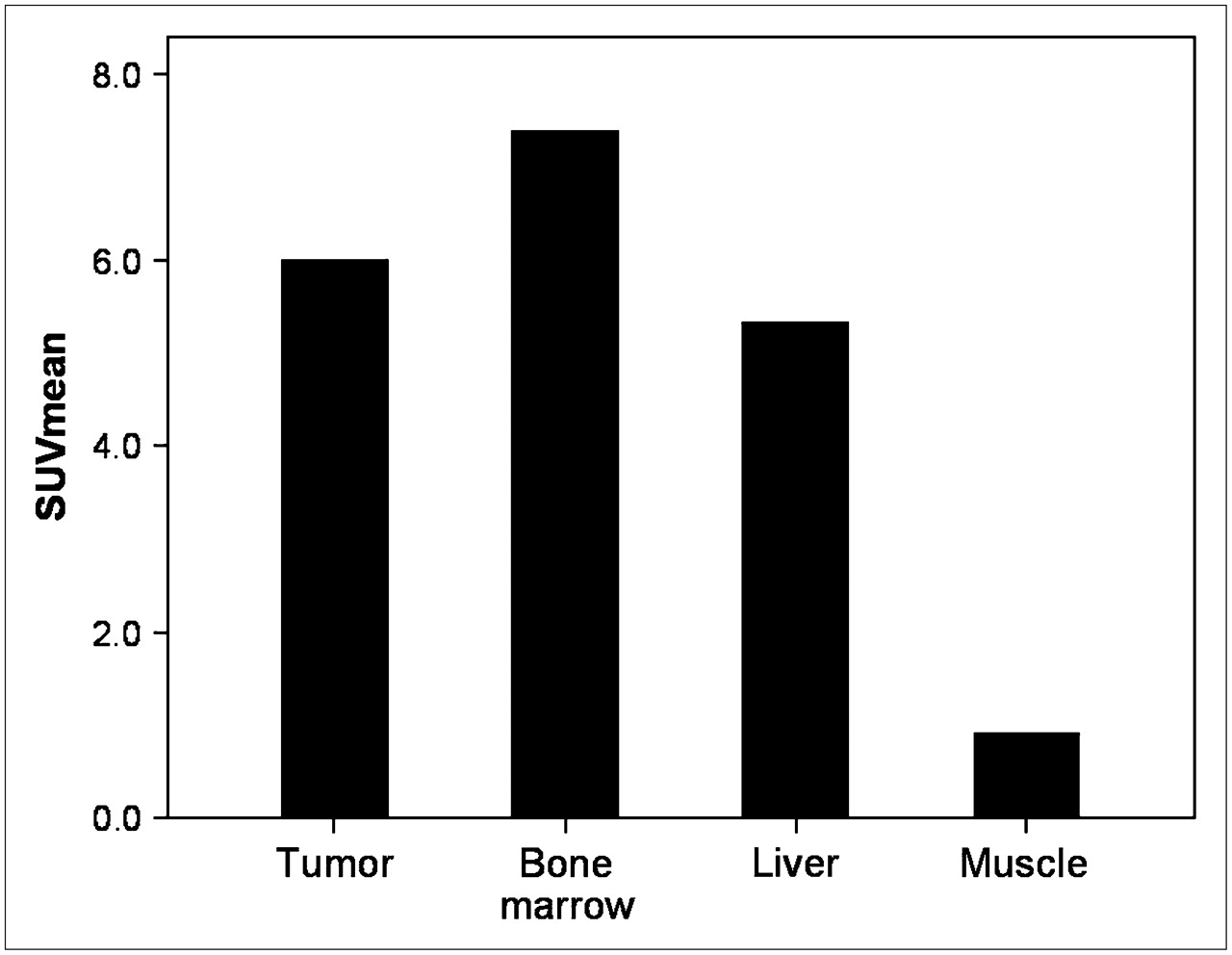
In all 45 patients, focal 18F-FLT uptake could be detected in the region of histologically proven gastric cancer. The mean 18F-FLT uptake (18F-FLT SUV) of the tumor sites was 6.0 ± 2.5 (median, 5.3; range, 2.4–12.7). Besides tracer accumulation in the tumor, high physiologic 18F-FLT uptake in proliferating bone marrow was observed (mean SUV, 7.4; median, 7.2; range, 3.7–10.6). The mean 18F-FLT SUV in a reference segment was 5.3 for liver (median, 4.9; range, 2.9–13.2) and 0.9 for muscle (median, 0.9; range, 0.4–1.3). Figure 1 illustrates the biodistribution of 18F-FLT in patients with gastric cancer.
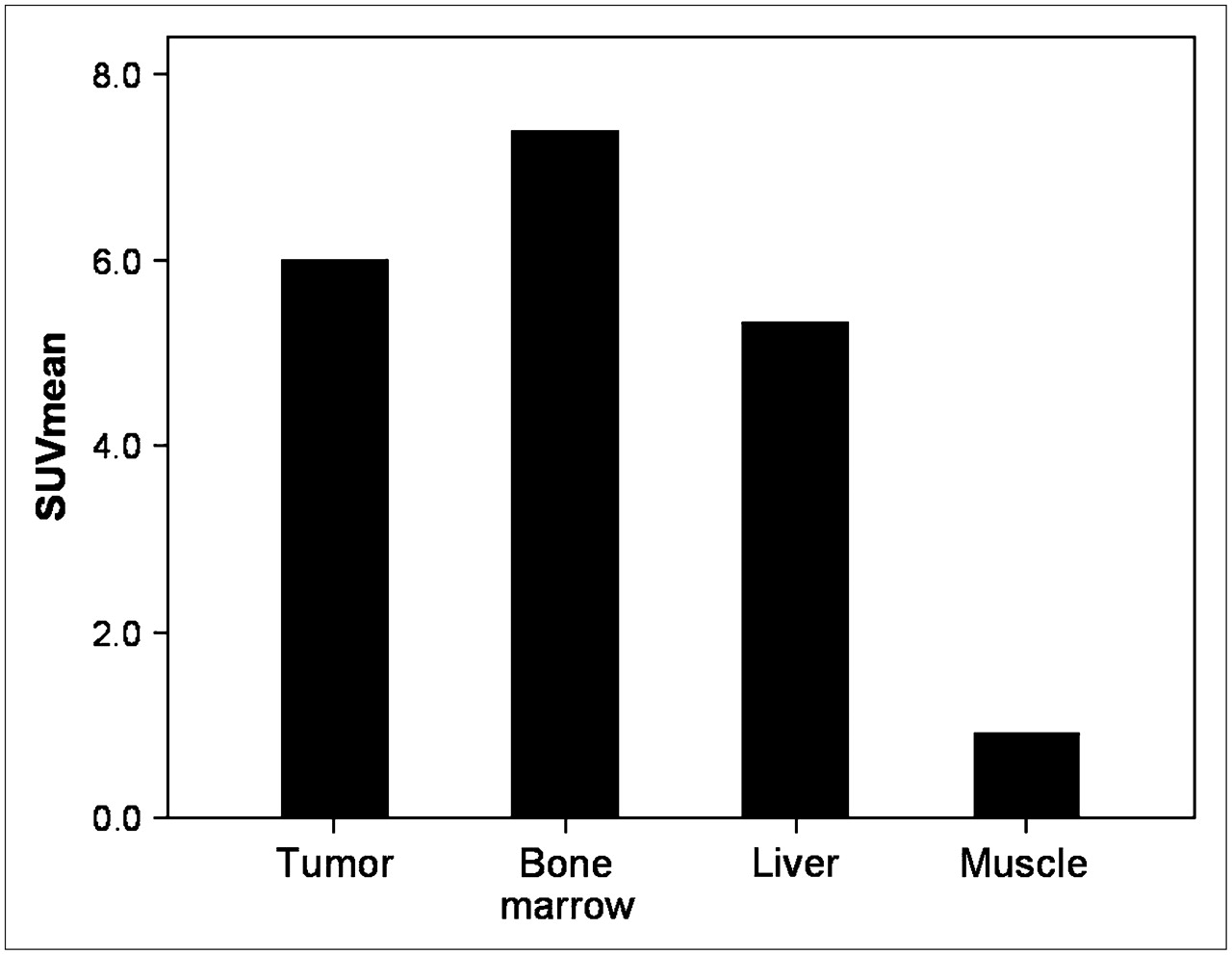
Biodistribution of 18F-FLT in all patients.
Focal 18F-FLT uptake in the tumor sites showed no significant dependence on location (proximal third, 6.1, vs. distal thirds, 5.9; P = 0.87), Lauren classification (intestinal subtype, 7.1, vs. nonintestinal subtype, 5.5; P = 0.11), or presence of mucinous cells (mucin-positive, 6.1, vs. mucin-negative, 6.0; P = 0.65). In contrast, the subgroup of tumors with signet ring cells had a significantly lower 18F-FLT uptake than did tumors without signet ring cells (5.4 vs. 7.0; P = 0.05).
Imaging with 18F-FDG PET/CT
In 14 of the 45 patients, the primary tumor was not detectable with 18F-FDG PET/CT (Table 1). Tumors with insufficient image contrast had signet ring cells more often than did 18F-FDG–positive tumors (11/14 [79%] vs. 16/31 [52%]), but this difference was not statistically significant (P = 0.09). Additionally, there was a tendency toward a higher proportion of 18F-FDG PET–negative tumors in the middle and distal thirds than in the proximal third of the stomach (8/14 [57%]), compared with 18F-FDG–positive tumors, but statistical significance was not reached (9/31 [29%]; P = 0.07).
Mean 18F-FDG uptake for the 18F-FDG–positive tumors was 8.4 ± 4.1 (median, 7.1; range, 3.8–19.0). The subgroup of 18F-FDG–positive tumors with signet ring cells had a significantly lower 18F-FDG uptake than did tumors without signet ring cells (6.4 vs. 10.7; P < 0.01). Additionally, tumoral 18F-FDG uptake correlated significantly with the Lauren classification. Tumors of the intestinal subtype had a significantly higher 18F-FDG uptake than did nonintestinal tumors (10.5 vs. 7.2; P < 0.01). In contrast, a difference in uptake dependent on the location (8.3 vs. 8.9; P = 0.62) and on the presence of mucinous content (8.3 vs. 8.5; P = 0.48) was not statistically significant.
Comparison of 18F-FLT and 18F-FDG Uptake
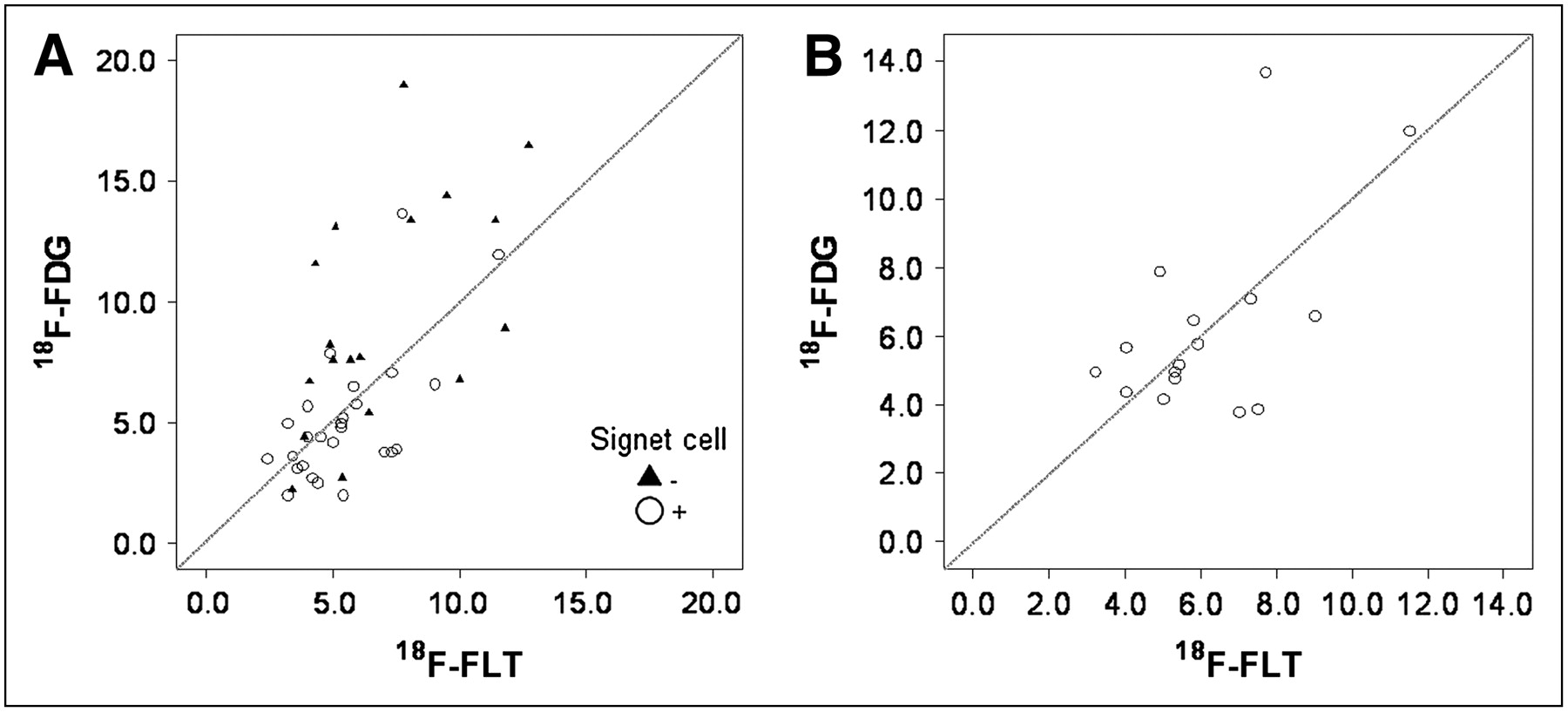
Analyzing all patients with an 18F-FDG uptake in gastric cancer higher than background activity (n = 31) showed a significant correlation between the mean SUVs of the 2 radiotracers studied (18F-FLT, 6.8 ± 2.6, vs. 18F-FDG, 8.4 ± 4.1; r = 0.46; P < 0.01) (Figs. 2 and 3). Despite this correlation, initial 18F-FDG uptake was significantly higher than initial 18F-FLT uptake for both mean SUV (P = 0.03) and maximum SUV (7.8 ± 3.0 vs. 11.5 ± 5.6; P < 0.01). In contrast, in the subgroup of signet ring cell–positive tumors (n = 27), there was no significant difference between 18F-FLT and 18F-FDG uptake as indicated by mean SUV (18F-FLT, 6.2 ± 2.1, vs. 18F-FDG, 6.4 ± 2.8; P = 0.94) or by maximum SUV (18F-FLT, 7.2 ± 2.6, vs. 18F-FDG, 8.4 ± 3.4; P = 0.07). Uptake of the 2 tracers showed no significant correlation in this subgroup (r = 0.38; P = 0.15) (Fig. 2). In the subgroup of 18F-FDG–negative tumors, the mean SUV of focal 18F-FLT uptake was 4.2 ± 1.2 (Table 1).
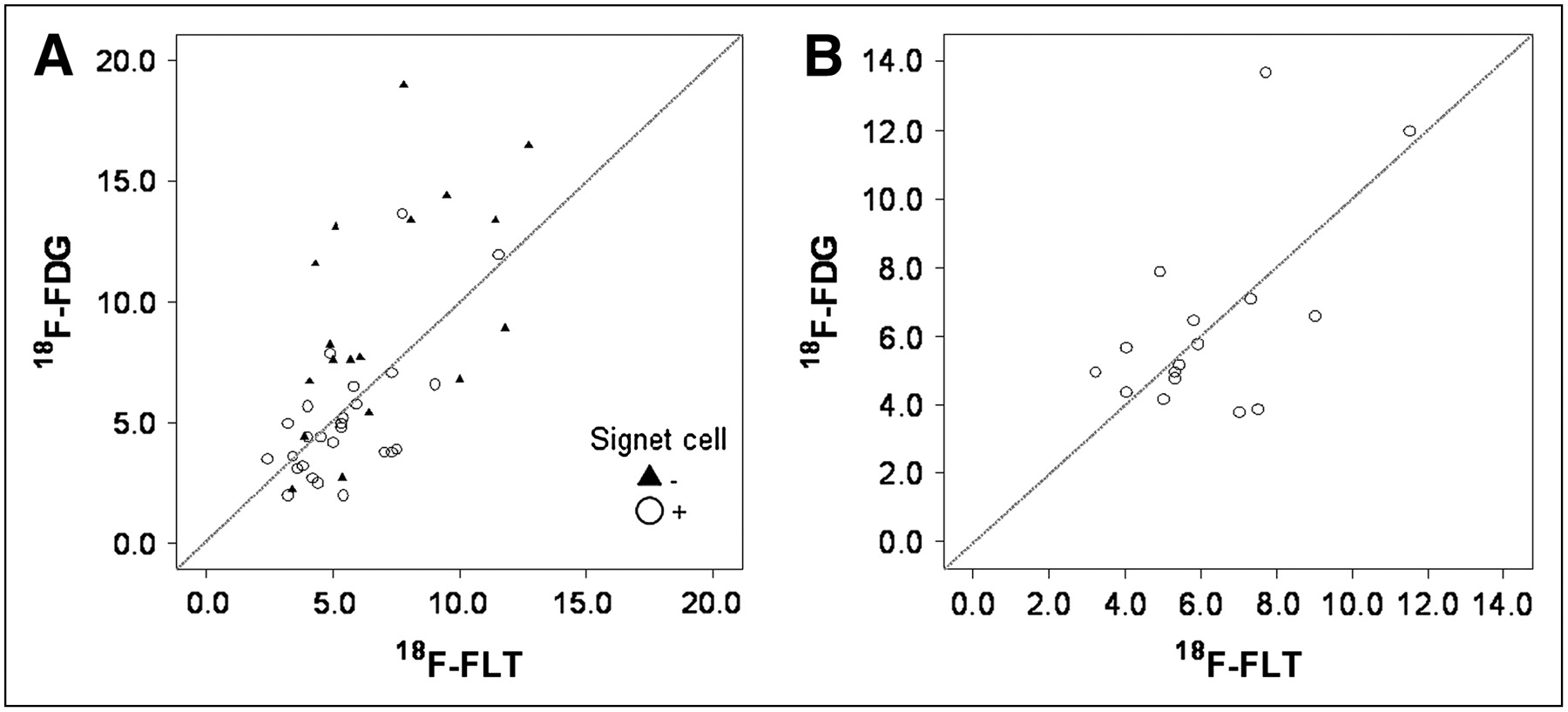
Correlation of SUV means for 18F-FLT and 18F-FDG in subgroup of 18F-FDG–positive patients (n = 31) (A) and subgroup of signet ring cell carcinomas positive for 18F-FDG PET uptake (n = 16) (B).

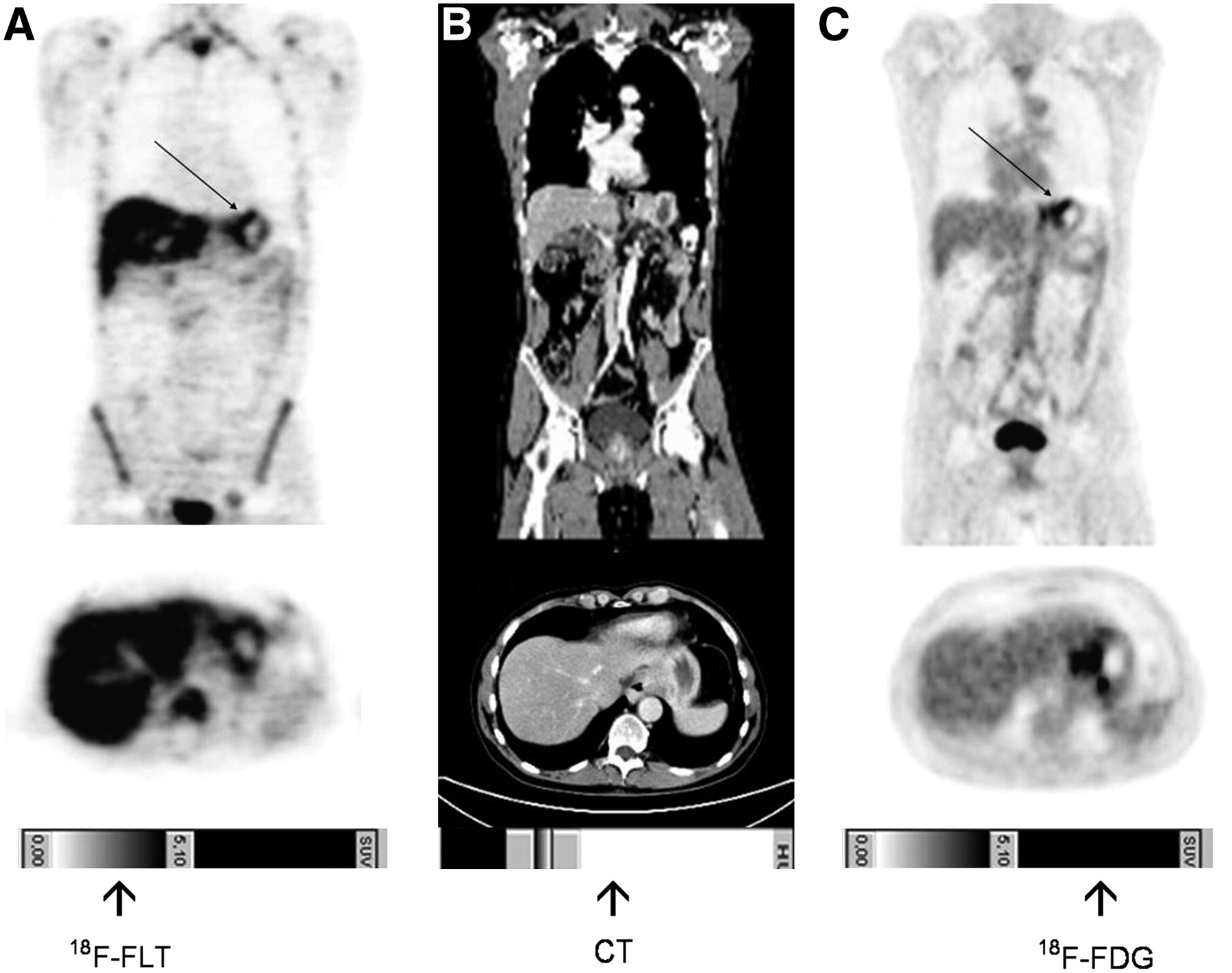
Coronal and transversal 18F-FLT PET (A), conventional CT (B), and 18F-FDG PET (C) views of patient with gastric cancer (linitis plastica, arrow).
DISCUSSION
This clinical study demonstrated the potential of 18F-FLT PET for imaging gastric cancer. In contrast to the standard radiotracer 18F-FDG, 18F-FLT was able to detect all locally advanced gastric cancers with sufficient contrast for quantification. Therefore, 18F-FLT may represent a superior radiotracer for visualization of stomach cancer, especially of histologic subtypes that frequently have low or no 18F-FDG uptake, as well as for response evaluation. Uptake of 18F-FLT in the malignant primary correlated significantly with the corresponding 18F-FDG uptake (r = 0.46); however, mean and maximum 18F-FDG SUV were significantly higher than the corresponding 18F-FLT values. This observation is in line with studies reporting higher uptake of 18F-FDG than of 18F-FLT in other solid tumors such as esophageal or lung cancer (14,20).
Interestingly, even 18F-FDG–negative tumors with signet ring cells or mucinous content were detected by 18F-FLT PET. Compared with tumors responding to neoadjuvant chemotherapy (as indicated by a rapid decrease in tumoral 18F-FDG uptake), signet ring cell–positive tumors are characterized by a different biological behavior resulting in lower response rates and impaired prognosis (21). Increased consumption of glucose is characteristic of most cancers and is in part related to overexpression of glucose transporters (22). As rationale for 18F-FDG–negative gastric tumors, it has been postulated that the low or absent 18F-FDG uptake in the nonintestinal subtype results from the high number of signet ring cells, leading to a reduced 18F-FDG concentration in the tumor. Another reason could be the lack of expression of the glucose transporter Glut-1 on the cell membrane of most nonintestinal gastric cancer tumors (23).
There was also a trend toward lower detection rates of 18F-FDG PET in the middle and distal thirds than in the proximal third of the stomach (P = 0.07, nonsignificant). This observation could be explained by the low or absent 18F-FDG uptake in the nonintestinal subtype resulting from the high number of signet ring cells. Compared with intestinal gastric cancer, nonintestinal gastric cancer shows a higher chromosomal stability, which might lead to a lower proliferation rate. Nonintestinal gastric cancer is characterized by a lower fractional allelic loss and a lower loss of heterozygosity being inversely correlated with the methylation rate (24). Nonintestinal tumors with a high methylation rate and low fractional allelic loss and loss of heterozygosity tend to have a worse prognosis than do intestinal tumors (24,25). Chromosomally stable tumors might show lower proliferative activity. Therefore, antiproliferative agents might be less effective, potentially leading to lower response rates in nonintestinal tumors.
In contrast to 18F-FDG, 18F-FLT PET specifically reflects activity of thymidine kinase 1, the key enzyme of the salvage pathway for producing thymidine monophosphate. The level of thymidine kinase 1 protein has proven to be an important determinant of 18F-FLT uptake in tumors. However, the detailed uptake mechanism remains to be determined. A recent study showed that 18F-FLT PET can be used to measure thymidylate synthase inhibition in tumors early after drug administration, indicating a potential use of 18F-FLT for early measurement of antiproliferative drug effects (26). There was a trend toward lower tumoral 18F-FLT uptake in nonintestinal than intestinal tumors, according to the Lauren classification. However, the presence of signet ring cells was the only histopathologic factor significantly influencing uptake of 18F-FLT, as was also shown previously for 18F-FDG (21).
Several limitations have to be considered when our results are transferred to the clinic. Our results apply to a specific group of patients with a high proportion of signet ring cell–containing tumors, reflecting a patient selection different from that of previous studies (21). However, the fact that our results were found exactly for this group of patients indicates that 18F-FLT PET may be used for imaging gastric cancer containing signet ring cells—a histologic subtype with a markedly reduced sensitivity on 18F-FDG PET. Furthermore, the impact of 18F-FLT PET for imaging locally advanced gastric cancers is rather limited considering that detection and diagnosis of gastric cancer remains the domain of conventional imaging modalities such as endoscopy, endoscopic ultrasound, and CT. However, studies investigating the role of 18F-FLT PET for monitoring therapy of gastric cancers may strongly influence clinical management.
Our study documents that 18F-FLT PET is a feasible tool for imaging tumors of an unfavorable histologic type (signet ring cell carcinoma) and low 18F-FDG uptake. 18F-FDG has been used successfully for treatment monitoring of adenocarcinomas of the esophagogastric junction and gastric cancers (14,20,21,27,28). However, some tumors have uptake insufficient to provide the image contrast needed for quantitative analysis of 18F-FDG PET. This pilot study provides the rationale for future use of 18F-FLT for treatment monitoring because all primaries could be visualized with 18F-FLT, suggesting that 18F-FLT PET can be used to tailor treatment to the chemosensitivity of an individual tumor.
CONCLUSION
In summary, this clinical study compared 18F-FLT PET with 18F-FDG PET for the detection of locally advanced gastric cancer. 18F-FLT PET had a higher sensitivity than 18F-FDG PET and might serve as a useful diagnostic adjunct for the quantitative assessment of proliferation. In the future, the addition of 18F-FLT PET to 18F-FDG PET could improve early evaluation of the response to neoadjuvant treatment of gastric cancer.
Acknowledgments
We appreciate the excellent contributions made by our colleagues Petra Watzlowik, Karin Kantke, and Michael Herz and the great support by Christine Praus and our technical staff members Brigitte Dzewas and Coletta Kruschke.
Footnotes
-
↵* Contributed equally to this work.
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 9, 2007.
- Accepted for publication September 6, 2007.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Fibroblast Activation Protein-Targeted PET/CT with 18F-Fibroblast Activation Protein Inhibitor-74 for Evaluation of Gastrointestinal Cancer: Comparison with 18F-FDG PET/CT
- The Predictive and Prognostic Value of Early Metabolic Response Assessed by Positron Emission Tomography in Advanced Gastric Cancer Treated with Chemotherapy
- Improving Patient Selection for 18F-FDG PET Scanning in the Staging of Gastric Cancer
- Early Determination of Prognosis by Interim 3'-Deoxy-3'-18F-Fluorothymidine PET in Patients with Non-Hodgkin Lymphoma
- Adjuvant Treatment for Gastric Cancer: Chemotherapy Versus Radiation
- PET Imaging of Proliferation with Pyrimidines