


Abstract
PET is a potentially useful modality for response analysis and prognosis prediction in patients with high-grade non-Hodgkin lymphoma (NHL). The thymidine analog 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) was recently introduced as a new tracer. 18F-FLT uptake correlates with tumor cell proliferation and is suggested to reflect early response to treatment. We performed a prospective study to evaluate the prognostic value of early interim 18F-FLT PET in patients with NHL. Methods: Patients with untreated NHL were enrolled between 2005 and 2007. Among them, 61 pairs of 18F-FLT PET images were obtained at baseline (pre), after 1 cycle of chemotherapy (interim), and at the end of all scheduled first-line chemotherapy (final). All 18F-FLT PET scans were interpreted by quantitative methods (maximum standardized uptake value [SUVmax] and mean standardized uptake value [SUVmean]). Receiver-operating-characteristic curve analysis was performed to define 18F-FLT PET positivity using a cutoff value predicting disease progression, relapse, or death. Survival outcome was measured by progression-free survival (PFS) and overall survival (OS) rates. Results: Receiver-operating-characteristic curve analysis of SUVmax for prediction of disease progression and death showed the highest area under the curve (AUC) in interim 18F-FLT PET scans (AUC of 0.841 for PFS and 0.834 for OS, with a cutoff of 1.86; P < 0.001), compared with pre and final 18F-FLT PET scans. The SUVmean in interim 18F-FLT PET scans also showed better prediction (AUC of 0.842 for PFS and 0.824 for OS, with a cutoff value of 1.65; P < 0.001) than pre and final 18F-FLT PET scans. Patients with an interim 18F-FLT PET SUVmax more than 1.86, who were defined as the interim PET-positive group, were associated with worse 5-y PFS and OS rates than the interim PET-negative group (for PFS: 52.0% vs. 80.7%, respectively, and P < 0.001; for OS: 56.2% vs. 81.4%, respectively, and P < 0.001). By multivariable analysis, the prognostic value of interim 18F-FLT PET positivity by SUVmax remained significant after adjustment with other prognostic factors (for PFS: hazard ratio, 7.82, 95% confidence interval, 1.65–36.96, and P = 0.009; for OS: hazard ratio, 5.55, 95% confidence interval, 1.47–33.77, and P = 0.014). Conclusion: In patients with aggressive NHL, early interim 18F-FLT PET is a significant predictor of PFS and OS. Early 18F-FLT PET imaging also has a potential to identify patients with delayed response and nonfavorable prognosis despite achieving a clinical complete response.
- positron emission tomography (PET)
- 18F-FLT
- non-Hodgkin lymphoma (NHL)
- standardized uptake value
- prognosis
PET with 18F-FDG has been widely used for staging and monitoring of malignant lymphoma (1,2). This technique is based on the principle that tumor cells are associated with increased glucose metabolism, compared with normal cells, and this modality is highly sensitive for detecting various tumor cells (3–5). The International Working Group response criteria for malignant lymphoma, which were previously based on CT data (6), were revised in 2007 to reflect the widespread use of 18F-FDG PET in response assessment (7).
Achievement of complete remission after first-line treatment is an important prognostic factor in patients with malignant lymphoma (8). However, a final response analysis performed after completion of all scheduled treatment does not modify the therapeutic strategy for high-risk patients based on their response to chemotherapy. The prognostic value of interim 18F-FDG PET has been investigated in patients with various types of malignant lymphoma (9–11), and recently the use of interim 18F-FDG PET after 2 cycles of rituximab-containing chemoimmunotherapy has been validated as a prognostic tool in patients with diffuse large B-cell lymphoma (DLBL) (12). However, some limitations of the technique, including nonspecific tracer uptake and certain difficulties with data interpretation, have emerged (13).
To improve the utility of early PET assessment, a new PET tracer, the thymidine analog 3′-deoxy-3′-18F-fluorothymidine (18F-FLT), has been introduced (14). The kinetics of 18F-FLT uptake in vivo reflect the level of thymidine kinase 1 activity and are thus highly associated with tumor cell proliferation (15). Previous data suggested the possibility of noninvasive tumor grading and early response assessments in patients with malignant diseases (16–21). The results suggested that 18F-FLT PET might predict outcomes more precisely than conventional methods in patients with non-Hodgkin lymphoma (NHL).
Therefore, we performed the present prospective study to evaluate the prognostic value of response analysis using 18F-FLT PET, particularly early interim 18F-FLT PET after 1 cycle of chemotherapy, in patients with NHL.
MATERIALS AND METHODS
Study Design and Population
Between 2005 and 2007, previously untreated patients with histologically proven NHL were prospectively enrolled in the present study at the National Cancer Center, Goyang, Korea. The study was designed to evaluate the prognostic value of interim response assessment using 18f-FLT PET after 1 cycle of chemotherapy in terms of disease progression and survival. Patients with disease of any stage, who were older than 18 y, of adequate performance status (Eastern Cooperative Oncology Group ≤ 3), and with adequate organ functions (serum creatinine ≤ 1.5 mg/dL, total bilirubin ≤ 1.2 mg/dL, liver enzymes ≤ 2 times the upper normal limit, and cardiac ejection fraction ≥ 45%) were included. Patients who had primary central nervous system lymphoma, secondary lymphoma after prior chemotherapy or radiotherapy, transformed lymphoma from another lymphoma subtype, or posttransplant lymphoproliferative disorder were excluded. Before chemotherapy, patients underwent baseline evaluation, including a physical examination, a blood test battery, bone marrow analysis, and imaging (CT and 18F-FDG PET scanning). An International Prognostic Index (IPI) value was calculated for all patients.
The objective of the present study was to evaluate the prognostic value of positive interim 18F-FLT PET results in terms of the outcomes of NHL. Clinical outcomes were defined as the 5-y progression-free survival (PFS) and overall survival (OS) rates. The study was approved by the Institutional Review Board of the National Cancer Center, Goyang, Korea, and all subjects provided written informed consent.
Treatment and response assessment were conducted as described below. All patients were treated with chemotherapy according to the pathologic diagnosis, age, performance status, and IPI score. Irradiation was sometimes used as adjuvant therapy after complete remission (CR) was achieved (in detail, early-stage DLBL who received 4 cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP) chemotherapy or bulky disease at diagnosis). The study protocol required an 18F-FLT PET scan at baseline (pre 18F-FLT PET), 3 wk after the first chemotherapy administration (interim 18F-FLT PET), and at the end of all planned induction therapy (final 18F-FLT PET). If indicated, postremission treatments including irradiation or high-dose chemotherapy with autologous stem cell transplantation were allowed after the final 18F-FLT PET scan was obtained. Patients were monitored regularly during the follow-up period using reference imaging studies such as CT and 18F-FDG PET scanning every 3 mo for 2 y and thereafter every 6 mo for 3 y.
18F-FLT PET Imaging and Analysis
18F-FLT was synthesized as described previously (22). Patients were injected with approximately 370 MBq of 18F-FLT (mean, 380.1; range, 326–444 MBq) without fasting before injection. All 18F-FLT PET images were obtained according to the PET/CT protocol approximately 60 min after injection (mean, 61 min; range, 53–69 min). Imaging was performed from the skull base to the proximal (Discovery LS PET/CT scanner; GE Healthcare). All images were calibrated with respect to the injected dose and patient weight. Noncontrast CT covering the region from the skull base to the upper thigh area was conducted during shallow breathing using a low-dose CT protocol for the attenuation map (90 mA, 140 kVp, 4.25-mm section width). Emission scans were obtained 60 min after intravenous administration of 18F-FLT, and the section width was 4.25 mm. The acquisition time was 5 min per bed position, and each image was reconstructed using ordered-subsets expectation maximization. The resolution of PET images from our scanner was 7–8 mm (full width at half maximum). We prepared 18F-FLT sufficiently often to ensure that no treatment schedule was delayed by more than 1 wk.
All 18F-FLT PET/CT images were reviewed using a dedicated workstation and software (AW; GE Healthcare), and uptake of 18F-FLT was assessed quantitatively. All 18F-FLT PET/CT scans were evaluated by 3 nuclear medicine physicians masked to clinical data and the results of other imaging studies. For semiquantitative analysis of tracer uptake, a region of interest was manually placed around the most prominent lesion (the lesion including the voxel with the highest 18F-FDG uptake), and a standardized uptake value was measured using the following equation to identify maximum standardized uptake value (SUVmax) and mean standardized uptake value (SUVmean): standardized uptake value (SUV) = 100 × (tissue radioactivity [Bq]/tissue weight [g])/(total injected activity [Bq]/body weight [g]). SUVmax was defined as the most prominent SUV visible in the scanned body, and SUVmean was defined as the average of the SUVs in the most prominent lesion with the circular region of interest of 10 mm in diameter. Agreement was reached for discordant cases of 18F-FLT PET/CT scans after the primary evaluation.
Statistical Analysis
To evaluate the prognostic value of 18F-FLT PET response analysis, we first calculated the cutoff level of residual 18F-FLT uptake that predicted relapse or disease progression of NHL using receiver-operating-characteristic curve analysis. SUVmax and SUVmean were measured on both the interim and the final 18F-FLT PET scans, and the area under the curve (AUC) values of each modality were compared to identify the levels that afforded the most precise predictions. 18F-FLT PET positivity was defined when the SUV uptake was higher than the calculated cutoff level.
The prognostic value of a positive 18F-FLT PET result was validated using the Kaplan–Meier method with the log-rank test. Survival outcomes were 5-y PFS and OS. PFS was defined as the interval from study enrollment to the date of death, relapse, or disease progression. OS was the time from enrollment to all-cause death. Cox’s proportional hazards model was used in multivariate analysis. All tests were 2-sided, and the significance level was set at 0.05. All statistical analyses were performed using SPSS 14.0 (SPSS Inc.).
RESULTS
Patient Characteristics and Outcomes
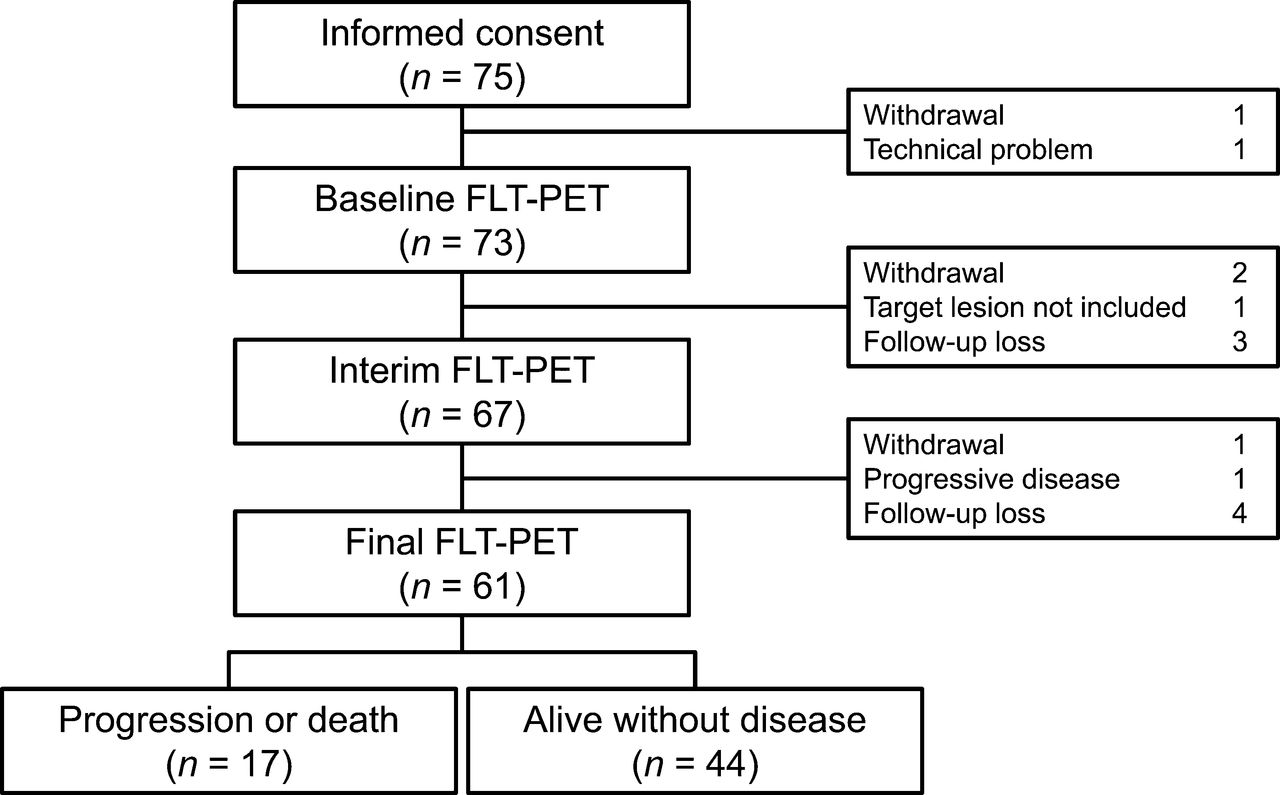
Informed consent was obtained from 75 newly diagnosed NHL cases during the study period. After enrollment, pre 18F-FLT PET could not be performed in 2 patients because of consent withdrawal by one patient and a technical problem with the other. The mean time difference between the date of consent and the pre 18F-FLT PET was 1.79 d (range, 0–10 d). Of the 73 (97.3%) patients who underwent pre 18F-FLT PET scans at diagnosis, 67 (89.3%) interim 18F-FLT PET scans were subsequently obtained after 1 cycle of chemotherapy. At the end of first-line chemotherapy, all 3 paired 18F-FLT PET scans, including final 18F-FLT PET scans, were available for 61 (81.3%) patients (Fig. 1).
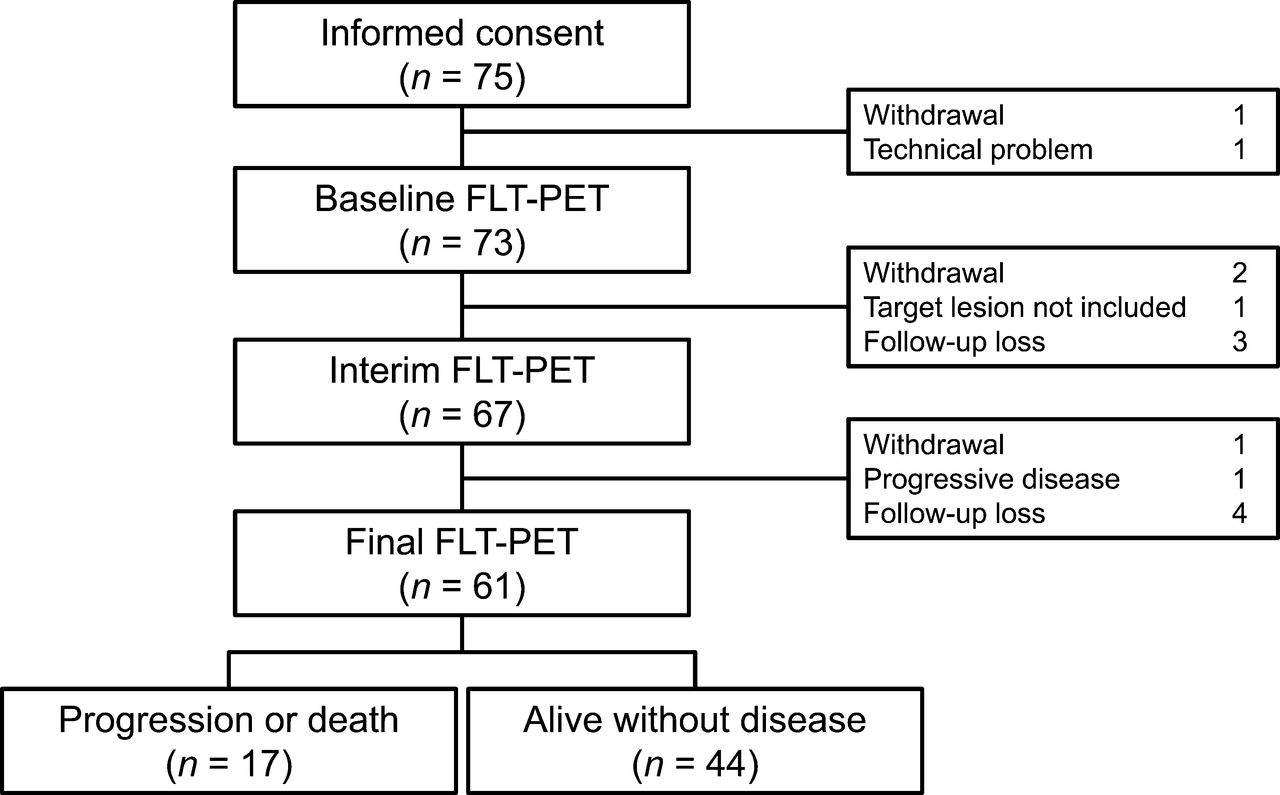
Consort diagram and clinical outcome of enrolled patients.
Data on these 61 patients were used in response analysis, and the patients’ characteristics are described in Table 1. The median age of the patients was 57 y (range, 29–80 y). Fifty-six patients (91.8%) had B cell lineage NHL, and 50 (82%) had the DLBL subtype. Fifty-four patients (96.4%) with CD20+ lymphoma received a rituximab-containing regimen as induction therapy. The median number of received chemotherapy cycles was 6 (range, 0–8). There were 20 (32.8%) patients with stage III–IV disease, and 13 patients (21.3%) had an IPI score of 3 or more. The final response to first-line induction chemotherapy based on reference methods (conventional CT or 18F-FDG PET) was available in all 61 patients, including 52 CRs (85.3%), 6 partial remissions (9.8%), and 3 progressive diseases (4.9%).
Characteristics of Analyzed Patients
After a median follow-up duration of 72 mo (range, 7.8–87.6 mo), 9 deaths were observed. All of these patients died of progressive disease. The 5-y PFS and OS rates of all enrolled patients were 71.4% and 77%, respectively.
Response Analysis of 18F-FLT Uptake
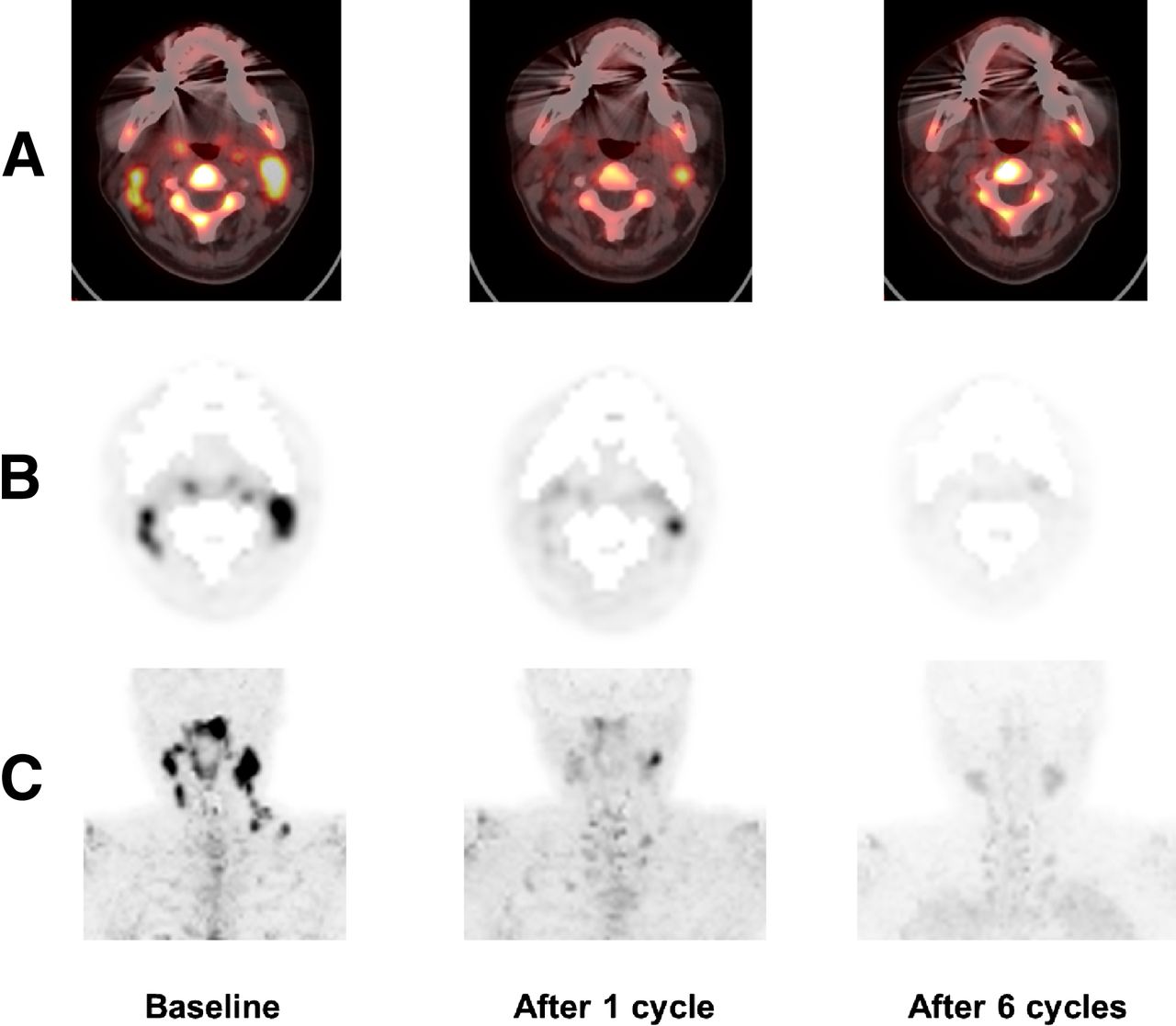
At baseline, the mean SUVmax of pre 18F-FLT PET was 8.21 (range, 1.03–26.49), and the SUVmean was 6.71 (range, 0.89–24.81). After 1 cycle of chemotherapy, the mean uptake was reduced to 2.68 of SUVmax (range, 0.46–15.98) and 2.16 of SUVmean (range, 0.38–11.14). Subsequently, the mean SUVmax fell further to 2.05 (range, 0.38–13.98) and SUVmean to 1.64 (range, 0.31–13.01) at the end of treatment of the 61 patients. Representative 18F-FLT PET images are shown in Figure 2.

Images of representative 18F-FLT PET scans. A 39-y-old woman with DLBL with involvement of multiple cervical lymph nodes (SUVmax, 7.7) achieved CR after induction chemotherapy. However, her interim 18F-FLT PET scan showed residual uptake (SUVmax, 4.6). She experienced relapse 16 mo after induction therapy and subsequently died because of disease progression. Corresponding sections of PET/CT fusion (A), axial (B), and maximum-intensity-projection 18F-FLT PET images (C) at different time points show regression of lymphoma. Nonspecific 18F-FLT uptake of bone was subtracted (B and C) to compare the mild residual 18F-FLT uptake after treatment. Subtraction was performed only in this figure.
When baseline 18F-FLT PET scans were compared with 18F-FDG PET scans, discrepancies were observed in 27 lesions, composed of twenty 18F-FLT–negative/18F-FDG–positive lesions and seven 18F-FLT–positive/18F-FDG–negative lesions. Of the twenty 18F-FLT–negative/18F-FDG–positive lesions, 7 were in mediastinal lymph nodes and 8 were caused by pneumonia, liver abscess, arthritis, or benign nodules. All other lesions were determined to be true lesions. Of the seven 18F-FLT–positive/18F-FDG–negative lesions, 4 featured irregular spinal uptake. The other 18F-FLT–positive/18F-FDG–negative lesions were not determined clinically to be either true or false.
Receiver-operating-characteristic curve analysis was performed to compare the utility of SUVmax and SUVmean detected on each 18F-FLT PET scan in the prediction of disease progression and death. The AUC values of residual SUVs predicting PFS and OS are described in Table 2. The AUCs derived from interim 18F-FLT PET were significantly higher than those at baseline and final 18F-FLT PET scans (P < 0.05 for all comparisons). The cutoff levels of residual SUVmax and SUVmean derived from the interim 18F-FLT PET were 1.86 and 1.65, respectively. The sensitivities and specificities of interim 18F-FLT PET positivity in predicting disease progression or death were 88.2% and 70.5% for SUVmax and 85.7% and 66.0% for SUVmean, respectively, using these cutoff levels. In addition, the positive predictive and negative predictive values were 53.6% and 93.9% for SUVmax and 60% and 94.4% for SUVmean, respectively.
AUC Values of 18F-FLT Uptake for Disease Progression or Death in Patients with NHL
The results of interim 18F-FLT PET analysis using SUVmax indicated that 33 (54.1%) patients achieved 18F-FLT PET negativity. At the end of first-line chemotherapy, the number of patients with negative PET results was increased to 42 (68.9%). Among them, 10 (16.4%) were slow responders who once showed positive residual SUVmax in interim 18F-FLT PET and subsequently achieved CR as assessed on the final PET (interim 18F-FLT PET–positive/final 18F-FLT PET–negative).
We also performed additional receiver-operating-characteristic analysis using the differences of SUVs between pre- and posttreatment 18F-FLT PET scans (supplemental data, section 1; supplemental materials are available at http://jnm.snmjournals.org). The diagnostic performances of interim Δ SUVmax and Δ SUVmean (the reduction of SUVmax and SUVmean from the baseline values) were better than the values of final Δ SUVmax and Δ SUVmean. The AUCs of interim Δ SUVmax and Δ SUVmean were 0.774 (P = 0.001; sensitivity, 82.4%; specificity, 70.5%; positive predictive value, 51.9%; and negative predictive value, 91.2%) and 0.745 (P = 0.003; sensitivity, 82.4%; specificity, 70.5%; positive predictive value, 51.9%; and negative predictive value, 91.2%) in the prediction of disease progression or death.
Survival Outcomes According to 18F-FLT PET–Based Response
Survival outcomes according to the 18F-FLT PET response are shown in Figure 3. Interim 18F-FLT PET positivity as revealed by residual SUVmax higher than the cutoff value was significantly associated with a worse 5-y PFS (51.98% vs. 80.70%, respectively; P < 0.001) and 5-y OS rates (56.24% vs. 81.44%, respectively; P < 0.001), compared with those of patients with negative interim 18F-FLT PET results. When we performed the same survival analysis using the residual SUVmean, patients with a positive interim 18F-FLT PET result also showed worse 5-y PFS (47.36% vs. 81.06%, respectively; P < 0.001) and 5-y OS rates (52.05% vs. 81.70%, respectively; P < 0.001) than did those with negative interim 18F-FLT PET. Interestingly, among responders who ultimately showed negative 18F-FLT PET results, slow responders who were interim 18F-FLT PET–positive/final 18F-FLT PET–negative had significantly worse 5-y PFS (56.3% vs. 93.6%, respectively; P < 0.001) and OS rates (57.1% vs. 93.8%, respectively; P < 0.001) than did early responders with interim 18F-FLT PET–negative/final 18F-FLT PET–negative results (Fig. 4).

Kaplan–Meier estimates of PFS and OS according to interim 18F-FLT PET (A and B) and final 18F-FLT PET (C and D) response analysis using SUVmax cutoff. There were significant differences in PFS and OS between 18F-FLT PET SUVmax–negative versus –positive patients (all P < 0.001).
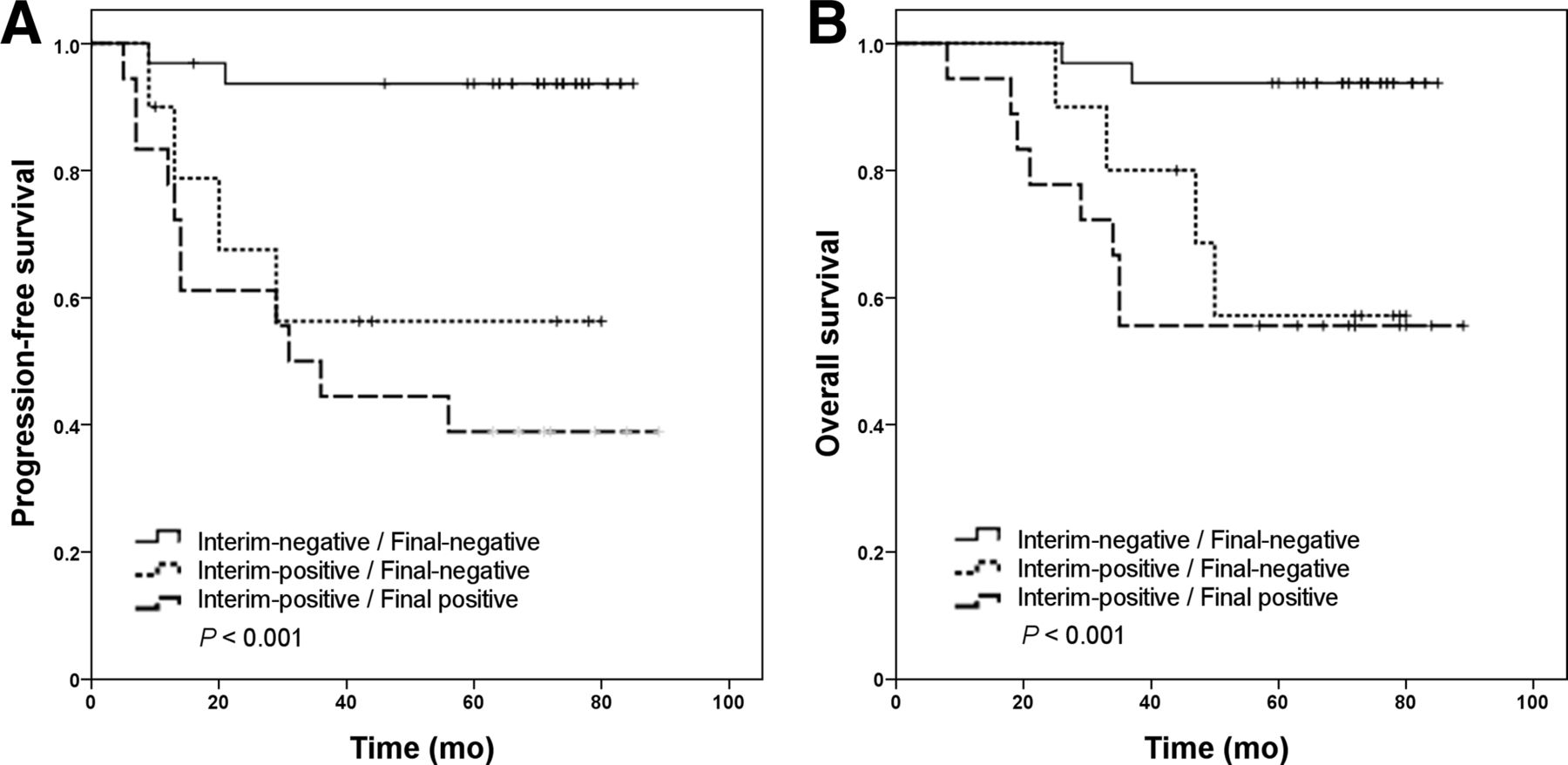
Kaplan–Meier estimates of PFS (A) and OS (B) according to type of responses. Patients who achieved PET CR after only 1 cycle of chemotherapy showed better PFS and OS than others (P < 0.001). Slow responders who were interim 18F-FLT PET–positive and final 18F-FLT PET–negative were also associated with poor PFS and OS.
To validate the prognostic value of residual 18F-FLT uptake detected on interim 18F-FLT PET scans, multivariable analysis was performed using factors that could have influenced patient prognosis and previously known prognostic factors (Table 3). A positive interim 18F-FLT PET result by SUVmax (an SUVmax higher than the cutoff of 1.86) remained significant after adjustment for both PFS (P = 0.009) and OS (P = 0.014). The hazard ratio associated with a positive interim 18F-FLT PET result was 7.82 (95% confidence interval, 1.65–36.96) for disease progression or death (PFS), and the hazard ratio for all-cause death (OS) was 5.55 (95% confidence interval, 1.47–33.77).
Multivariate Analysis of Interim 18F-FLT PET/CT Response by SUVmax for Disease Progression and Survival
DISCUSSION
The purpose of this study was to determine the prognostic value of the 18F-FLT PET response, and particularly that of early interim 18F-FLT PET analysis, in patients with NHL. We found that interim 18F-FLT PET discriminated patients with poor prognosis from others after only 1 cycle of chemotherapy. The 5-y PFS rates according to interim 18F-FLT PET results were 80.7% for PET-negative patients and 51.98% for PET-positive patients when the SUVmax cutoff of 1.86 was used.
Early identification of a high-risk group likely to experience relapse or progression during management of NHL has been studied for decades. Precise discrimination of high-risk patients using interim PET might enable modification of treatment strategies. However, no consensus on interpretation of interim PET data or application of such data in practice has yet been attained. The prognostic value of interim PET in patients with NHL, mainly those with DLBL using 18F-FDG, has been known since the early 2000s (23–25). These studies showed that patients with significant residual 18F-FDG uptake after 2–3 cycles of chemotherapy had 2-y PFS rates of only 0%–30%. However, the widespread use of rituximab in NHL patients is associated with false-positive 18F-FDG PET findings (13,26), suggesting a need for validation of the utility of interim 18F-FDG PET response analysis in the rituximab era. Recently, 2 studies on interim 18F-FDG PET in DLBL patients treated with rituximab-containing regimens were published (12,27). The authors showed that positive interim 18F-FDG PET had prognostic value in predicting PFS in the rituximab era. Casasnovas et al. (27) reported that the 2-y PFS rate was 57% in the PET-positive group using a quantitative method after 2–4 cycles of chemotherapy. Safar et al. (12) reported that the 3-y PFS rate was 47% in patients with positive PET results using visual analysis after 2 cycles of chemotherapy. Thus, the PFS rates of PET-positive groups seem to be higher than those reported in studies conducted before the rituximab era. In addition, false-negative 18F-FDG PET results have been reported in patients with specific tumor types, such as marginal zone lymphoma and peripheral T cell lymphoma, and such results have also been associated with tumor size, location, and presence of underlying diabetes (28).
With the introduction of 18F-FLT, this new tracer has been expected to improve the utility of early PET assessment of patients with malignant lymphoma, compared with 18F-FDG PET. 18F-FLT uptake has been known to correlate well with tumor cell proliferation and early reduction of tumor cells (15,29). We hypothesized that 18F-FLT uptake would reflect early cellular changes after the administration of chemotherapy.
In an effort to improve the utility of early PET assessment, modifications to the interpretation of PET scans have been proposed recently. These modifications include quantitative analyses using SUVs instead of dichotomous visual analysis. Casasnovas et al. (27) observed a significant association between reduction in the 18F-FDG SUVmax over 2 cycles of chemotherapy and prolonged survival in DLBL patients. Safar et al. (12) also reported that a reduction in SUVmax by more than 66% and negative visual analysis of an interim 18F-FDG PET scan, conducted after 2 cycles of a rituximab-containing regimen for DLBL, were significantly associated with prolonged PFS and OS. In our study, we investigated whether the 18F-FLT could provide an improved response analysis in patients with NHL using semiquantitative methods. The residual SUVmax on interim 18F-FLT PET was useful to predict both disease progression and death. The AUC for PFS was 0.841 and that for OS was 0.834, with a cutoff of 1.86.
No standardized guidelines for the interpretation of 18F-FLT PET scans, particularly in terms of interim response analysis, have been established. In the current study, we adopted quantitative methods using SUVmax and SUVmean for 18F-FLT PET interpretation. High residual 18F-FLT uptake (SUVmax and SUVmean) after chemotherapy was significantly associated with disease progression or death. To obtain more objective results, several other methods were introduced into our data analysis, such as the δ values of SUVmax and SUVmean (the differences between the values obtained on pre versus interim and final 18F-FLT PET/CT). Use of δ values reduced the predictability of both PFS and OS, despite of its complexity. We ultimately found that direct measurement of interim SUVmax and SUVmean showed the best results in terms of predicting clinical outcomes.
In this study, we performed interim 18F-FLT PET analysis early, because we hypothesized this modality might capture the sensitivity of tumor cells to chemotherapeutic agents. Similarly, Hermann et al. (29) investigated the early response of 18F-FLT uptake in high-grade NHL, showing that patients with a marked reduction of 18F-FLT uptake within 1 wk after the first dose of chemotherapy subsequently achieved a CR at the end of therapy. In our data, end-of-treatment 18F-FLT PET scans identified more responders who achieved PET CR than did interim 18F-FLT PET scans. Responders identified at the end of treatment consisted of early responders who were PET-negative after only 1 cycle of chemotherapy and slow responders who were interim PET-positive but subsequently achieved PET negativity after repeated chemotherapy cycles. The proportion of slow responders in this study was 16.4%. Unfortunately, these patients exhibited worse clinical outcomes, compared with early responders (5-y OS, 57.1% vs. 93.8%). Evaluating the early response to chemotherapy with 18F-FLT PET scans could identify slow and suboptimal responders with poor prognosis. It also discriminated patients with good prognosis. These results suggest the possibility of personalized treatment based on early response to chemotherapy. The slow responders might be rescued by risk-adapted treatment. However, whether intensified treatment based on early PET response could prolong survival outcomes has not yet been proven. Moskowitz et al. (30) applied a risk-adapted therapy strategy based on interim 18F-FDG PET responses; however, they could not validate the benefit of this therapy in patients with DLBL. In the future studies for risk-adapted therapy, we should make an effort to develop more effective treatment regimens than R-CHOP and to refine the PET-based response analysis. False-positive 18F-FDG PET results are problematic in many cases, and biopsy during active chemotherapy may often be difficult to perform. If interim 18F-FLT PET could noninvasively discriminate high-risk patients more precisely than 18F-FDG PET, it might help us provide individualized management to patients with NHL, although future prospective clinical trials are warranted.
It is difficult to assert that 18F-FLT is better than 18F-FDG because our study was not originally designed to compare 18F-FLT PET with 18F-FDG PET. Previously, a few studies have directly compared 18F-FDG PET and 18F-FLT PET scans. Kasper et al. (31) performed 18F-FDG PET and 18F-FLT PET scans simultaneously in NHL patients who had residual masses at the end of induction therapy. Nine (18.8%) discrepancies were evident, and 18F-FDG–positive but 18F-FLT–negative results seemed to be associated with prolonged OS, compared with 18F-FDG–positive/18F-FLT–positive results. However, the scans did not show any additional advantage of 18F-FLT PET over 18F-FDG PET alone in predicting survival outcome. In our study, 18F-FLT PET scans yielded accurate information on some patients with false-positive 18F-FDG PET lesions. However, it was difficult to define spinal involvement of NHL because of the physiologic uptake of 18F-FLT. It is necessary to develop conclusive consensus views on response analysis and interpretation of 18F-FLT PET data obtained from site-specific lesions.
Finally, some limitations of our study should be noted. Most of our patients had the DLBL subtype, and it is uncertain whether interim 18F-FLT PET analysis would work equally well in patients with T cell or indolent B cell lymphoma, compared with patients with DLBL. When we performed subgroup analysis using DLBL patient data only, the results were similar to those described above, indicating that response analysis based on interim 18F-FLT PET was feasible (supplemental data, section 2). In addition, we did not conduct histologic confirmation of PET-positive lesions (such confirmation was done in previous studies) (30,31). In practice, it is difficult to perform invasive procedures, such as biopsies, in patients with hematologic malignancies who are on active chemotherapy.
CONCLUSION
In patients with aggressive NHL, early interim 18F-FLT PET can provide superior prediction of PFS and OS. Early 18F-FLT PET imaging also has a potential to identify patients with delayed response and nonfavorable prognosis despite achieving a clinical complete response. Because this is the first study to evaluate the prognostic value of interim 18F-FLT PET, further studies to establish a standard protocol for 18F-FLT PET and interpretation criteria are needed. In the future, well-designed prospective trials will be required to validate the usefulness of interim 18F-FLT PET in modifying the treatment strategies in high-risk NHL patients and compare it with 18F-FDG PET/CT.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by the National Cancer Center grant (NCC-1110190-2, NCC-0510510). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Jan. 16, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 1, 2013.
- Accepted for publication August 16, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}