


Abstract
Current clinical and imaging tools remain suboptimal for early assessment of prognosis and treatment response in aggressive lymphomas. PET with 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) can be used to measure tumor cell proliferation and treatment response. In a prospective study in patients with advanced-stage B-cell lymphoma, we investigated the prognostic and predictive value of 18F-FLT PET in comparison to standard imaging with 18F-FDG PET and clinical outcome. Methods: Sixty-five patients were treated with an induction/consolidation regimen consisting of 4 cycles of R-CHOP-14 (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) followed by 3 cycles of ICE (ifosfamide, carboplatin, etoposide). 18F-FLT PET was performed at baseline and at interim (iPET) after 1–2 cycles of therapy. 18F-FDG PET was performed at baseline, after cycle 4, and at the end of therapy. The relationship between PET findings, progression-free survival (PFS) and overall survival (OS) was investigated. Results: With a median follow-up of 51 mo, PFS and OS were 71% and 86%, respectively. 18F-FLT iPET, analyzed visually (using a 5-point score) or semiquantitatively (using SUV and ΔSUV) predicted both PFS and OS (P < 0.01 for all parameters). Residual 18F-FLT SUVmax on iPET was associated with an inferior PFS (hazard ratio, 1.26, P = 0.001) and OS (hazard ratio, 1.27, P = 0.002). When 18F-FDG PET was used, findings in the end of treatment scan were better predictors of PFS and OS than findings on the interim scan. Baseline PET imaging parameters, including SUV, proliferative volume, or metabolic tumor volume, did not correlate with outcome. Conclusion: 18F-FLT PET after 1–2 cycles of chemotherapy predicts PFS and OS, and a negative 18F-FLT iPET result may potentially help design risk-adapted therapies in patients with aggressive lymphomas. In contrast, the positive predictive value of 18F-FLT iPET remains too low to justify changes in patient management.
Over the past decade, several changes in the management of diffuse large B-cell lymphoma (DLBCL) have occurred. For instance, the addition of the chimeric monoclonal antibody rituximab (R) to the standard CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) chemotherapy backbone has improved 5-y overall survival (OS) by approximately 15% (1,2). However, DLBCL shows substantial heterogeneity in its clinical behavior, and new management strategies, including the early identification of poor responders, are needed to improve patient outcome.
The role of interim PET (iPET) with 18F-FDG after a few cycles of chemotherapy in identifying patients with poor outcome has been investigated (3–9). Our group studied the utility of 18F-FDG iPET as part of a chemotherapy program consisting of induction with R-CHOP-14 followed by consolidation with ICE (ifosfamide, carboplatin, etoposide) (4). In that study, we biopsied sites with residual 18F-FDG uptake on iPET after 4 cycles of chemotherapy. All patients with a negative biopsy (or a negative iPET) received consolidation with 3 cycles of ICE, whereas patients with positive biopsy received RICE (rituximab, ifosfamide, carboplatin, etoposide) for 3 cycles followed by high-dose therapy and autologous stem cell rescue. Notably, this study demonstrated a high rate of false-positive 18F-FDG iPET, which was also described by other groups (10). In the current study we, therefore, investigated whether PET imaging with the proliferation marker 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) (11) after 1 or 2 cycles of therapy could provide better prognostic and predictive information than 18F-FDG PET does in patients with advanced-stage large cell lymphoma.
MATERIALS AND METHODS
Study Design and Patient Population
After providing written informed consent, 65 patients with advanced-stage, CD20-positive DLBCL, primary mediastinal large B-cell lymphoma, or follicular lymphoma grade 3B were enrolled in a prospective study (http://clinicaltrials.gov/show/NCT00712582). The Institutional Review Board approved the study. All patients were eligible for autologous transplantation and met inclusion criteria as reported previously (4). Patients underwent staging with contrast-enhanced CT (covering chest, abdomen, and pelvis) and 18F-FDG PET/CT (444 ± 44 MBq). Additional 18F-FDG scans were obtained after 4 cycles and 6 wk after completion of chemotherapy. Plasma glucose before 18F-FDG injections was 92 ± 15 mg/dL. 18F-FLT PET/CT (296 ± 30 MBq) was performed at baseline and at interim (cohort 1 postcycle 1, planned n = 30; cohort 2 postcycle 2, planned n = 30). Initial therapy for all patients consisted of dose-dense R-CHOP-14 for 3 cycles (rituximab, 375 mg/m2 days 1 and 3; cyclophosphamide, 1,000 mg/m2; doxorubicin, 50 mg/m2; vincristine, 1.4 mg/m2 [uncapped]; and prednisone, 100 mg oral daily days 2–6). Cycle 4 consisted of CHOP alone (same doses) and was followed by 18F-FDG iPET. Consolidation consisted of ICE chemotherapy (3) for patients with an initial proliferation index of less than 80%, whereas patients with proliferation index of 80% or more received augmented RICE (rituximab, 375 mg/m2 day1; etoposide, 200 mg/m2 every 12 h × 3 doses; ifosfamide, 5 g/m2/d by continuous infusion × 2; carboplatin area under the curve 5 d 3 [maximum, 800 mg]) for 3 cycles.
PET/CT Imaging and Analysis
Patients fasted for 6 h before radiotracer injection. PET/CTs from mid skull to upper thighs were obtained 60 min after injection on Discovery scanners (GE Healthcare) and were analyzed using the PET VCAR program (GE Healthcare). Volumetric regions of interest were placed in reference regions (mediastinal blood pool and normal liver) and over all sites of abnormal uptake in lymph nodes, soft-tissue organs, or bones. All scans were interpreted by 2 nuclear medicine physicians. For visual analysis of 18F-FDG iPET, we used a 5-point scale (12); grades 1–3 were considered normal. Grades 4 and 5 were considered abnormal, defining grade 4 as uptake considerably (∼20%) higher than liver and grade 5 as increase in number or intensity of 18F-FDG–avid lesions. Abnormal 18F-FLT uptake was defined as intensity higher than that in surrounding local background. 18F-FLT response was classified as grade 1, no residual uptake; grade 2, uptake less than or equal to local background; grade 3, uptake slightly greater than local background; grade 4, improvement from baseline with at least 1 lesion showing uptake clearly higher than local background; and grade 5, increase in lesion size, number, or intensity. Grades 1–3 were considered complete response, grade 4 partial response, and grade 5 progression. 18F-FLT analysis was restricted to lymph nodes and soft-tissue organs other than liver (high physiologic uptake in liver and bone marrow precludes reliable assessment of these organs). The metabolic tumor volume (volume of 18F-FDG–avid lymphoma, MTV) and total proliferative volume (volume of 18F-FLT–avid lymphoma, TPV) were defined using PET VCAR and applying a 42% threshold (13). ΔSUVmax ([SUVbaseline – SUVinterim]/SUVbaseline) was calculated by comparing a single disease site with the highest uptake in each scan (9) and comparing the summed SUV of the 5 most avid disease sites in each scan. Bone lesions were excluded from SUV-based analysis to enable head-to-head comparison of 18F-FDG and 18F-FLT findings.
Statistical Analysis
OS time was calculated from the start of treatment until the date of death or last follow-up. Progression-free survival (PFS) was calculated from the start of treatment until the date of disease progression, death, or last follow-up. Survival analysis was performed using the Kaplan–Meier method for dichotomous variables and compared using the log-rank test. Cox proportional hazards regression was used to assess continuous variables. For all iPET scans, patients were dichotomized by residual uptake: grade 1–3 versus grade 4 and 5. A sensitivity analysis was performed to identify the thresholds for change in SUV or SUVmax. This was performed using maximal χ2 test for PFS or OS. We used Kaplan–Meier analysis with the log-rank test to examine the relationship between PFS, OS, and the PET 5-point scale response. Because of limited power, multivariate survival analyses could not be performed. P values of less than 0.05 were considered significant. Analyses were performed using SPSS Statistical Software (version 22.0, 2013; IBM Corp.) or R software (version 3.0.1; R-Foundation for Statistical Computing).
RESULTS
Patient Characteristics
All 65 patients enrolled to the protocol were analyzed for PFS and OS (Table 1). Two patients progressed before 18F-FDG iPET, 1 patient progressed between iPET and end of planned therapy, and 1 patient developed drug-related toxicity. The remaining 61 patients completed treatment according to the protocol. Accordingly, 63 patients were analyzable for 18F-FDG iPET and 61 patients for 18F-FDG end-of-treatment PET. For logistic reasons (unavailability of radiotracer, scheduling difficulty in patients with rapidly progressive disease, or withdrawn consent), only 52 patients underwent 18F-FLT scanning at baseline, and 55 underwent interim 18F-FLT scanning.
Clinical and Demographic Characteristics
Baseline Imaging Characteristics
All patients had 18F-FDG–avid disease (Table 2). 18F-FLT uptake was always lower than 18F-FDG uptake, regardless of disease site. Discrepant findings (18F-FDG–positive/18F-FLT–negative) were observed for 90 of 2,860 regions (3%), mainly because disease in bones (69 regions) or liver (6 regions) was not detected on the 18F-FLT scan. Other regions of 18F-FDG–positive/18F-FLT–negative disease were noted in lymph nodes (n = 11), lungs (n = 3), and spleen (n = 1). However, all of these patients presented with multiple other disease sites that were clearly 18F-FLT–positive. There were no patients with disease recognized only on 18F-FLT PET/CT.
PET Imaging Findings
iPET/CT During Chemotherapy
Fifty-five patients underwent 18F-FLT iPET after 1 cycle (n = 27) or after 2 cycles (n = 28) of R-CHOP. Time between the end of cycle and 18F-FLT iPET was 9.8 ± 1.9 d for cohort 1 and 9.4 ± 1.2 d for cohort 2. Complete proliferative response (CPR) was observed in 29 patients (grade 1, n = 21; grade 2, n = 7; grade 3, n = 1), including 3 patients without baseline 18F-FLT PET: because aggressive lymphoma is follicular lymphoma–avid at baseline (14–16), lack of uptake in residual nodes on iPET was considered CPR. The other 26 patients showed partial response (grade 4, n = 22) or progression (grade 5, n = 4). CPR tended to be more common after cycle 2 (78% vs. 44% after cycle 1, Supplemental Table 1 [supplemental materials are available at http://jnm.snmjournals.org]). However, differences were not significant and therefore data were analyzed jointly. Eighteen patients showed diffusely increased splenic uptake attributable to recent granulocyte colony-stimulating factor administration. The median 18F-FLT ΔSUV was 77%.
On 18F-FDG iPET, performed 18 ± 1 d after cycle 4, complete metabolic response was noted in 38 patients (grade 1, n = 24; grade 2, n = 10; and grade 3, n = 4). Grade 4 (partial response) was noted in 24 patients and grade 5 (progression) in 1 patient. The median 18F-FDG ΔSUV was 89%. Among patients with 18F-FDG uptake grades 1–3, the median ΔSUV was 89% (range, −74% to −96%) as compared with 80% (range, +7.3% to −95%) in patients with grades 4 or 5. Similar numbers were derived when analyzing the 5 lesions with the most intense uptake at baseline and at interim in each patient (median ΔSUV of 76% and 88% for 18F-FLT and 18F-FDG, respectively).
Biopsy Findings and Patient Management After Interim 18F-FDG Scan
Twenty-one patients with persistent 18F-FDG uptake on iPET (SUV range, 2.1–27.4) underwent biopsy to verify imaging findings. Eleven of these sites were residual mediastinal or mesenteric masses. Residual disease was proven only in 2 patients (SUV, 5.3 and 27.4); the other 19 biopsies (SUV, 2.1–6.6) showed inflammation only. Only the 2 patients with a positive biopsy underwent high-dose therapy and autologous stem cell transplant; all remaining patients received ICE-based consolidation only. Only 6 of the 21 patients had a positive 18F-FLT iPET result (1 biopsy-positive, 5 biopsy-negative).
Survival Analysis and Assessment of Prognostic Factors
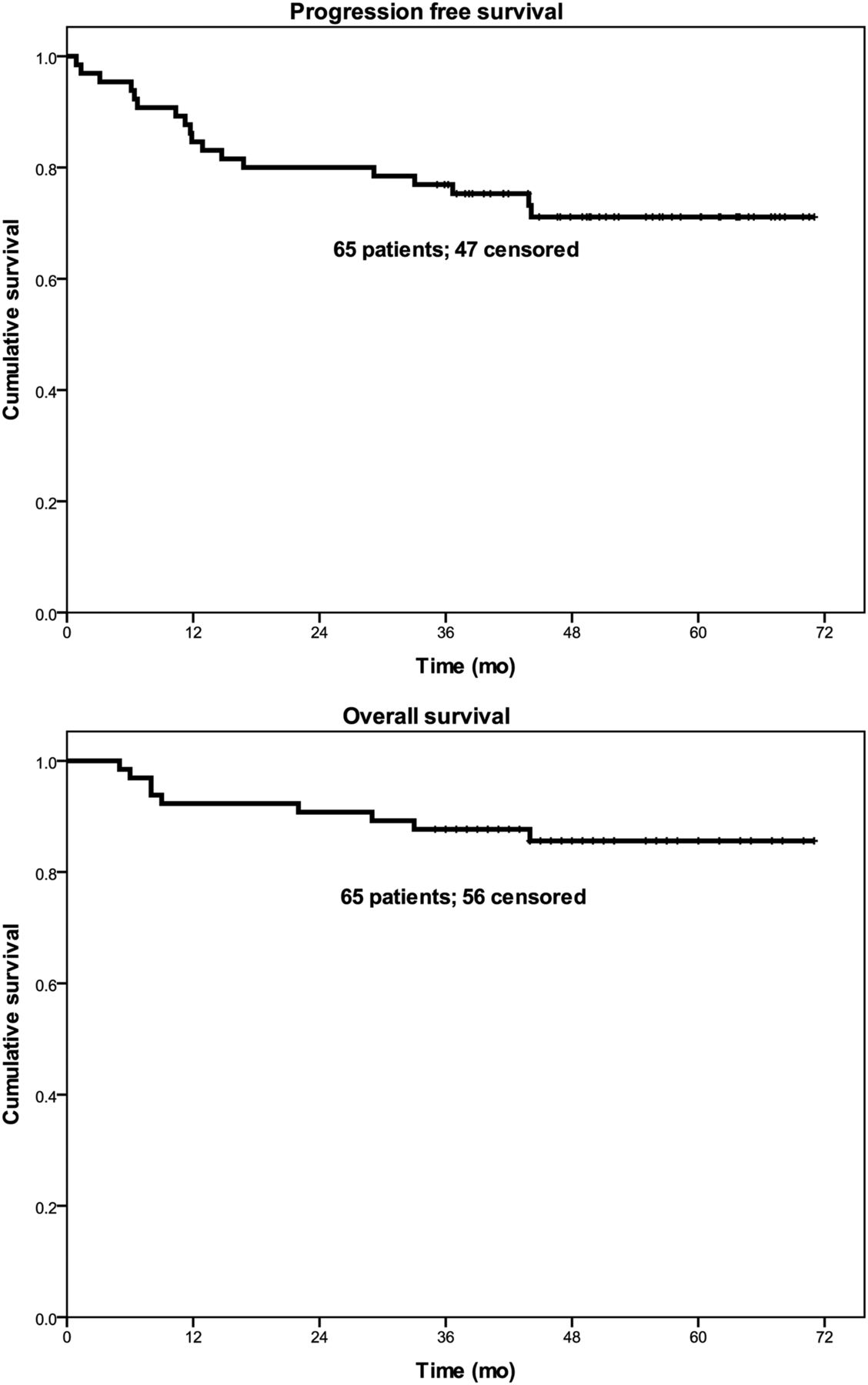
At a median follow-up for surviving patients of 51 mo (range, 35–71 mo), the Kaplan–Meier estimates for the proportion of patients alive and progression-free were 87% and 71%, respectively (Fig. 1). None of the clinical parameters were associated with outcome including age, sex, B symptoms, elevated lactate dehydrogenase, poor Karnofsky performance score, stage, extranodal site involvement (>1 site), Ki-67, or international prognostic index score.

PFS and OS for entire patient population.
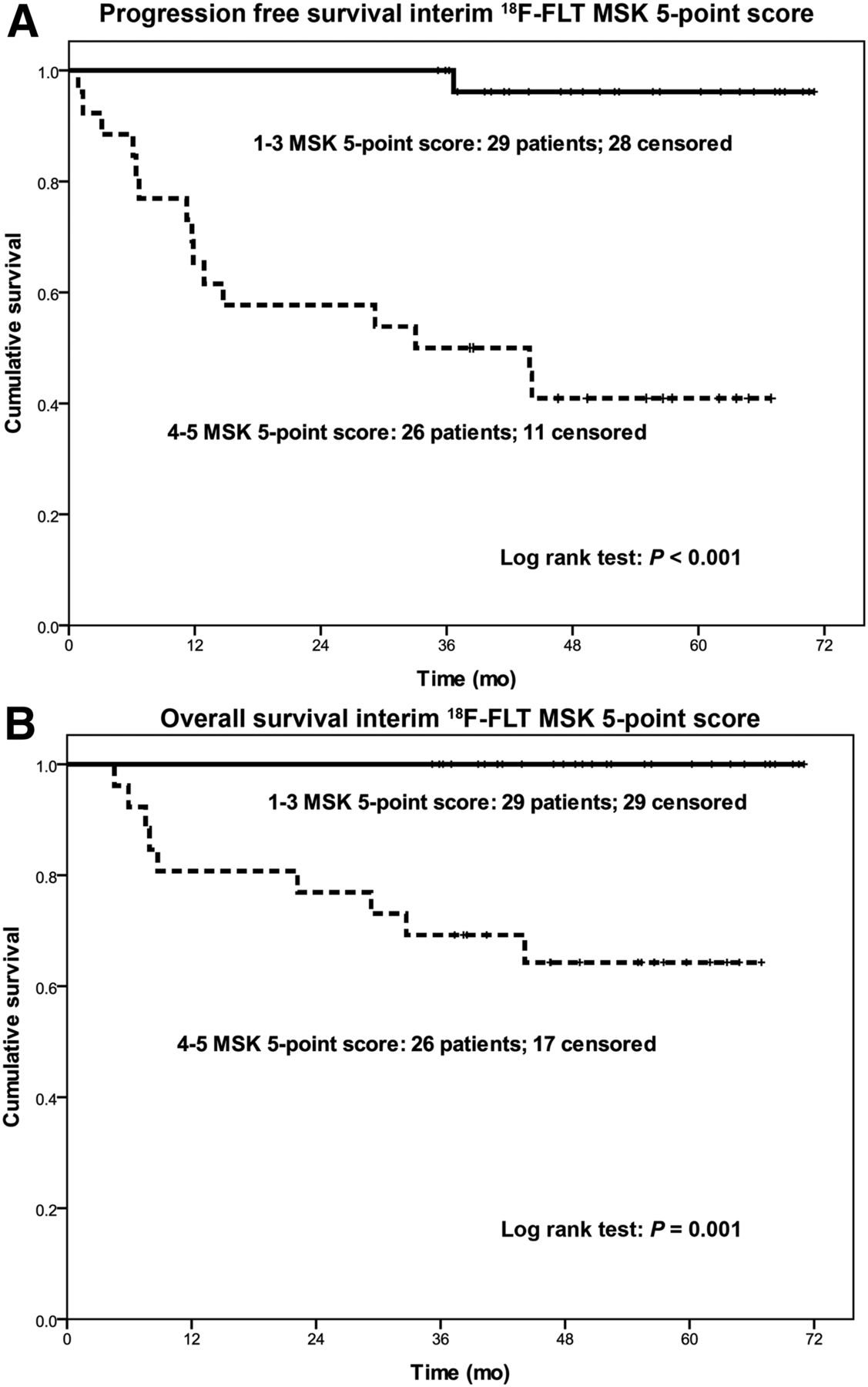
Findings on baseline 18F-FLT or 18F-FDG PET (in particular SUVmax, 18F-FDG MTV, and 18F-FLT TPV) were not associated with patient outcome. Further analysis was therefore focused on PET response parameters. Tables 3 and 4 show the relationships between response on 18F-FLT iPET and patient outcome. 18F-FLT uptake by visual analysis (grades 1–3 vs. grades 4–5) was predictive of PFS and OS (Fig. 2). A χ2 analysis (Table 4) revealed optimal cut-points for residual SUV (4.6) and ΔSUV (36%). Analysis of PFS according to these cut-points was highly predictive (Fig. 3). Nevertheless, in view of the small sample size these cut-points should be interpreted with caution and require further validation.
Univariate Analysis for PFS
Maximal χ2 Statistics for PFS

PFS (A) and OS (B) as stratified by 5-point visual score on 18F-FLT iPET. MSK = Memorial Sloan Kettering.

PFS as stratified by SUVmax on 18F-FLT iPET (A) and by 18F-FLT ΔSUV (B).
Regarding 18F-FDG iPET, residual uptake (visual grades 1–3 vs. grades 4–5) predicted PFS (Fig. 4) but not OS (not shown). To evaluate the impact of ΔSUV, we analyzed both PFS and OS at the median. There was a significant improvement in PFS (Table 3) and a trend to improved OS for patients with ΔSUV greater than the median. Similar results were obtained when analyzed by residual SUVmax on iPET: patents with SUVmax below median experienced better PFS and a trend to better OS. We then investigated whether a cutoff could be determined that optimized the prognostic significance of ΔSUV δ and SUVmax (Table 4). Of note, analyzing a total of 5 lesions in each pair of scans was no more informative or predictive than analysis confined to the single hottest lesion per scan. We also evaluated the prognostic value of the previously proposed postcycle 4 18F-FDG ΔSUV 77% (9). In our dataset, only 4 patients showed an ΔSUV of less than 77%. Therefore, neither this cutoff nor other proposed cutoffs for 18F-FDG iPET provided meaningful separation of prognostic groups. We then applied the estimated cut-point for 18F-FDG ΔSUV (83%) from our maximal χ2 analysis (M: 1.99, P = 0.34). Thus, whereas 18F-FDG ΔSUV predicted PFS in the univariate analysis, we could not identify a clear cutoff to separate prognostic groups because there was considerable overlap: ΔSUV was 89% in patients without progression (range, −74% to −97%) and 76% in patients who progressed (range, +7% to −94%).
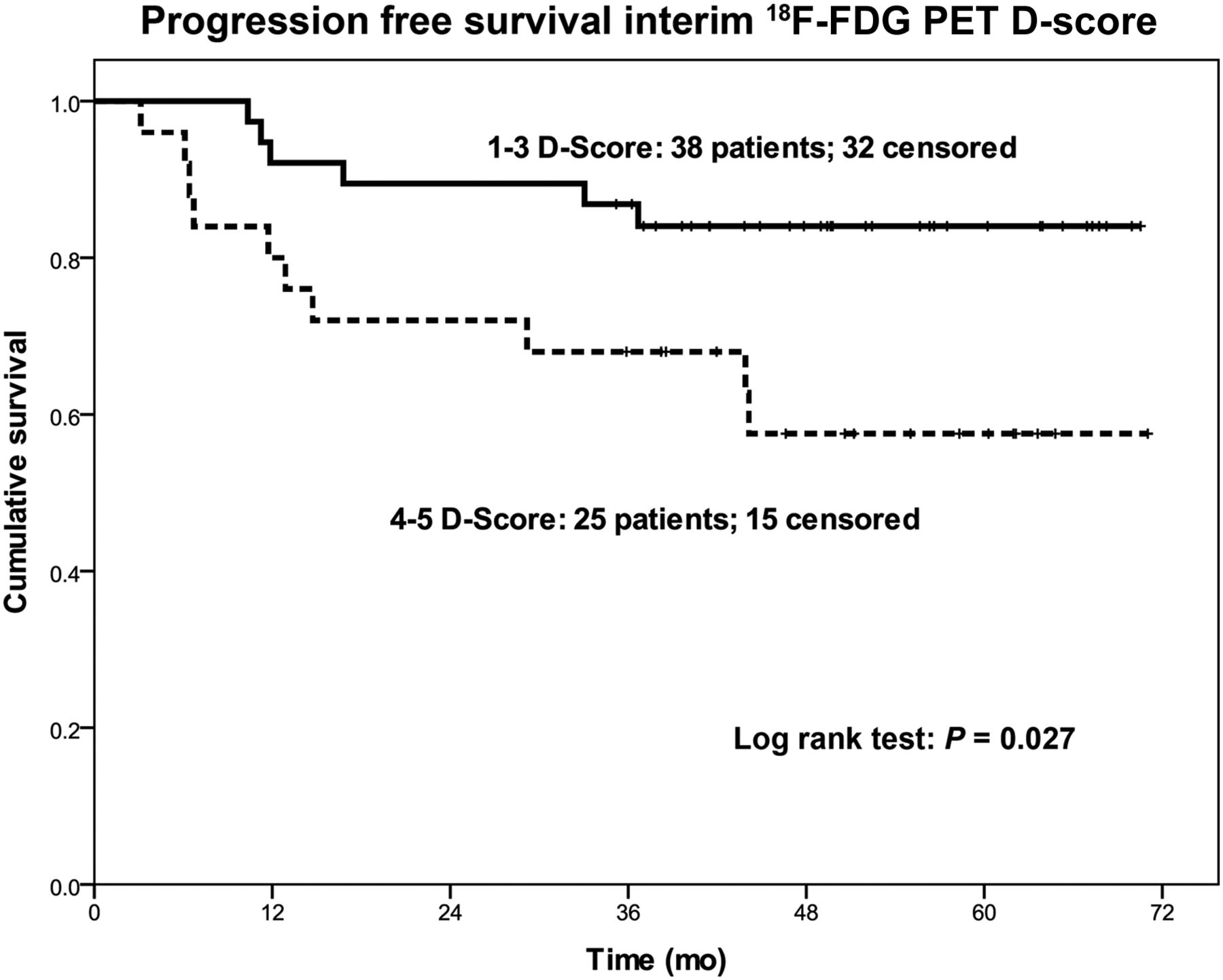
PFS as stratified by 5-point score on 18F-FDG iPET.
Among parameters analyzed for the end of treatment 18F-FDG scan, residual SUV and ΔSUV from baseline to final scan were both associated with both PFS (hazard ratio, 1.18 and 0.96, respectively, each P < 0.05) and OS (hazard ratio, 1.20 and 0.96, respectively, each P < 0.05). The final visual score was predictive of PFS (P = 0.03) but not OS.
DISCUSSION
In the current study, early 18F-FLT iPET had a high negative predictive value, with a negative scan clearly identifying patients with good prognosis. This information might help optimizing risk-adapted therapy for patients with advanced-stage aggressive lymphoma. In contrast, the positive predictive value (PPV) of 18F-FLT iPET, although somewhat better than the PPV for 18F-FDG iPET, remains too low to justify changes in patient management. Contrary to expectation and suggestions in the literature, volumetric parameters (18F-FLT TPV, 18F-FDG MTV) were not associated with patient outcome when our induction/consolidation treatment regimen was used.
18F-FLT is a proliferation marker for PET imaging (11), with high correlation between Ki-67 and 18F-FLT SUV reported in lymphoma (17). One might therefore expect high baseline 18F-FLT SUV or high 18F-FLT TPV to be markers of poor prognosis, but our findings do not support this hypothesis. However, visual inspection of residual 18F-FLT uptake on iPET predicted both PFS and OS. Quantitative parameters, such as residual 18F-FLT SUV and ΔSUV on iPET, also predicted patient outcome, although cut-points identified in χ2 analysis require independent validation in a larger dataset. The optimal timing of 18F-FLT iPET remains to be determined. Because no prior prospective study had identified an optimal time point for iPET with 18F-FLT, we investigated 2 early time points and studied 2 cohorts. CPR tended to be more common after cycle 2; thus, whereas complete resolution of uptake can be observed earlier, scanning after cycle 2 may be more meaningful for risk stratification. Regardless, early response assessment with 18F-FLT iPET may potentially inform patient management. For example, patients with negative 18F-FLT iPET can likely be cured with standard chemotherapy. In fact, if the high negative predictive value of 18F-FLT iPET is confirmed in future studies, some patients with high ΔSUV might potentially be cured with an abbreviated chemotherapy regimen, maintaining excellent outcome but reducing treatment-related toxicity. Thus, 18F-FLT PET may be useful to guide a de-escalation of therapy strategy. An early negative 18F-FLT iPET result may also be reassuring and help eliminate biopsies of sites with residual 18F-FDG uptake on iPET as this uptake is likely false-positive. In contrast, the PPV of 18F-FLT does not appear sufficiently high to justify any escalation of therapy strategy (including therapy with novel agents) without biopsy confirmation. Regardless, 18F-FLT iPET appears more accurate (in particular postcycle 2) in predicting patient outcome than 18F-FDG PET is. A recent multicenter study showed that early iPET with 18F-FDG after 1 cycle of therapy cannot safely discriminate prognostic groups in large cell lymphoma (18).
Experience with 18F-FLT PET in lymphoma is limited. In some studies (14,15), 18F-FLT ΔSUV on iPET after 1 cycle emerged as a predictor of survival, but baseline 18F-FLT SUV did not. An optimal cut-point was not reported. In another study including 50 patients with DLBCL (16), residual SUV greater than 1.9 and ΔSUV less than 65% after 1 cycle of R-CHOP identified patients with worse PFS and OS in receiver-operating characteristic analysis. We suggest caution when interpreting these suggested cut-points. Larger studies and standardization of time points and imaging techniques are required before any particular SUV number of ΔSUV can be applied for clinical decision making. It is difficult to compare our study to these prior investigations because of differences in patient population, lack of established criteria for interpretation of 18F-FLT iPET, and differences in statistical approaches to data interpretation. Nevertheless, the overall (albeit limited) evidence suggests 18F-FLT iPET as a promising marker for early response assessment in aggressive lymphomas.
18F-FDG iPET is used routinely to assess treatment response in DLBCL (9,19). In some studies, iPET provided meaningful prognostic information (3,5,8,9), but in other studies, the end-of-treatment scan proved to be more informative (6,7,20). We previously (4) reported a low PPV of 18F-FDG iPET, at least in part resulting from rituximab-induced inflammation in the R-CHOP regimen (10) and from the use of iPET interpretation criteria that are now obsolete (12,21). In the current study, 18F-FDG iPET again showed limited PPV, despite altering the drug regimen and timing of iPET regarding the preceding cycle and despite using updated iPET interpretation criteria. Higher PPVs were reported with standard regimens that are probably less effective (9), but 18F-FDG iPET remains a suboptimal test in the setting of an induction/consolidation regimen. In contrast, 18F-FDG PET performed after completion of chemotherapy provided better prognostic information.
Measuring ΔSUV may improve the predictive value and interobserver agreement in reading 18F-FDG iPET (5,8,9,22). Cutoffs of 66% for iPET after 2 cycles (5) and 70%–92% after 4 cycles (5,9,23,24) have been proposed. We could not confirm any of these cut-points in the setting of our induction/consolidation regimen. Although ΔSUV appears highly reproducible, visual assessment remains the first essential step in scan interpretation; ΔSUV should not be used in isolation.
There is growing interest in studying volumes of PET-avid disease (25–28). Direct comparison of published data is hampered by considerable heterogeneity in methodologies and patient populations. For instance, Sasanelli et al. (26) segmented 18F-FDG MTV in 114 patients with large cell lymphoma using a 41% threshold. Their raw data (median, 315 mL; range, 4–2,650 mL) are similar to our findings. However, whereas an MTV of 550 mL, derived from receiver-operating characteristic analysis, proved significant in their analysis, we did not find any association between median MTV and patient outcome. Similarly, 18F-FLT TPV did not prove prognostic in our analysis. It is conceivable that any prognostic value TPV might convey in other settings was overcome by the effectiveness of our induction/consolidation therapy regimen.
Our prospective study has some limitations. For logistic reasons, not all patients underwent 18F-FLT PET as planned, and 18F-FLT and 18F- FDG iPET were performed at different time points. Performing additional 18F-FDG iPET after 1 or 2 cycles was not feasible for logistic and financial reasons and because of dosimetry concerns. The overall sample size was also limited by current cost for 18F-FLT and funding. 18F-FLT was of limited use for disease in bone and liver (because of high physiologic uptake); nevertheless, 18F-FLT predicted for early failure in a setting where 18F-FDG did not (4). Although 18F-FLT is widely available from commercial vendors, it remains an investigational agent.
CONCLUSION
18F-FLT iPET was a clinically meaningful predictor of treatment response, which may potentially help design risk-adapted therapies in patients with aggressive lymphomas.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by core grant P30 CA008748. Ariela Noy received research and travel support from Pharmacyclics, Alison Moskowitz served as consultant to Merck and received research support from Seattle Genetics. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 30, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication September 11, 2015.
- Accepted for publication December 4, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}