


Abstract
The objective of this study was to compare 18F-3′-fluoro-3′-deoxy-l-thymidine (FLT) PET with clinical TNM staging, including that by 18F-FDG PET, in patients with non-small cell lung cancer (NSCLC). Methods: Patients with NSCLC underwent whole-body 18F-FDG PET and whole-body 18F-FLT PET, using a median of 360 MBq of 18F-FDG (range, 160–500 MBq) and a median of 210 MBq of 18F-FLT (range, 130–420 MBq). 18F-FDG PET was performed 90 min after 18F-FDG injection, and 18F-FLT PET was performed 60 min after 18F-FLT injection. Two viewers independently categorized the localization and intensity of tracer uptake for all lesions. All 18F-FDG PET and 18F-FLT PET lesions were compared. Staging with 18F-FLT PET was compared with clinical TNM staging based on the findings of history, physical examination, bronchoscopy, CT, and 18F-FDG PET. From 8 patients, standardized uptake values (SUVs) were calculated. Maximal SUV and mean SUV were calculated. Results: Sixteen patients with stage IB–IV NSCLC and 1 patient with strong suspicion of NSCLC were investigated. Sensitivity on a lesion-by-lesion basis was 80% for the 8 patients who received treatment before 18F-FLT PET and 27% for the 9 patients who did not receive pretreatment, using 18F-FDG PET as the reference standard. Compared with clinical TNM staging, staging by 18F-FLT PET was correct for 8 of 17 patients: 5 of 9 patients in the group with previous therapy and 3 of 8 patients in the group without previous therapy. The maximal SUV of 18F-FLT PET, at a median of 2.7 and range of 0.8–4.5, was significantly lower than that of 18F-FDG PET, which had a median of 8.0 and range of 3.7–18.8 (n = 8; P = 0.012). The mean SUV of 18F-FLT PET, at a median of 2.7 and range of 1.4–3.3, was significantly lower than that of 18F-FDG PET, which had a median of 6.2 and range of 2.8–13.9 (n = 6; P = 0.027). Conclusion: 18F-FLT PET is not useful for staging and restaging NSCLC.
PET, using 18F-FDG, has been accepted as a noninvasive metabolic imaging method for the staging of lung cancer (1). 18F-FDG uptake reflects glucose consumption (2). However, 18F-FDG is not a selective tracer, since it also accumulates in inflammatory cells. For instance, macrophages invade tumors and appear in inflammatory lesions, causing false-positive 18F-FDG PET results (3–5). Another problem is decreased uptake during hyperglycemia (6). Furthermore, because avidly taken up by the brain, 18F-FDG PET lacks sensitivity for imaging brain metastases.
In the search for more specific PET tracers, 18F-fluoro-3′-deoxy-3′-l-fluorothymidine (FLT) has been developed by Shields and Grierson. 18F-FLT may not have these drawbacks (7,8). This pyrimidine analog is phosphorylated by the enzyme thymidine kinase 1, which leads to intracellular trapping (8). Enzyme thymidine kinase 1 concentration increases almost tenfold during DNA synthesis, and 18F-FLT uptake may therefore accurately reflect cellular proliferation (9).
Few data are available on the clinical comparison of 18F-FLT with 18F-FDG for staging and restaging of non-small cell lung cancer (NSCLC) (10–12). The aim of the study was to compare 18F-FLT PET with clinical TNM staging in patients with NSCLC, including 18F-FDG PET.
MATERIALS AND METHODS
Patients
In this prospective study, patients with histologically or cytologically confirmed NSCLC who attended the outpatient department for various treatments were included. For all patients, disease was staged according to the TNM system before 18F-FLT PET (13). Clinical TNM staging was based on the findings of patient history, physical examination, bronchoscopy, chest radiography, CT, and 18F-FDG PET. All patients had been or were to be included in chemotherapy or radiotherapy protocols at the time of the inclusion. Organ functions such as those of liver, kidney, and bone marrow had to be within normal limits. Pregnant patients and patients with psychiatric disorders were excluded. The Medical Ethics Committee of the Groningen University Hospital approved the study protocol. All patients gave written informed consent.
Tracer Synthesis
18F-FLT was synthesized according to the method of Machulla et al. (14). 18F-FLT was produced by 18F-fluorination of the 4,4′-dimethoxytrityl-protected anhydrothymidine, followed by a deprotection step. After purification by reversed-phase high-performance liquid chromatography, the product was made isotonic and passed through a 0.22-μm filter. 18F-FLT was produced with a radiochemical purity of >95% and specific activity of >10 TBq/mmol. 18F-FDG was synthesized according to the method of Hamacher et al. by an automated synthesis module (15).
PET
All 18F-FLT PET scans were attenuation corrected and obtained on an ECAT EXACT HR+ (Siemens/CTI Inc.). Nine 18F-FDG PET scans were attenuation corrected and obtained on an ECAT EXACT HR+. The remaining 8 18F-FDG PET scans were non-attenuation corrected, of which 4 were obtained on an ECAT EXACT HR+ and 4 on an ECAT 951/31. It is our experience that the difference between the 2 cameras and between the use of attenuation-corrected and non-attenuation-corrected technique for 18F-FDG PET is negligible for staging NSCLC. Because 18F-FLT was the experimental tracer and our experience with 18F-FLT in lung cancer was limited, we used only attenuation-corrected images obtained with the EXACT HR+ camera. Patients were instructed to fast for at least 6 h before undergoing PET. They also were instructed to drink 1 L of water before being imaged, to stimulate 18F-FLT and 18F-FDG excretion from the renal calyces. For injection of the radiopharmaceuticals, a venous cannula was inserted into the forearm of the patient. From this cannula, a 2-mL blood sample was taken to measure the serum glucose level before each 18F-FDG PET scan. The median interval between 18F-FDG PET and 18F-FLT PET was 3 d, and the range was 1–63 d. Patients were injected with a median of 360 MBq of 18F-FDG (range, 160–500 MBq) and a median of 210 MBq of 18F-FLT (range, 130–420 MBq). Ninety minutes after 18F-FDG injection and 60 min after 18F-FLT injection, interleaved attenuation-corrected whole-body scanning was performed from crown to femur, with 3 and 5 min allowed per bed position for transmission and emission scanning, respectively. Data from multiple bed positions were iteratively reconstructed (ordered-subsets expectation maximization) into attenuated and nonattenuated 18F-FLT and 18F-FDG whole-body PET images (16).
Data Analysis
Two experienced PET physicians evaluated the 18F-FLT PET images independently and were unaware of patients’ clinical information, including 18F-FDG PET findings. The observers ranked the intensity of uptake in each lesion in comparison with background uptake in the lungs. The intensity was ranked as 0 (no visible uptake), 1 (slight increase in uptake), 2 (moderate increase in uptake), or 3 (strong increase in uptake). The observers reached a consensus on a lesion-by-lesion basis according to the same intensity scale for differently scored lesions. Thereafter, lesions ranked as 0 or 1 were grouped as hypo- or normometabolic lesions and lesions that ranked as 2 or 3 were grouped as hypermetabolic lesions.
To compare the staging properties of 18F-FLT PET with those of the clinical TNM system, the presence or absence of pulmonary, mediastinal, and distant hypermetabolic lesions was used. The mediastinal lesions were assigned according to the Mountain and Dresler classification of regional lymph nodes (17). The exact location of N1 and N2 lesions is difficult to assess on PET, and these lesions were therefore read in conjunction with CT after all PET scans had been evaluated. Lesions outside the mediastinum were described according to their anatomic locations.
After analysis of the lesions and the staging properties, standardized uptake value (SUV) was calculated from the attenuation-corrected 18F-FDG PET and 18F-FLT PET scans. The visually most hypermetabolic lesion on 18F-FLT PET images of each patient was compared with the corresponding lesion on transaxial 18F-FDG PET sections. The slice with the highest uptake was selected for ROI analysis. After selecting the plane with the maximum SUV, an ROI was drawn manually. ROIs were placed at the 70% contour of the maximal SUV in the tumor when possible. In other cases, ROIs were drawn manually. The SUVs of 18F-FLT PET and 18F-FDG PET were compared. Images were displayed on a Sun Microsystems workstation. ROI calculation was performed with Clinical Applications Programming Package (version 5; CTI).
Statistical Analysis
The degree of interobserver agreement for detection of 18F-FLT PET and 18F-FDG PET lesions was quantified with κ-statistics. For analyses of the intensity of each lesion, the values from the consensus readings were used. Sensitivity was calculated on a lesion level, using the number of pulmonary, mediastinal, and distant hypermetabolic lesions. Sensitivity is expressed as mean, with 95% coincidence interval (CI). Staging properties of 18F-FLT PET based on the presence or absence of pulmonary, mediastinal (expressed as N1 and N2 lesions), or distant hypermetabolic lesions were compared with the clinical TNM staging system. The Wilcoxon signed-rank test was used to compare maximal SUV and mean SUV between 18F-FDG PET and 18F-FLT PET. Two-tailed P values < 0.05 were considered significant.
RESULTS
Patients
From January 2002 until March 2003, 17 consecutive patients were included in this study. Their characteristics are shown in Table 1. Nine patients were included for primary staging and 8 patients were included for restaging. Seven of the restaged patients completed therapy before undergoing PET. Patient 3 was scanned during chemotherapy, because of clinical progression. All patients had histologically confirmed tumors, with the exception of patient 17, who had no malignancy but was included because of strong suspicion of malignancy. Primarily, histologic confirmation was difficult to obtain in this patient and therefore PET was performed to get more information.
Patient Characteristics and Detectability of Hypermetabolic Lesions on 18F-FLT PET as Compared with Standard 18F-FDG PET
Accuracy of 18F-FLT PET
18F-FLT PET produced easily interpretable images (Fig. 1). Most prominent physiologic uptake of the tracer was observed in liver, bone marrow, intestines, and bladder. Negligible and uniform tracer uptake was observed in the lungs. No uptake of tracer was observed in the brain, mediastinum, or myocardium.

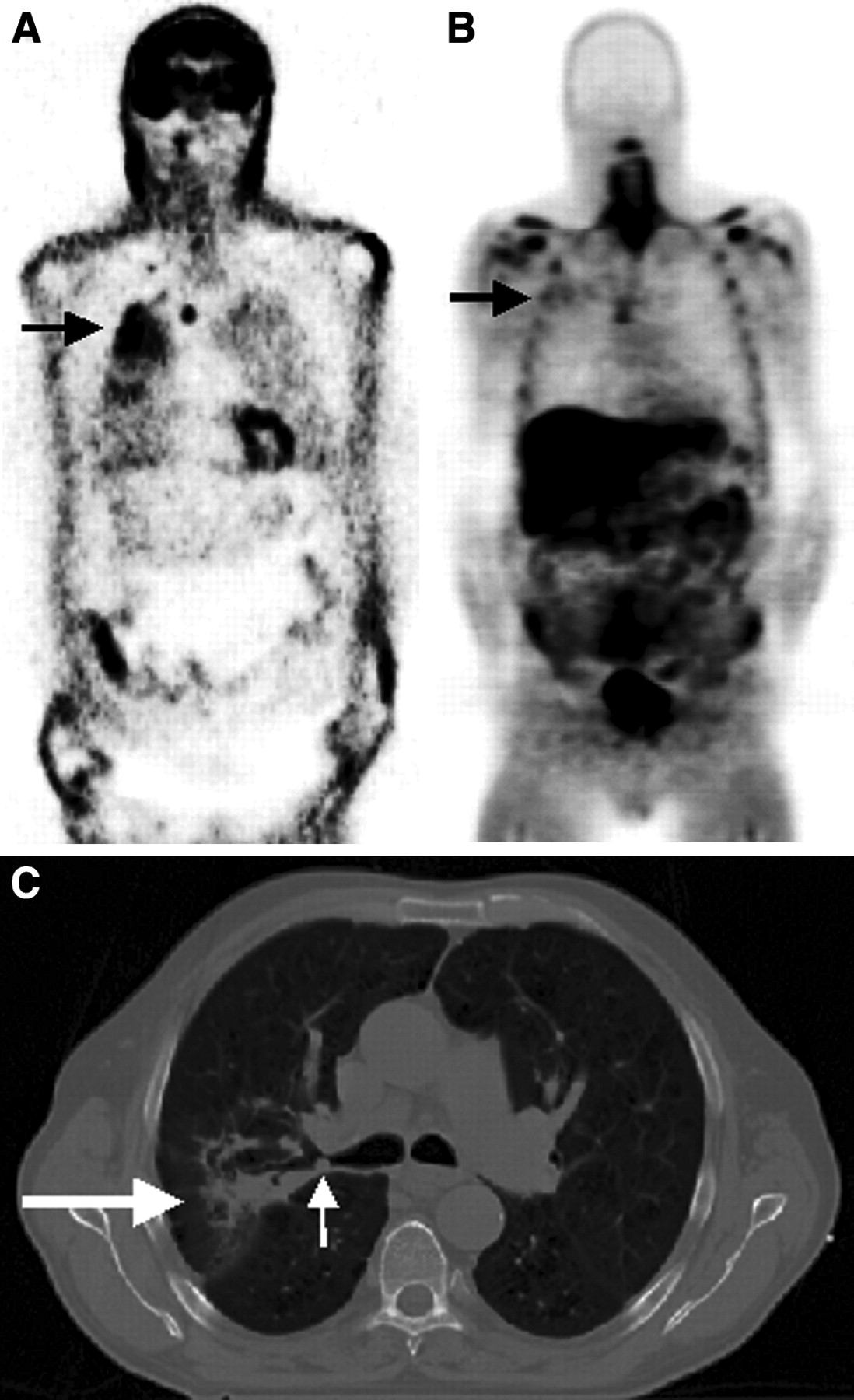
Coronal 18F-FDG PET image (A), 18F-FLT PET image (B), and CT image (C) of patient 11, diagnosed with squamous cell carcinoma in the right upper bronchus (small white arrow) and distally with suspected postobstruction pneumonia (large white arrow) on CT. Avid uptake of 18F-FDG can be seen in a pretracheal lesion and in the primary tumor, which is in an area of elevated uptake, probably postobstructive pneumonia (black arrow). Less avid uptake of 18F-FLT can be seen in the area of the tumor, and little 18F-FLT uptake can be seen in the suspected infected area (black arrow).The bone marrow of ribs and the shoulder bones, liver, and intestine show physiologic 18F-FLT uptake.
Interobserver agreement for the detection of lesions (κ) was 0.51 (SE = 0.06) for 18F-FLT PET and 0.55 (SE = 0.06) for 18F-FDG PET.
The overall sensitivity of 18F-FLT PET for the detection of all hypermetabolic lesions was 37% (95% CI, 29%–45%), compared with detection of those lesions on 18F-FDG PET (Table 2). The sensitivity of 18F-FLT PET for the detection of pulmonary, mediastinal (expressed as N1 and N2 lesions), and distant hypermetabolic lesions was, respectively, 50% (95% CI, 34%–66%), 56% (95% CI, 37%–75%), and 21% (95% CI, 12%–30%) using 18F-FDG PET as the reference standard. Sensitivity was calculated on a lesion-by-lesion basis for 18F-FLT PET using 18F-FDG PET as the reference standard. In the 8 patients without pretreatment, sensitivity was 80% (95% CI, 67%–93%), and in the 9 patients with pretreatment, sensitivity was 27% (95% CI, 3%–51%).
Maximum and Mean SUV and Wilcoxon Nonparametric Test
Compared with clinical TNM staging, staging by 18F-FLT PET was correct for 8 of 17 patients (Table 1): 5 of 9 patients in the group with previous therapy and 3 of 8 patients in the group without previous therapy.
Uptake of 18F-FDG was significantly higher than that of 18F-FLT, when expressed as maximal SUV and mean SUV. Maximal SUV was a median of 2.7 (range, 0.8–4.5) for 18F-FLT PET and a median of 8.0 (range, 3.7–18.8) for 18F-FDG PET (n = 8; P = 0.012). Mean SUV was a median of 2.7 (range, 1.4–3.3) for 18F-FLT PET and a median of 6.2 (range, 2.8–13.9) for 18F-FDG PET (n = 6; P = 0.027).
Additional 18F-FLT PET Findings
In patient 11, CT showed a T1 tumor suggestive of malignancy in the right upper lobe. On both 18F-FDG PET and 18F-FLT PET, mediastinal hypermetabolic lesions were detected (Fig. 1). On 18F-FDG PET and CT, the primary tumor was located within an area suggestive of postobstructive inflammation. On 18F-FDG PET, this area showed diffuse 18F-FDG uptake. In contrast, this inflammation was not visible on 18F-FLT PET, as could be expected. Patient 9 was treated with radiation therapy of the acetabulum. The field of radiation therapy and the remnant of the metastasis showed slightly decreased 18F-FLT activity. This lesion was ranked as hypometabolic, because the observers were unaware of the clinical history of the patient (Fig. 2). On 18F-FDG PET, this area appeared as a hypermetabolic lesion, although one must bear in mind that this appearance could have been caused by locally increased uptake in inflammatory tissue (Fig. 2). Patient 4 demonstrated a photopenic defect in the liver, which corresponded to a photopenic defect in a hypermetabolic liver lesion on 18F-FDG PET (Fig. 3). Vital tumor tissue in the margin cannot be discriminated from the surrounding tissue because of the high physiologic 18F-FLT uptake in the liver. This lesion was suspected to be a liver metastasis seen on CT.
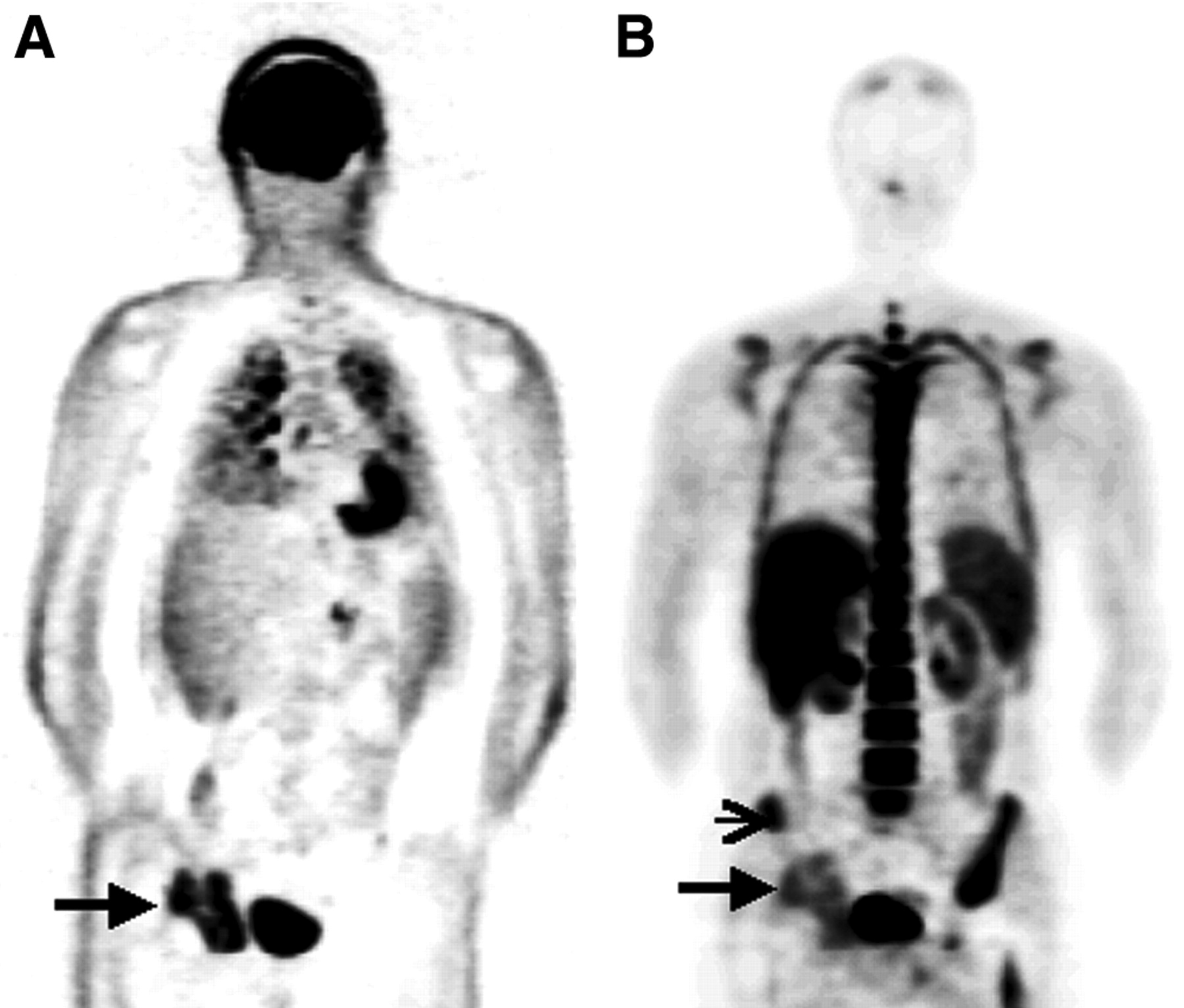
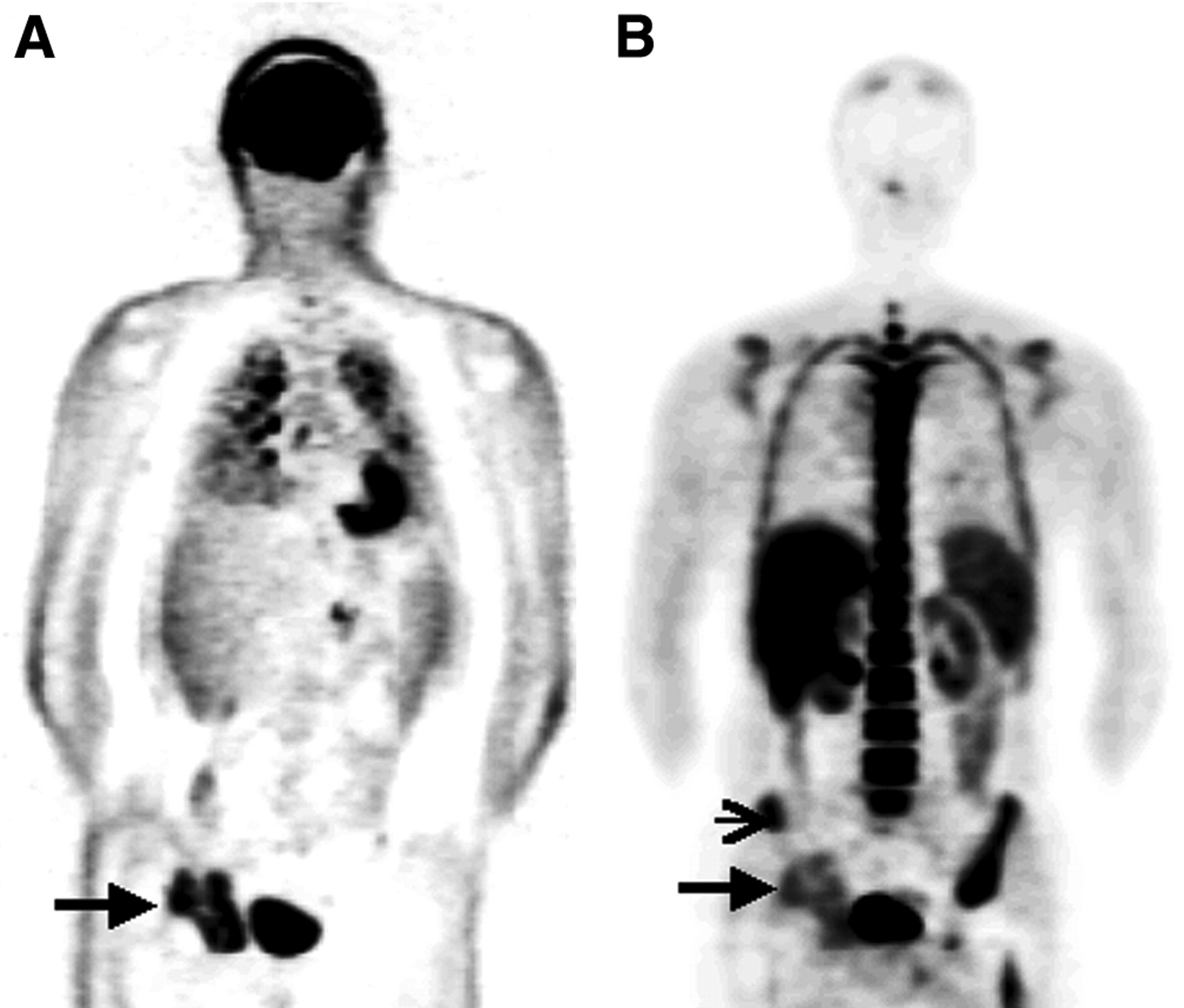
Coronal 18F-FDG PET image (A) and 18F-FLT PET image (B) of patient 9, with multiple lesions in both lungs on 18F-FDG PET and no lesions on 18F-FLT PET. Metastasis in the right acetabulum, which had been irradiated 1 wk earlier, is prominent on 18F-FDG PET (large arrow) but less intense on 18F-FLT PET (large arrow). In addition, irradiated bone marrow cranial of tumor has become metabolically inactive, as is seen on 18F-FLT as uptake less intense than that in nonirradiated bone marrow (small arrow).

Coronal and transaxial 18F-FDG PET (A), 18F-FLT PET (B), and CT (C) images of patient 4, diagnosed with a large tumor in the right lower lung and a large metastasis in the liver (large arrows on PET images). The liver metastasis, with a 4.5-cm diameter, can be seen on CT. 18F-FDG PET showed avid uptake in the lung tumor and liver metastasis, whereas 18F-FLT uptake was slightly less in the pulmonary lesion and almost absent in the liver metastasis.
DISCUSSION
Despite the potential of 18F-FLT for imaging proliferation of cancer, our results indicate that 18F-FLT is inferior to 18F-FDG for staging NSCLC. This finding is consistent with findings reported in 2 recently published abstracts and 1 article (10–12).
This study focused on the staging properties of 18F-FLT PET in patients with (foremost) disseminated NSCLC. The sensitivity of mediastinal and distant hypermetabolic lesions was low, resulting in incorrect staging in 9 of 17 patients (5 in the group that received pretreatment and 4 in the group that did not). Most of the visible 18F-FLT lesions were categorized as less intense than the comparable lesions on 18F-FDG PET. Other studies have confirmed that 18F-FLT PET is not an accurate tracer for staging NSCLC (10–12).
18F-FLT uptake is related to cellular proliferation, whereas 18F-FDG uptake is related to increased glucose metabolism. Because most cancer cells are metabolically active but fewer cells are proliferating, a higher net uptake of 18F-FDG than of 18F-FLT in the tumor can be expected. Besides tumor cells, many inflammation cells are usually present in malignant lesions, resulting in a higher 18F-FDG uptake than 18F-FLT uptake (3). Moreover, it is known that the 18F-FLT phosphorylation rate in vitro is about 30% of the phosphorylation rate of serum thymidine by thymidine kinase 1, possibly explaining the low 18F-FLT uptake in the tumor (18,19). In this study, of a small and heterogeneous group of patients, the maximal SUV of 18F-FLT ranged from 0.8 to 4.5, compared with 3.7 to 18.8 for 18F-FDG. Vesselle et al. also found low 18F-FLT uptake, with maximal SUVs ranging from 0.9 to 6.9 (20); Buck et al. found maximal SUVs ranging from 1.3 to 10.4 (12). Lesions with a low SUV can increase the risk for misinterpretation and thus influence the accuracy of staging with 18F-FLT PET.
Other mechanisms might explain the low sensitivity of 18F-FLT PET for the detection of NSCLC lesions. One explanation in this study could be that 9 patients received chemotherapy or radiation therapy before undergoing PET. The effects of chemotherapy on 18F-FLT uptake have been studied in vitro and in vivo in animals. These studies were performed on esophageal cells 24 and 72 h after treatment with 4 different types of chemotherapy and on mice with fibrosarcoma 24 and 48 h after treatment with 5-FU (21,22). The studies showed that the increase or decrease of 18F-FLT uptake in the tumor after chemotherapy depends on the type of chemotherapy. However, no clinical data are available to explain the decreased uptake of 18F-FLT in NSCLC patients with progression after first- and second-line chemotherapy. In the 8 patients who did not receive previous therapy, the results for staging were also poor, concordant with the preliminary results of Yap et al., who found a poor sensitivity for 18F-FLT PET in untreated NSCLC patients as well (10). On one hand, a decrease of 18F-FLT after therapy could be a major advantage for 18F-FLT PET over 18F-FDG PET and should not be interpreted per se as a lack of sensitivity. On the other hand, the group of pretreated patients showed clinical progression of disease, indicating a lower sensitivity for 18F-FLT PET. The ideal situation would be to obtain pathologic confirmation of the lesions, to correlate the cellular activity with 18F-FLT uptake.
CONCLUSION
Our study indicated that not only pulmonary lesions but also mediastinal and distant metastatic lesions are not well identified by 18F-FLT PET. Therefore, staging with 18F-FLT PET in patients with NSCLC is not recommended.
Acknowledgments
This research was funded by Dutch Cancer Foundation grant 2000-2299.
Footnotes
Received Feb. 29, 2004; revision accepted Apr. 29, 2004.
For correspondence or reprints contact: David C.P. Cobben, MD, PET Center, University of Groningen Hospital, P.O. Box 30.001, 9700 RB Groningen, The Netherlands.
E-mail: D.C.P.Cobben{at}pet.azg.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Differential 18F-FDG and 18F-FLT Uptake on Serial PET/CT Imaging Before and During Definitive Chemoradiation for Non-Small Cell Lung Cancer
- Monitoring Tumor Response to Therapy with 18F-FLT PET
- Imaging Surrogates of Tumor Response to Therapy: Anatomic and Functional Biomarkers
- Imaging of Cell Proliferation: Status and Prospects
- A Multicenter Clinical Trial on the Diagnostic Value of Dual-Tracer PET/CT in Pulmonary Lesions Using 3'-Deoxy-3'-18F-Fluorothymidine and 18F-FDG
- 18F-FLT PET in Hematologic Disorders: A Novel Technique to Analyze the Bone Marrow Compartment
- PET Evaluation of Lung Cancer
- Functional Imaging in Lung Cancer