


Abstract
Some new radiotracers might add useful information and improve diagnostic confidence of 18F-FDG imaging in tumors. A multicenter clinical trial was designed to investigate the diagnostic performance of dual-tracer (18F-FDG and 3′-deoxy-3′-18F-fluorothymidine [18F-FLT]) PET/CT in pulmonary nodules. Methods: Fifty-five patients underwent dual-tracer imaging in 6 imaging centers using the same models of equipment and standardized protocols. The images were interpreted by a collective group of readers who were unaware of the clinical data. The diagnostic performance using either tracer alone or dual-tracers together, with or without CT, was compared. The histological diagnosis or clinical findings in a 12-mo follow-up period served as the standard of truth. Results: In 16 patients with malignant tumor, 16 with tuberculosis, and 23 with other benign lesions, the sensitivity and specificity of 18F-FDG and 18F-FLT were 87.5% and 58.97% and 68.75% and 76.92%, respectively. The combination of dual-tracer PET/CT improved the sensitivity and specificity up to 100% and 89.74%. The 3 subgroups of patients could be best separated when the 18F-FLT/18F-FDG standardized uptake value ratio of 0.4–0.90 was used as the threshold. Conclusion: By reflecting different biologic features, the dual-tracer PET/CT using 18F-FDG and 18F-FLT favorably affected the diagnosis of lung nodules.
It has been known for years that 18F-FDG PET is of little value in certain types of tumors in spite of its wide acceptance in clinical oncology. One of the major shortcomings of 18F-FDG was its nonspecific uptake by some benign lesions (1). Therefore, several alternative PET tracers were developed and tried to complement 18F-FDG. Among them 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) is receiving greater interest because it is an analog of thymidine and its uptake reflects cellular proliferation. In vitro and in vivo studies had shown a higher uptake of 18F-FLT by the proliferating tumors (2,3). In a study on non–small cell lung cancer, a correlation was found between 18F-FLT uptake and MIB-1 monoclonal antibody cytochemical staining of nuclei (4). In another study, Buck et al related the increased 18F-FLT uptake exclusively to malignant tumors (5). However, to the best of our knowledge, 18F-FLT has not been investigated comprehensively in clinical settings. We recently conducted a randomized, blinded, prospective multicenter clinical trial (MCCT) on PET/CT of pulmonary nodules using both 18F-FDG and 18F-FLT. The aims of this trial were (a) to verify the diagnostic performance of 18F-FDG, 18F-FLT, and dual-tracer imaging, (b) to determine the possible clinical advantage of dual-tracer PET/CT, and (c) to test the reliability and objectivity of the diagnostic criteria established in the trial.
MATERIALS AND METHODS
General Description of Study
This 2-y multicenter clinical trial was designed by a special task group consisting of nuclear medicine physicians, statisticians, Good Clinical Practice (GCP) staff, and law workers. The first half-year was dedicated to the staff training, preparation and printing of data sheets, case reporting forms, standard of operational protocol (SOP), and other documents. The clinical imaging and data analysis took place in the next 1.5 y. Seven medical centers participated in the trial. One center acted as the organizer, taking the responsibility for collecting, verifying, and centrally processing data. The other 6 centers imaged the patients. To ensure the integrity of the data and the objectivity of the evaluation, the images acquired and processed using the standardized protocols and quality control—as well as the data recorded in the normalized forms—were collected by the organizing center, where a workstation had been installed for centralized processing. The images were interpreted in a randomized, blinded, collective reading, and the consensus diagnosis was compared with the standard of truth. The study protocol had been approved by the regional or hospital medical ethic committees.
Patient Enrollment
Patients entered the study in a sequential order. The inclusion criteria included (a) radiologic evidence of a pulmonary nodule or nodules(≤3), (b) no definite diagnosis, (c) no specific treatment before the study, (d) no significant dysfunction or disorder of major organs as suggested by laboratory or clinical signs (e.g., blood glucose < 6.16 mmol/L, alanine aminotransferase < 40 U/L, and urea < 7.50 mmol/L), (e) willingness to follow the study protocols and to give written consent for participation in the trial, and (f) possible clinical outcome expected within the foreseeable duration of follow-up. The age and sex of the patients were of no concern in this trial.
The exclusion criteria included (a) diagnosis already defined, (b) severely ill or with metabolic abnormalities such as hyperglycemia, (c) unlikely to comply with the study protocols, and (d) unable to provide necessary clinical data. A patient's data would be excluded from the final analysis if a question existed on the quality of either radiotracer or PET/CT scan or the diagnosis was still in doubt at the time of final collective image reading.
Equipments and Acquisition Parameters
A similar model of PET/CT scanner (Discovery ST; GE Healthcare) and the same kinds of cyclotron (MiniTrace; GE Healthcare) and synthesizer (TracerLab FxFN; GE Healthcare) were used for PET/CT and radiotracer production in this trial. An obligatory standardized quality-control program was followed by all imaging centers and was subject to the organizer's inspections. To protect the patients from undue radiation dosage, a low-dose CT scan was acquired with the following settings: 120 kV, 100∼250 mAs with automatic adjustment, 0.8-s rotation, 1.25-mm collimation, and a pitch varied according to the geometry of the CT detector (4, 8, or 16 slices). The PET scanner has a 15.7-cm axial field width and a spatial resolution of 4-mm full width at half maximum at 1 cm from the center. PET images were acquired in 3-dimensional mode, with 2.5 min per bed and 3 or 4 bed positions covering the entire chest. In some cases, whole-body 18F-FDG imaging was performed from the bottom of the pelvis to the chin. The images were reconstructed in a Fourier rebinning iterative algorithm. Delayed imaging with similar acquisition parameters was recommended whenever possible.
Radiopharmaceuticals
Both 18F-FDG and 18F-FLT were automatically synthesized in each imaging center. The raw materials and agents for the synthesis were purchased by the organizer from the same supplier and delivered to each center. Both syntheses and quality control for every preparation of the pharmaceuticals strictly followed the SOPs and were subject to inspection. The labeling yield, radiochemical purity, and specific radioactivity of the product were checked and recorded after each production. The products had to meet certain criteria—for example, the radiochemical yield must be >10% and the radiochemical purity must be >95%, to be used for imaging.
Imaging Protocols
Each patient was imaged twice using 18F-FDG and 18F-FLT within 7 d. The order of 18F-FDG or 18F-FLT scanning of each patient was determined randomly by a binary code produced by a computer. The patient was asked to fast over 4 h and to rest for 15 min before administration of 300∼400 MBq radioactive tracers. The images were acquired at 60min after injection. On the basis of the clinical situation and the patient's agreement, some patients had a delayed scan at 120 min after injection. Within 7 d, the whole procedure was repeated using the alternative radiopharmaceutical.
Image Interpretation
The CT images were displayed as 5-mm cross-axial slices. The morphologic features of the nodule(s) were checked—such as the size, density, cavity, calcification, notch on margin, spiculated margin or plural contraction, and so forth—and the CT value was assessed. The PET images were visually inspected with the maximum standardized uptake value (SUVMAX) determined from a circular region of interest (ROI) over the entire lesion. The uptake of a lesion was also scored in the following manner. In the case of 18F-FDG, 0 = no uptake; 1 = uptake lower than that of the mediastinum; 2 = uptake equal to or greater than that of the mediastinum but lower than that of the liver; 3 = obvious uptake higher than that of the liver; and 4 = very strong uptake. For 18F-FLT, 0 = no uptake, 1 = barely visible uptake, 2 = uptake lower than half the value of the thoracic vertebrae, 3 = obvious uptake similar to that of the vertebrae, and 4 = very high uptake.
The differential threshold for malignancy was set as SUVFDG ≥ 2.5, scoreFDG ≥ 2 and SUVFLT ≥ 1.4, scoreFLT ≥ 1. A lesion would be classified as malignant if uptake of both 18F-FDG and 18F-FLT or SUV and score were above the threshold, and the uptake of 18F-FLT was lower than that of 18F-FDG.
In cases of >1 lesion, the maximum scores and SUVs assessed among all lesions were chosen as the representative ones. The results in this trial were presented thereafter on a patient basis rather than on a lesion basis.
Data Collection and Verification
The original copies of working sheet and data record for each patient were sealed individually and, along with each patient's image data, sent to the organizing center over the Internet or by means of a CD-ROM. All sets of the serially numbered forms were required to be sent back to the organizing center whether they were or were not used. No correction or modification was allowed on the original records. After completion of the trial, the following datasets were collected from every center:
Two original copies of PET/CT working sheet, one for each imaging-session.
Two packages of raw image data from the dual-tracer PET/CT imaging.
The original follow-up records, with the date and type of surgical procedure and the pathologic diagnosis or the date and findings on follow-up.
The original copies of radiopharmaceutical production sheet, with the information on the production, quality control, and the raw material and agents used for each synthesis.
The signed consent form from every subject.
A summary of all cases, successful or failed, with the relevant information and explanations.
A summary of the execution of the MCCT by each imaging center.
A group of physicians, physicists, radiochemists, administrators, and inspectors in the organizing center verified all data before further processing. Any noncompliance with the MCCT protocols resulted in exclusion of the patient's data. Forty patients were eventually excluded from the final analysis because of unsatisfactory image quality (n = 5), failure in 18F-FLT synthesis (n = 29), or incomplete follow-up data (n = 6). Only 55 patients passed the data verification in the final analysis.
Collective Image Reading
Two sessions of blinded, collective image reading were carried out in this trial. The first session was organized in the sixth month after the initiation of the trial with 3 independent readers who had a CT or PET professional background. The purpose of the first reading was to verify the interpretation criteria. The final reading session took place on completion of the trial with an expanded team of readers. Only the results of the final reading session were analyzed and reported in this article.
Nine readers took part in the final collective reading. Four had professional CT backgrounds and the other 5 had professional nuclear medicine backgrounds. All readers were responsible for the primary PET/CT image interpretation in their own imaging centers. They had 1∼4 y working experience with PET/CT when the trial began.
In the collective reading, the images were reconstructed and assessed using the central workstation. Every patient's images were read 7 times using different strategies—18F-FDG, 18F-FLT, CT alone, 18F-FDG + 18F-FLT, 18F-FDG + CT, 18F-FLT + CT in pairs, and, finally, the combination of 18F-FDG + 18F-FLT + CT. In each round of reading, the present order of the patients' images was randomized and the heading of images was masked before viewing. The readers read all images unaware of any patient's information. The images were projected onto a screen. The display window and angles were adjusted as reader(s) requested assistance from an independent operator. No discussion was allowed among readers; each reader had to make his or her own judgment on each subject and score the images. The recording sheet of every reader was collected before the next round of reading. The imaging diagnosis was determined by a consensus reached by at least 5 of 9 readers, and the corresponding score was determined by averaging. A ratio of SUVFLT/SUVFDG was also calculated in the collective reading. On completion of the final collective reading, the data were available to the readers, and the results were statistically analyzed in light of the standard of truth.
Endpoint and Standard of Truth
The endpoint of this trial was determined as either the pathologic evidence obtained from surgical processes or the clinical conclusion derived from the therapeutic response or from imaging or laboratory findings in follow-up over 1 y after imaging. Therefore, the standard of truth was the histologic diagnosis or the validated clinical evidence derived at the end of 12-mo follow-up period.
Statistical Analysis
Commercial (SPSS11.0) and dedicated (MINITABLE for 6 Sigma; GE Healthcare) software packages were used for the statistical analysis. The comparison on the diagnostic performances of image interpretation strategies and the correlation between SUVs and scores were analyzed. A statistician took an active part in the design, data check, and final analysis in this trial.
RESULTS
Clinical Trial
The first patient in this MCCT was imaged in January 2006, and the follow-up of the last patient was completed by June 2007. Among 55 patients entering the final analysis (Table 1), 33 were males and 22 were females (age range, 17- to 82-y-old). There were 28 patients with a solitary pulmonary nodule and 27 with 2 or 3 nodules. The size of the nodules ranged from 6 to ∼110 mm, with the majority of lesions < 30 mm (n = 35). Because the 6 imaging centers covered wide geographic areas in China, with populations of different living habits and environment, the underlining diseases of our subjects were quite heterogeneous. The final diagnosis included 16 lung cancers, 16 tuberculoses, and 23 other benign lesions (inflammation, pseudotumor, granuloma, and other benign conditions). The diagnosis was confirmed via surgical processes (operation or biopsy) in 27 patients or via other clinical processes in 28 patients. No side effects were reported with either radiopharmaceutical or in PET/CT scanning.
Summary of Subjects
18F-FDG Images
A positive uptake of 18F-FDG was noted in nearly all lesions (Fig 1A). The uptake varied in intensity, with a SUVMAX of 0.75∼16.0 and corresponding scores of 0∼4. The mean SUV ± SD in patients with a malignancy (n = 16) was 8.13 ± 3.69 (range, 2.0∼16.0), and the score was 3.12 ± 0.86 (range, 1.22∼4.0), higher than that of tuberculoses (TB) (n = 16) and other benign diseases (n = 23). The corresponding values in the latter 2 groups were 5.71 ± 2.90 (range, 1.24∼12.79), 2.73 ± 0.70 (range, 0.89∼3.89), and 4.71 ± 0.74 (range, 0.75∼16.0), 1.96 ± 1.33 (range, 0.61∼4.0), respectively. ANOVA revealed a significant difference between groups in both SUV (F2,52 = 4.583, P = 0.015) and score (F2,52 = 6.338, P = 0.006). The Games–Howell test suggested that significant difference existed only between tumor and other benign lesions in both SUV (P = 0.021) and score (P = 0.005). There was a nonlinear correlation between the 18F-FDG SUVMAX and the 18F-FDG scores (r2 = 0.51, P = 0.000; Fig. 2).

Patient 15 (male, 69-y-old) with adenocarcinoma of right lung (18F-FDG/18F-FLT = 0.43). (A) 18F-FDG PET images are displayed in coronal and transaxial slices (SUVMAX = 10.8). (B) 18F-FLT PET in the same patient (SUVMAX = 4.6). Difference on image quality was noticeable.

Nonlinear correlation existed between SUVMAX and scores of 18F-FDG.
18F-FLT Images
In general, the uptake of 18F-FLT by a pulmonary lesion was lower than that of 18F-FDG (Fig. 1B). The higher uptake by liver and bone marrow of vertebrae and ribs made the detection of small lesion(s) by 18F-FLT more difficult. The SUVMAX and scores in malignancies were 3.54 ± 1.98 (range, 0.9∼9.40) and 1.64 ± 1.14 (range, 0∼3.81). The values in TB were 1.65 ± 0.99 (range, 0∼3.3) and 1.21 ± 0.66 (range, 0∼1.61), and in other benign lesions, the values were 1.56 ± 1.60 (range, 0–5.10) and 0.80 ± 0.81 (range, 0.44∼2.17), respectively. ANOVA also indicated a significant difference among groups in SUV (F2,52 = 7.119, P = 0.002) and score (F2,52 = 6.786, P = 0.005). The Games–Howell test confirmed the significance of SUV difference between tumor, TB (P = 0.007), and other benign lesions (P = 0.033) but not between the 2 benign groups, whereas the score differed only between tumor and other benign diseases (P = 0.041). A linear correlation was noted between the 18F-FLT SUVMAX and 18F-FLT scores (r2 = 0.59, P = 0.000; Fig. 3).

Linear correlation existed between SUVMAX and scores of 18F-FLT.
18F-FLT and 18F-FDG Ratios
Interestingly, the ratio between 18F-FLT SUVMAX and 18F-FDG SUVMAX (18F-FLT/18F-FDG) was found to be more accurate than any other criteria in the separation of different subgroups of patients (Fig. 4). Among 29 lesions with an 18F-FLT/18F-FDG ratio < 0.40, 14 were TB (Fig. 5), 12 were inflammation, and only 3 were malignant. All lesions with an 18F-FLT/18F-FDG ratio > 0.90 were inflammation (Fig. 6), whereas in 17 lesions with an 18F-FLT/18F-FDG ratio between 0.40 and 0.90, 13 were malignant. The difference in the 18F-FLT/18F-FDG ratio between the 3 subgroups was statistically significant (F2,49 = 5.361, P = 0.008). The Games–Howell test indicated a significant difference between tumor and TB (0.45 ± 0.146 vs. 0.27 ± 0.140, P = 0.005) and between TB and other benign disease (0.61 ± 0.450, P = 0.007) but not between tumors and inflammation (P = 0.269), probably due to a rather large SD in the latter subgroup of patients.
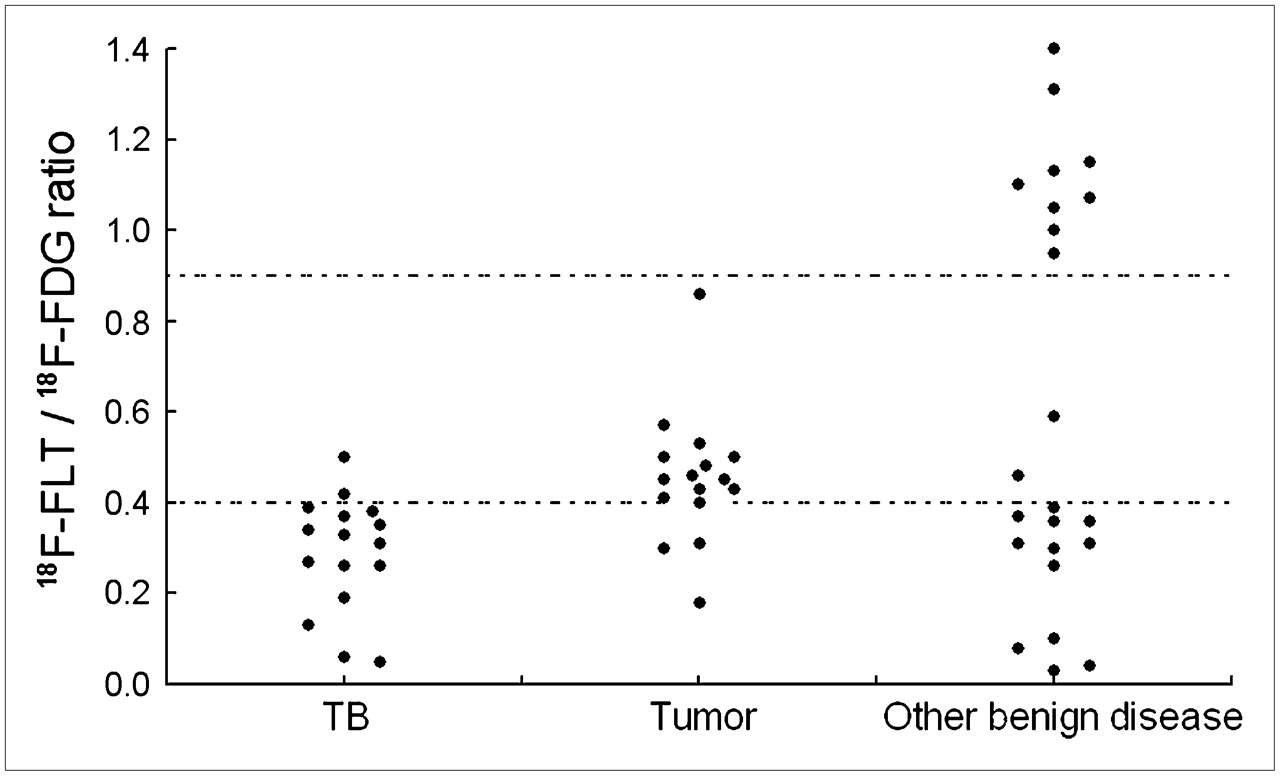
Subgroups of patients with TB, tumor, and other benign diseases could be separated using an 18F-FLT/18F-FDG SUV ratio of 0.40∼0.90. Thirteen of 16 tumors were in this range; only 2 TB and 2 inflammations were false-positive. Fourteen TB and 12 inflammations had 18F-FLT/18F-FDG ratios lower than 0.39. Nine patients had inflammatory lesions with 18F-FLT/18F-FDG ratios higher than 0.95.

Patient 12 (female, 65-y-old) with 1.5 × 1.4 cm lesion at right upper lobe. Confirmed diagnosis was tuberculoses. SUVFDG = 5.0, SUVFLT = 1.3, and 18F-FLT/18F-FDG = 26%.

Patient 16 (female, 73-y-old) with1.7 × 1.2 cm confirmed inflammatory nodule in right upper lung. SUVFDG = 2.2, SUVFLT = 2.2, and 18F-FLT/18F-FDG = 100%.
Dual-Phase 18F-FDG and 18F-FLT Scans
Only 34 patients had delayed 18F-FDG and 25 patients had delayed 18F-FLT (n = 25) imaging. The change in the radiotracer uptake between early and delayed imaging varied unpredictably. In delayed 18F-FDG imaging, 5 of 6 tumors, 9 of 12 TB, and 9 of 16 inflammations had their SUVs increased in delayed imaging, whereas decreased SUVs were noted in 1 of 6 tumors, 3 of 12 TB, and 4 of 16 inflammations. The mean ± SD of delayed SUVFDG was 8.97 ± 4.26 in tumor, 6.69 ± 3.04 in TB, and 4.76 ± 3.41 in inflammation. The ΔSUV was 24% ± 31%, 20.9% ± 35.3%, and 4.52% ± 26.95%, respectively. Increased 18F-FLTSUV was noted in 3 of 7 tumors, 3 of 8 TB, and 2 of 10 inflammations. Four tumors, 5 TB, and 6 inflammations had decreased SUVFLT in delayed scanning. The delayed 18F-FLTSUV was 4.18 ± 2.71, 1.59 ± 1.10, and 1.34 ± 0.91, and the ΔSUV was −0.09% ± 13.31%, −12.3% ± 20.48%, and 10.6% ± 41.35% in the 3 subgroups of patients, respectively. Statistically, no difference in ΔSUV could be demonstrated between groups using either radiotracer.
Diagnostic Performance of Different Imaging Strategies
In the final collective image reading, 18F-FDG PET correctly detected 14 of 16 malignant lesions. However, false-positive scans were noted in 16 of 39 benign cases. The sensitivity of 18F-FLT PET was lower (11/16) and so was its false-positive rate (9/39). The low-dose CT alone had a diagnostic efficiency similar to that of 18F-FLT (sensitivity, 11/16; specificity, 29/39). When the images were read in pairs—such as 18F-FDG + CT, 18F-FLT + CT, or 18F-FDG + 18F-FLT—the specificity improved, especially when 18F-FLT was read with 18F-FDG. CT showed its value in cases of solitary pulmonary nodule (SPN) < 10 mm or with very low uptake when reading became more difficult. The diagnostic performance was obviously improved when the 3 sets of images were read together, resulting in the highest sensitivity, specificity, and accuracy (Table 2). The χ2 test based on expected correct–wrong reading suggested that at least 1 strategy had an important influence on the overall diagnostic performance (χ2 = 18.225, P = 0.006) and that the paired 18F-FDG + 18F-FLT had the highest correct reading over other strategies; therefore, this strategy probably had the highest contribution to the interpretation accuracy (Table 3).
Diagnostic Performance of Different Reading Strategies in 55 Patients
χ2 of Expected Correct and Wrong Reading Counts of Different Strategies
Cases with False Result
The data of 3 patients with lung malignancy were misinterpreted as benign in the collective reading. All were males (age range, 46- to 70-y-old). Bronchioalveolar cell carcinoma was pathologically proven in 2 patients. Careful reevaluation of the other case found an out-of-record “antitumor” therapy of unknown nature before the patient entered the study; therefore, the therapeutic effect on his lesions at the time of imaging could not be excluded.
False-positive results were encountered in 2 inflammatory nodules and 2 tuberculoses. One patient underwent surgery on the basis of the 18F-FLT/18F-FDG PET result, to confirm a lesion of TB. The other patient with TB responded to anti-TB treatment. The lesions of other 2 patients revealed no change in follow-up without antitumor treatment.
DISCUSSION
Design of Trial
The limitation of 18F-FDG in the evaluation of lung tumors has been well documented. The reported positive predictive value of 18F-FDG PET or PET/CT in pulmonary lesions was as low as 44.6% (6). 18F-FLT was developed to reflect the proliferation rate of the lesions and to characterize malignant tumor growth (7,8). The current dual-tracer study was designed to prove the following assumptions: (a) 18F-FDG and 18F-FLT provide information relating to different aspects of tumor biology; (b) dual-tracer imaging, with 18F-FDG and 18F-FLT complementary to each other, adds diagnostic confidence; and (c) the criteria in dual-tracer PET/CT image interpretation are objective, accurate, and easy to use. Enormous efforts were taken in this MCCT to avoid known bias that would affect the results.
Comparison of 18F-FLT and 18F-FDG
In most of the cases, 18F-FDG PET detected more lesions than18F-FLT. The image quality of 18F-FDG was also superior with higher SUVs. The better image quality was believed to be due primarily to its comparatively lower background and more uniform tissue distribution. However, as well described by many authors, nonspecific uptake was noted in a number of benign lesions, especially in tuberculoses. Using SUVMAX = 2.5 as the differential threshold, 18F-FDG PET in our study had a fairly low specificity of 58.97% and an accuracy of 67.27%. These figures were lower than those reported earlier (6). The major reason for the lower accuracy was believed to be the relatively higher proportion of TB among the studied subjects, resulting from a higher prevalence of TB in the districts covered by our imaging centers. Another factor to be considered was that most of our patients had multiple pulmonary nodules. It was recognized earlier that the false-positive rate of 18F-FDG PET was higher in cases of multiple lung lesions (6).
In comparison with 18F-FDG, 18F-FLT images was more “noisy.” The positive bone marrow of the thoracic cage interfered with the evaluation of intrathoracic lesions. In most cases, the uptake of 18F-FLT was lower than that of 18F-FDG, which was in accordance with other reports. For example, Buck et al reported that 18F-FLT uptake was only 50% of 18F-FDG uptake in positive nodal metastases of non–small cell lung cancer. 18F-FLT had better specificity (76.92% vs. 58.97%) in our study, but the increased 18F-FLT uptake was not “related exclusively to malignant tumors” as Buck et al. described (5). The uptake of 18F-FLT was present to various degrees in many TB lesions and other benign lesions. This was not entirely unexpected because false-positive 18F-FLT PET had been reported (3,9). The mechanism of false-positive 18F-FLT uptake is poorly understood. We noted that in our patients, the extent of 18F-FLT accumulation in positive benign lesions did not correlate with that of the granulomatous tissue. In our previous in vitro study (Y Tan and J Tian, unpublished data, March 2006), the uptake of 18F-FLT by Escherichia coli in the growth phase was 6-fold higher than that of 3 tumor cell lines cultured simultaneously. Yap et al reported a false-positive 18F-FLT PET scan in a case of interstitial pneumonia with a Ki67 of 15% (9). Yamamoto et al. also reported a slightly increased Ki67 (2.6% ± 2.2%) in inflammatory cells (3). Thus, one may postulate that the 18F-FLT uptake could increase in response to active DNA synthesis in any tissue, including growing microbes. The effect of 18F-FLT transportation across cell membranes or a phosphorylation pathway other than thymidine kinase 1 should also be considered (10,11). Because of its nontumor uptake, 18F-FLT might not be suitable to work alone or to replace 18F-FDG in the diagnosis or differentiation of pulmonary lesions.
One problem with 18F-FLT was its fairly low production yield and success rate in synthesis (7,12). With the commercially available automatic synthesizer used in our trial, the production succeeded only two thirds of the time, with an average yield of around 13%. The unsatisfactory production efficacy negatively affected the clinical application of the tracer and required improvement of the synthetic techniques (13). An unusual high failure rate in synthesis was noted in southern China, which suggested that environmental factors—such as humidity or temperature—might influence the production procedure or the raw materials.
Additional Diagnostic Gains of Dual-Tracer PET
In the current study, 18F-FDG and 18F-FLT images read in pairs helped in establishing the correct interpretation. The 18F-FLT/18F-FDG ratio was more accurate in revealing the nature of the pulmonary pathologies. A ratio between 0.4 and 0.90 depicted most tumors correctly. A similar finding was recognized when the data of previous studies using both 18F-FDG and 18F-FLT were reviewed carefully. Recalculating the assessable data in their studies, we found that the 18F-FLT/18F-FDG ratios in 12 of 18 tumors by Yamamoto et al. (3), 8 of 11 tumors by Buck et al. (5), and 8 of 12 tumors by Yap et al. (9) were in the same range. However, in the study of Cobben et al. (14), the 18F-FLT/18F-FDG ratio of malignant lesions was lower, but their late 18F-FDG PET imaging at 90min after injection might result in higher SUVFDG—thus, lowering 18F-FLT/18F-FDG ratio. The higher 18F-FLT/18F-FDG ratio in our inflammation was believed to be due to the lower uptake of 18F-FDG by the lesions. Two of 3 benign lesions reported by Yap et al also had 18F-FLT/18F-FDG ratios > 100%.
There was no clear explanation for the different 18F-FLT/18F-FDG ratios among the subgroups of patients. It was known that 18F-FLT is transported into cells via an equilibrative nucleoside transporter–mediated facilitated transport mechanism, phosphorylated by enzyme thymidine kinase 1, and accumulated as mono-, di-, and triphosphate nucleotides in cells (15). It might be correct to assume that all of these biochemical processes keep some sort of balance with the energy metabolism of the cells, resulting in a rather fixed 18F-FLT/18F-FDG ratio. The difference in 18F-FLT/18F-FDG SUV ratios between tumors, TB, and inflammation could be useful clinically in separating the different pathologies when neither 18F-FDG nor 18F-FLT could face the challenge alone.
Multimodality imaging has been a hot topic in recent years. Early in 2007, Kim et al. reported that the combination of 18F-FDG PET and CT improved the diagnostic efficacy in solitary pulmonary lesions, with the best performance in ROC analysis (16). Another recent report on liver cancer confirmed that dual-tracer PET/CT had an incremental value and a complementary advantage when compared with single-tracer imaging in the evaluation of metastasis (17). In our study, the combination of biologic probes (18F-FDG and 18F-FLT) and of metabolic and anatomic imaging modalities(PET and CT) increased the diagnostic sensitivity and accuracy in a rather heterogeneous group of patients. Two imaging modalities are definitely better than one.
The radiation burden of dual-tracer, dual-modality imaging of the patients must be addressed. The effective dose equivalent of 18F-FLT was estimated by Vesselle et al. (18) as 0.031 mSv/MBq (114 mrem/mCi), which is compatible with that of 18F-FDG (0.029mSv/MBq). If 2 doses of 400 MBq were administered in a short interval, the total radiation dose a patient received would be 11.6 + 12.4 = 24 mSv. In view of the potential benefit that the more confident diagnosis could bring to the patients, the dual-tracer strategy should be valued favorably, at least for those with an equivocal diagnosis.
Other Interesting Findings
SUV and Score.
In the current study, a good correlation was found between SUV and score for both 18F-FDG and 18F-FLT. It was also shown that the simple scoring based on visual inspection had a diagnostic efficacy similar to that of quantitative SUV. This was in accordance with the reports by Kim et al. (16) and Hashimoto et al. (19) that semiquantitative means, such as SUV, could hardly add diagnostic value over visual inspection in PET.
Dual-Phase Study.
Controversial statements about the usefulness and reliability of delayed imaging of 18F-FDG have appeared in the literature. In our study, the change in SUV between an early scan and a delayed scan was quite unpredictable. It seemed very unlikely to us that the nature of pulmonary lesions could be differentiated satisfactorily on the basis of dual-phase 18F-FDG or 18F-FLT PET.
Value of Low-Dose CT (LDCT).
The value of LDCT was appreciated in assisting smaller lesion detection and drawing of ROIs on PET images, especially for 18F-FLT PET. LDCT might miss a few lesions, as O et al (20) noted, and the unsatisfactory performance of CT in our study might result from the inclusion criteria that precluded the lesion with typical morphologic features.
Limitations of the Trial.
There were several limitations in the design and execution of the current MCCT. First, we used LDCT only; no other classical procedures, such as multiplanar reconstruction or contrast enhancement, were undertaken. This might underestimate the value of CT, although the usefulness of LDCT had been verified previously (21). Second, the imaging was acquired and processed using just one model of scanner; the quantitative criteria derived from our study must be cautiously referenced when other devices are used. Third, the number of patients was inadequate, and the composition of diseases was heterogeneous; therefore, not all conclusions may be suitable for the situation in another country or in another study. Because of the limited number of subjects, it was premature to analyze the imaging characteristics according to different histologic types of tumors or diseases. Fourth, the 1-y follow-up was not long enough. Thus far, we have no data relating to the influence of dual-tracer PET/CT on the long-term clinical outcome of our patients and we have no evidence on the cost-effectiveness of dual-tracer PET/CT. Last, but not the least, the collective blinded reading was organized with readers of different professional backgrounds and inadequate experience and training, and the adjustment of viewing angle and window settings might influence other readers' attention and judgment—therefore, a subjective factor could not be completely excluded.
CONCLUSION
In this prospective, randomized multicenter clinical trial, dual-tracer PET/CT using 18F-FLT and 18F-FDG improved the diagnostic accuracy of differentiating pulmonary nodules. 18F-FLT and 18F-FDG reflected different aspects of biologic features but neither tracer alone could guarantee satisfactory diagnostic performance. Although visual inspection scores worked well as quantitative SUVs for both tracers, the SUV ratio between 18F-FLT and 18F-FDG worked best in the differentiation of malignancies, TB, and other benign lesions. Considering the limited number of patients and the heterogeneity of underlining diseases of our study population, the real clinical values, long-term clinical impact, and cost-effectiveness of the dual-tracer PET/CT in the diagnosis of pulmonary nodules are worthy of further investigation.
Acknowledgments
This trial was technically supported and sponsored by GE Healthcare, China, and The Chinese Society of Nuclear Medicine. The contributions of Drs. Hongli Li and Shuang Wang of GE, China, and all staff in the imaging centers are deeply appreciated.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 5, 2007.
- Accepted for publication November 12, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of 18F-FLT PET in Patients with Neuroendocrine Neoplasms: A Prospective Head-to-Head Comparison with 18F-FDG PET and Ki-67 in 100 Patients
- Interobserver Agreement of Qualitative Analysis and Tumor Delineation of 18F-Fluoromisonidazole and 3'-Deoxy-3'-18F-Fluorothymidine PET Images in Lung Cancer
- Clinical analysis of 76 patients pathologically diagnosed with pulmonary cryptococcosis
- Imaging Colon Cancer Response Following Treatment with AZD1152: A Preclinical Analysis of [18F]Fluoro-2-deoxyglucose and 3'-deoxy-3'-[18F]Fluorothymidine Imaging