


Abstract
3′-Deoxy-3′-18F-fluorothymidine (18F-FLT) has been suggested as a new PET tracer for imaging tumor proliferation. We investigated the use of 18F-FLT to monitor the response of tumors to radiotherapy and photodynamic therapy (PDT) in mice. Methods: C3H/He mice bearing an SCCVII tumor were treated with single-dose x-ray irradiation of 20 Gy. Tumor uptake was examined for 18F-FLT, 3H-thymidine (3H-Thd), 18F-FDG, and 14C-deoxyglucose (14C-DG) at 6 h, 12 h, 24 h, 3 d, and 7 d after radiotherapy. BALB/c nu/nu mice bearing a HeLa tumor were treated with PDT. Tumor uptake was examined for the 4 tracers at 24 h after PDT. Expression of proliferating cell nuclear antigen (PCNA) was determined in untreated and treated tumors. Results: In the biodistribution study, considerable uptake of 18F-FLT was observed in both tumor types. Tumor volumes decreased to 39.3% ± 22.4% at 7 d after radiotherapy. The PCNA labeling index was reduced in x-ray–irradiated tumors (control, 53.2% ± 8.7%; 6 h, 38.5% ± 5.3%; 24 h after radiotherapy, 36.8% ± 5.3%). 18F-FLT uptake in tumor expressed as the percentage of the injected dose per gram of tumor (%ID/g) decreased significantly at 6 h and remained low until 3 d after radiotherapy (control, 9.7 ± 1.2 %ID/g; 6 h, 5.9 ± 0.4 %ID/g; 24 h, 6.1 ± 1.3 %ID/g; 3 d after radiotherapy, 6.4 ± 1.1 %ID/g). 18F-FDG uptake tended to gradually decrease but a significant decrease was found only at 3 d (control, 12.1 ± 2.7 %ID/g; 6 h, 13.3 ± 2.3 %ID/g; 24 h, 8.6 ± 1.8 %ID/g; 3 d after radiotherapy, 6.9 ± 1.2 %ID/g). PDT resulted in a reduction of the PCNA labeling index (control, 82.0% ± 8.6%; 24 h after PDT, 13.5% ± 12.7%). Tumor uptake of 18F-FLT decreased (control, 11.1 ± 1.3 %ID/g; 24 h after PDT, 4.0 ± 2.2 %ID/g), whereas 18F-FDG uptake did not decrease significantly after PDT (control, 3.5 ± 0.6 %ID/g; 24 h after PDT, 2.3 ± 1.1 %ID/g). Changes in the uptake of 18F-FLT and 18F-FDG were similar to those of 3H-Thd and 14C-DG, respectively. Conclusion: In our model system, changes in 18F-FLT uptake after radiotherapy and PDT were correlated with those of 3H-Thd and the PCNA labeling index. The decrease in 18F-FLT uptake after treatments was more rapid or pronounced than that of 18F-FDG. Therefore, 18F-FLT may be a feasible PET tracer for monitoring response to therapy in oncology.
Deregulated proliferation is one of the key features of malignant tumors and imaging of tumor proliferation is expected to improve the management of patients with cancer. Morphologic imaging techniques, which have been the standard method to identify treatment efficacy, depict tumor response as changes in tumor size and composition. Changes in size, however, are often delayed and it is difficult to evaluate early response to treatment by morphologic imaging techniques.
PET can aid in this task, because metabolic and physiologic changes precede size change. The fluorine-labeled glucose analog 18F-FDG has been the most widely used agent in PET tumor imaging. However, increased glycolysis is not an essential property of proliferating cells and 18F-FDG is taken up by inflammatory cells such as macrophages (1). Therefore, considerable efforts have been invested in seeking more suitable PET tracers for imaging tumor proliferation (2). Recently, a fluorine-labeled thymidine analog, 3′-deoxy-3′-18F-fluorothymidine (18F-FLT), has been developed as a candidate for imaging cell proliferation. 18F-FLT is phosphorylated by thymidine kinase 1, the key enzyme of the pyrimidine salvage pathway of DNA synthesis, and metabolically trapped as a phosphorylated form (3).
18F-FLT was firstly applied for PET in 1998 (4) and, since then, 18F-FLT has been shown to accumulate in a variety of tumors and its uptake could reflect the tumor proliferation (4–9). However, there have been few reports on the use of 18F-FLT for monitoring tumor response to therapy.
The aim of this study was to investigate the use of 18F-FLT for monitoring response to anticancer treatments in mouse models. We clarified that the change of 18F-FLT uptake after radiotherapy or photodynamic therapy (PDT) correlated well with the proliferative activity of transplanted tumors.
MATERIALS AND METHODS
Radiopharmaceuticals
18F-FLT and 18F-FDG were produced by the Central Research Laboratory, Hamamatsu Photonics K.K. 18F-FLT was synthesized by nucleophilic substitution of nosylate precursor (precursor FLT [1-(2-deoxy-3-o-(4-nitrobenzenesulfonyl)-5-o-(4,4′-dimethoxytrityl)-d-threopentofuranosyl)-3-(2,4-dimethoxybenzyl)thymine]) according to the method developed by Grierson and Shields with minor modification (10). 18F-Fluoride was produced with the cyclotron, using the 18O (p, n)18F nuclear reaction by irradiation of a water target containing 18O-enriched water. 18F-FDG was synthesized with an automated FDG synthesis module. Methyl-3H-thymidine ([3H-Thd]; specific activity, 2.22–3.2 TBq/mmol) and 2-deoxy-d-1-14C-glucose ([14C-DG]; specific activity, 1.85–2.29 GBq/mmol) were purchased from Amersham Biosciences Corp.
Animals and Tumor Models
Five- to 7-wk-old female C3H/He mice (Japan SLC, Inc.) and BALB/c nu/nu mice (CREA Japan, Inc.) were used. Subcutaneous tumors were established in the thigh of C3H/He mice with SCCVII, a murine squamous cell carcinoma cell line, and in the thigh of BALB/c nu/nu mice with HeLa, a human uterine cervical adenocarcinoma cell line. When the size of tumor reached 6–10 mm in diameter at 10–14 d after the injection of 5 × 106 cells, the mice were used for experiments. In all animal experiments, the mice were not anesthetized after tracer injection. The experimental protocol was fully accredited by the laboratory Animal Care Committee of the Hamamatsu University School of Medicine.
18F-FLT Uptake in Untreated Tumor and Normal Tissue
The biodistribution of 18F-FLT was assessed in untreated tumor-bearing mice. Twelve C3H/He mice transplanted with SCCVII and 4 BALB/c nu/nu mice transplanted with HeLa were injected intravenously with 1.8–2.5 MBq 18F-FLT via lateral tail vein. SCCVII-bearing mice were sacrificed at 0.5, 1, and 2 h after radiotracer injection. HeLa-bearing mice were sacrificed at 1 h. Blood, normal tissue (heart, lung, kidney, spleen, muscle, femur, small intestine), and tumor samples were rapidly excised. All samples were weighed, and the radioactivity was measured in an auto-well γ-counter (Aloka ARC-2000), applying a decay correction. Accumulation of tracers in tumor or normal tissues was expressed as the percentage of the injected dose per gram of tumor per 20 g of mouse weight (%ID/g).
X-Ray Irradiation
C3H/He mice transplanted with SCCVII were anesthetized with 1 mg sodium pentobarbital intraperitoneally and then fixed with adhesive tape to place the tumor-bearing thigh in the field of irradiation. The other parts of the body were left outside of the radiation field. Tumors were exposed to a single dose of 20 Gy at a dose rate of 2.25 Gy/min.
Changes in Tumor Volume After Radiotherapy
Eight C3H/He mice transplanted with SCCVII were randomly assigned to 2 groups: 1 treatment group and 1 control group. Each group consisted of 4 mice. From the day of the irradiation, tumor size was determined with a caliper measuring the largest diameter (a) and the perpendicular diameter (b). Tumor volume was calculated according to the formula 0.5 × a × b2, assuming an elliptic geometry. Growth curves were generated as a change of relative tumor volume based on the volume on the day of irradiation.
PDT
BALB/c nu/nu mice transplanted with HeLa were injected intravenously with 6 mg/kg of ATX-S10(Na) (13,17-bis[1-carboxypropionyl]carbamoylethyl-8-ethenyl-2-hydroxy-3-hydroxyiminoethylidene-2,7,12,18-tetramethylporphyrin sodium salt) via tail vein. ATX-S10(Na) is a second-generation photosensitizer, which was developed to reduce the hyperphotosensitivity of porfimer sodium (11). Three hours later, the mice were restrained for light exposure. A 10- to 14-mm-diameter area encompassing the tumor was irradiated with a semiconductor diode laser of 670-nm wavelength (LD670C; Hamamatsu Photonics K.K.) at a fluence of 100 J/cm2. Tumors were inspected until 7 d after PDT in 5 mice.
Expression of Proliferating Cell Nuclear Antigen (PCNA)
Untreated SCCVII and HeLa tumors, SCCVII tumors at 6 and 24 h after radiotherapy, and HeLa tumors at 24 h after PDT were fixed in formalin, embedded in paraffin, and cut into 5.0-μm sections. Tumors were obtained from 4 mice in each group. One section per tumor was examined. Sections were incubated with biotinylated PCNA monoclonal antibody (Zymed Laboratory Inc.); streptoavidin peroxidase was used as a signal generator and diaminobenzidine tetrahydrochloride was used as a choromogen to stain PCNA-containing nuclei a dark brown. All sections were counterstained with hematoxylin for counting the total cell number. In each run, sections of small intestine were stained as positive controls and sections of brain were used as negative controls. First, the PCNA-stained section was scanned at low power to select areas exhibiting a high concentration of PCNA-positive cells and high cellular density. Then, the numbers of PCNA-positive and hematoxylin-positive cells were counted in 5 randomly selected fields of view per section using a BH2 microscope (Olympus Optical) at ×400 magnification. At least 500 cells were counted in each field. The PCNA labeling index was established as the percentage of PCNA-positive cells.
Tumor Uptake of Radiopharmaceuticals After Radiotherapy
In SCCVII-bearing mice, tumor uptake of 18F-FLT or 18F-FDG was assessed at 6 h, 12 h, 24 h, 3 d, and 7 d after radiotherapy. Untreated mice served as controls. Twenty-seven mice were used for 18F-FLT (untreated control, n = 4; 6 h, n = 5; 12 h, n = 5; 24 h, n = 4; day 3, n = 5; day 7, n = 4). Twenty-nine mice were used for 18F-FDG (untreated control, n = 5; 6 h, n = 5; 12 h, n = 5; 24 h, n = 5; day 3, n = 5; day 7, n = 4). The mice received 1.8–2.5 MBq 18F-FLT or 1.8–2.5 MBq 18F-FDG.
The uptake of 3H-Thd and 14C-DG in x-ray–irradiated tumor was determined by the dual-tracer technique. A mixture of 0.0925 MBq 3H-Thd and 0.037 MBq 14C-DG was administered to untreated mice and to mice at 6 h, 12 h, 24 h, 3 d, and 7 d after radiotherapy. Thirty mice were used for this dual-tracer experiment (untreated control, n = 6; 6 h, n = 4; 12 h, n = 5; 24 h, n = 5; day 3, n = 5; day 7, n = 5).
The mice were killed at 1 h after radiotracer injection. Tumors were rapidly excised and weighed. Radioactivity was measured in an auto-well γ-counter for 18F and in a liquid scintillation counter using the double-window technique for 3H and 14C. Tumor uptake of radiotracers was calculated as in the biodistribution study.
Tumor Uptake of Radiopharmaceuticals After PDT
Tumor uptake of 18F-FLT, 18F-FDG, 3H-Thd, and 14C-DG was measured in HeLa-bearing BALB/c nu/nu mice at 24 h after PDT. Untreated mice served as controls. Eight mice were used for 18F-FLT (control, n = 4; PDT, n = 4). Eight mice were used for 18F-FDG (control, n = 4; PDT, n = 4). Twelve mice were used for the dual-tracer experiment of 3H-Thd and 14C-DG (control, n = 6; PDT, n = 6). The administered dose of radiopharmaceuticals and the methods for evaluating tumor uptake were the same as those in the experiments for radiotherapy.
Statistical Analysis
Statistical analysis was performed with SPSS for Windows software, version 11.0.1 (SPSS, Inc.). All data are expressed as mean ± SD. The differences between untreated controls and x-ray–irradiated groups with respect to radiotracer uptake and the PCNA labeling index were analyzed by the Kruscal–Wallis test with adjustment by the Bonferroni method for multiple comparisons. P < 0.05 was considered statistically significant.
Differences between untreated controls and PDT-treated groups with respect to radiotracer uptake and the PCNA labeling index were tested with the Mann–Whitney Wilcoxon test. P < 0.05 was considered statistically significant.
RESULTS
18F-FLT Uptake in Untreated Tumor and Normal Tissue
Because tumor uptake of 18F-FLT in SCCVII at 1 h after injection was not significantly different from that at 2 h (data not shown), we conducted the following experiments with 18F-FLT at the 1-h time point. Figure 1 shows the tissue distribution of 18F-FLT in SCCVII-bearing C3H/He mice and in HeLa-bearing BALB/c nu/nu mice at 1 h after injection. High radioactivity was noted in the kidney and small intestine as well as the tumors. Splenic uptake was also high in C3H/He mice.

Biodistribution of 18F-FLT in C3H/He mice transplanted with SCCVII and in BALB/c nu/nu mice transplanted with HeLa at 1 h after injection. Data are expressed as mean ± SD.
Radiotherapy and Tumor Uptake of 18F-FLT in SCCVII-Bearing Mice
The growth curve of SCCVII tumor in untreated and x-ray–irradiated mice is shown in Figure 2. Radiotherapy with 20 Gy resulted in tumor shrinkage and the relative tumor volume decreased to 39.3% ± 22.4% at 7 d after radiation. Tumors grew again after 14 d and the relative volume at day 21 was 98.6% ± 94.1%. There was a significant decrease in the PCNA labeling index in tumors obtained at 6 and 24 h after radiotherapy (control, 53.2% ± 8.7%; 6 h, 38.5% ± 5.3%; 24 h, 36.8% ± 5.3%, P < 0.05; Table 1).

Changes in relative tumor volume in control mice and x-ray–irradiated mice. Mice bearing SCCVII received 20 Gy at day 0. Data are expressed as mean ± SD. Radiotherapy resulted in tumor shrinkage and no tumor regrowth was found until 14 d after radiation. Tumors grew again after 14 d.
PCNA Labeling Index in Tumors After Radiotherapy and PDT
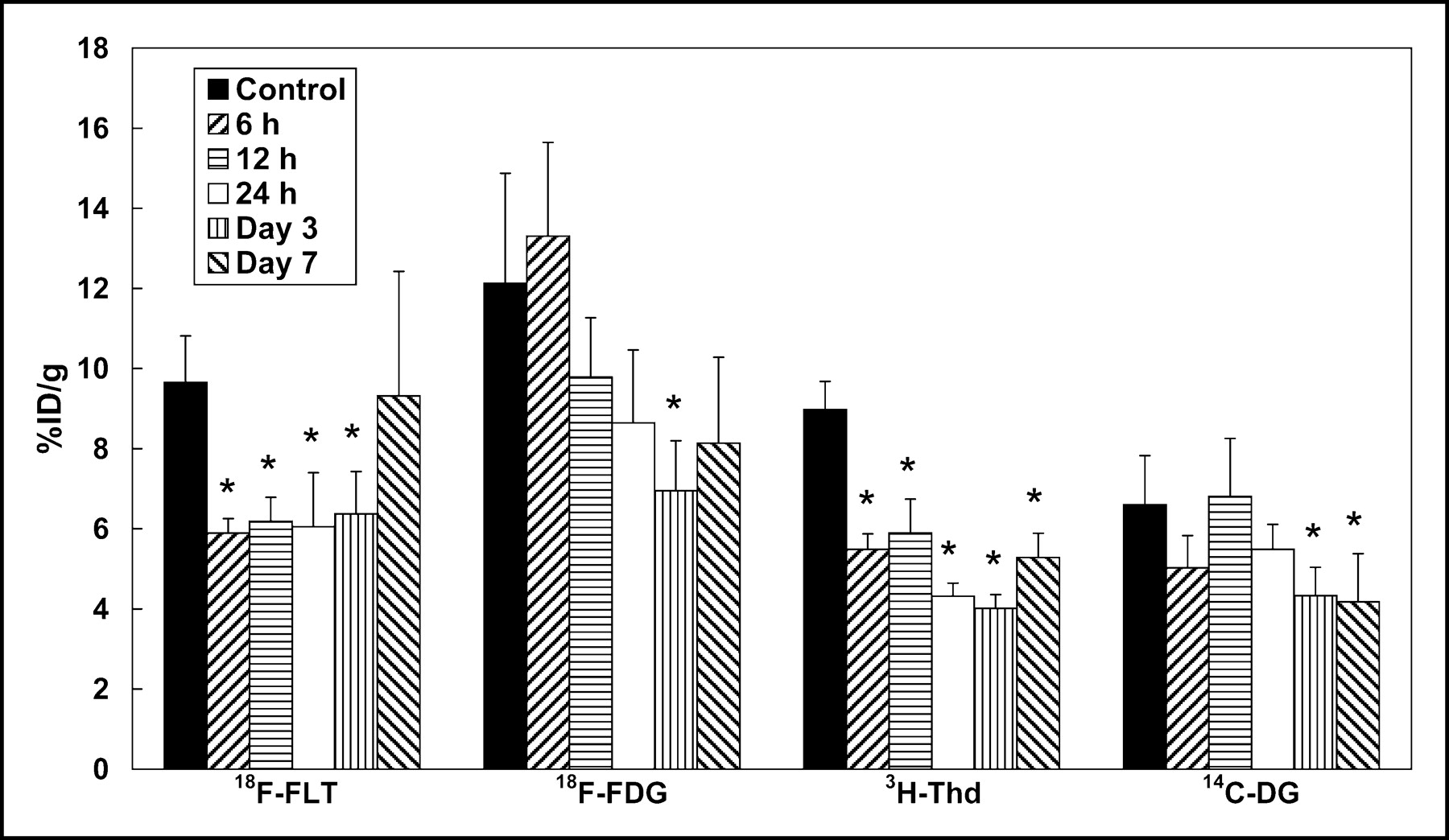
Tumor uptake of 18F-FLT decreased significantly at 6 h after radiotherapy and remained low until 3 d (P < 0.05; Fig. 3). At 7 d after x-ray irradiation, there was a tendency for 18F-FLT uptake to increase (control, 9.7 ± 1.2 %ID/g; 6 h, 5.9 ± 0.4 %ID/g; 12 h, 6.2 ± 0.6 %ID/g; 24 h, 6.1 ± 1.3 %ID/g; day 3, 6.4 ± 1.1 %ID/g; day 7, 9.3 ± 3.1 %ID/g). A decrease in 3H-Thd uptake was observed at all time points (control, 9.0 ± 0.7 %ID/g; 6 h, 5.5 ± 0.4 %ID/g; 12 h, 5.9 ± 0.8 %ID/g; 24 h, 4.3 ± 0.3 %ID/g; day 3, 4.0 ± 0.3 %ID/g; day 7, 5.3 ± 0.6 %ID/g). The uptake of 18F-FDG and 14C-DG tended to gradually decrease. A statistically significant decrease in tumor uptake of 18F-FDG was found only at 3 d (control, 12.1 ± 2.7 %ID/g; 6 h, 13.3 ± 2.3 %ID/g; 12 h, 9.8 ± 1.5 %ID/g; 24 h, 8.6 ± 1.8 %ID/g; day 3, 6.9 ± 1.2 %ID/g; day 7, 8.1 ± 2.1 %ID/g) and that of 14C-DG at 3 and 7 d after radiotherapy (control, 6.6 ± 1.3 %ID/g; 6 h, 5.0 ± 0.8 %ID/g; 12 h, 6.8 ± 1.4 %ID/g; 24 h, 5.5 ± 0.6 %ID/g; day 3, 4.3 ± 0.7 %ID/g; day 7, 4.2 ± 1.2 %ID/g).
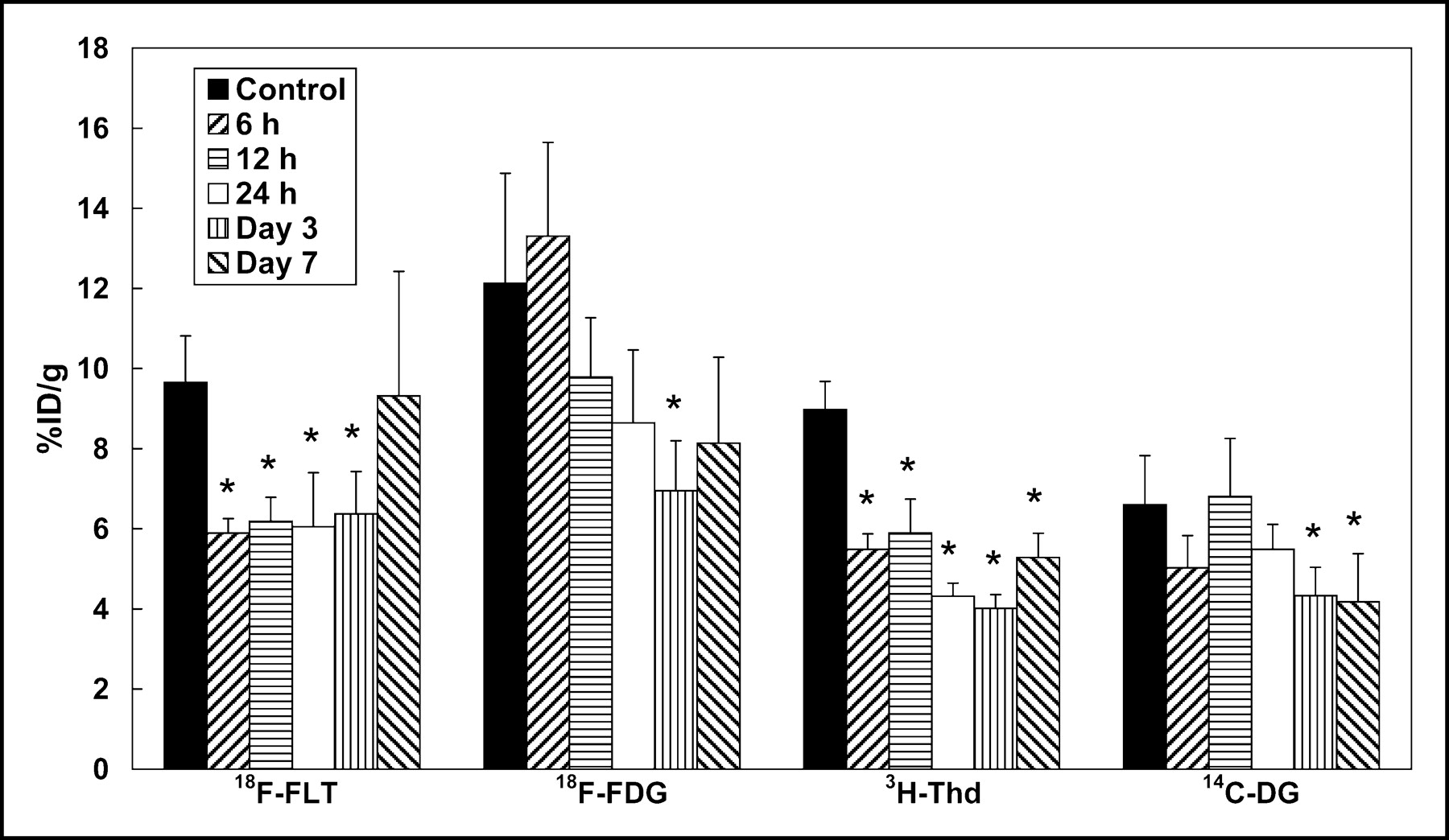
Tumor uptake of 4 tracers after radiotherapy. Data are expressed as mean ± SD. Asterisks indicate statistically significant differences compared with untreated controls (P < 0.05). Tumor uptake of 18F-FLT decreased significantly at 6 h, 12 h, 24 h, and 3 d after radiotherapy compared with untreated controls. There was a significant decrease in 3H-Thd uptake at 6 h, 12 h, 24 h, 3 d, and 7 d compared with untreated controls. Tumor uptake of 18F-FDG and 14C-DG did not show a statistically significant decrease at 6, 12, and 24 h after radiotherapy.
PDT and Tumor Uptake of 18F-FLT in HeLa-Bearing Mice
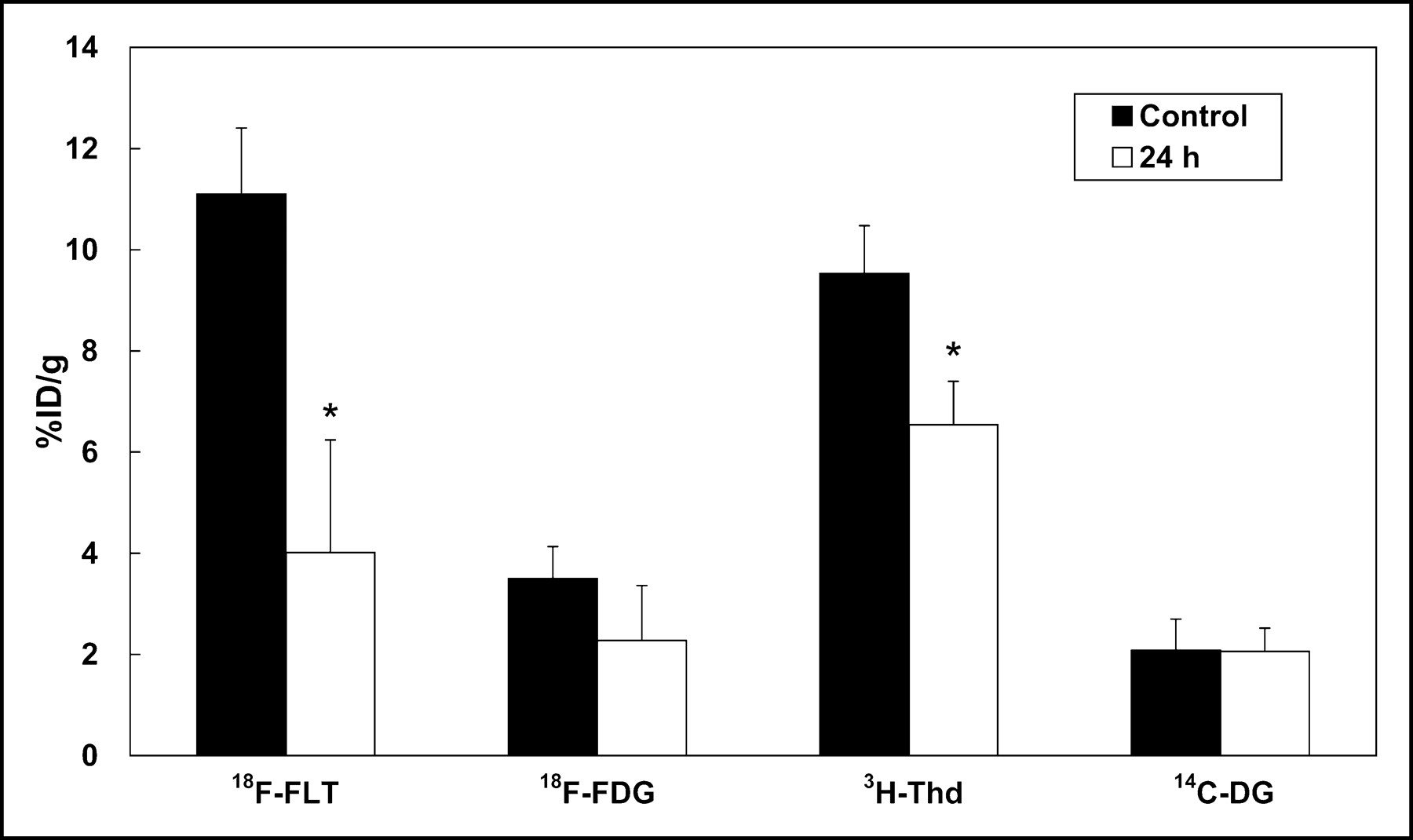
Massive edema was observed at 24 h after PDT. On the third day, tumors shrunk and their color turned blackish-brown, which represented necrosis. The PCNA labeling index decreased significantly at 24 h after PDT (control, 83.2% ± 8.6%; PDT, 13.5% ± 12.7%, P < 0.05; Table 1). A significant decrease in 18F-FLT or 3H-Thd uptake was observed in PDT-treated tumors (control, 11.1 ± 1.3 %ID/g; PDT, 4.0 ± 2.2 %ID/g for 18F-FLT; control, 9.5 ± 1.0 %ID/g; PDT, 6.5 ± 0.9 %ID/g for 3H-Thd, P < 0.05; Fig. 4). There was no significant difference between untreated controls and PDT-treated tumors in the uptake of 18F-FDG and 14C-DG (control, 3.5 ± 0.6 %ID/g; PDT, 2.3 ± 1.1 %ID/g for 18F-FDG; control, 2.1 ± 0.6 %ID/g; PDT, 2.1 ± 0.5 %ID/g for 14C-DG).
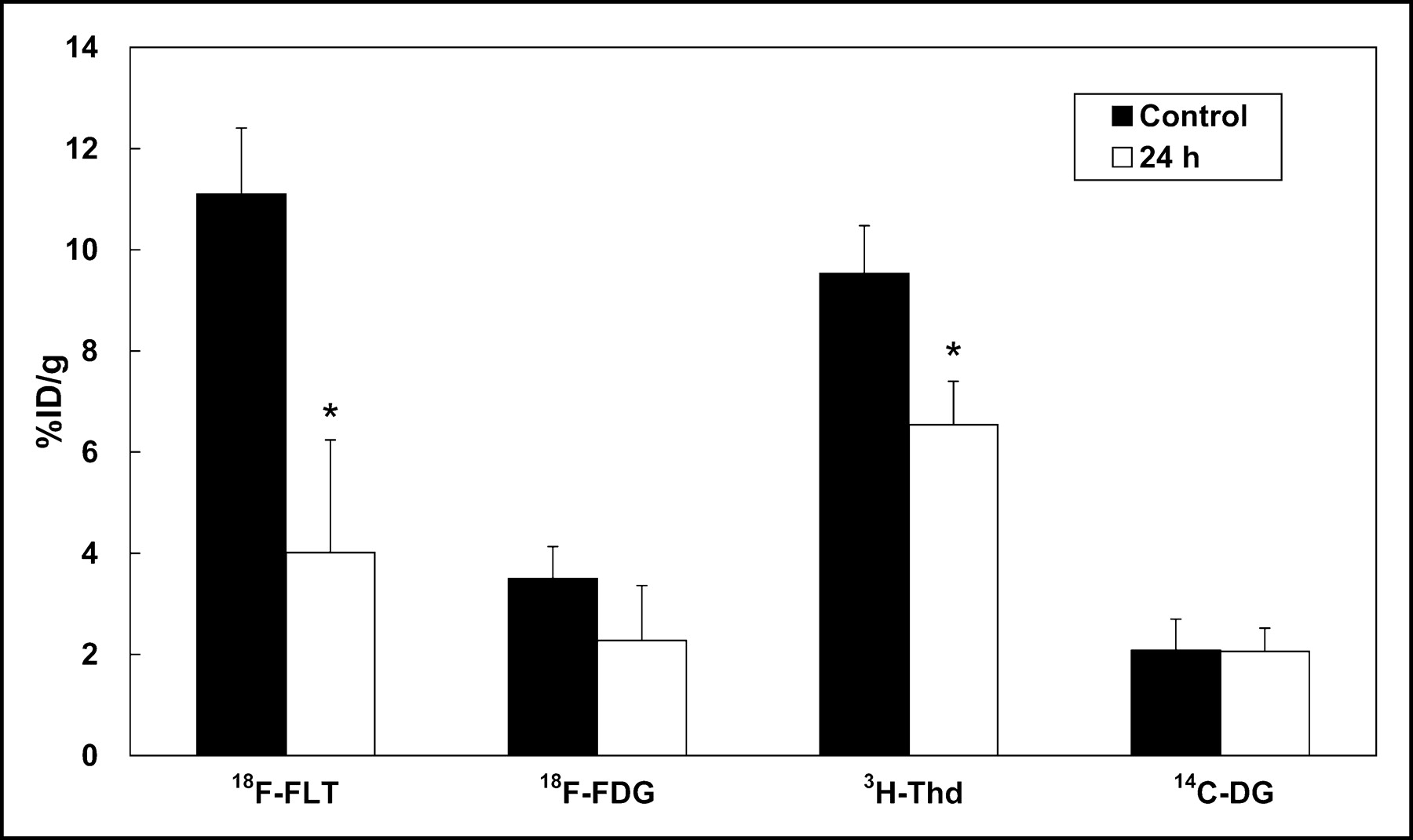
Tumor uptake of 4 tracers at 24 h after PDT. Data are expressed as mean ± SD. Asterisks indicate statistically significant differences compared with untreated controls (P < 0.05). A significant decrease of tumor uptake of 18F-FLT and 3H-Thd was observed in PDT-treated tumors. There was no significant difference between untreated controls and PDT-treated tumors in the uptake of 18F-FDG and 14C-DG.
DISCUSSION
This study demonstrated that 18F-FLT uptake by transplanted tumors showed a rapid response to radiotherapy and PDT preceding objective tumor shrinkage. Changes in 18F-FLT uptake were similar to those of 3H-Thd except at 7 d after radiotherapy. 3H-Thd is rapidly incorporated into DNA and has been widely used as a marker of cell proliferation. Although 18F-FLT is not incorporated into DNA, 18F-FLT would be a reliable marker for cell proliferation as well as 3H-Thd. There was a tendency for 18F-FLT uptake to increase at 7 d after x-ray irradiation. Tumor size remained stable for a further 7 d and only a mild increase in tumor size was observed 21 d after radiotherapy. Further examination is needed to clarify the role of 18F-FLT as an indicator of tumor regrowth.
18F-FLT uptake in tumor was also validated by comparison with the PCNA labeling index. PCNA is a 36-kDa nuclear polypeptide that is related to the cell proliferation (12). A previous study indicated that PCNA, synthesized during the late G1-to-S phase, is an auxiliary for DNA polymerase (13). Correlation between 18F-FLT uptake and the PCNA labeling index after radiotherapy and PDT also suggests the usefulness of 18F-FLT for monitoring cell proliferation.
PDT is a new treatment modality for solid tumors. The procedure consists of the administration of a photosensitizer that accumulates preferentially in the tumor, followed by local illumination of neoplastic tissues with red light (14,15). PDT has been shown to induce tumor necrosis through initial vascular damage and to direct tumor cell killing induced by singlet oxygen (16). Because 18F-FLT is useful for monitoring the effect of PDT, which has a different antitumor mechanism from radiotherapy, 18F-FLT could be applicable to other types of anticancer therapy.
In C3H/He mice, high uptake was found in the spleen and small intestine, which are organs with a high proliferative activity in mice. High uptake in the kidneys suggests a renal excretion of 18F-FLT. Uptake in the spleen was not high in BALB/c nu/nu mice in comparison with C3H/He mice. Distribution of 18F-FLT in normal tissues may be different among strains of mice.
A decrease in tumor uptake of 18F-FDG was found only 3 d after radiotherapy, and 18F-FDG uptake did not decrease significantly after PDT. 14C-DG showed a change similar to that of 18F-FDG. These results may be attributable to a minimal change in glycolysis in tumor cells or an increase in glucose uptake by inflammatory tissues early after radiotherapy or PDT. Work with animal tumors and cultured cells has suggested that radiolabeled thymidine is a better indicator of cell proliferation than 18F-FDG (17,18). Furthermore, Barthel et al. showed an early decrease in 18F-FLT uptake by RIF-1 tumors after 5-fluorouracil treatment, which was more pronounced than that of 18F-FDG (19). Our results agree with the findings that the uptake of radiolabeled thymidine provided more accurate assessments of the early response to anticancer therapy than that of 18F-FDG.
CONCLUSION
We have shown that the decrease in 18F-FLT uptake after radiotherapy and PDT was more rapid or pronounced than that of 18F-FDG. 18F-FLT uptake correlated well with 3H-Thd uptake and the PCNA labeling index. The change in 18F-FLT uptake was supposed to reflect proliferative activity after anticancer treatment. Therefore, 18F-FLT is expected to be a feasible PET tracer for monitoring the response to therapy in oncology.
Acknowledgments
The authors are grateful to Yasuhiro Magata, PhD, and Mikako Ogawa, MS, of Photon Medical Research Center, Hamamatsu University School of Medicine, for their technical assistance. This study was supported in part by a Grant-in-Aid for Scientific Research (1240187) and Special Coordination Funds for the Promotion of Science and Technology (Research and Development of Technology for Measuring Vital Function Merged with Optical Technology) from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
Footnotes
Received Feb. 19, 2004; revision accepted Apr. 29, 2004.
For correspondence or reprints contact: Masahiro Sugiyama, MD, Department of Radiology, Hamamatsu University School of Medicine, Handayama 1-20-1, Hamamatsu, Japan 431-3192.
E-mail: masahiro{at}akiha.hama-med.ac.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Molecular Imaging to Plan Radiotherapy and Evaluate Its Efficacy
- Predictive Value of Early-Stage Uptake of 3'-Deoxy-3'-18F-Fluorothymidine in Cancer Cells Treated with Charged Particle Irradiation
- Early Response Monitoring with 18F-FDG PET and Cetuximab-F(ab')2-SPECT After Radiotherapy of Human Head and Neck Squamous Cell Carcinomas in a Mouse Model
- Acute Cytotoxic Effects of Photoimmunotherapy Assessed by 18F-FDG PET
- Usefulness of 3'-Deoxy-3'-18F-Fluorothymidine PET for Predicting Early Response to Chemoradiotherapy in Head and Neck Cancer
- 18F-FDG PET/CT for Image-Guided and Intensity-Modulated Radiotherapy
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- Evaluation of D-18F-FMT, 18F-FDG, L-11C-MET, and 18F-FLT for Monitoring the Response of Tumors to Radiotherapy in Mice
- Kinetic Modeling of 3'-Deoxy-3'-18F-Fluorothymidine for Quantitative Cell Proliferation Imaging in Subcutaneous Tumor Models in Mice
- [18F]Fluorothymidine Positron Emission Tomography before and 7 Days after Gefitinib Treatment Predicts Response in Patients with Advanced Adenocarcinoma of the Lung
- Imaging of Cell Proliferation: Status and Prospects
- Dynamic Small-Animal PET Imaging of Tumor Proliferation with 3'-Deoxy-3'-18F-Fluorothymidine in a Genetically Engineered Mouse Model of High-Grade Gliomas
- Preclinical Efficacy of the c-Met Inhibitor CE-355621 in a U87 MG Mouse Xenograft Model Evaluated by 18F-FDG Small-Animal PET
- Early Detection of Chemoradioresponse in Esophageal Carcinoma by 3'-Deoxy-3'-3H-Fluorothymidine Using Preclinical Tumor Models
- Positron Emission Tomography As an Imaging Biomarker
- Dynamic Imaging of Transient Metabolic Processes by Small-Animal PET for the Evaluation of Photosensitizers in Photodynamic Therapy of Cancer
- Reproducibility of 3'-Deoxy-3'-18F-Fluorothymidine MicroPET Studies in Tumor Xenografts in Mice