


Abstract
Malignant gliomas and metastatic tumors are the most common brain tumors. Neuroimaging plays a significant role clinically. In low-grade tumors, neuroimaging is needed to evaluate recurrent disease and to monitor anaplastic transformation into high-grade tumors. In high-grade and metastatic tumors, the imaging challenge is to distinguish between recurrent tumor and treatment-induced changes such as radiation necrosis. The current clinical gold standard, MRI, provides superior structural detail but poor specificity in identifying viable tumors in brain treated with surgery, radiation, or chemotherapy. 18F-FDG PET identifies anaplastic transformation and has prognostic value. The sensitivity and specificity of 18F-FDG in evaluating recurrent tumor and treatment-induced changes can be improved significantly by coregistration with MRI and potentially by delayed imaging 3–8 h after injection. Amino acid PET tracers are more sensitive than 18F-FDG in imaging recurrent tumors and in particular recurrent low-grade tumors. They are also promising in differentiating between recurrent tumors and treatment-induced changes.
Malignant brain tumors are a heterogeneous group of diseases, each with its own biology, prognosis, and treatment. The most common tumor types are metastatic tumors and malignant gliomas. The American Cancer Society estimated that, in 2005, primary brain tumors were the cause of death of approximately 12,760 people. Metastatic tumors are more common; more than 100,000 people die per year with symptomatic intracranial metastases (1). The initial presentation and diagnostic approaches are similar, but the natural courses of disease are different. This article focuses on PET with 18F-FDG and 18F-labeled amino acid tracers in malignant gliomas and metastatic tumors, with a special focus on radiation necrosis, tumor recurrence, and PET-guided biopsy. The article discusses the clinical course and treatment of the tumors; clinical issues pertinent to neuroimaging; the benefits and limitations of the current gold standard, MRI; the role of the established PET tracer 18F-FDG; and the potential of PET tracers alternative to 18F-FDG, such as amino acid tracers, with emphasis on 18F-labeled amino acid tracers.
EPIDEMIOLOGY AND CLASSIFICATION OF GLIOMAS
According to the classification of the World Health Organization (WHO), gliomas are of 3 main types—astrocytomas, oligodendrogliomas, and mixed oligoastrocytomas—which can usually be distinguished by their histologic features (2). These tumors are typically heterogeneous in that different levels of malignant degeneration can occur in different regions within the same tumor. Analysis of the most malignant region of the tumors establishes grading: low-grade, or WHO grades I and II, and high-grade, or WHO grades III and IV. Grading is based on the degree of nuclear atypia, mitosis, microvascular proliferation, and necrosis, with increasing anaplasia as tumor grade increases. The histologic features of the tumor and the age and performance status of the patient are major prognostic factors on outcome (3). There are 3 subtypes of low-grade gliomas: pilocytic astrocytoma (grade I), astrocytoma (grade II), and oligodendroglioma (grade II). High-grade gliomas include anaplastic tumors (astrocytoma and oligodendroglioma, grade III) and glioblastoma (grade IV). Glioblastoma is the most malignant and most common glioma, accounting for 45%–50% of all gliomas (4). The mean age at onset is 61 y for glioblastoma and 40 y for anaplastic astrocytoma (5). Men are more frequently affected than women, with a sex ratio of 3:2. Low-grade tumors typically affect younger patients than do high-grade gliomas (fourth versus sixth decade of life).
TREATMENT AND OUTCOME
High-Grade Gliomas
The clinical course of glioblastoma is usually rapid and fatal, with a median survival of 1 y. Median survival for anaplastic tumors is 2–3 y.
The treatment for anaplastic astrocytoma and glioblastoma is similar. The current standard of care for newly diagnosed glioblastoma is surgical resection to the extent feasible, followed by adjuvant radiotherapy. Maximum resection is important to quickly relieve symptoms and to establish a diagnosis and is associated with lengthened survival and improved neurologic function (6–8). Postoperative radiation has provided a significant survival advantage over surgery alone (9,10). Long-term survival is less than 5% after surgical resection and radiation or chemotherapy (11). Conventional chemotherapy typically has yielded a response rate of 5%–10% (12). Concurrent radiation with the chemotherapy agent temozolomide has recently been shown to improve survival in patients with newly diagnosed glioblastoma, with a 2-y survival rate of 26.5% with radiotherapy plus temozolomide and 10.4% with radiotherapy alone (13,14).
After the initial treatment, these tumors invariably recur. Patients are treated with a variety of chemotherapeutic agents, and this treatment is an active area of investigation. Patients are followed clinically for neurologic symptoms and through neuroimaging with MRI, the current clinical gold standard. A rapidly enlarging, enhancing lesion on MRI with or without clinical symptoms usually establishes a diagnosis of progressing tumor. However, difficulty with distinguishing between tumor extent and treatment-induced changes such as radiation necrosis limits imaging of the extent of contrast enhancement in malignant gliomas (15). Difficulty also exists in evaluating treatment response with MRI, in that reliable prognostic information often cannot be obtained until many weeks after treatment starts (16).
Low-Grade Gliomas
Although both grade I and grade II gliomas are classified as low-grade tumors, they are diverse clinically. Grade I tumors such as pilocytic astrocytomas are well-circumscribed contrast-enhancing tumors. They develop mainly in children and young adults. As a rule, pilocytic astrocytomas grow slowly and stabilize spontaneously. Malignant transformation rarely occurs. Surgical resection alone leads to cure or long-term survival in most cases, with 80% of patients reaching a 20-y survival. Radiotherapy and possibly chemotherapy are reserved only for unresectable tumors in patients with progressive deficits (17). This article focuses on grade II tumors.
Low-grade gliomas are more indolent than their high-grade counterparts but are associated with significant neurologic disability and are fatal. Reference to these lesions as benign gliomas has generally been abandoned (18). Histologic features of anaplasia, including microscopic endothelial proliferation and necrosis, are absent. Mitotic activity is low. The proliferation index, assessed by MIB-1 antibody targeting the Ki-67 antigen expressed only in proliferative stages of the cell cycle, is generally low at 2%–4% (19). Tumor cells acquire genetic defects that result in anaplastic transformation to a high-grade lesion. At the time of tumor progression, 50%–70% lesions are of high grade (20,21). They may also progress without anaplastic transformation.
Optimal treatment of low-grade gliomas is controversial. Surgery has long been important in their diagnosis and treatment. Surgical resection of the full extent of the tumor is important in establishing an accurate diagnosis, because many tumors are heterogeneous. Recently, in 38% of 81 patients, a discrepancy was shown between the diagnosis made from small biopsy samples and the diagnosis made from resected specimens (22). Evidence exists that a radical resection may improve symptom control, particularly with regard to seizures (23). However, the impact of the timing and extent of surgery on patient outcome remains the subject of much debate (18). Earlier surgery does not seem to prevent or delay anaplastic transformation, and the effect of surgery on overall survival and progression-free survival is uncertain. Although radiotherapy has played an important part in the management of low-grade glioma, the efficacy and timing of this treatment have also been debated. A recent study of 311 patients demonstrated that radiation after the initial resection may improve progression-free survival but had no effect on overall survival (24).
Astrocytomas and oligodendrogliomas are radiographically indistinguishable, although oligodendrogliomas are more likely to be calcified. Recognition of oligodendrogliomas is important in that oligodendroglioma and, to a lesser extent, mixed oligoastrocytoma carry a better prognosis and greater responsiveness to chemotherapy than does pure astrocytoma (25,26). Oligodendroglial tumors have a more distinct genetic profile than do astrocytomas. Somatic deletions of chromosomes 1p and 19q are the most import events in tumorigenesis, occurring in about 40%–70% of tumors (27). In general, this deletion of 1p and 19q renders tumors more responsive to chemotherapy. The 5-y survival of patients with astrocytomas is around 37%, whereas 70% of patients with oligodendrogliomas are alive 5 y after diagnosis (28).
The general consensus is that early intervention is preferable in low-grade gliomas when increasing symptoms or radiographic progression is observed, because changes are frequently associated with dedifferentiation to a higher-grade tumor (18). Early and adequate tissue sampling is important given the potential for nonenhancing tumors to be anaplastic gliomas rather than low-grade gliomas. Maximal resection is an option in patients whose tumors can be resected. For younger patients who undergo a complete resection, periodic observation with MRI for clinical or radiographic signs of tumor recurrence is a viable option. Radiotherapy is recommended for older patients, especially if total resection is not possible. Chemotherapy is also an option, particularly for patients whose tumors harbor 1p/19q deletion.
Intracranial Metastasis
Cerebral metastases remain a common complication among patients with systemic cancer. The tumor types most likely to metastasize to the brain are lung, breast, and melanoma (29). Median survival for cerebral metastases remains less than 1 y, with most patients dying from systemic disease. Traditionally, these patients were treated with whole-brain irradiation, because many have multiple lesions. Surgery allows pathologic verification when diagnosis is uncertain. Surgery is indicated in patients with a relatively good performance status and in patients with large, solitary lesions associated with a significant mass effect. In patients who had solitary metastases and were randomized to whole-brain irradiation with or without surgical resection, surgery with whole-brain irradiation showed a survival advantage (30,31). Recently, stereotactic radiosurgery has emerged as an alternative to whole-brain irradiation and surgery, especially in surgically inaccessible lesions. Stereotactic radiosurgery allows the precise delivery of a high dose of radiation to a defined target in a single treatment session. Patients previously treated with radiotherapy can be retreated with stereotactic radiosurgery in the event of tumor progression. Stereotactic radiosurgery can also be used to treat patients with multiple lesions. Comparative studies of surgery and stereotactic radiosurgery have not been performed (29). Stereotactic radiosurgery is well tolerated, but necrosis is a complication that can occur several months later and may mimic tumor recurrence. Chemotherapy and targeted therapy are active areas of investigation for cerebral metastases.
IMAGING MODALITIES
Conventional Imaging Studies
The clinical gold standard, MRI, provides excellent anatomic details. Standard T1- and T2-weighted MRI is highly sensitive in determining the size and location of brain tumors, as well as mass effect, edema, hemorrhage, necrosis, and signs of increased intracranial pressure. Most high-grade tumors such as glioblastoma lead to destruction of the blood–brain barrier (BBB), with subsequent leakage of contrast medium. Low-grade tumors usually show no or minimal enhancement. A high-grade glioma normally presents as an irregular hypodense lesion on T1-weighted MRI, with various degrees of contrast enhancement and edema. Ringlike enhancement surrounding irregularly shaped foci of presumed necrosis is suggestive of glioblastoma. However, anaplastic tumors can often present as nonenhancing tumors, and even glioblastoma may present initially as a nonenhancing lesion, especially in older patients. Likewise, some tumors that appear to be of low grade may contain areas of anaplastic tumor. In addition, the low specificity of MRI in distinguishing neoplastic disease from vascular or inflammatory processes can be a problem in some cases.
It is clinically challenging to evaluate disease status with MRI in patients who have been treated. First, treatment-induced changes such as radiation necrosis can be difficult to distinguish from recurrent tumor (15,32). This issue is becoming clinically more critical now that concurrent chemoradiation and stereotactic radiosurgery are being used more extensively, because both treatments increase the prevalence of necrosis. Second, dexamethasone has been shown to reduce tumor size, as seen on MRI (33). Many glioma patients are under treatment with corticosteroids, and withholding this drug for the purpose of an imaging study would ethically not be feasible. Last, it is challenging with MRI to evaluate recurrent low-grade tumors without anaplastic transformation, because changes on MRI can often be difficult to distinguish from treatment-induced changes.
18F-FDG PET
Imaging of brain tumors with 18F-FDG was the first oncologic application of PET (34–36). 18F-FDG is actively transported across the BBB into the cell, where it is phosphorylated. 18F-FDG uptake is generally high in high-grade tumors. The prognostic value of 18F-FDG uptake is well established: High uptake in a previously known low-grade tumor establishes the diagnosis of anaplastic transformation (37,38).
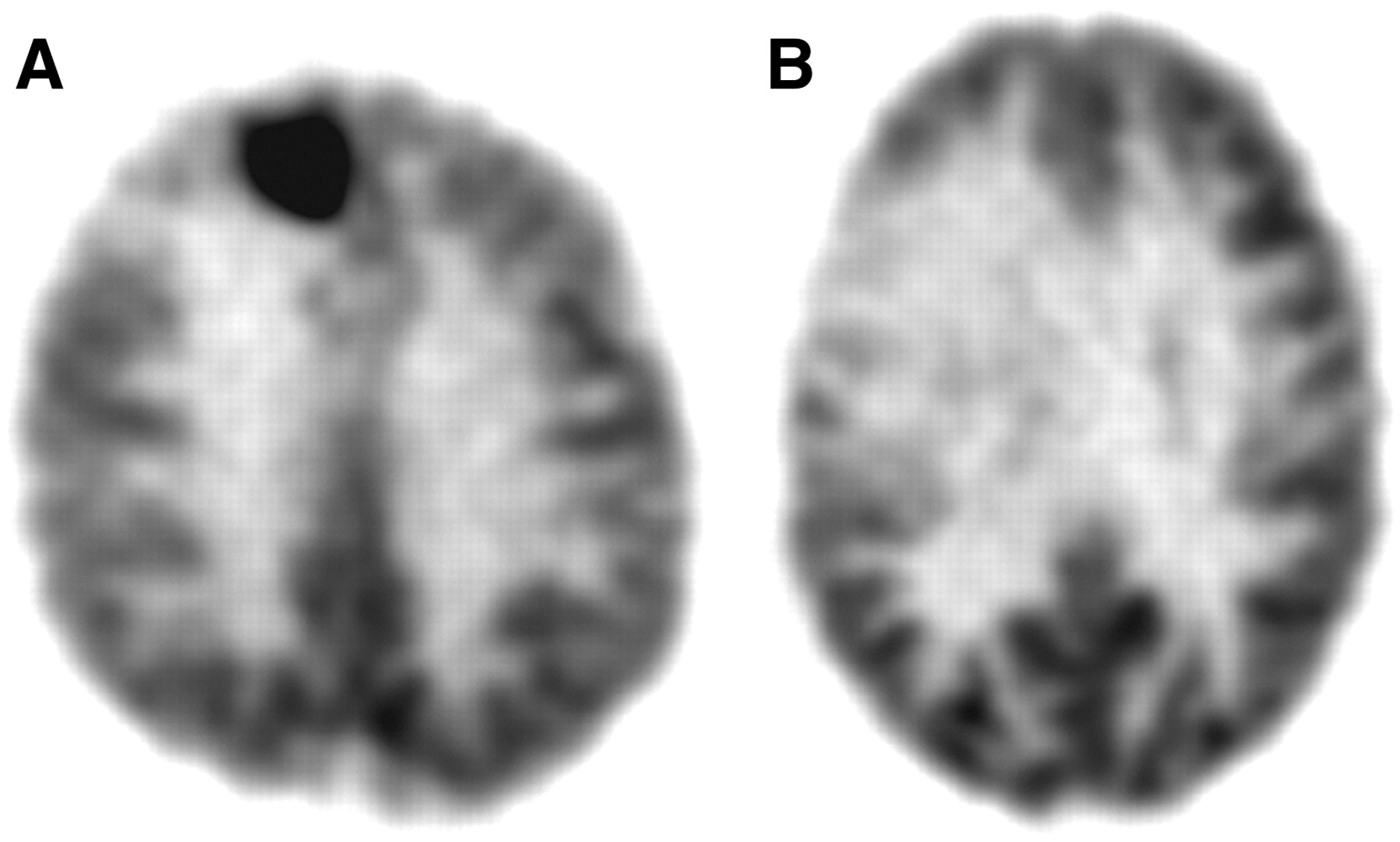
However, recent studies have demonstrated some diagnostic limitations of 18F-FDG PET (39,40). Because of the high rate of physiologic glucose metabolism in normal brain tissue, the detectability of tumors with only modest increases in glucose metabolism, such as low-grade tumors and in some cases recurrent high-grade tumors, is difficult. 18F-FDG uptake in low-grade tumors is usually similar to that in normal white matter, and uptake in high-grade tumors can be less than or similar to that in normal gray matter, thus decreasing the sensitivity of lesion detection (Fig. 1). Further, the coupling of 18F-FDG uptake and glucose metabolism in tumors can be radically different from that in normal tissue. It was demonstrated that 18F-FDG uptake in tumors could be increased whereas glucose metabolism could not (41). 18F-FDG uptake can vary greatly; high-grade tumors may have uptake that is only similar to or slightly above that in white matter, especially after treatment (36).

18F-FDG PET of newly diagnosed tumors: glioblastoma (A) and grade II oligodendroglioma (B).
Coregistration with MRI.
Coregistration of 18F-FDG PET images with MR images greatly improves the performance of 18F-FDG PET, and it is critical to have the MR images available while the 18F-FDG PET images are interpreted (42). Because recurring tumor may show 18F-FDG uptake equal to or lower than uptake in the normal cortex, reference to the MR image delineates the area of interest. In the area of interest, any 18F-FDG uptake higher than the expected background level in the adjacent brain should be considered recurrent tumor if that uptake corresponds to abnormalities on MRI, even though the uptake may be equal to or less than that in normal cortex (Fig. 2).
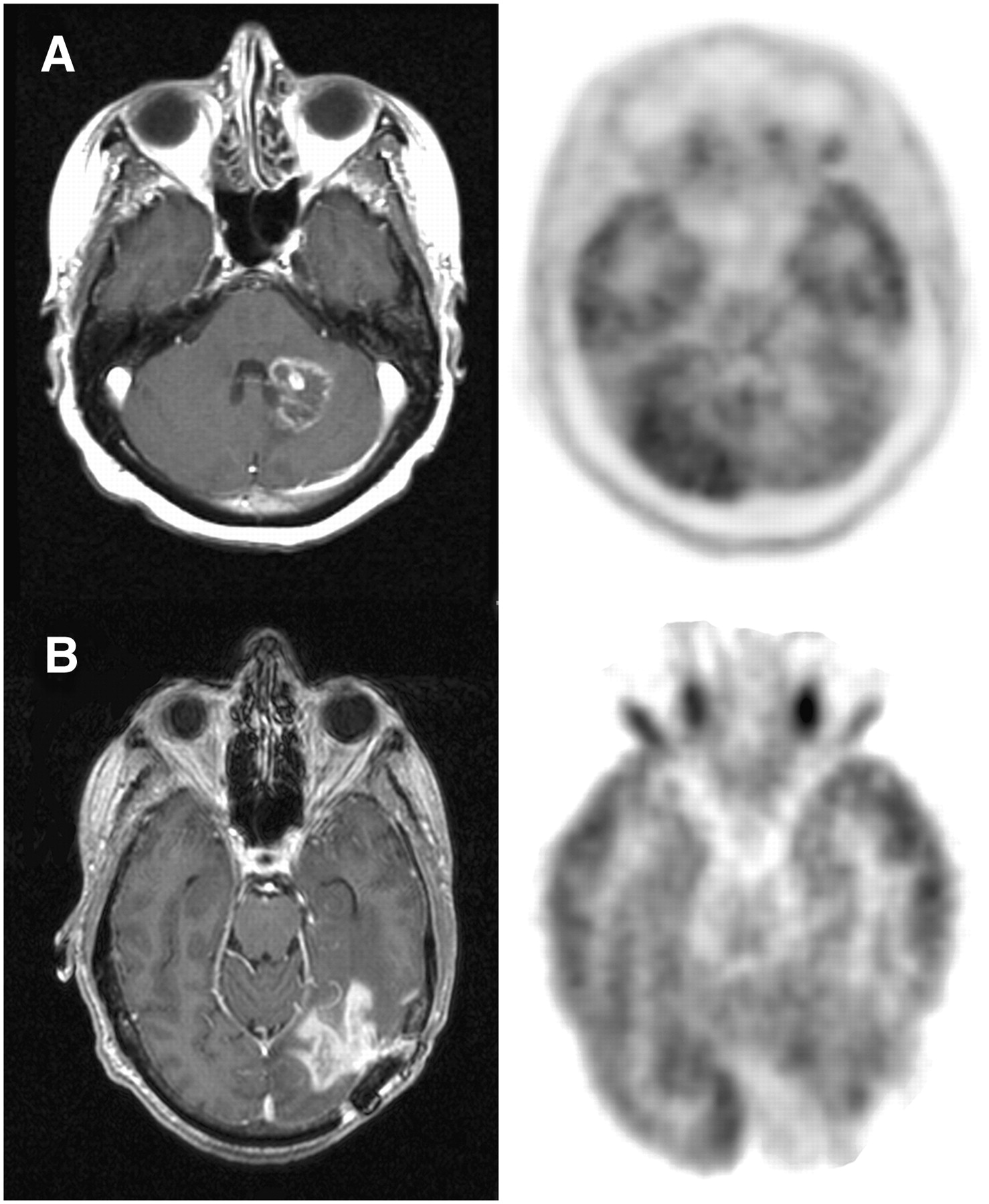
Image coregistration of 18F-FDG PET and MRI. (A) A 45-y-old woman with radiation necrosis. MRI showed a new contrast-enhancing lesion 4 mo after stereotactic radiosurgery for metastatic breast cancer. 18F-FDG PET showed mild uptake not higher than background level of adjacent brain tissue. Radiation necrosis was diagnosed, and MRI lesion regressed during follow-up. (B) A 54-y-old man with recurrent glioblastoma. MRI showed a new contrast-enhancing lesion. 18F-FDG PET showed moderate uptake lower than that of normal gray matter but higher than expected background level of adjacent brain tissue and corresponding to abnormal contrast-enhancing region on MRI. Surgery demonstrated recurrent glioblastoma with Ki-67 of 40%.
Delayed Imaging.
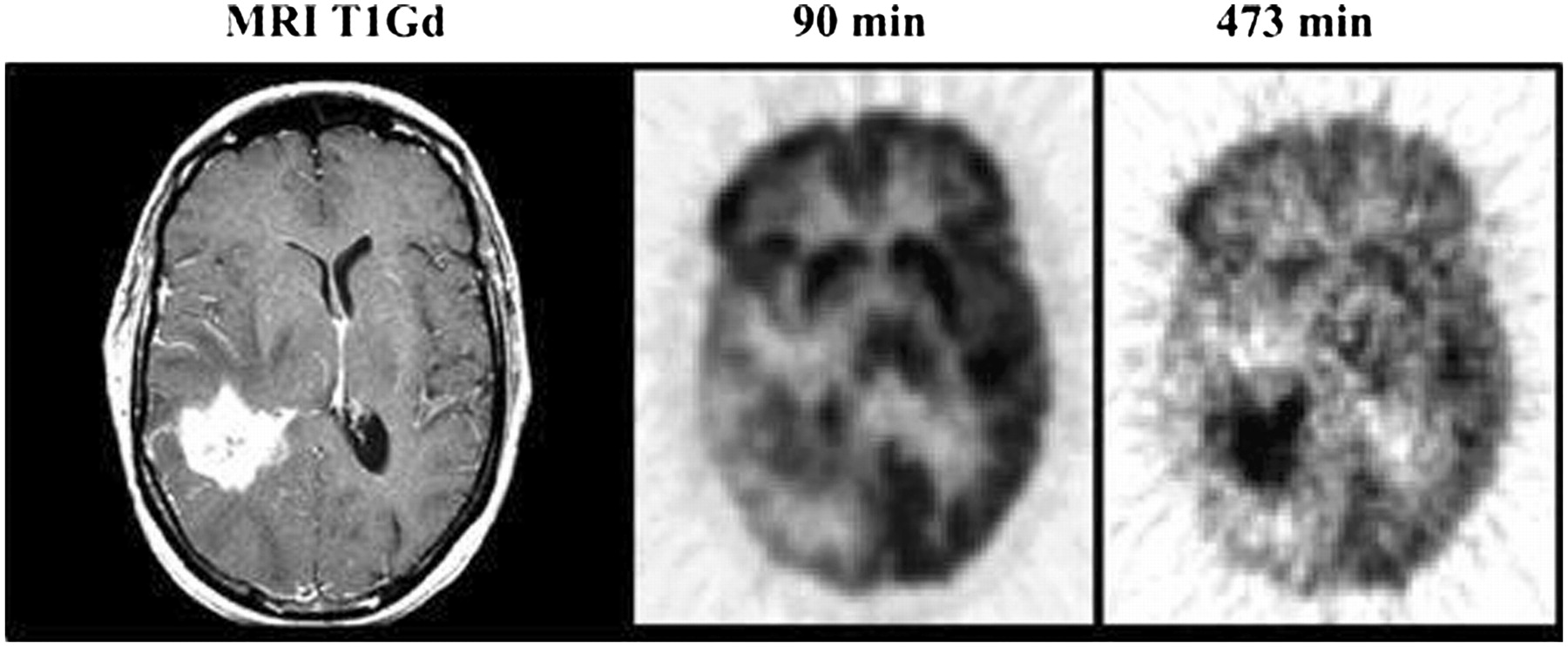
Early studies reported enhanced detection of brain tumors with glucose loading, with a 27% increase in the 18F-FDG uptake ratio of tumor to normal gray matter (43). However, glucose loading can be difficult to perform clinically because of the need for intravenous glucose infusion and blood glucose monitoring. Recently, an interesting study showed that 18F-FDG imaging 3–8 h after injection can improve the distinction between tumor and normal gray matter (44). The authors hypothesized that glucose excretion from the cells would be increased when the interval between 18F-FDG administration and PET data acquisition was extended, that this excretion would be greater in normal brain tissue than in tumor, and that delayed imaging might therefore improve the delineation of tumor from normal gray matter. Nineteen patients with gliomas were imaged form 0 to 90 min and once or twice later at 180–480 min after injection. In 12 of 19 patients, visual analysis of delayed images up to 8 h after injection showed these images to better distinguish the high uptake in tumors from uptake in gray matter (Fig. 3). Standardized uptake values (SUVs) were also greater in tumors than in normal gray or white matter on delayed imaging. The authors used kinetic modeling to demonstrate that the rate constant of FDG-6-phosphate degradation k4 values was not significantly different between tumor and normal brain tissue at early imaging times but was lower in tumor than in normal brain tissue at delayed times, suggesting that higher FDG-6-phosphate degradation at delayed times may be responsible for higher excretion of 18F-FDG from normal tissue than from tumor.
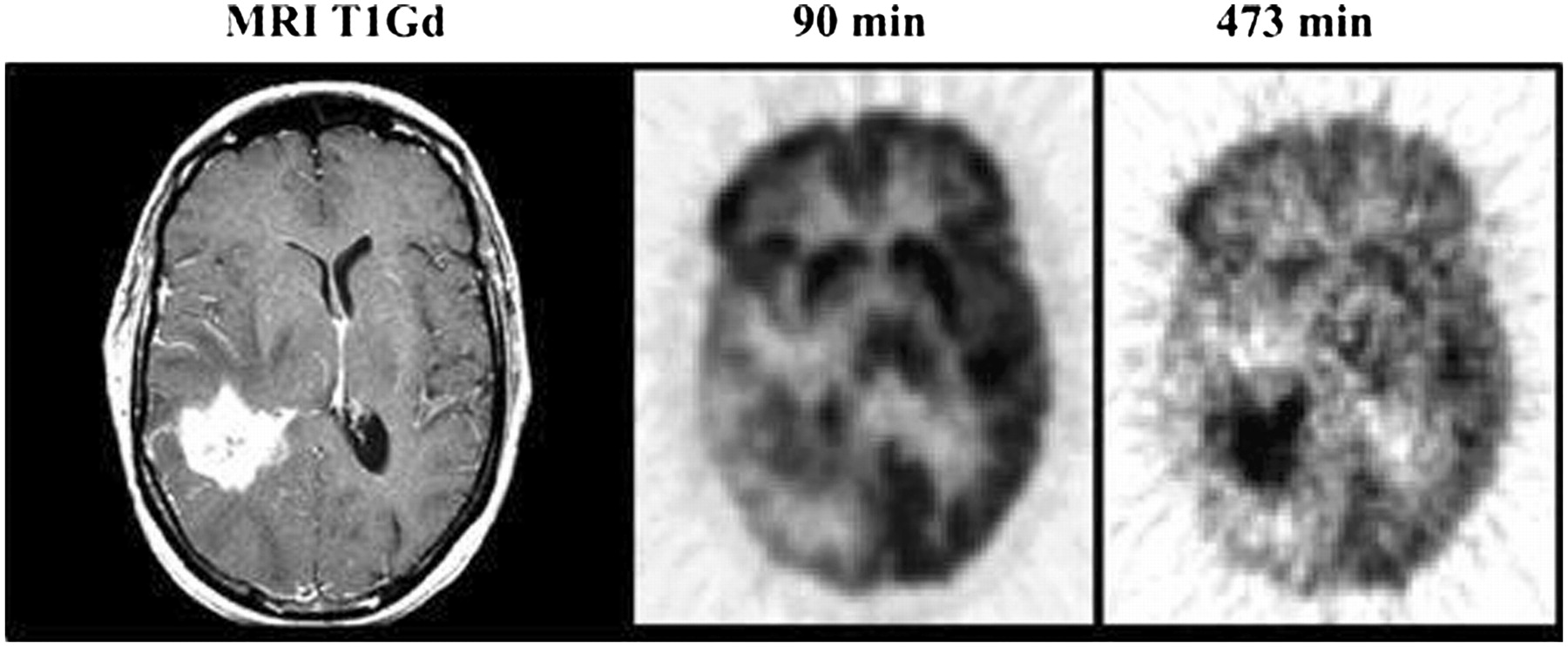
A 45-y-old woman with recurrent right temporal glioblastoma. MRI shows contrast enhancement. Tumor–to–gray matter delineation is more prominent later, at 473 min, than at 90 min. (Adapted from (44).)
Amino Acid PET Tracers
Amino acid PET tracers and amino acid analog PET tracers constitute another class of tumor-imaging agents (45,46). They are particularly attractive for imaging brain tumors because of the high uptake in tumor tissue and low uptake in normal brain tissue and, thus, higher tumor–to–normal-tissue contrast. The best-studied amino acid tracer is 11C-methionine (47). Because of the short half-life of 11C (20 min), 18F-labeled aromatic amino acid analogs have been developed for tumor imaging (48). Tumor uptake of O-(2-18F-fluoroethyl)-l-tyrosine (FET) and 3,4-dihydroxy-6-18F-fluoro-l-phenylalanine (FDOPA) has been reported to be similar to that of 11C-methionine (49,50). The 18F-FDOPA metabolite 3-O-methyl-6-18F-fluoro-l-DOPA has also been investigated for brain tumor imaging with PET (51). The diagnostic accuracy of 18F-FDOPA was recently reported to be superior to that of 18F-FDG in evaluating recurrent low-grade and high-grade gliomas (52).
Amino acids are transported into the cell via carrier-mediated processes (53). Amino acid imaging is based on the observation that amino acid transport is generally increased in malignant transformation (54,55). In animal models, upregulation of the amino acid transporter in the supporting vasculature of brain tumor tissue has been shown responsible for increased facilitation of amino acid transport into the tumor cell (56). Factors involved in this active transport have been reviewed: flux of the amino acid to the tissue, the intrinsic activity of the amino acid transporter, and the rate of intracellular amino acid metabolism (48). Amino acid transport is generally accepted to be the rate-limiting step, even for the few amino acid tracers that are incorporated into the proteins. The relationship between proliferative activity and amino acid transport was investigated in 3 glioma cell lines (57). The authors elegantly demonstrated, using nonmetabolized amino acid, that increased amino acid transport in tumor cells involves all phases of the cell cycle and that upregulation of amino acid transport (L and A systems) occurs in the absence of increased vascular permeability. Thus, amino acid transport is increased in tumor cells regardless of the phase of the cell cycle, and this upregulation of transport does not depend on breakdown of the BBB. An earlier study showed that amino acid transport into brain tumors does not depend on, but may be enhanced by, a breakdown in the BBB (58). Uptake of 11C-methionine was significant in low-grade astrocytoma but not as high as in glioblastoma. However, 11C-methionine uptake was even higher in meningioma (lack of BBB) than in glioblastoma. In contrast, 18F-FDG uptake is higher in glioblastoma than in meningioma. Therefore, transport across the BBB is not the rate-limiting step for 18F-FDG, whereas transport across the BBB does appear to be the rate-limiting step for amino acid tracers such as 11C-methionine. Transport of the 18F-amino acid analog 3-O-methyl-6-18F-fluoro-l-DOPA via sodium-independent, high-capacity amino acid transport systems has been demonstrated in tumor cell lines (59).
EVALUATION OF DISEASE STATUS
Radiation Necrosis
The actual incidence of radiation necrosis is not known because few studies have been performed on patients treated with radiation only, and chemotherapy is known to increase the risk of radiation necrosis when both modalities are used (60). Now that stereotactic radiosurgery is used more extensively, and now that it has become standard practice to combine chemotherapy with radiation for high-grade gliomas, the incidence of radiation necrosis is likely to increase. The types of radiation injuries have been reviewed previously (Table 1). Acute injury involves tumor swelling and occurs hours to weeks after the completion of radiation. This type of injury usually is reversible and has a good prognosis. Early delayed injury involves demyelination, occurs weeks to months after the completion of radiation, and also is reversible. Late injury involves liquefactive or coagulative necrosis and usually is irreversible. Late injury can occur months to years after the completion of radiation. The pattern of radiation injury may vary from diffuse periventricular white matter lesions to focal or multifocal lesions. Radiation injury may also occur distant from the original treatment (61). Radiation necrosis is difficult to differentiate from tumor growth on MRI and is especially challenging in early delayed and late injuries because recurring tumor can occur along the same time lines.
Characteristics of Radiation Injuries
18F-FDG PET.
Early studies reported that 18F-FDG PET had a sensitivity of 81%–86% and a specificity of 40%–94% for distinguishing between radiation necrosis and tumor (62). In general, methods to define a cutoff SUV were not reliable, because the relative use of glucose and 18F-FDG varied widely for brain tumors and was different from that for normal brain (41,63). Attempts to use the ratio of lesion to contralateral normal white matter or gray matter yielded poor results (40), although this finding was a subject of controversy because another group achieved good results using receiver-operating-characteristic analysis (64). This difficulty with using the ratio approach to diagnose recurrent tumor was due to the fact that an area of treated brain has a wide range of background metabolic activity and usually is of lower metabolic activity than normal untreated brain. Recurring tumors can have a similarly varied degree of metabolic activity that also can frequently be lower than that of normal brain. Diagnostic performance appears better in gliomas than in metastatic lesions and is worse in lesions treated with stereotactic radiosurgery (60).
Thus, when one is interpreting 18F-FDG PET images of a treated brain to distinguish recurrent tumor from radiation necrosis, it is critical to evaluate lesion activity not by the absolute uptake value, and not by the ratio to untreated normal brain tissue, but by whether lesion activity is above the expected background activity in adjacent brain tissue. It is also critical to have the MRI structural information available for correlation. In a series of 44 lesions treated with stereotactic radiosurgery, 18F-FDG PET alone had a sensitivity of 65% in subjects with metastases but reached 86% when MRI and PET images were coregistered (65). Any area of 18F-FDG uptake higher than the expected background activity in adjacent brain tissue was considered suggestive, as was any area of 18F-FDG uptake in a region showing contrast enhancement on coregistered MR images (Fig. 2). A series of 117 postradiotherapy patients demonstrated a sensitivity of 96% and specificity of 77% in distinguishing recurrent tumor from radiation necrosis when such criteria were used (66).
Much of the wide range of 18F-FDG PET performance in evaluating radiation necrosis may be attributable to differences in the timing of PET after radiation, in the type of radiation, and in the type of tumor. 18F-FDG uptake was shown to vary with the timing after radiation treatment, and overlap of 18F-FDG uptake between radiation necrosis and residual tumor could be considerable (67). The optimal time for performing 18F-FDG PET after radiation is not known (67). The general recommendation is that, for the purpose of evaluating tumor growth, 18F-FDG PET should not be performed less than 6 wk after the completion of radiation treatment.
A potentially useful approach would be to use delayed imaging, because it apparently enhances the tumor–to–normal-brain uptake ratio (44). An attractive hypothesis is that, like normal brain tissue, necrotic tissue would show greater 18F-FDG excretion at delayed times than would tumor. Further studies are needed to evaluate whether this approach can increase diagnostic accuracy in distinguishing radiation necrosis from recurrent tumor.
Other PET Tracers.
Because amino acid tracers appear more sensitive than 18F-FDG PET in visualizing tumor, they also have potentially better diagnostic performance than 18F-FDG PET in evaluating radiation necrosis. However, the degree of amino acid uptake in radiation necrosis lesions is not well known. 11C-Methionine has been available for 2 decades, but few studies have been published on its performance in differentiating radiation necrosis from brain tumor recurrence (60). In a study of 21 patients with brain metastases treated by stereotactic radiosurgery, 11C-methionine correctly identified 7 of 9 recurrences and 10 of 12 radiation injuries (68).
In rats, uptake of 18F-FET, 18F-FDG, and 18F-choline has been compared in acute lesions caused by cerebral radiation injury (inflammatory cells) and in acute cryolesions (disruption of BBB) (69). Both 18F-FDG and 18F-choline accumulated in macrophages, a common inflammatory mediator in radiation necrosis, but 18F-FET uptake was absent from macrophages. Moreover, the ratio of 18F-FET uptake in radiation necrosis to that in normal cortex was much lower than the corresponding ratios for 18F-FDG and 18F-choline, suggesting that 18F-FET is promising for differentiating radiation necrosis from tumor recurrence. Absence of 18F-FET uptake in a case of radiation necrosis has been reported (49). In a recently reported study with 18F-FDOPA, a lesion–to–normal-brain ratio of less than 1.6 and a lesion-to-striatum ratio of less than 1.0 were demonstrated in 4 cases of radiation necrosis (from treatment of metastatic lung cancer, metastatic melanoma, glioblastoma, and grade III astrocytoma) (52). Although these results appear promising, larger systematic studies are needed to evaluate the accuracies of these amino acid tracers in differentiating radiation necrosis from recurrent tumor.
Evaluation of Recurrent Tumors
18F-FDG PET.
High 18F-FDG uptake in a previously diagnosed low-grade glioma with low 18F-FDG uptake is diagnostic of anaplastic transformation (Fig. 4). This increase in 18F-FDG uptake is strongly prognostic. Twenty-eight patients with low-grade glioma were studied with 18F-FDG PET and followed for a mean of 27 mo (38). All 19 patients with tumors that were hypometabolic on PET were alive at the end of the follow-up period, whereas 6 of 9 patients with hypermetabolic patterns on PET had died.
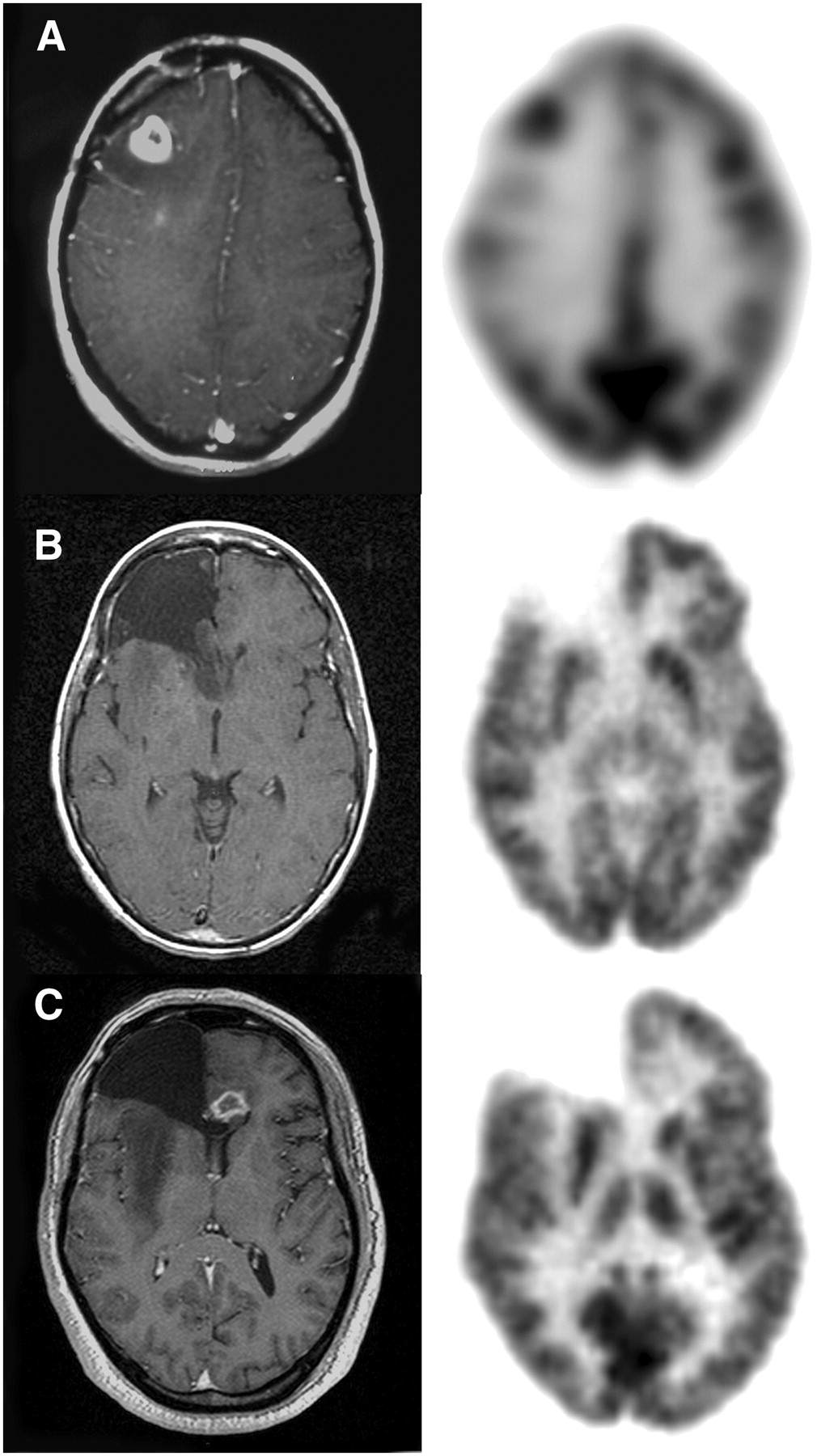
MRI and 18F-FDG PET of recurrent tumors. (A) Anaplastic transformation in previously resected and irradiated grade II astrocytoma. Intense 18F-FDG uptake corresponds to new contrast-enhancing lesion on MRI. (B) Recurrent grade II oligodendroglioma. No increased 18F-FDG uptake is seen. (C) Patient with previously resected and irradiated right frontal grade II astrocytoma. New contrast-enhancing lesion in left frontal lobe corresponds to minimally increased 18F-FDG uptake. This lesion was resected, and grade IV tumor was found.
18F-FDG PET performs generally well in identifying growing high-grade gliomas. In lesions that are equivocal on MRI, 18F-FDG PET may have limited sensitivity (52). 18F-FDG PET is generally not sensitive in identifying recurrent low-grade tumors without anaplastic transformation (Fig. 4).
Amino Acid Tracers.
In contrast to 18F-FDG uptake, amino acid uptake has been shown to be increased relative to normal brain tissue in most low- and high-grade tumors, and radiolabeled amino acids might therefore be preferable for evaluating recurrent tumors (47). Initial research focused on 11C-labeled amino acids, particularly 11C-methionine (40). However, because of the short half-life of 11C, the applicability of this tracer is limited to facilities with on-site cyclotrons, and the demand for 18F-labeled analogs has been increasing.
The usefulness of 11C-methionine PET in 45 brain lesions that did not show increased uptake on 18F-FDG PET was evaluated (70). Thirty-four of these lesions were at the initial presentation, and 11 were being evaluated for recurrence. There were 24 gliomas, 5 metastatic tumors, 4 meningiomas, 2 other brain tumors, and 10 benign lesions. 11C-Methionine demonstrated increased uptake in 31 of 35 tumors (89% sensitivity). For 24 gliomas, 11C-methionine demonstrated positive uptake in 22 (92% sensitivity). All 10 benign brain lesions (cysticercosis, radiation necrosis, tuberculous granuloma, hemangioma, organized infarction, and benign cyst) showed normal or decreased 11C-methionine uptake (100% specificity). 11C-Methionine was false-negative in cases of intermediate oligodendroglioma, metastatic tumor, chordoma, and cystic ganglioma.
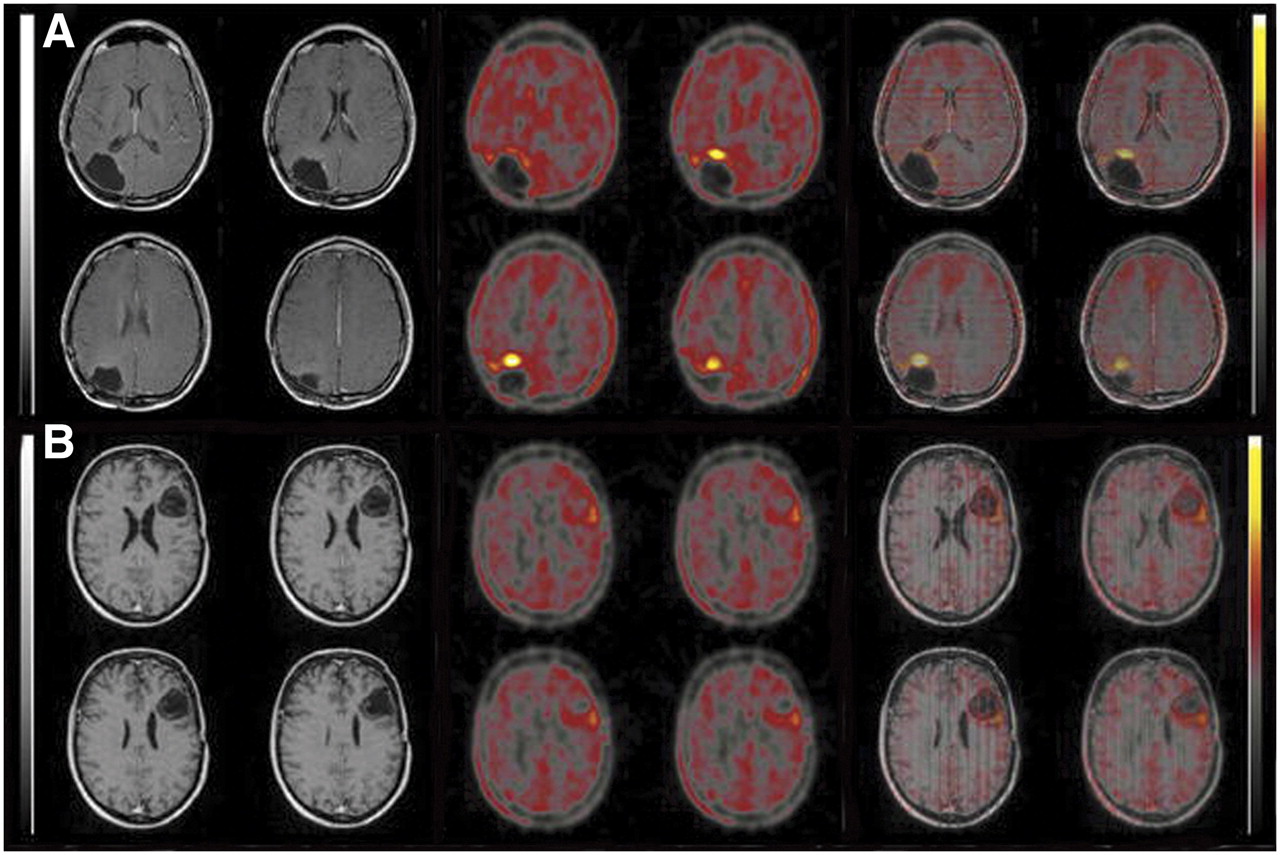
An initial study demonstrated that uptake of 18F-FET in brain tumors is similar to that of 11C-methionine (49). The diagnostic value of 18F-FET PET was evaluated in 53 patients with clinically suspected recurrent glioma (71). All patients had gliomas and initially underwent surgery and various additional treatments. Forty-three patients initially had high-grade gliomas and 10 patients had low-grade gliomas. All 42 patients with confirmed recurrent tumors had focally increased 18F-FET uptake, whereas only low, homogeneous 18F-FET uptake was seen at the margins of the resection cavity in the 11 patients without recurrence. Thus, 18F-FET was able to distinguish between recurrent tumor and therapy-induced benign changes with 100% accuracy. In this study, focal and high 18F-FET uptake was considered suggestive of tumor recurrence, whereas low and homogeneous uptake around the resection cavity was considered a benign posttreatment change (Fig. 5). Assuming that the expression of amino acid transporters is upregulated in tumor tissue but not in tissues affected by posttreatment changes, one can attribute increased amino acid uptake into this tissue mainly to treatment-induced disruption of the blood–brain barrier. The best differentiation between benign posttreatment changes and recurrent tumor was found at a threshold of 2.0 for the ratio of maximum SUV to background or a threshold of 2.2 for the absolute maximum SUV. Using the maximum SUV or an 80% isocontour yielded similar results. The diagnostic accuracy of 18F-FET PET and MRI was compared in 45 patients with 34 high-grade and 11 low-grade gliomas (72). 18F-FET PET and MRI produced a correct diagnosis in 44 and 36 patients, respectively. When a threshold of 2.2 was used for the maximum SUV, the specificity of 18F-FET PET was 92.9% and the sensitivity was 100%. The sensitivity of MRI was 93.5% and the specificity was 50%. 18F-FET PET was concordant with MRI in 37 patients and discordant in 8 patients. The authors cautioned that the high sensitivity and specificity of 18F-FET PET may be due to the fact that tumor recurrence was suspected in all patients on the basis of the MRI findings. The authors also suggested that because MRI has high sensitivity but poor specificity, it should be used first, as a screening test. In the event of suspected tumor recurrence, additional 18F-FET PET investigation seems to differentiate between posttreatment changes and tumor recurrence and to avoid both under- and overtreatment.
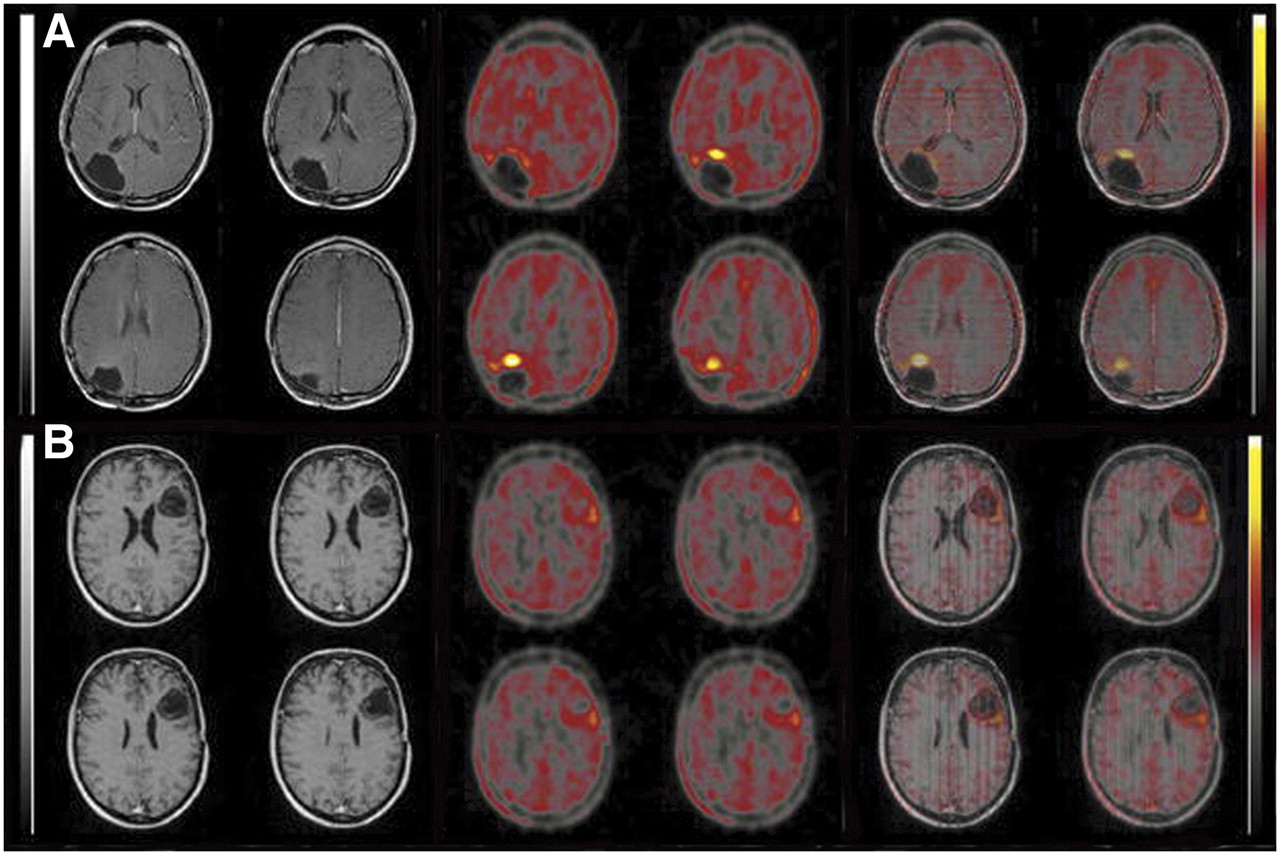
MRI, 18F-FET PET, and fused images. (A) A 30-y-old man who had undergone initial surgery, radiation therapy, and intralesional radioimmunotherapy for anaplastic astrocytoma. Biopsy-proven recurrent tumor (WHO grade IV) occurred 20 mo after initial diagnosis. MRI shows no contrast enhancement and was rated normal. PET shows focal 18F-FET uptake. Maximal SUV is 3.0, with ratio of 4.0 to background. (B) A 42-y-old woman who had undergone initial surgery and radiation therapy for WHO II astrocytoma. This patient was proven free of tumor by biopsy 67 mo after initial diagnosis. MRI shows suggestive contrast enhancement at border of cavity, whereas only moderate 18F-FET uptake is present on PET. Maximal SUV is 1.7, with ratio of 1.75 to background. (Adapted from Figure 1 of (71) with the kind permission of Springer Science and Business Media.)
In general, 18F-FET PET has not been shown useful in differentiating low- from high-grade tumors, although some investigators reported that the kinetic profile in 18F-FET uptake for low- and high-grade tumors might be a useful feature for distinguishing the 2 types of tumors (73).
For many years, 18F-FDOPA imaging of the integrity of the striatal dopamine pathway has been used to evaluate patients with movement disorders (74–76). However, 18F-FDOPA is also an amino acid analog and was shown to be taken up at the BBB in normal brain by the neutral amino acid transporter (77,78). The initial report of 18F-FDOPA imaging of a glioma was as an incidental finding in a patient undergoing evaluation of movement disorders (79). Subsequently, 18F-FDOPA PET and 11C-methionine PET of brain tumors were compared in 19 patients (50). No significant difference in uptake between 18F-FDOPA and 11C-methionine was found in either low- or high-grade tumors.
The most detailed and comprehensive study of 18F-FDOPA in brain tumors was published last year. 18F-FDOPA was compared with 18F-FDG in 30 patients with brain tumors, and the diagnostic accuracy of 18F-FDOPA was evaluated in a subsequent expansion of the study to an additional 51 patients (52). Initially, 30 patients with brain tumors, newly diagnosed or previously treated, were prospectively studied. The distribution of cases based on the WHO histopathologic classification was as follows: 7 patients had newly diagnosed glioma (3 grade II, 1 grade III, and 3 grade IV), and 23 were previously treated with surgical resection or radiation (original primary tumors: 2 grade II, 3 grade III, and 15 grade IV; metastatic brain tumors: 1 breast, 1 lung, and 1 melanoma). All patients were studied with 18F-FDOPA and 18F-FDG PET within the same week. MRI studies of the brain were acquired in all patients within 1 wk before the PET scans. The accuracy of the imaging data was validated by histology or subsequent clinical follow-up.
Time–activity curves demonstrated that the highest tracer uptake in tumor and cerebellum generally occurred between 10 and 30 min after injection. Tracer activity in the striatum did not peak until 50 min after injection. Thus, tumor uptake from 10 to 30 min after injection is near maximum and occurs sufficiently early to avoid peak uptake in the striatum.
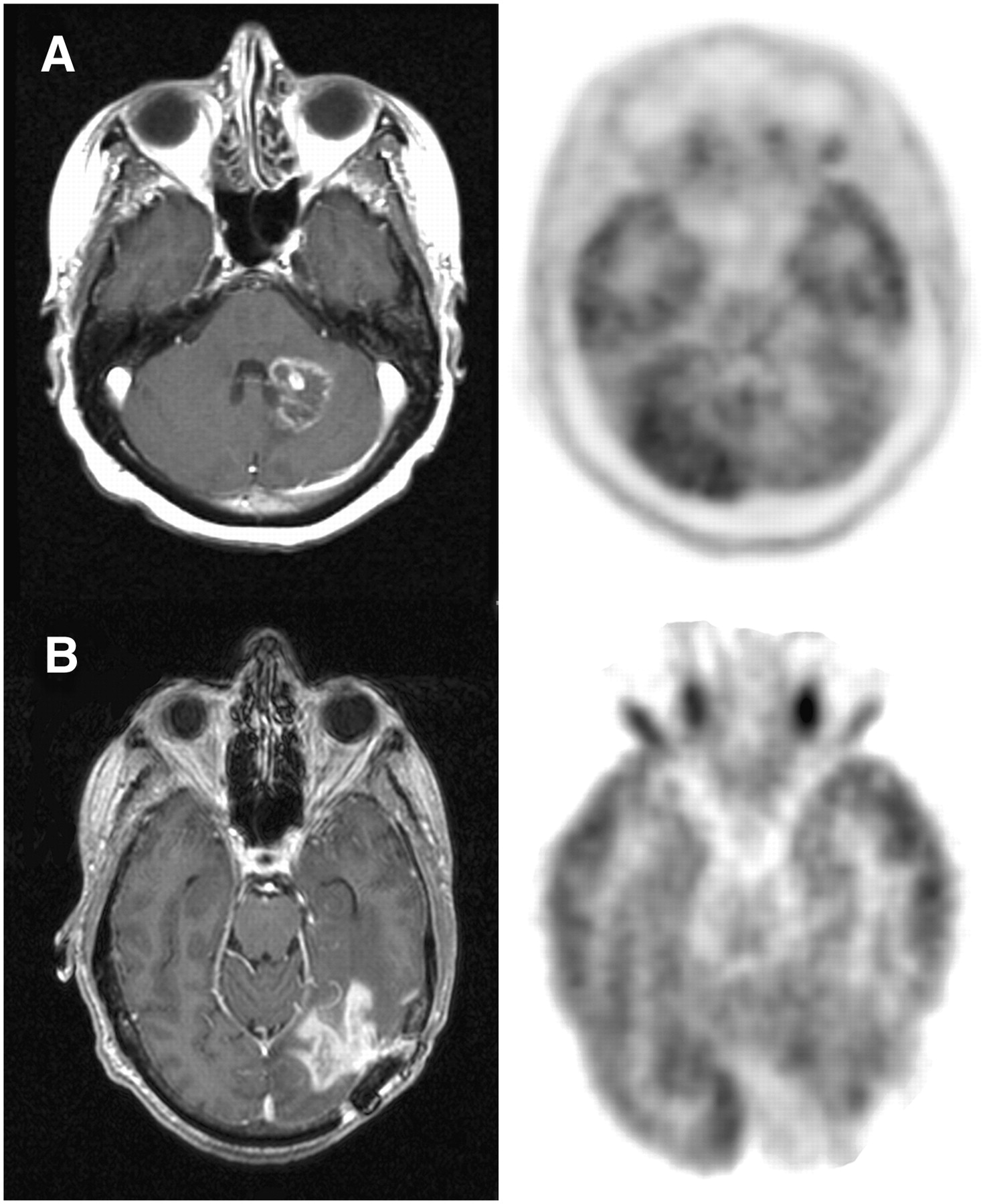
With the criterion that any tracer activity above the background level of adjacent brain be considered abnormal, 22 of 23 high- and low-grade tumors were visualized with 18F-FDOPA, with 1 false-negative finding occurring in a patient with residual low-grade tumor (Fig. 6). All 3 patients without active disease (in long-term remission) lacked visible uptake on 18F-FDOPA PET scans. Four patients with radiation necrosis had low but visible 18F-FDOPA uptake. Thus, 18F-FDOPA had a sensitivity of 96% and a specificity of 43%, with an overall accuracy of 83% (95% confidence interval, 70%–97%). The corresponding positive predictive value was 85%, and the negative predictive value was 75%.

MRI, 18F-FDG PET, and 18F-FDOPA PET of newly diagnosed tumors: glioblastoma (A) and grade II oligodendroglioma (B). (Reprinted from (52).)
With the same visual criterion, 14 of 23 tumors were visualized using 18F-FDG PET (sensitivity, 61%). Similar to 18F-FDOPA, 18F-FDG showed no visible uptake in 3 stable patients in long-term remission and showed a low level of uptake in 4 patients with radiation necrosis (specificity, 43%). Thus, 18F-FDOPA was more sensitive overall than 18F-FDG in identifying tumors. 18F-FDOPA PET in gliomas demonstrated lower SUVs than did 18F-FDG. However, the contrast between tumor and normal tissue was higher than that with 18F-FDG because of the low 18F-FDOPA uptake in normal brain tissue. This higher contrast proved useful in detecting low-grade and recurrent tumors. For example, 8 of 9 recurrent tumors were negative for uptake on 18F-FDG PET but positive on 18F-FDOPA PET (Fig. 7). Of these 9 patients, 5 had low-grade and 4 had high-grade tumor. If only high-grade tumors were considered, 18F-FDG sensitivity would be 78% (14/18), rather than 61% (14/23), in detecting recurrent tumors, compared with 96% for 18F-FDOPA (22/23). 18F-FDOPA may thus help to detect low-grade and recurrent tumors with greater sensitivity than 18F-FDG.

Use of MRI, 18F-FDG PET, and 18F-FDOPA PET in evaluating recurrent tumors: glioblastoma (A) and grade II oligodendroglioma (B). (Reprinted from (52).)
Standard visual analysis of 18F-FDOPA PET seemed adequate in that it provided a high sensitivity in identifying tumor. However, the specificity was low because all radiation necrosis lesions had low but visible tracer uptake. Therefore, receiver-operating-characteristic analysis was used to identify the 18F-FDOPA uptake ratio for tumor to normal tissue that would give the best sensitivity and specificity: tumor to normal contralateral hemisphere (T/N), tumor to striatum (T/S), or tumor to white matter (T/W). The specificity of 18F-FDOPA brain tumor imaging could be greatly increased by using a T/S threshold of 0.75 or 1.0, a T/N threshold of 1.3, or a T/W threshold of 1.6.
18F-FDOPA PET was subsequently expanded to a larger population of 51 patients to test these thresholds generated from receiver-operating-characteristic analysis of the first 30 patients studied (Table 2). Three patients had newly diagnosed gliomas (2 grade II and 1 grade III), and 47 patients were evaluated for recurrence (original primary tumors: 13 grade II, 13 grade III, and 21 grade IV). One newly identified lesion was subsequently found to be benign reactive changes. Thresholds of 0.75 or 1.0 for T/S, 1.3 for T/N, and 1.6 for T/W were used to test the sensitivity, specificity, positive predictive value, and negative predictive value (Table 3).
Clinical Characteristics of Groups 1 and 2 for 18F-FDOPA Study
Diagnostic Accuracy with 18F-FDOPA PET Using Various Tumor–to–Normal-Tissue Thresholds in Groups 1 and 2
Although a T/S ratio of 0.75 resulted in a slightly higher accuracy of 95% and sensitivity of 98%, a ratio of 1.0 provided slightly lower sensitivity, 92%, but higher specificity, 95% (Table 3). The latter ratio is clinically more practical because it does not require quantitative measurement, is visually more obvious, and is still highly accurate (accuracy of 93%, with positive predictive value of 98% and negative predictive value of 80%). The authors suggested using a T/S of 1.0 for first-line assessment and a T/S of 0.75 in inconclusive cases. In addition, one could use a T/S of 1.0 when clinical suspicion of radiation necrosis is higher and a T/S of 0.75 when clinical suspicion of recurrent tumor is higher.
Tumor grade did not significantly affect tracer uptake in 81 lesions in 18F-FDOPA PET studies, a finding that is consistent with most studies using amino acid tracers (51–53). Likewise, no statistically significant difference in uptake levels was seen between contrast-enhancing tumors and nonenhancing tumors, in agreement with the notion that similar to tumor accumulation of other amino acid tracers, tumor accumulation of 18F-FDOPA activity is most likely mediated through a specific transport system, rather than requiring breakdown of the BBB (56).
18F-FDOPA demonstrated excellent visualization of high- and low-grade tumors and was more sensitive and specific than 18F-FDG for evaluating recurrent tumors. 18F-FDOPA may prove particularly valuable for examining recurrent low-grade gliomas because these tumors are difficult to evaluate by MRI and are usually not visible on 18F-FDG PET. The study also suggested that 18F-FDOPA might be valuable for distinguishing recurrent tumor from radiation necrosis, although a larger series of radiation necrosis cases is needed for confirmation.
PET GUIDANCE OF DIAGNOSIS AND THERAPY
PET-Guided Biopsy
Brain tumors are histologically heterogeneous. MRI-guided stereotactic biopsy does not always yield a valid diagnosis or tumor grading, because some regions of the nonenhancing tumors may be high-grade. Accurate grading and diagnosis are especially important for directing the therapeutic approach and providing the prognosis in patients with nonresectable tumors. 18F-FDG PET–guided biopsy has previously been reported (80). Because amino acid tracers have shown higher sensitivity in imaging tumors that, with 18F-FDG, are either hypo- or isometabolic to normal cortex, combining 18F-FDG and an amino acid tracer for guidance of biopsy has been investigated.
The combination of 18F-FDG and 11C-methionine for guidance of stereotactic biopsy was studied in 32 patients with unresectable gliomas (81). The double-tracer approach was proposed for these patients because they presented with a tumor considered unresectable and located in the cortical or subcortical gray matter—hence, likely of lower sensitivity on 18F-FDG. PET images were coregistered with MRI and were analyzed to determine which tracer offered the best information for target definition. All 32 patients had histologically documented glioma: 10 glioblastomas, 12 anaplastic astrocytomas, and 10 low-grade gliomas. 18F-FDG uptake was equal to or less than uptake in the surrounding gray matter in 18 patients, including 3 with glioblastoma, 6 with anaplastic astrocytoma, and 9 with low-grade glioma. 18F-FDG was used for target selection when its uptake was higher in tumor than in gray matter (14 patients). 11C-Methionine was used for target selection when 18F-FDG uptake was less than or equal to uptake in gray matter (18 patients). Sixty-one of the 70 stereotactic trajectories were based on PET-defined targets and showed abnormal 11C-methionine uptake. All 61 11C-methionine–positive trajectories yielded a diagnosis of tumor. The remaining 9 trajectories were 11C-methionine–negative and nondiagnostic. The authors concluded from the study that because 11C-methionine provides a more sensitive signal, it is the tracer of choice for single-tracer PET-guided neurosurgical procedures on gliomas.
The added value of 18F-FET PET was investigated in 31 patients with suspected gliomas (82). PET and MRI were coregistered, and 52 neuronavigated tissue biopsies were taken from lesions with both an abnormal MRI signal and increased 18F-FET uptake (match), as well as from areas with an abnormal MRI signal but normal 18F-FET uptake or vice versa (mismatch). 18F-FET findings were negative in 3 patients with an ischemic infarct and demyelinating disease, and these 3 patients were excluded from the study. Of the remaining 28 patients, tumor was diagnosed in 23 and reactive changes were found in the other 5. The diagnostic performance of MRI alone was compared with that of MRI combined with 18F-FET. MRI yielded a sensitivity of 96% for the detection of tumor tissue but a specificity of 53%. Combined use of MRI and 18F-FET PET yielded a sensitivity of 93% and a specificity of 94%. Thus, the authors concluded that combined use of MRI and 18F-FET PET significantly improves the identification of tumor tissue.
The predictive value of 18F-FET PET and MRI spectroscopy was compared in 50 patients with suspected diffused gliomas (83). Lesion-to-brain ratios greater than 1.6 for 18F-FET uptake were considered indicative of tumor. The results of MRI spectroscopy were considered positive when N-acetylaspartate was decreased in conjunction with an absolute increase of choline and an N-acetylaspartate–to–choline ratio of 0.7 or less. The diagnostic accuracy in distinguishing neoplastic from nonneoplastic tissue could be increased from 68% with the use of MRI alone to 97% with the use of MRI in conjunction with 18F-FET PET and MRI spectroscopy. Sensitivity and specificity for tumor detection were 100% and 81%, respectively, for MRI spectroscopy and 80% and 88%, respectively, for 18F-FET PET. Histologic studies did not reveal tumor tissue in any lesions that were negative on 18F-FET PET and MRI spectroscopy. Tumor was diagnosed for 97% of the lesions that were positive with both methods.
PET-Guided Treatment
Because PET activity reflects tumor metabolic activity, using PET to guide treatment seems to be a logical approach. Studies using PET to delineate tumor volumes for radiation therapy have been reported. In a study of 27 patients with glioblastoma, dose escalation using an 18F-FDG PET–defined volume was investigated (84). Patients were treated initially with standard conformal fractionated radiotherapy with volumes defined by MRI. 18F-FDG PET was performed after an initial dose of 45–50.4 Gy. Patients with tumors positive for 18F-FDG PET uptake were treated with an additional 20 Gy to a total dose of 79.4 Gy based on volume as defined by 18F-FDG uptake plus a 0.5-cm margin. 18F-FDG PET defined unique volumes for radiation dose escalation. Multivariate analysis demonstrated that 18F-FDG PET uptake was the only parameter significant for predicting survival and time to tumor progression. However, in a subsequent report of 40 patients, such radiation dose escalation based on 18F-FDG PET volume did not result in improved survival or time to tumor progression, compared with historical controls (85).
PET (or SPECT)/CT or PET (or SPECT)/MRI fusion with 11C-methionine and 123I-a-methyl-tyrosine was studied in 44 patients with recurrent glioblastoma after surgery and postoperative conventional radiotherapy (86). Fused imaging was used to delineate the volume in planning for fractional stereotactic radiotherapy. This volume was compared with the volume determined using CT or MRI alone. A significant survival advantage was found: a 9-mo median survival in patients whose treatment volume was based on fused imaging, versus a 5-mo median survival in patients whose treatment planning was based on CT or MRI alone. 11C-Methionine was also used with CT or MRI to delineate the target volume in patients with meningiomas (87). Information from 11C-methionine was found useful for determining gross tumor volume.
OTHER PET TRACERS AND FUTURE DIRECTIONS
18F-FLT PET
The thymidine analog 3′-deoxy-3′-18F-fluorothymidine (FLT) PET was developed as a noninvasive method to evaluate tumor cell proliferation (88). Uptake of 18F-FLT correlates with thymidine kinase-1 activity, an enzyme expressed during the DNA synthesis phase of the cell cycle (89). Thymidine kinase-1 activity is high in proliferating cells and low in quiescent cells. Phosphorylation of 18F-FLT intracellularly by thymidine kinase-1 results in trapping of the negatively charged 18F-FLT monophosphate (90,91). Although 18F-FLT appears to have limited sensitivity, uptake of 18F-FLT by tumors correlates with Ki-67, a common proliferation index used ex vivo, as demonstrated in several extracranial cancers (92–96). 18F-FLT uptake has also been investigated in brain tumors, and similar correlations have been observed (97–102). Thus, 18F-FLT has the potential to monitor treatment response and to serve as a prognostic marker.
18F-Fluoromisonidazole PET
18F-Fluoromisonidazole is a nitroimidazole derivative that has been developed as a PET agent to image hypoxia (103). Metabolites of 18F-fluoromisonidazole are trapped exclusively in hypoxic cells (104). Hypoxia in tumors is a pathophysiologic consequence of structurally and functionally disturbed angiogenesis along with deterioration of the ability of oxygen to diffuse through tissues. Hypoxia is associated with tumor progression and resistance to radiotherapy (105). Investigation of brain tumors with 18F-fluoromisonidazole PET demonstrated a correlation with perfusion at 0–5 min after injection, whereas late images at 150–170 min after injection were independent of perfusion and BBB disruption (106). 18F-Fluoromisonidazole uptake was found in high-grade gliomas but not in low-grade gliomas, and a significant relationship was found between 18F-fluoromisonidazole uptake and expression of the angiogenesis marker VEGF-R1 (107). Thus 18F-fluoromisonidazole may have a role in directing and monitoring targeted hypoxic therapy.
68Ga-DOTA-TOC
The somatostatin analog 68Ga-DOTA-d-Phe1-Tyr3-octreotide (DOTA-TOC) was investigated in meningiomas, because they show high expression of the somatostatin receptor subtype 2. In contrast to 18F-FDG, 68Ga-DOTA-TOC showed a high meningioma-to-background ratio (108) and added valuable information on the extent of meningiomas beneath osseous structures, especially at the skull base. Further, kinetic studies showed that high uptake of 68Ga-DOTA-TOC in meningiomas can be explained by the high value for vascular fraction and markedly low values for k2 and k4, leading to significantly greater k1/k2 and k3/k4 ratios and receptor binding in meningiomas than in reference tissue (109).
SUMMARY
Although MRI remains the gold standard for the diagnosis and follow-up of malignant brain tumors, 18F-FDG PET has a potential role in providing prognostic information. In previously treated patients, 18F-FDG PET can be helpful in differentiating recurrent tumor from radiation necrosis. It is critical to have the MRI information available while 18F-FDG PET studies are interpreted. Delayed 18F-FDG PET may increase diagnostic accuracy.
Amino acid tracers are promising in that they are more sensitive in imaging brain tumors. Amino acid tracers may also be useful in distinguishing recurrent tumors from radiation necrosis, although further studies are needed.
The use of PET to plan and monitor treatment is an active area of investigation. With the development of targeted therapies, PET biomarkers might be used to select patients who are likely to respond to treatment, as well as to monitor treatment response. Patients who do not respond to a particular treatment can avoid unnecessary toxicity and be switched to a different, potentially more efficacious, regimen earlier on.
Acknowledgments
This study was supported by grant P50 CA086306 from the National Cancer Institute, National Institute of Health, and by contract DE-FC03-87-ER60615 from the U.S Department of Energy.
Footnotes
-
Guest Editor: H. William Strauss, Memorial Sloan-Kettering Cancer Center
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH SEPTEMBER 2008.
-
No potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.
- 94.
- 95.
- 96.↵
- 97.↵
- 98.
- 99.
- 100.
- 101.
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- Received for publication January 31, 2007.
- Accepted for publication April 19, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Improving 18F-FDG PET Quantification Through a Spatial Normalization Method
- Evaluation of patient STress level caused by radiological Investigations in early Postoperative phase After CRANIOtomy (IPAST-CRANIO): protocol of a Swiss prospective cohort study
- A Clinical PET Imaging Tracer ([18F]DASA-23) to Monitor Pyruvate Kinase M2-Induced Glycolytic Reprogramming in Glioblastoma
- Spatial Relationship of Glioma Volume Derived from 18F-FET PET and Volumetric MR Spectroscopy Imaging: A Hybrid PET/MRI Study
- Diagnostic Accuracy of Amino Acid and FDG-PET in Differentiating Brain Metastasis Recurrence from Radionecrosis after Radiotherapy: A Systematic Review and Meta-Analysis
- Re-irradiation for Recurrent Primary Brain Tumors
- Targeting CD146 with a 64Cu-labeled antibody enables in vivo immunoPET imaging of high-grade gliomas
- Lessons From Anti-Vascular Endothelial Growth Factor and Anti-Vascular Endothelial Growth Factor Receptor Trials in Patients With Glioblastoma
- Gain of Glucose-Independent Growth upon Metastasis of Breast Cancer Cells to the Brain
- Pituitary Incidentaloma Found on O-(2-18F-Fluoroethyl)-L-Tyrosine PET
- A Meta-Analysis on the Diagnostic Performance of 18F-FDG and 11C-Methionine PET for Differentiating Brain Tumors
- Utility of Diffusion Tensor Imaging in Evaluation of the Peritumoral Region in Patients with Primary and Metastatic Brain Tumors
- 18F-FDOPA PET for Differentiating Recurrent or Progressive Brain Metastatic Tumors from Late or Delayed Radiation Injury After Radiation Treatment
- In Vitro and In Vivo Characterization of 2-Deoxy-2-18F-Fluoro-D-Mannose as a Tumor-Imaging Agent for PET
- Analysis of the Growth Dynamics of Angiogenesis-Dependent and -Independent Experimental Glioblastomas by Multimodal Small-Animal PET and MRI
- MR Imaging of Neoplastic Central Nervous System Lesions: Review and Recommendations for Current Practice
- Cost-Effectiveness Analysis of Amino Acid PET-Guided Surgery for Supratentorial High-Grade Gliomas
- Impact of 3,4-Dihydroxy-6-18F-Fluoro-L-Phenylalanine PET/CT on Managing Patients with Brain Tumors: The Referring Physician's Perspective
- Discriminant Analysis of 18F-Fluorothymidine Kinetic Parameters to Predict Survival in Patients with Recurrent High-Grade Glioma
- Multimodality Assessment of Brain Tumors and Tumor Recurrence
- Voxel-Based Analysis of Dual-Time-Point 18F-FDG PET Images for Brain Tumor Identification and Delineation
- Hyperpolarized 13C Spectroscopic Imaging Informs on Hypoxia-Inducible Factor-1 and Myc Activity Downstream of Platelet-Derived Growth Factor Receptor
- Kinetics of 3'-Deoxy-3'-18F-Fluorothymidine During Treatment Monitoring of Recurrent High-Grade Glioma
- Updated Response Assessment Criteria for High-Grade Gliomas: Response Assessment in Neuro-Oncology Working Group
- Evaluation of Treatment-Associated Inflammatory Response on Diffusion-Weighted Magnetic Resonance Imaging and 2-[18F]-Fluoro-2-Deoxy-D-Glucose-Positron Emission Tomography Imaging Biomarkers
- 18F-FDG PET/CT for Image-Guided and Intensity-Modulated Radiotherapy
- Diagnostic Accuracy of 11C-Methionine PET for Differentiation of Recurrent Brain Tumors from Radiation Necrosis After Radiotherapy