


Further development and validation of 18F-labeled 3′-deoxy-3′fluorothymidine (FLT) is presented by Buck et al. in this issue of The Journal of Nuclear Medicine (1). Although the use of PET has exploded within the last few years, this has primarily resulted from the application of 18F-FDG in oncology research and clinical practice. The study of Buck et al. further explores the use of 18F-FLT (Fig. 1) and begins a necessary comparison with 18F-FDG. 18F-FDG has found wide applicability in clinical oncology, since it is simple to use and can be distributed commercially. 18F-FDG is useful in the diagnosis, staging, and restaging of a wide variety of tumor types and in the evaluation of their treatment. Although 18F-FDG is the only PET tracer now routinely used in clinical oncology, many other tracers have been produced and tested by investigators. If PET is going to continue to expand, other tracers that complement the information provided by 18F-FDG will need to be found.
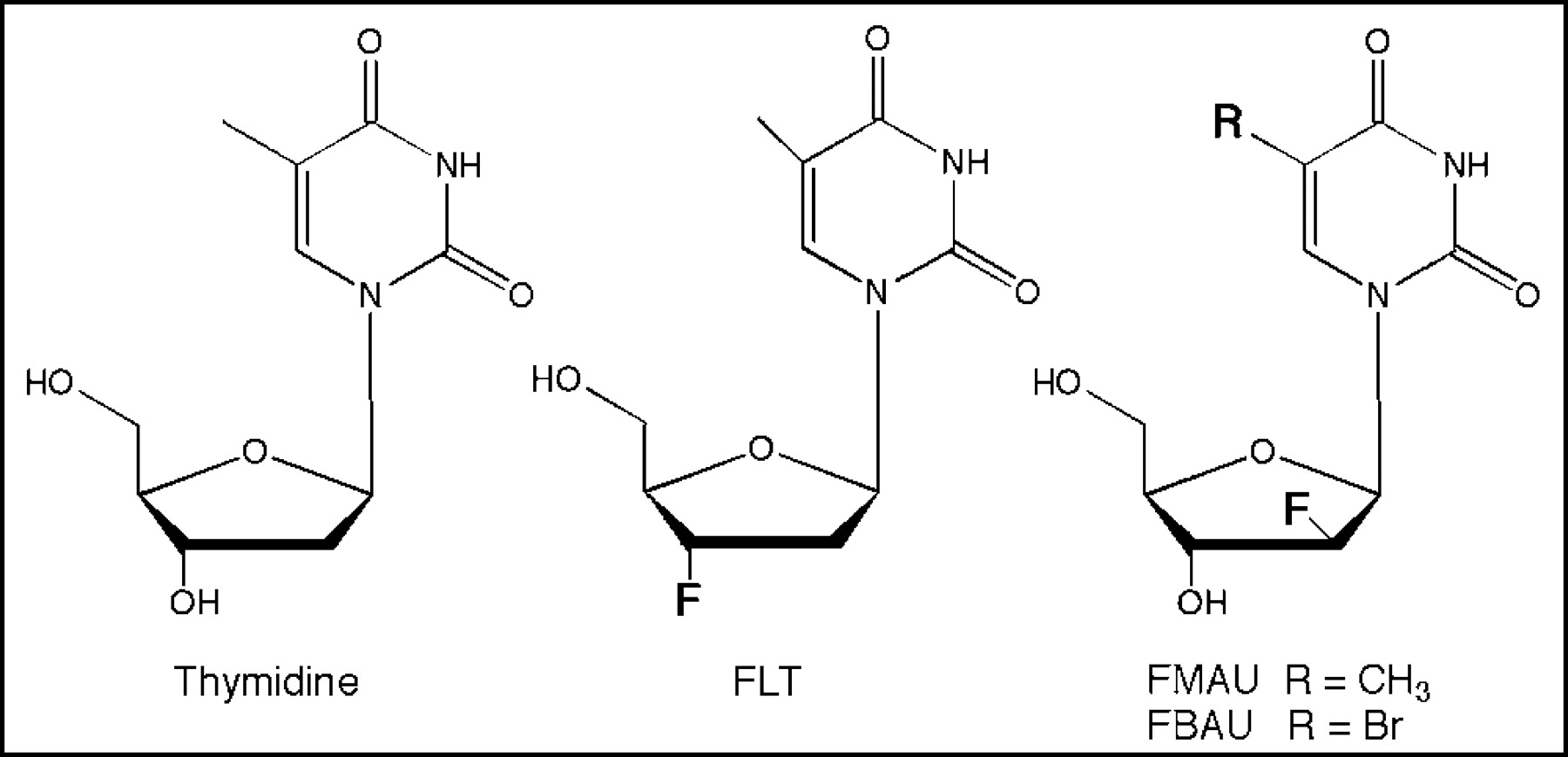
For oncologic use, the measurement of tumor growth and DNA synthesis are attractive targets for imaging. Many investigators have thus been led to test a variety of DNA precursors for tumor imaging. Based on the work originally done in the laboratory using 3H- and 14C-labeled thymidine, synthesis of 11C-thymidine was developed for use with PET (2,3). Imaging with 11C-thymidine is of great interest, since it is the native pyrimidine base used in DNA synthesis. Although such an approach is useful in research and validation studies, the practical limitations of this tracer will preclude it from gaining wide acceptance, and it has been evaluated by only a few research centers. Routine clinical use is not practical, given the short half-life of 11C-thymidine and its rapid biodegradation. The result has been a search for analogs of thymidine that might have superior imaging properties. Fortunately, thymidine analogs have been widely studied by both the pharmaceutical industry and academic scientists as possible therapeutic compounds. The study of these analogs was first undertaken by Dr. Charles Heidelberger, who, seeking thymidine analogs that could interfere with DNA synthesis, produced 5-fluorouracil in 1957. Although 5-fluorouracil and its related nucleoside fluorodeoxyuridine have found use as antineoplastic agents, they also undergo rapid catabolism limiting their use for routine imaging. Similar problems have limited the use of other halogenated thymidine analogs (5-iododeoxyuridine and 5-bromodeoxyuridine) substituted in the 5-position on the pyrimidine ring (4,5). Imaging with such agents, however, has been useful in understanding their pharmacokinetics. Placing a fluorine in the 2′- or 3′-positions of the sugar, however, has lead to the production of analogs that resist catabolism, since they are stable to thymidine phosphorylase, which cleaves the glycosidic bond.
18F-FLT was originally produced after investigators discovered the anti-HIV properties of azidothymidine. In the initial phase I trial in patients with AIDS, 18F-FLT was found to have higher toxicity at clinically useful doses (100 mg/d given for weeks) (6). Such pharmacologic studies of unlabeled 18F-FLT, however, demonstrate that it can safely be given at the tracer doses used by PET. The synthesis of 18F-labeled FLT has been worked out, and it can be made by a couple of different major routes using precursors that are now commercially available. Initial studies of 18F-FLT in animals and subsequent pilot patient studies have demonstrated that the tracer produces images of high contrast of both proliferating tissues and tumors (7,8). As predicted, it resists degradation but does undergo glucuronidation. Because the fluorine is placed in the 3′-position in the sugar, 18F-FLT, like its parent drug azidothymidine, works as a terminator of the growing DNA chain. Little 18F-FLT is actually accumulated in DNA; rather, it is retained intracellularly after phosphorylation by thymidine kinase 1 (9). Very much analogous is the imaging of the glucose use pathway with 18F-FDG after trapping by hexokinase (10). Both compounds therefore reflect accumulation by transport and subsequent activation by the first step in the utilization pathways. 18F-FLT does not reflect the whole of DNA synthesis, just as 18F-FDG does not reflect the whole of glucose use. This limitation may prove to be important in some situations, but so far, it has not been a problem. In cell lines, 18F-FLT retention correlated with 3H-thymidine uptake (r = 0.88, despite the fact that DNA incorporation was 0.2% and more than 90%, respectively, for the 2 tracers (11)). In a few studies, thymidine kinase 1 levels have been found to correlate with cell proliferation. The study of Buck et al. and a recent study of Vesselle et al. clearly add to this literature in demonstrating the 18F-FLT retention in lung cancer correlates with tumor proliferation (1,8). The average standardized uptake value (SUV) for 18F-FLT was found to correlate nicely with Ki-67 immunohistochemistry, with r = 0.92 and 0.84, in the studies of Buck et al. and Vesselle et al., respectively. Dynamic imaging was also performed in the study of Vesselle and improved the correlation slightly. S-phase fraction, measured by flow cytometry, also correlated with 18F-FLT retention. This correlation appears to be better than that between Ki-67 staining and the kinetic measurement of 11C-thymidine retention (r = 0.58), although the latter was done on a mixed group of abdominal tumors (12). Although the data with 18F-FLT look promising, one still must prove that 18F-FLT will track proliferation in at least most situations. This issue is particularly important after therapy, since one could envision situations in which DNA synthesis might be impaired, while thymidine kinase 1 activity persisted for a time.
As the PET community continues to validate the use of 18F-FLT, the determination of how it compares with 18F-FDG will be critical. Are there situations in which 18F-FLT might be more accurate in diagnosis, staging, and the assessment of treatment response? The study of Buck et al. (1) begins to address this issue. Their study demonstrated that 18F-FDG produces higher-contrast images (mean SUV, 4.1) than does 18F-FLT (mean SUV, 1.8). Although 18F-FLT can miss slowly proliferative tumors, its specificity was 100% in their study. On the other hand, 18F-FLT has not always been 100% specific. In our dog studies we found that 18F-FLT is taken up in some normal lymph nodes, and in a patient with sarcoidosis we have seen increased 18F-FLT retention in involved lymph nodes. It is important to realize that the inflammatory reaction can involve proliferation of some cellular elements. At this point, it will be important to determine which clinical situations merit the use of 18F-FLT, rather than 18F-FDG. This determination will require careful study, taking into account the strengths and limitations of each tracer. 18F-FLT has lower background activity in the brain and thorax. On the other hand, 18F-FLT is limited in its ability to image in the bone marrow because of normal cellular proliferation and in the liver because of glucuronidation. The most demanding use of PET in oncology may be the early assessment of treatment response. If one can document that PET reliably demonstrates treatment failure, then a switch to second-line therapy may be indicated. 18F-FDG has been studied for this use in a few trials. Further trials with both 18F-FDG and 18F-FLT are clearly needed before oncologic physicians will be comfortable with this application.
Finally, 18F-FLT is not the only pyrimidine analog that can be used to measure proliferation. FMAU (1-(2′-deoxy-2′-fluoro-β-D-arabinofurano-syl)thy- mine) and FBAU (1-(2′-deoxy-2′-fluoro-β-D-arabinofuranosyl)-5-bromouracil) were initially labeled with 11C and 76Br, respectively, and more recently, both have been labeled with 18F (13–15). These compounds are incorporated into DNA, which offers theoretic advantages (16). Further studies will be needed to determine whether such tracers offer practical improvements over 18F-FLT. Differences in metabolism may be more important in determining which tracer may best be used for different tumors or areas of the body. For example, the high retention of FMAU in the liver may impair imaging in the upper abdomen compared with 18F-FLT, while FMAU is less readily cleared into the bladder than 18F-FLT, leading to improved FMAU imaging of the pelvis.
In summary, the development of PET will require new tracers that track different cellular pathways for use in oncology. 18F-FLT offers a promising approach to imaging cellular growth and has now been used at several centers around the world. The recent studies are an important step in validating and determining the best way to use this tracer.
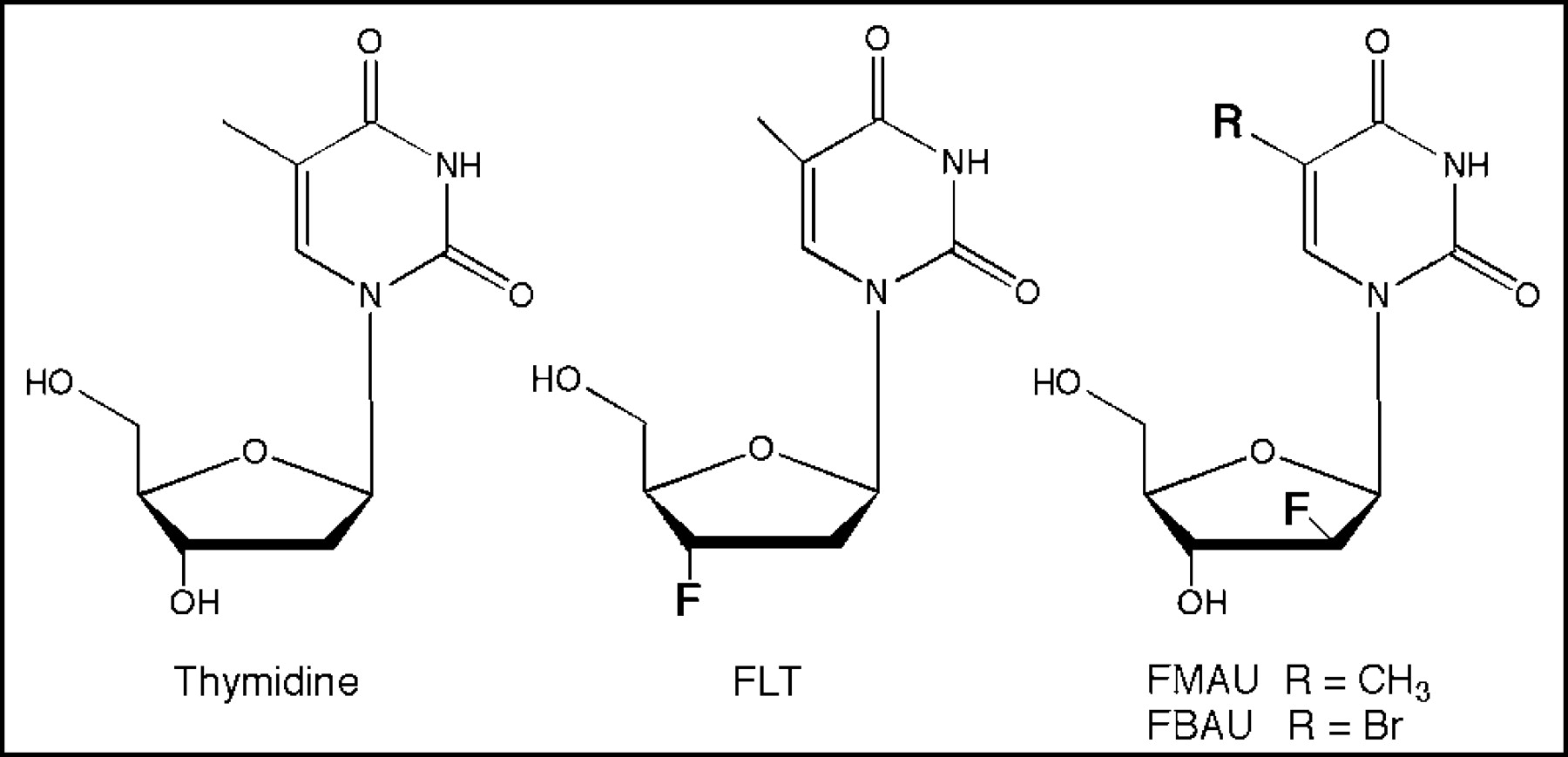
Structures of thymidine, 18F-FLT, and related analogs.
Footnotes
Received May 12, 2003; revision accepted May 20, 2003.
For correspondence or reprints contact: Anthony F. Shields, MD, PhD, Division of Hematology/Oncology, Harper Hospital, 5-Hudson, 3990 John R. St., Detroit MI 48201.
E-mail: shieldsa{at}karmanos.org
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Utilizing novel fluorothymidine PET imaging in a phase I study of veliparib on an intermittent and continuous schedule given in combination with carboplatin in metastatic breast cancer
- [18F]CFA as a clinically translatable probe for PET imaging of deoxycytidine kinase activity
- The Use of Novel PET Tracers to Image Breast Cancer Biologic Processes Such as Proliferation, DNA Damage and Repair, and Angiogenesis
- Assessment of Cellular Proliferation in Tumors by PET Using 18F-ISO-1
- 3'-Deoxy-3'-18F-Fluorothymidine PET Predicts Response to V600EBRAF-Targeted Therapy in Preclinical Models of Colorectal Cancer
- Structure-guided Engineering of Human Thymidine Kinase 2 as a Positron Emission Tomography Reporter Gene for Enhanced Phosphorylation of Non-natural Thymidine Analog Reporter Probe
- Changes in 18F-Fluorodeoxyglucose and 18F-Fluorodeoxythymidine Positron Emission Tomography Imaging in Patients with Non-Small Cell Lung Cancer Treated with Erlotinib
- Different Modes of Transport for 3H-Thymidine, 3H-FLT, and 3H-FMAU in Proliferating and Nonproliferating Human Tumor Cells
- Kinetics of 3'-Deoxy-3'-18F-Fluorothymidine During Treatment Monitoring of Recurrent High-Grade Glioma
- PET Monitoring of Therapy Response in Head and Neck Squamous Cell Carcinoma
- Molecular Imaging In Tumor Treatment Response
- Imaging Surrogates of Tumor Response to Therapy: Anatomic and Functional Biomarkers
- Preferential Tumor Targeting and Selective Tumor Cell Cytotoxicity of 5-[131/125I]Iodo-4'-Thio-2'-Deoxyuridine
- The role of clinical imaging in oncological drug development
- Imaging and Oncologic Drug Development
- Synthesis and In Vivo Evaluation of 2 High-Affinity 76Br-Labeled {sigma}2-Receptor Ligands
- The Progress and Promise of Molecular Imaging Probes in Oncologic Drug Development