


Abstract
R-CHOP (rituximab, cyclophosphamide, doxorubicine, vincristine, and prednisone)–like chemotherapy is the standard therapy in aggressive B-cell lymphoma. 18F-FDG PET has high prognostic implications at treatment completion but is limited as an early predictor. Here, we present the results of a prospective study correlating the initial uptake of the in vivo proliferation marker 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) with the clinical outcome of patients with aggressive non-Hodgkin lymphoma treated with R-CHOP. Methods: Sixty-six eligible patients were evaluated prospectively with 18F-FLT PET before R-CHOP. PET was performed 45 min after injection of 300–370 MBq of 18F-FLT. Mean and maximum standardized uptake values (SUVs) were calculated on a lesion-by-lesion basis. Response was assessed at the end of therapy. International Prognostic Index (IPI) scores and clinical parameters (Ann Arbor stage, lactate dehydrogenase, performance status, extranodal disease) were determined in all patients. Response was assessed according to revised response criteria after the end of therapy. After treatment, patients were followed in intervals from 4 wk to 6 mo (mean follow-up, 23.1 mo [range, 1–63 mo]), and progression-free and overall survival were determined. Results: All lymphoma lesions identified by a reference method (18F-FDG PET/CT or multislice CT of the trunk) showed increased focal tracer uptake (mean 18F-FLT SUV, 7.3 ± 2.5). Response assessment revealed progressive disease in 4, partial response in 3, and complete response (CR) in the remaining 55 patients. The IPI score was predictive for achieving CR (P = 0.034). Importantly, initial mean SUV was also significantly higher in patients who showed progressive disease and partial response than in patients who achieved CR (P = 0.049). In addition, we found a significant correlation between IPI score and initial 18F-FLT uptake. Conclusion: Taken together, high 18F-FLT uptake is a negative predictor of response to R-CHOP treatment in aggressive B-cell non-Hodgkin lymphoma and correlates with the IPI score. Thus, 18F-FLT PET may represent a useful tool for implementing risk-adapted treatment in these patients.
CHOP (cyclophosphamide, doxorubicine, vincristine, and prednisone), or CHOP-like chemotherapy in combination with the chimeric monoclonal anti-CD20 antibody rituximab (R-CHOP), is the standard of care in diffuse large B-cell lymphoma (DLBCL) (1,2). Despite improved overall response rates, progression-free survival, and overall survival in the rituximab era, many patients do not achieve a durable remission after first-line treatment and ultimately die from the disease. Therefore, it remains crucial to identify these patients before or early in the course of treatment. Heretofore, the use of 18F-FDG PET has proven useful for identifying patients who have an excellent prognosis after standard treatment but has failed to accurately identify patients who would benefit from alternative treatment strategies or who should be included into clinical trials because of a dismal outcome with R-CHOP–like therapy (3,4).
Introduction of the thymidine analog 3′-deoxy-3′-18F-fluorothymidine (18F-FLT), a PET tracer derived from the cytostatic drug azidovudine, allows in vivo imaging of proliferating tissues and malignant tumors (5). Recently, published studies demonstrated a significant correlation of tumor cell proliferation and 18F-FLT uptake in lymphoma and solid tumors (6–12). Preliminary studies have also shown that 18F-FLT PET allows noninvasive assessment of tumor grading and early response assessment (6,10). Predictive markers are desirable, guiding optimal treatment in lymphoma; yet the suitability of the initial 18F-FLT uptake has not been studied thus far. Therefore, the aim of this study was to correlate the initial uptake of the proliferation marker 18F-FLT with the clinical outcome of patients with DLBCL treated with standard R-CHOP.
MATERIALS AND METHODS
Patient Selection, Histology, and Treatment
Seventy lymphoma patients 18 y of age or older were referred to our center and included into this prospective trial (38 men, 32 women; mean age ± SD, 59 ± 15 y). Participation in this study was offered to all consecutive patients with aggressive B-cell lymphoma such as DLBCL or follicular lymphoma grade IIIB. During the recruitment period, an additional 15 patients would have been eligible to participate (∼20% of the total study collective); however, because of the severity of clinical symptoms and limited availability of 18F-FLT, induction therapy had to be initiated immediately and pretherapeutic PET could not be performed.
Patients with a history of malignancies or preceding chemo- or radiotherapy were excluded. All biopsies were either performed and analyzed or reviewed at our institution by 2 independent expert hematopathologists. Ki67 immunohistochemistry was performed as previously described (13). Lymphomas were categorized according to the updated classification of the World Health Organization (14). Histopathology revealed aggressive B-cell lymphoma in 66 patients (64 DLBCLs and 2 follicular lymphoma grade IIIB), follicular lymphoma grade I in 2 patients, and anaplastic T-cell non-Hodgkin lymphoma in 2 patients (Table 1). Details of the study were explained by a physician, and written informed consent was obtained from all patients. The International Prognostic Index (IPI) scores (15) and clinical stages for all DLBCL and follicular lymphoma grade IIIB patients are shown in Table 2. A study of a subgroup of 22 patients that investigated the feasibility of repeated 18F-FLT PET early in the course of treatment for identifying responding patients by a significant drop of the 18F-FLT retention in aggressive non-Hodgkin lymphoma was published previously (10).
Histology of All Screened Lymphoma Patients (n = 70)
Characteristics of Eligible Patients (n = 66)
All eligible patients were scheduled to undergo systemic chemotherapy with R-CHOP (n = 66). 18F-FLT PET was performed in all 66 patients within 4 d before treatment. Treating physicians were unaware of the findings of the 18F-FLT PET studies, and these results did not affect treatment decisions. The study protocol was approved by the local ethics committee of Technische Universitaet Muenchen.
PET
18F-FLT was synthesized as previously described (16). Imaging was performed on a whole-body high-resolution PET scanner (ECAT HR+; Siemens/CTI). This device simultaneously acquires 47 contiguous slices with a slice thickness of 3.4 mm. The in-plane image resolution of transaxial images was approximately 8 mm in full width at half maximum, with an axial resolution of approximately 5 mm in full width at half maximum.
Static emission images were acquired 45 min after injection of approximately 300 MBq (range, 270–340 MBq) of 18F-FLT. Emission data were corrected for random coincidences, dead time, and attenuation and reconstructed by filtered backprojection (Hanning filter with cutoff frequency 0.4 cycles per bin). The matrix size was 128 × 128 pixels, with a pixel size of 4.0 × 4.0 mm. The image pixel counts were calibrated to activity concentrations (Bq/mL) and decay corrected using the time of tracer injection as a reference.
PET Data Analysis
All PET scans were evaluated by 2 observers blinded to the clinical data and the results of other imaging studies. Circular 2-dimensional regions of interest with a diameter of 1.5 cm (corresponding to 10 pixels) were placed in the area with the highest tumor activity, as previously published (10). Mean standardized uptake value (SUVmean) and maximum SUV (SUVmax) were calculated from each region of interest using the formula SUV = measured activity concentration (Bq/g) × body weight (g)/injected activity (Bq). For further analyses, mean values from both observers were used. Regions of interest were also placed in the following tissues: liver (right liver lobe, excluding the central part and the liver margins), bone marrow, and gluteal muscle. This algorithm has been demonstrated to be a valuable tool for assessing therapy response (10,17,18). For definition of regions of interest and data analysis, custom software developed at our institution in interactive data language (Research Systems, Inc.) was used.
Reference Methods, Clinical Evaluation, and Follow-up
Diagnostic baseline CT or 18F-FDG PET/CT (n = 37) of the head and neck, thorax, abdomen, and pelvis were performed within 1 wk before chemotherapy, serving as a reference for the presence of nodal or extranodal manifestation sites of aggressive lymphoma. Because 18F-FDG PET/CT for the detection and staging of lymphoma is not reimbursed and currently is not a standard pretreatment assessment, it is not included as a reference in all patients. From January 2007, 18F-FDG PET/CT was routinely performed for staging purposes in 37 of 42 recruited patients.
Patients were reevaluated using CT after 3 courses of R-CHOP and at the end of chemotherapy. Treatment response was classified as complete response (CR), partial response (PR), no change (NC), or progressive disease (PD), according to the standardized response criteria for non-Hodgkin lymphoma (19). In the case of residual lymph node enlargement, 18F-FDG PET was performed and analyzed according to the revised response criteria for malignant lymphoma (20). Treatment response was further evaluated according to standard protocols, including clinical evaluation, ultrasound, chest radiography, CT, and laboratory tests, every 3 mo.
Statistical Analysis
Statistical analyses were performed at the Institute of Medical Statistics and Epidemiology at Technische Universitaet Muenchen using PASW statistics software (version 18.0; SPSS, Inc.). Quantitative values were expressed as mean ± SD, median, and range. Related metric measurements were compared using the Wilcoxon signed-rank test, and the Mann–Whitney U test was used to compare quantitative data between 2 independent samples. To assess the prognostic impact of continuous variables with regard to survival, Martingale residual analysis was performed (21). Smoothing spline equations have been fitted to the residual plots to depict the shape of the functional relationship between the continuous prognostic variable and risk of death.
The Fisher exact test was used for comparison of frequencies, and Spearman correlation coefficients were calculated to quantify bivariate correlations of measurement data. Exact 2-sided 95% confidence intervals (CIs) were reported for estimates of sensitivity and specificity. All statistical tests were conducted 2-sided, and a P value of less than 0.05 was considered to indicate statistical significance.
RESULTS
Clinical Stage and Response to Therapy
Sixty-six patients met the inclusion criteria. According to the initial staging, 18 patients (27%) presented with stage I disease. Stages II, III, and IV were found in 10 (15%), 6 (9%), and 32 (49%) patients, respectively, as indicated by the reference methods (diagnostic CT or 18F-FDG PET/CT). Detailed characteristics of all eligible patients are shown in Table 1. End-of-therapy assessment was available in 62 patients and indicated CR in 55 patients, PR in 3, and PD in 4. Four patients were lost to follow-up.
Correlation of Initial 18F-FLT Uptake with Response
18F-FLT PET was performed successfully in all 66 patients (Fig. 1). All 18F-FLT PET scans were visually rated as positive, resulting in a detection rate of 100%. Mean uptake of 18F-FLT in lymphoma manifestations (mean FLT SUV) was 7.3 (range, 1.0–18.2). Corresponding maximum 18F-FLT uptake ranged from 1.2 to 20.4, resulting in a mean SUVmax of 9.4. To determine the predictive value of pretreatment 18F-FLT uptake, 18F-FLT SUVs were correlated with treatment response. Because of the low number of patients with PR and PD, the initial 18F-FLT uptake was compared for patients in CR (n = 55) and with patients in non-CR (n = 7). The initial mean SUVmean was significantly lower for patients achieving a CR (mean SUVmean, 7.1; range, 1.0–18.2) than for patients not achieving CR (mean SUVmean, 9.5; range, 6.2–13.7, P = 0.049) (Fig. 2). Thus, pretreatment 18F-FLT PET SUVmean may predict CR achievement. The same tendency, but without statistical significance (P = 0.218), was observed for SUVmax, which showed lower values for patients achieving CR (mean SUVmax, 9.4; range, 1.2–20.4) than for patients not achieving CR (mean SUVmax, 11.0; range, 7.0−16.4).

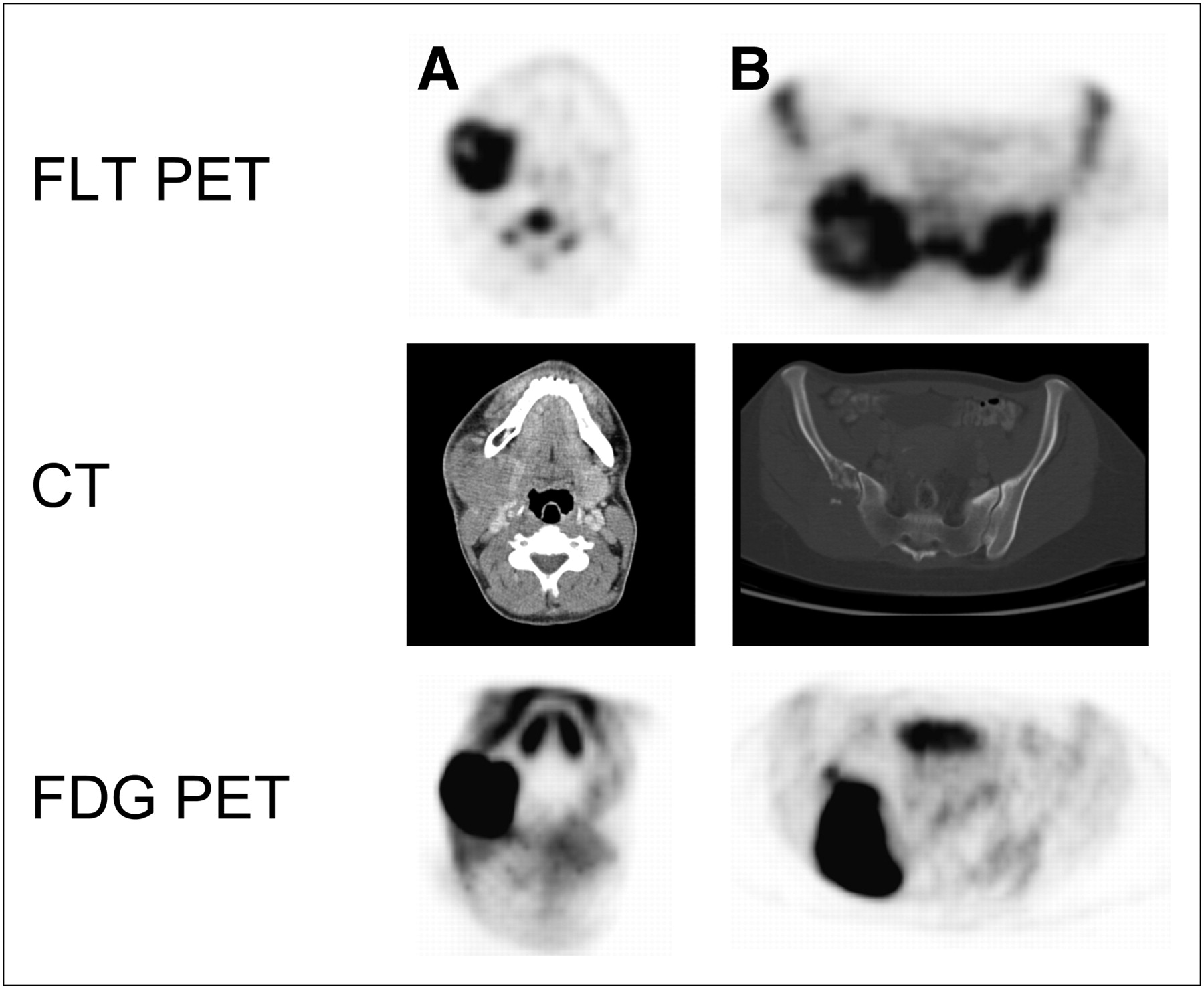
Transaxial views of 18F-FLT PET, helical CT, and 18F-FDG PET for 2 patients with DLBCL. (A) A 41-y-old man with retromandibular lymphoma showing intense 18F-FDG and 18F-FLT uptake in projection of retromandibular lymph node. This stage IA patient revealed PD under therapy. (B) A 40-y-old woman (stage IVA) with histologically proven lymphoma in right iliac bone and sacrum. 18F-FDG PET shows intensely increased uptake in right ilium and sacrum. Corresponding 18F-FLT PET images allow detection of increased asymmetric uptake in right ilium and sacrum despite high physiologic 18F-FLT uptake in proliferating bone marrow. Transaxial views of helical CT display osteodestruction of right ilium. Restaging after end of therapy revealed CR.
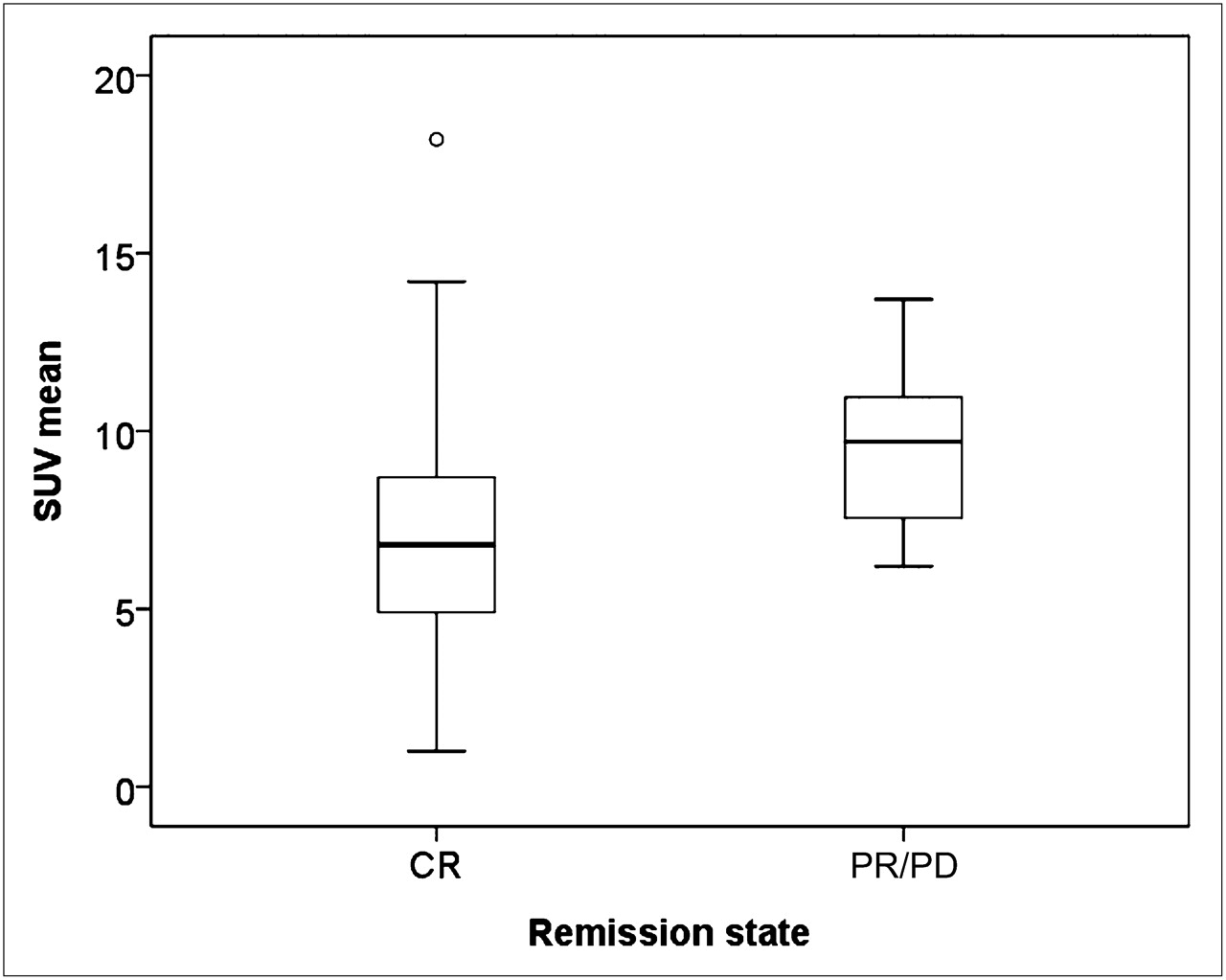
Initial 18F-FLT uptake (SUVmean) in patients achieving CR vs. patients with PR or PD (P = 0.049; difference in median values, 2.5 [95% CI, 0.0–5.2]).
Correlation of Initial 18F-FLT Uptake with IPI Score and Proliferation Index
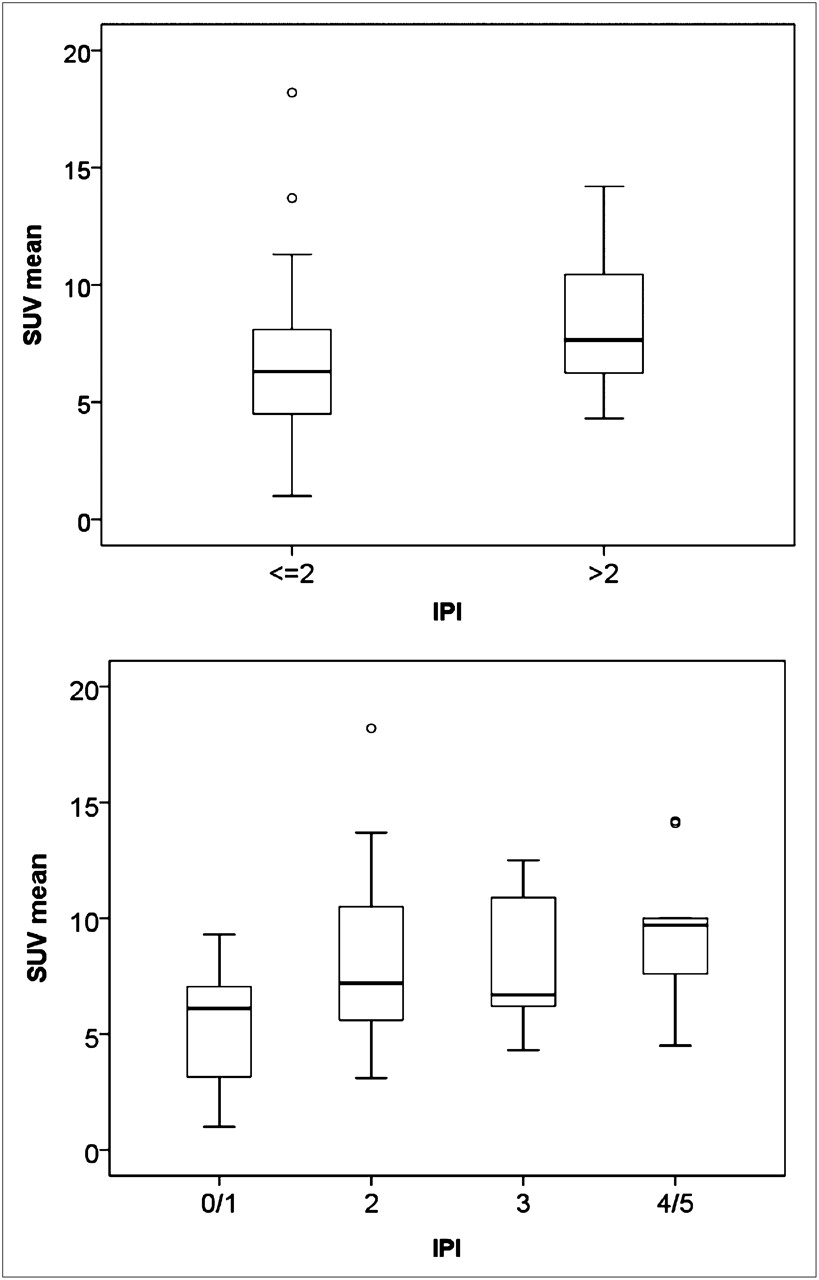
The IPI is the main prognostic tool for survival in patients with DLBCL. This score ranges from 0 to 5 points, comprising 4 risk groups (15). For correlation with the initial 18F-FLT uptake, IPI score subgroups were formed with scores of 2 or less (low and low-intermediate risk) and more than 2 (high-intermediate and high risk). For both SUVmean and SUVmax, 18F-FLT uptake was significantly lower in the subgroup with an IPI score of 2 or less than in the group with an IPI score of more than 2 (SUVmean, 6.6 vs. 8.6; P = 0.012; SUVmax, 8.7 vs. 10.7; P = 0.002). In addition, trend analysis revealed a significant positive relationship between SUVmean levels and IPI risk groups (Spearman ρ, +0.44, P < 0.001) (Fig. 3). Similar results were found for SUVmax (Spearman ρ, +0.41, P < 0.001).

Initial 18F-FLT uptake (SUVmean) in patients with IPI score lower than or equal to 2, compared with patients with IPI score greater than 2 (P = 0.012; difference in medians, 2.1 (95% CI, 0.5–3.7) (top). Trend analysis of initial 18F-FLT uptake (SUVmean) with IPI risk groups (Spearman ρ, +0.44, P < 0.001) (bottom).
Ki67 immunohistochemistry could be performed in 43 of 66 patients. Ki67-positive lymphoma cells ranged between 35% and 95% (mean, 67% ± 17%; median, 70%). Correlation analysis between initial 18F-FLT uptake and Ki67 proliferation index showed a tendency to higher Ki67 proliferation rates in patients with higher initial 18F-FLT uptake. However, no statistical significance was found (Spearman ρ, 0.21; P = 0.18). Also, Ki67 immunoreactivity in lymphoma specimens of patients achieving CR and patients with non-CR was not significantly different (P = 0.61; median for CR: 70%, range, 35%–95%, vs. median for non-CR: 73%, range, 60%–85%).
Prognostic or Predictive Value of Initial 18F-FLT Uptake with Regard to Survival
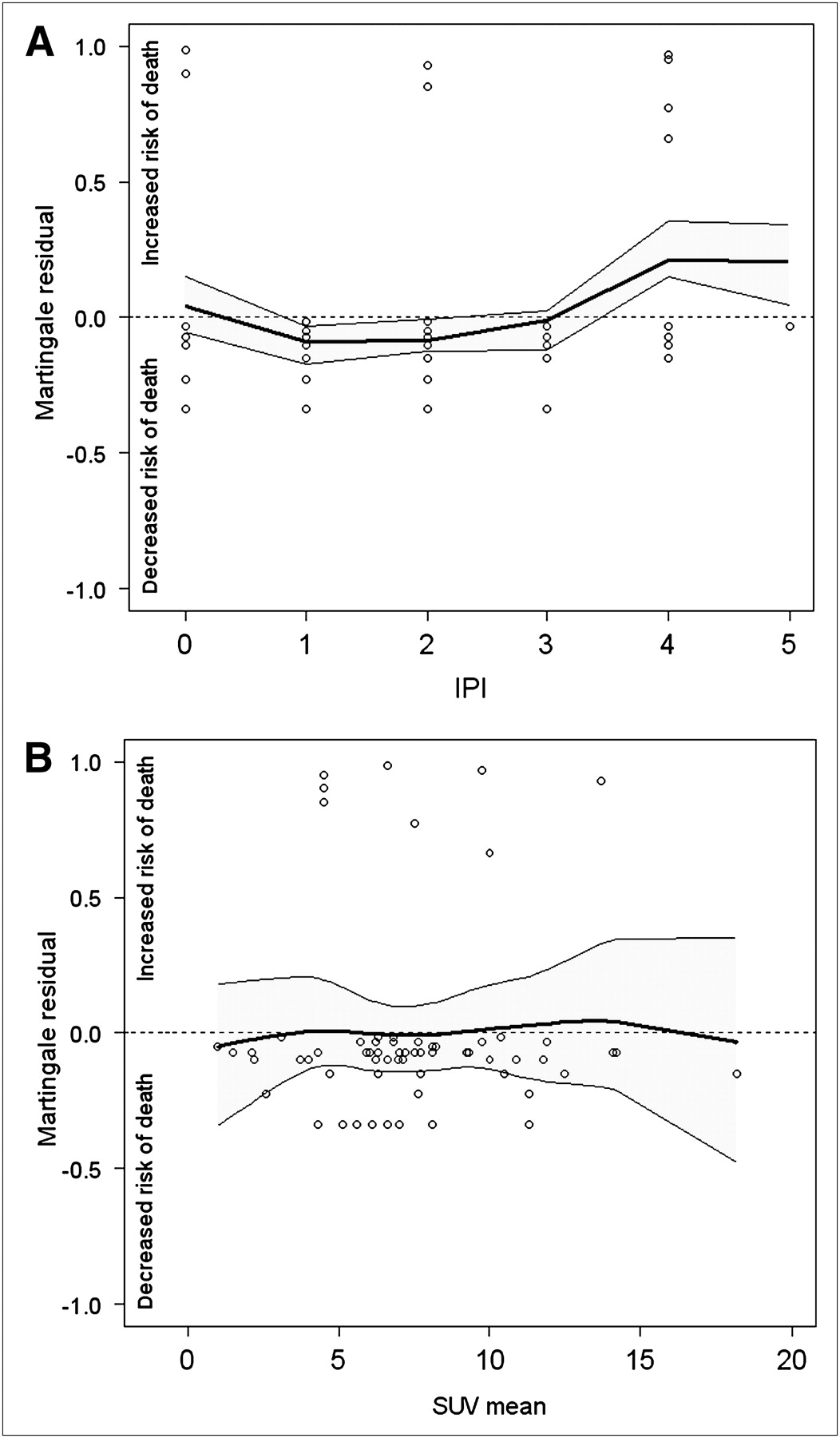
Follow-up was available in 62 patients. The median follow-up was 18.1 mo (mean, 22.6 mo; range, 1.1–63.1 mo). During this interval, 4 patients experienced recurrence and 8 patients died. Lymphoma-associated death was found in 3 patients. Martingale residual analysis was performed for all 8 death events but revealed no relevant correlation between survival and initial 18F-FLT uptake (Fig. 4B). The corresponding estimated hazard ratio per 1-point increment of 18F-FLT SUVmean was 1.03 (95% CI, 0.83–1.27, P = 0.80). However, initial SUVmean was significantly higher in the 3 patients with lymphoma-associated deaths (mean, 11.1; range, 9.7–13.7) than in those with non–lymphoma-associated deaths (mean, 6.6; range, 4.5–7.5; P = 0.036) or in all included patients (mean, 7.3; P = 0.034). Thus, high initial 18F-FLT uptake might be used as a surrogate marker for prediction of unfavorable outcome under R-CHOP chemotherapy.

(A) Martingale residual analysis of IPI score and risk of death. Solid lines depict smoothing spline function, with simultaneous 95% confidence bands. Three patients with lymphoma-associated death had IPI scores of 2, 4, and 4. Corresponding estimated hazard ratio per 1-point increment of IPI score was 1.43 (95% CI, 0.81–2.52, P = 0.22). (B) Martingale residual plots of overall survival and initial 18F-FLT uptake. Solid lines depict smoothing spline function, with simultaneous 95% confidence bands. Corresponding estimated hazard ratio per 1-point increment of 18F-FLT SUVmean was 1.03 (95% CI, 0.83–1.27, P = 0.80). Initial 18F-FLT uptake was significantly higher in 3 patients with lymphoma-associated death (mean, 11.1; range, 9.7–13.7) than in those with non–lymphoma-associated deaths (mean, 6.6; range, 4.5–7.5; P = 0.036) and in whole study cohort (mean, 7.3; P = 0.034).
Association of IPI Score, Response, and Survival
Because the IPI score is the standard prognostic tool for survival in DLBCL patients, we tested the predictive value of the IPI score regarding response to therapy in our patient population. Similar to initial 18F-FLT uptake, the IPI score revealed a statistically significant difference between patients in CR and non-CR. Patients achieving CR had a significantly lower IPI score (median, 2; range, 0–5) than patients rated as PD or PR (median, 4; range, 0–4) (P = 0.039). In contrast, Martingale residual analysis revealed no relevant association between IPI score and risk of death (Fig. 4A). The corresponding estimated hazard ratio per 1-point increment of IPI score was 1.43 (95% CI, 0.81–2.52, P = 0.22). Taken together, these data demonstrate that both the well-established IPI score and the initial 18F-FLT uptake were able to predict treatment outcome in our study.
DISCUSSION
18F-FLT has been demonstrated to reflect proliferation-dependent retention of nucleosides in malignant lymphoma, which can be assessed noninvasively by PET (13). However, the predictive and prognostic potential of pretherapeutic imaging using 18F-FLT remains to be determined. To the best of our knowledge, this is the first study investigating the predictive value of 18F-FLT PET regarding response to treatment and survival in aggressive B-cell non-Hodgkin lymphoma. Compared with patients not achieving a CR (the PR/PD group), patients who achieved CR with R-CHOP treatment, as assessed by well-established response criteria, had a significantly lower SUVmean 18F-FLT uptake before treatment. This might indicate that a higher proliferation rate, as measured by 18F-FLT PET, is a negative predictor regarding CR. Regarding SUVmax, 18F-FLT uptake was also higher in the PR/PD group than in the CR group; however, the difference was not statistically significant, presumably because of the low number of treatment failures in our study cohort. Quite notably, among the deceased patients, the 3 patients who died from progressive lymphoma showed the highest 18F-FLT uptake values (SUVmean, 9.7, 10.0, and 13.7). This result thus indicates that 18F-FLT PET may identify a poor prognostic subgroup. It is tempting to speculate that 18F-FLT uptake correlates with a poor-outcome subgroup that has been identified in molecular studies using gene expression technologies (22,23). Overall, the response rate in our patient population was rather high (CR in 55/66 patients)—partly explained by the fact that the 18F-FLT PET scanning prolonged the diagnostic work-up, resulting in a delay of treatment initiation. Accordingly, patients who were considered to require immediate therapy by the treating clinician and patients with reduced performance status may be underrepresented in this study.
Our data clearly show that the initial 18F-FLT uptake significantly correlates with the IPI score (P = 0.049) and response to treatment. IPI score, representing the best prognostic indicator for survival, was able to predict achievement of CR versus non-CR in our study (15). This observation further underlines the potential of in vivo proliferation imaging and provides evidence for 18F-FLT uptake as a predictive tool comparable to the well-established IPI score. However, prediction of survival is clinically more relevant than prediction of response to treatment. Because of the low number of events, we could not show a predictive relevance of the initial 18F-FLT uptake for survival in this study. However, these findings are encouraging and warrant analysis in a larger cohort. In a small study with 20 head and neck cancer patients, it was also shown that initial 18F-FLT and 18F-FDG uptake correlates with survival (24). Besides these limited data, correlation of initial 18F-FLT uptake and survival has not yet been studied in other tumor entities.
Nearly all patients presented with intense uptake of the radionucleoside 18F-FLT, and all of the lymphoma lesions identified by conventional imaging modalities (spiral CT, 18F-FDG PET/CT) were visible by 18F-FLT PET. The high sensitivity for detection of aggressive lymphoma is in agreement with several previously published trials (6,10,13,25,26). Even osseous lesions were detectable because of focal 18F-FLT uptake greater than the surrounding bone marrow. However, it has been reported previously that the sensitivity of 18F-FLT PET in tissues with high physiologic 18F-FLT uptake (e.g., bone marrow or liver) is lower than that of 18F-FDG PET or conventional imaging procedures (6). Our study is by far the largest clinical trial using 18F-FLT PET for the characterization of aggressive lymphoma (n = 66). A major strength of our study is a high number of patients assessed who demonstrated that proliferation imaging is a sensitive and reliable procedure potentially suitable also for initial staging of aggressive B-cell lymphoma (6,25,26).
Before translating these results into clinical routine practice, several important limitations have to be considered. First, in this study only 8 patients died during follow-up, and only 3 deaths were lymphoma-associated. This favorable prognosis of patients observed in our series requires confirmation of our data and our conclusions in a larger cohort. Second, this study investigated the prognostic relevance of only the initial 18F-FLT uptake without evaluating changes in 18F-FLT uptake during the course of the treatment, which might represent a better predictive tool. A clear advantage for 18F-FLT, compared with the standard tracer 18F-FDG, is its higher specificity for malignant tumors (7). 18F-FDG PET allows the imaging of increased consumption of glucose, which is a characteristic of most tumor cells and is partially related to overexpression of the glucose transporter type 1 and increased hexokinase activity (27). However, the specificity is reduced because of physiologic glucose uptake in brown fat tissue, colonic and gynecologic activity, infections and inflammations, and rebound thymic hyperplasia. Nonspecific 18F-FDG accumulation in inflammatory lesions is of major importance for therapy monitoring. Overestimation of 18F-FDG uptake might occur in tumors with an inflammatory component or, more often, might occur because of chemotherapy- or radiation-mediated inflammatory processes. This unspecific uptake may persist for weeks or months, potentially influencing the assessment of changes in glucose metabolism during therapy response assessment (28). Moskowitz et al. demonstrated that most 18F-FDG–positive lesions detected by interim PET were negative as determined by repeated biopsy (4). These limitations of 18F-FDG PET strongly indicate potential applications for 18F-FLT, which seems to be more specific than 18F-FDG. Although false-positive findings have been reported also for 18F-FLT PET caused by proliferating lymphocytes in reactive lymph nodes, 18F-FLT might be suitable or even superior to 18F-FDG for monitoring response to treatment, particularly in the setting of interim PET analyses (29).
CONCLUSION
Our data demonstrate that 18F-FLT PET is a promising and sensitive tool for the detection of lymphoma lesions and for predicting response to treatment in aggressive B-cell lymphoma. In addition, we found a significant correlation of 18F-FLT uptake and the IPI score, which still represents the main prognostic tool in DLBCL. Our current data clearly justify further evaluation in larger cohorts to confirm initial or interim 18F-FLT PET as a predictive tool in the management of DLBCL patients.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We appreciate the excellent contributions made by our colleagues Stephan Nekolla, Sandra van Marwick, Nikolas von Bubnoff, Katharina Götze, and Folker Schneller and the great support by our technical staff members Brigitte Dzewas and Coletta Kruschke. This work was supported by the collaborative research center SFB 824, project C3, and the German Research Foundation (DFG) “Imaging for Selection, Monitoring and Individualization of Cancer Therapies.”
Footnotes
↵* Contributed equally to this work.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication October 24, 2010.
- Accepted for publication February 8, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FLT PET/CT as a Prognostic Imaging Biomarker of Disease-Specific Survival in Patients with Primary Soft-Tissue Sarcoma
- Prospective Study of 3'-Deoxy-3'-18F-Fluorothymidine PET for Early Interim Response Assessment in Advanced-Stage B-Cell Lymphoma
- Early Determination of Prognosis by Interim 3'-Deoxy-3'-18F-Fluorothymidine PET in Patients with Non-Hodgkin Lymphoma
- [18F]-FLT Positron Emission Tomography Can Be Used to Image the Response of Sensitive Tumors to PI3-Kinase Inhibition with the Novel Agent GDC-0941
- How Many PET Tracers Do We Need?
- A Pilot Study to Evaluate 3'-Deoxy-3'-18F-Fluorothymidine PET for Initial and Early Response Imaging in Mantle Cell Lymphoma