


Abstract
Mantle cell lymphoma (MCL) is a B-cell non-Hodgkin lymphoma. Proliferation activity is considered an important prognostic marker. Immunohistochemical analysis from core biopsy or lymph node may not represent the proliferation rate. We investigated the in vivo proliferation marker 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) to characterize MCL. Methods: Eight untreated MCL patients were recruited prospectively. 18F-FLT PET/CT was performed 45 min after injection of 18F-FLT. 18F-FDG PET/CT served as reference. Mean 18F-FLT standardized uptake values were assessed per lesion and compared with respective 18F-FDG uptake. Correlation of mean 18F-FLT and 18F-FDG uptake in the hottest lesion to Ki67 immunostaining was performed. Five patients underwent repetitive early 18F-FLT PET. Results: All lymphoma lesions identified by 18F-FDG PET/CT showed increased 18F-FLT uptake. Semiquantitative analysis revealed a high mean 18F-FLT standardized uptake value of 9.9 (range, 5.5–15.9). Mean 18F-FLT uptake and Ki67 expressions showed a strong positive correlation. Conclusion: PET using 18F-FLT as a biomarker for proliferative activity showed a high sensitivity for MCL. 18F-FLT uptake shows a correlation with proliferation. Our results warrant further analysis of 18F-FLT PET in MCL.
Mantle cell lymphoma (MCL) is a subtype of B-cell non-Hodgkin lymphoma characterized by the translocation t(11;14)(q13;q32) resulting in nuclear overexpression of cyclin D1 in most patients. In addition to the constitutive expression of the cell cycle regulatory protein cyclin D1, various aberrations in apoptotic and DNA damage response pathways have been reported. At initial diagnosis, most patients present with an advanced disease stage (Ann Arbor stage III or IV). Despite major advances in the clinical management of MCL, including treatment with monoclonal anti-CD20–specific antibodies (rituximab), high-dose cytarabin, and consolidation myeloablative therapy followed by hematopoietic stem cell support, MCL is still considered a noncurable disease (1–4).
18F-FDG PET is a noninvasive imaging technique that is suggested for posttreatment imaging and has been proven useful for routine staging or interim assessment of diffuse large B-cell lymphoma and Hodgkin lymphoma (5–8). In MCL, the sensitivity of 18F-FDG PET is close to 100%, but 18F-FDG PET has not yet proven to be beneficial for either response assessment or posttreatment surveillance (9–11). Introduction of the thymidine analog 3′-deoxy-3′-18F-fluorothymidine (18F-FLT), a PET tracer derived from the cytostatic drug azidovudine, allows in vivo imaging of proliferating tissues and malignant tumors (12). Here, we present a pilot study that evaluates initial and early interim 18F-FLT PET and provide evidence for the suitability of 18F-FLT as an imaging biomarker for noninvasive characterization of MCL.
MATERIALS AND METHODS
Patients and Clinical Data
This study was approved by the ethics committee of the Medical Faculty of Technische Universität München. Eight patients met the inclusion criteria (first diagnosis of MCL, indication for systemic treatment, age ≥ 18 y, and full contractual capability) and were included after signing the informed consent form. According to the initial staging, 1 patient presented with stage II disease and 7 patients with stage IV disease, as indicated by the reference methods (clinical evaluation, bone marrow biopsy, and CT scan). The MCL international prognostic index (MIPI) score was calculated as described earlier (13). Patient characteristics are shown in Table 1.
Patient Characteristics (n = 8)
Histology and Immunohistochemistry
Lymphomas were classified according to the updated World Health Organization classification system (14). Slides of 5- to 6-μm sections cut from formalin-fixed paraffin-embedded tissues were deparaffinized and stained with hematoxylin and eosin (Dako), dehydrated, and then covered with a coverslip. For immunohistochemistry, 2-μm sections were deparaffinized. Antigen retrieval was performed by pressure cooking in citrate buffer (pH 6) for 7 min. All 8 patients were cyclin D1–positive as assessed by immunohistochemistry (clone sp4; DCS Innovative Diagnostik-Systeme). Proliferation was analyzed using the proliferation marker Ki67 (monoclonal antibody clone MIB-1; Dako). Two independent hematopathologists analyzed high-power fields (×40) of each primary MCL.
Imaging and Data Analysis
Baseline 18F-FLT PET and 18F-FDG PET/CT examinations were performed within 1 wk before therapy, together with routine staging modalities (clinical examination, CT, bone marrow biopsy). 18F-FLT PET was repeated in 5 patients at an average of 6.2 d (median, 6.0; range, 5.0–7.0 d) after the start of the first course of immunochemotherapy. 18F-FLT was synthesized as previously described (15). PET was performed 45 min after injection of approximately 300 MBq of 18F-FLT (range, 270–340 MBq) as previously described (16). All PET scans were evaluated by 2 observers unaware of the clinical data and the results of other imaging studies. Circular regions of interest (diameter, 1.5 cm) were placed in the area with the highest tumor activity, as previously published (17). Mean standardized uptake values (SUVs) were calculated from each region of interest using the formula SUV = measured activity concentration (Bq/g) × body weight (g)/injected activity (Bq).
Statistical Analysis
Statistical analyses were performed using PASW Statistics software (version 18.0; SPSS, Inc.). Because of the small sample size and the rather explorative nature of the study, no formal tests were conducted. The arithmetic mean, median, and range were reported for description of quantitative data. Correlation coefficients according to Pearson (r) or, if appropriate, according to Spearman (ρ), were calculated with 95% confidence intervals.
RESULTS
18F-FLT Uptake Values in MCL and Correlation with 18F-FDG Uptake Parameters
In 7 of 8 patients 18F-FLT PET (Fig. 1, representative images) and 18F-FDG PET scans showed increased uptake, whereas, after removal of a single lymph node, 1 patient showed no residual lymphoma tissue on PET. Initial mean uptake of 18F-FLT in lymphoma manifestations (mean 18F-FLT SUVmean) was 9.9 (median, 8.2; range, 5.5–15.9). Corresponding maximum 18F-FLT uptake values ranged from 6.2 to 19.6, resulting in a mean of maximum SUV (SUVmax) of 11.6 (median, 9.5). Corresponding uptake values for the baseline 18F-FDG PET scan were 7.4 for mean SUVmean (median, 7.6; range, 3.0–10.3) and 8.8 for mean SUVmax (median, 9.6; range, 4.0–11.7). Mean SUVmean and mean SUVmax were higher for 18F-FLT than for 18F-FDG, reaching statistical significance only for SUVmean (P = 0.043 and 0.051, respectively). Correlation of 18F-FLT and 18F-FDG uptake values was revealed to be strongly positive (Spearman ρ, +0.76; 95% confidence interval [CI], +0.01 to +0.96; Fig. 2A). Up to 5 lesions in every patient were measured, revealing a heterogeneous uptake pattern (Table 1). However, intrapatient variability of uptake values appeared to be less than the interpatient variability.
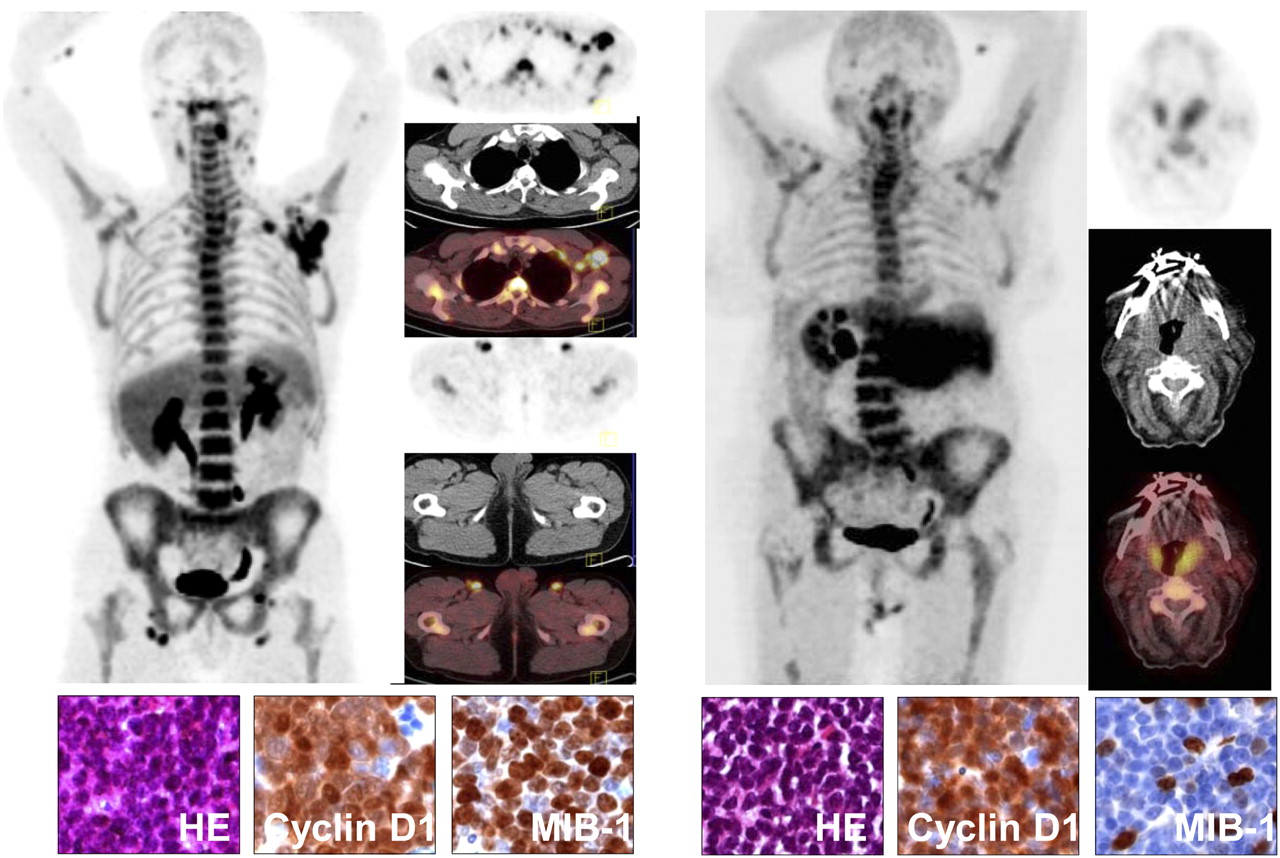
(Left) 18F-FLT PET images of patient 7 with blastoid MCL. Representative hematoxylin and eosin staining, cyclin D1, and Ki67 (MIB-1) immunohistochemistry (80% positivity). (Right) 18F-FLT PET images of patient 4 with classic MCL. Representative hematoxylin and eosin staining, cyclin D1, and Ki67 (MIB-1) immunohistochemistry (10% positivity). HE = hematoxylin and eosin.
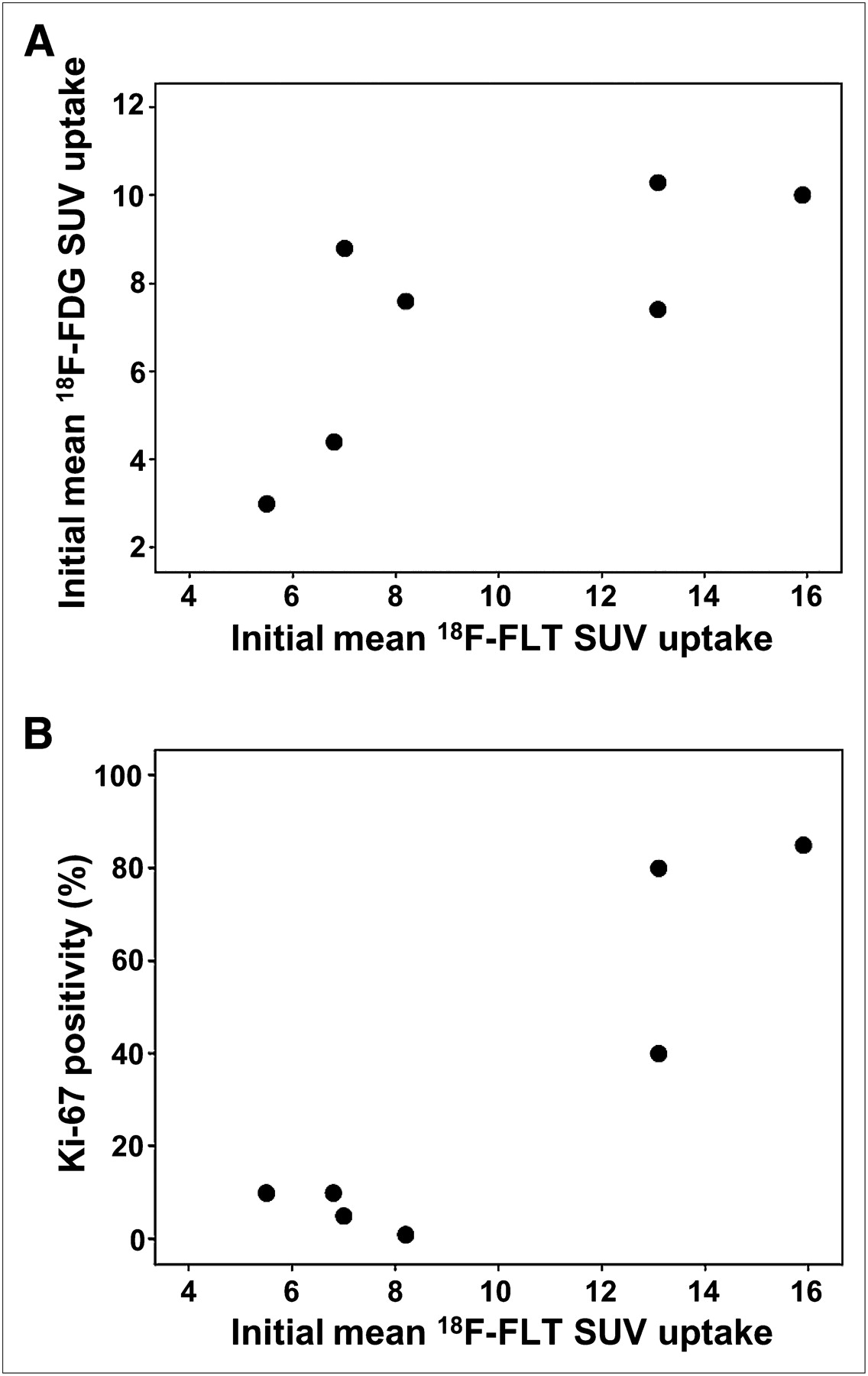
Correlation between initial mean 18F-FLT SUVmean and initial mean 18F-FDG-SUVmean uptake (A) and initial mean 18F-FLT SUVmean uptake and Ki67 positivity (%) (B).
Correlation of 18F-FLT Uptake Parameters to Ki67 Expression and MIPI Score
Ki67 immunohistochemistry was performed in all PET-positive patients (n = 7). Ki67-positive lymphoma cells ranged between 1% and 85% (mean, 33%; median, 10%). Correlation analysis between initial 18F-FLT uptake and Ki67 proliferation index showed a strong correlation, namely higher Ki67 proliferation in patients with higher initial 18F-FLT uptake values (Pearson r, +0.91; 95% CI, +0.50 to +0.99). The MIPI ranged from 5.4 to 7.1 (mean, 6.4; median, 6.3), and the MIPI including Ki67 (MIPI-Ki67) ranged from 6.2 to 8.0 (mean, 7.1; median, 7.2). Mean initial 18F-FLT uptake values and MIPI-Ki67 showed a strong positive correlation (Pearson r, +0.84; 95% CI, +0.25 to +0.98; Fig. 2B). There was no considerable correlation between 18F-FLT uptake and MIPI (Spearman ρ, +0.14; 95% CI, −0.69 to +0.81).
Early Response Assessment by 18F-FLT Uptake Parameters
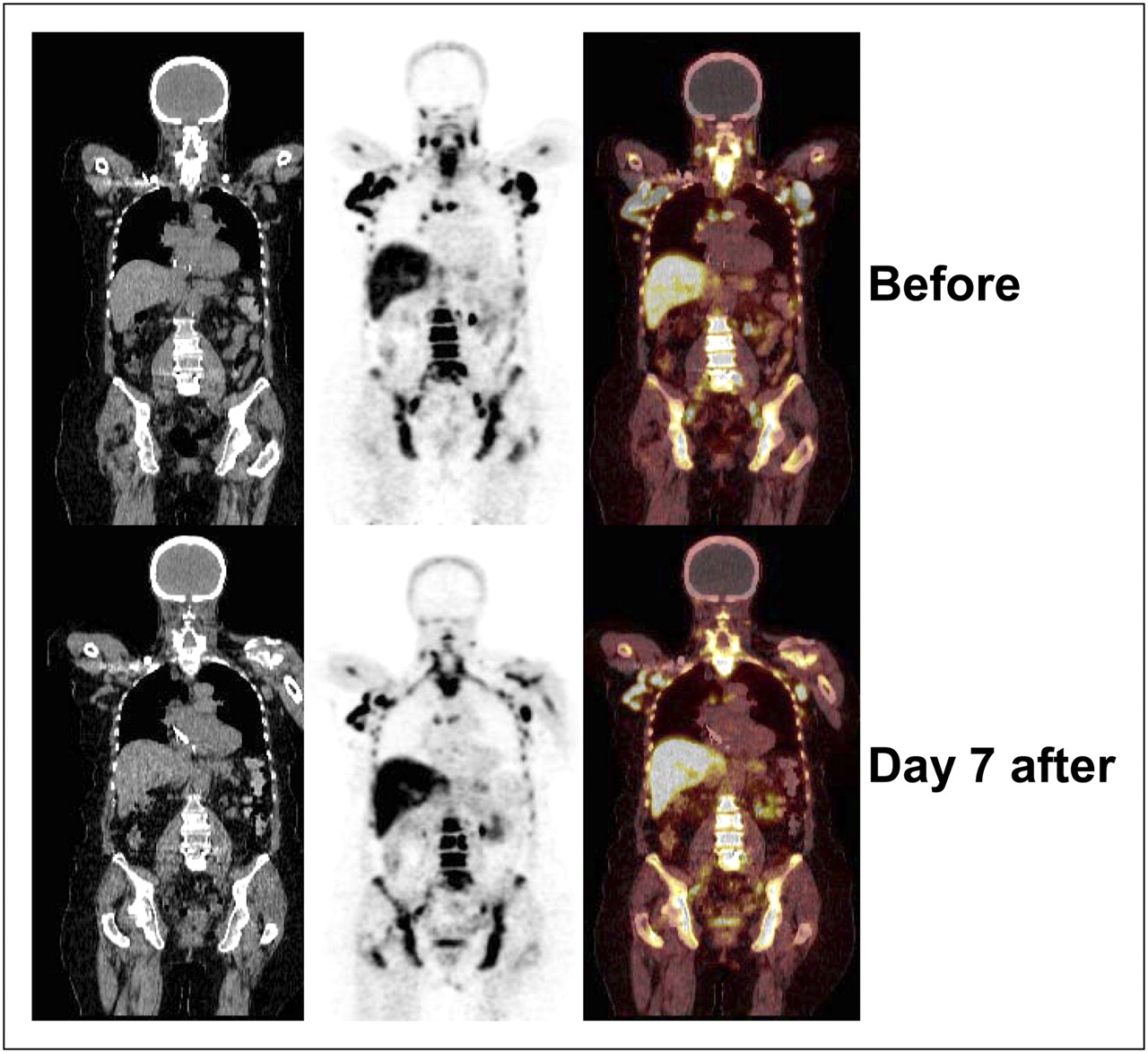
Five patients participated in the early response assessment phase of this study. One week after the start of treatment, 18F-FLT uptake showed a mean SUVmean decrease of 45% (range, −15% to 96%). The corresponding mean SUVmax decrease was 44% (range, −15% to 94%). We observed a heterogeneous change in 18F-FLT uptake, with an SUV decrease greater than 80% in 2 patients (SUVmean, 84% and 96%; SUVmax, 84% and 94%), whereas in 2 patients 18F-FLT uptake decreased by only 20% and 38% for SUVmean (25% and 35% for SUVmax, respectively, Fig. 3), and in 1 patient the uptake even increased (15% each for SUVmean and SUVmax, respectively).

Early response assessment by 18F-FLT PET. Shown are images of patient 5 before initiation of immunochemotherapy and at day 7 after initiation of chemotherapy. SUVmean and SUVmax decreased by 38% and 35%, respectively.
Clinical Response Assessment
One patient received rituximab monotherapy. All other patients received combined immunochemotherapy (Table 1). All patients responded to antibody therapy or immunochemotherapy (with 6 patients achieving complete response as assessed by conventional CT staging and 2 patients with a partial response, 1 after cycle 6 and 1 after cycle 3, with therapy ongoing). Because of the low number or patients, no correlation between 18F-FLT or MIPI and response was assessed.
DISCUSSION
All evaluable patients presented with intense uptake of the radionucleoside 18F-FLT, and all of the MCL lesions identified by conventional imaging modalities (spiral CT, 18F-FDG PET/CT) were visible by 18F-FLT PET. The good visibility of aggressive lymphoma by 18F-FLT PET is in agreement with several previously published trials in other subentities (17,18). Several studies have analyzed the 18F-FDG PET avidity of MCL (9,10). These reports indicate that the sensitivity in detecting bone marrow involvement is rather low (9), and our results indicate that this is even more the case for 18F-FLT PET.
A combined clinical and biologic score (MIPI) has recently been established that allows a reliable estimation of the individual clinical course. In addition, cell proliferation assessment (Ki67) is a strong prognostic marker (13). These results confirmed a previous transcriptome analysis that identified a predictive 20-gene proliferation signature (19). Even in this small pilot study, we were able to detect a strong positive correlation between proliferation, as assessed by Ki67 staining or MIPI-Ki67, and 18F-FLT uptake. This correlation indicates that 18F-FLT PET is a proper sensitive tool to estimate the proliferative activity of MCL, which has been shown earlier for 18F-FDG PET when comparing blastoid versus classic MCL (9).
Four of 5 patients who entered the early response assessment part of the study showed a substantial decrease in 18F-FLT uptake. Because of the low number of patients and the short follow-up period, descriptive results have been presented regarding individual changes of the 18F-FLT SUV early after start of therapy. Because all patients in this study responded to treatment, we cannot at this point come to a conclusion on the predictive value of 18F-FLT PET for response assessment. Negativity for minimal residual disease (MRD) assessed by polymerase chain reaction after 3–4 cycles of immunochemotherapy has recently been shown to be a highly predictive marker for progression-free survival (20). A positive correlation between early 18F-FLT PET responses and MRD negativity at midterm may allow the establishment of the clinical value of this imaging technique in MCL and may in the long term lead to therapeutic changes based on imaging results.
CONCLUSION
Our data demonstrate that 18F-FLT PET is a promising and sensitive tool for the detection of MCL lesions. Even in our limited-patient-number study, we detected a strong positive correlation (lower 95% confidence limit, modest positive correlation) of 18F-FLT uptake and proliferation assessed by Ki67 staining. Our data justify further evaluation in larger cohorts, especially with regard to response and the predictive MRD levels to integrate initial or interim 18F-FLT PET as a predictive tool in the clinical management of MCL patients.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Brigitte Dzewas and Coletta Kruschke for expert technical support. This work was supported by the Collaborative Research Centre SFB 824 Imaging for Selection, Monitoring and Individualization of Cancer Therapies (Deutsche Forschungsgemeinschaft, project C3) and the Transregional Collaborative Research Centre TRR 54 Growth and Survival, Plasticity and Cellular Interactivity in Lymphoid Malignancies (Deutsche Forschungsgemeinschaft, project C5). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Nov. 7, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication June 20, 2011.
- Accepted for publication August 30, 2011.





{kind=link}
{kind=link}
{kind=link}