


Abstract
The aim of this prospective phase II study was to evaluate the tumor response of neuroendocrine tumors to high-dose targeted irradiation with 7.4 GBq/m2 of the radiolabeled somatostatin analog 90Y-1,4,7,10-tetra-azacyclododecan-4,7,10-tricarboxy-methyl-1-yl-acetyl-d-Phe-Tyr3-octreotide (DOTATOC). In addition, we investigated the clinical benefit of 90Y-DOTATOC regarding the malignant carcinoid syndrome and tumor-associated pain. Methods: Thirty-nine patients (mean age, 55 y) with progressive neuroendocrine gastroenteropancreatic and bronchial tumors were included. The treatment consisted of 4 equal intravenous injections of a total of 7.4 GBq/m2 90Y-DOTATOC, administered at intervals of 6 wk. After each treatment cycle, a standardized clinical benefit assessment using the National Cancer Institute grading criteria (NCI-CTC) was performed. Results: The objective response rate according to World Health Organization (WHO) criteria was 23%. For endocrine pancreatic tumors (13 patients), the objective response rate was 38%. Complete remissions were found in 5% (2/39), partial remissions in 18% (7/39), stable disease in 69% (27/39), and progressive disease in 8% (3/39). A significant reduction of clinical symptoms could be found in 83% of patients with diarrhea, in 46% of patients with flush, in 63% of patients with wheezing, and in 75% of patients with pellagra. The overall clinical benefit was 63%. All responses (both clinical benefit and WHO response) were ongoing for the duration of follow-up (median, 6 mo; range, 2–12 mo). Side effects were grade 3 or 4 (NCI-CTC) lymphocytopenia in 23%, grade 3 anemia in 3%, and grade 2 renal insufficiency in 3%. Conclusion: High-dose targeted radiotherapy with 7.4 GBq/m2 90Y-DOTATOC is a well-tolerated treatment for neuroendocrine tumors, with remarkable clinical benefit and objective response.
Neuroendocrine tumors (NETs) represent a collection of diverse tumor types derived from common cell lines and unified by the secretion of neuropeptides. The excessive secretion of neuropeptides may give rise to distinct clinical syndromes. Malignant NETs and syndromes have a poor prognosis because curative surgery can be offered to <5% of all patients (1–5). Nevertheless, surgery remains a cornerstone in both managing severe clinical syndromes and facilitating medical treatment. Chemotherapy was considered the treatment standard of NETs until the 1980s, when therapies with α-interferon and somatostatin analogues that could significantly improve clinical management were developed. Determination of somatostatin receptor subtype in tumor tissues and development of subtype-specific analogues for therapy are new approaches in the treatment of NETs and the carcinoid syndrome (1–3,6–12). In recent years, many research groups in nuclear medicine and radiopharmacy have been trying to develop a somatostatin analog that has high affinity to the somatostatin receptor and can be linked to a therapeutic β-emitting radioisotope. If isotopes emitting β-particles are used for peptide labeling, the radiation emitted from a radiolabeled peptide bound to a tumor cell may also kill neighboring cells because the pathlength of β-particles can extend over several cell diameters. The crossfire of β-particles can, in theory, destroy both somatostatin receptor-positive and somatostatin receptor-negative tumor cells. In 1996, the first promising dodecanetetraacetic acid–chelated somatostatin analog was presented (13)—a hydrophilic peptide vector that can be labeled stably with either the β-emitting therapeutic radionuclide yttrium (90Y) or diagnostic indium (111In) (14–19). The affinity of 90Y-labeled 1,4,7,10-tetra-azacyclododecan-4,7, 10-tricarboxy-methyl-1-yl-acetyl-d-Phe (1)-Tyr3-octreotide (DOTATOC) to the somatostatin receptor, especially to its subtypes 2 and 5, was found to be high. In a phase I study, we found that 33% of the patients who received cumulative doses of >8.5 GBq/m2 90Y-DOTATOC without kidney protection had dose-limiting renal toxicity (19). The maximum tolerated dose defined in this phase I trial was 6 GBq/m2 (33% less than 8.5 GBq/m2) with amino acid–kidney protection, and in a phase II trial with this dose the overall response rate (according to World Health Organization [WHO] criteria) was 24% in patients with NETs of gastroenteropancreatic or bronchial origin (20). Therefore, this study was undertaken to evaluate the clinical benefit and objective response rate of high-dose treatment (7.4 GBq/m2 with renal protection).
MATERIALS AND METHODS
The study was approved by the local ethical committee and the Swiss authorities.
Selection of Patients
We included 39 patients (mean age, 55 y) with gastroenteropancreatic or bronchial NETs. To be included, patients had to have a histologically confirmed diagnosis of NET, progressive disease before starting the treatment, strongly positive tumors on 111In-DOTATOC or 111In-pentetreotide (OctreoScan; Mallinckrodt, Inc., St. Louis, MO) scintigrams, a life expectancy > 6 mo, adequate organ function, no concurrent antitumor treatment, and written informed consent. Patients were excluded if they were younger than 18 y or pregnant, had a history of life-threatening atopic reactions, or had a severe concomitant illness, including severe psychiatric disorders.
Radiotracer
A dodecanetetraacetic acid–modified somatostatin analog named DOTATOC was synthesized in a 5-step procedure performed according to good medical practice (19–22). 111In- and 90Y-DOTATOC was prepared according to previously described procedures using 8 μg DOTATOC dissolved in 190 μL 0.4 mol/L sodium acetate buffer (pH 5.5) with 7 mg gentisic acid and 222 MBq 111InCl3 (0.05 mol/L HCl; Mallinckrodt Medical, Petten, The Netherlands). The solution was heated at 95°C for 25 min, and the quality was controlled using a Sep-Pak C18 cartridge (Waters, Milford, MA) and high-performance liquid chromatography. As a therapeutic radiometal, the pure β-emitter 90yttrium was linked stably to DOTATOC with preservation of receptor-binding affinity (dissociation constant, 2.6 ± 0.5 nmol/L; labeling yield, >99.5%).
Treatment
A fractionated treatment protocol was performed with 4 equal-dose intravenous injections administered at 6-wk intervals, resulting in a total of 7.4 GBq/m2 90Y-DOTATOC. For each session, patients were hospitalized for 2–3 d in accordance with the legal requirements for radioactivity protection and scintigraphic localization control. Thirty minutes before the injection of each treatment dose, 500 mL Hartmann-HEPA 8% amino acid solution (Ringer’s lactated Hartmann solution, Proteinsteril [B. Braun Medical AG, Sempach, Switzerland] HEPA 8%, Mg 5-Sulfat [B. Braun Medical AG]) were given to inhibit tubular reabsorption of the radiopeptide DOTATOC, followed by an additional 2,000 mL within 2.5 h after 90Y-DOTATOC bolus injection. In each 90Y-DOTATOC session, 111 MBq 111In-DOTATOC were injected simultaneously to control for DOTATOC binding. One, 24, and 48 h after injection, static images (5 min per image) were acquired using a gamma camera with a large field of view (Diacam; Siemens Medical Systems, Inc., Hoffman Estates, IL), equipped with a medium-energy parallel-hole collimator (matrix, 64 × 64; zoom, 1).
Evaluation of Results and Assessment of Clinical Benefit
Four weeks before the first and 8–12 wk after the last internal radiotherapy, tumor growth and tumor response were monitored by either conventional CT, sonography, or MRI. Tumor response was defined according to the WHO standard criteria and was evaluated every 3 mo along with blood counts and chemistry. In addition, complete blood cell and platelet counts were obtained every 2 wk for at least 6 wk after therapy and every 3 mo thereafter. Thyroid-stimulating hormone was measured after every treatment cycle. Side effects of 90Y-DOTATOC treatment were investigated and scored according to the National Cancer Institute grading criteria (NCI-CTC).
A detailed questionnaire using the NCI-CTC was developed. The last consecutive 21 patients were asked to fill out the questionnaires about their disease history and their clinical features and score them according to the NCI-CTC before and after each cycle of treatment. For the first 18 patients, the questionnaire was not available yet.
RESULTS
Patients
The study included 13 patients with endocrine pancreatic tumors (EPT), 12 patients with NET of intestinal origin, 3 patients with NET of bronchial origin, 9 patients with NET of unknown origin, and 2 patients with other NET entities. All patients showed tumor growth as assessed with radiologic or scintigraphic scans before starting 90Y-DOTATOC therapy. Detailed patient characteristics are listed in Table 1.
Patient Characteristics
Tumor Response and Survival
The responses of the individual tumor types are listed in Table 2. For illustration, 2 scintigraphic examples of remissions are shown in Figures 1–4. Eight to 12 wk after therapy, the tumor response was monitored by CT in 30 patients, sonography in 5 patients, and MRI in 4 patients.
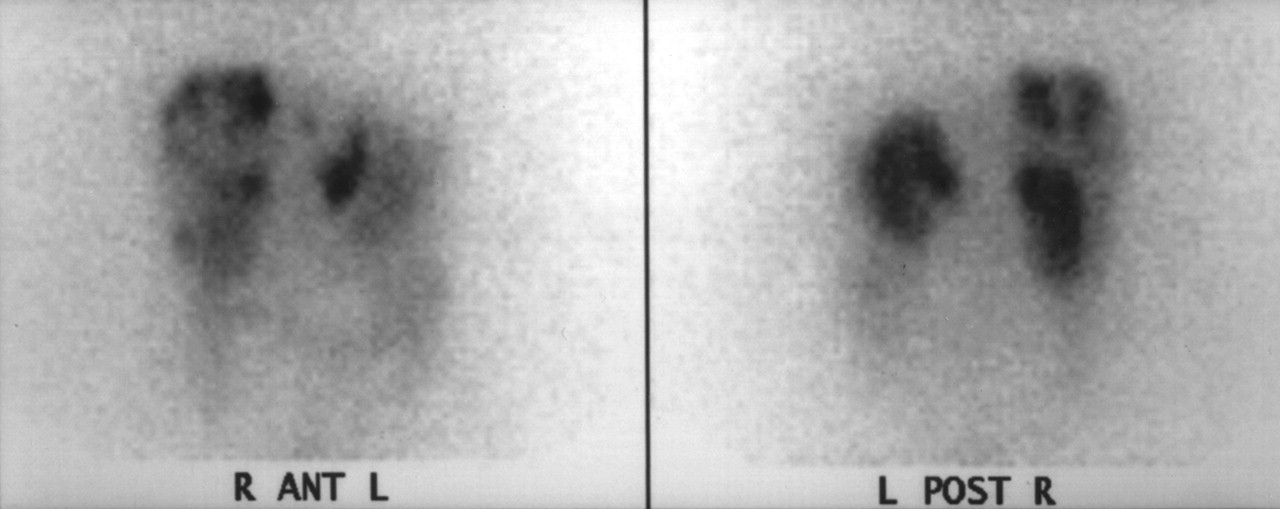
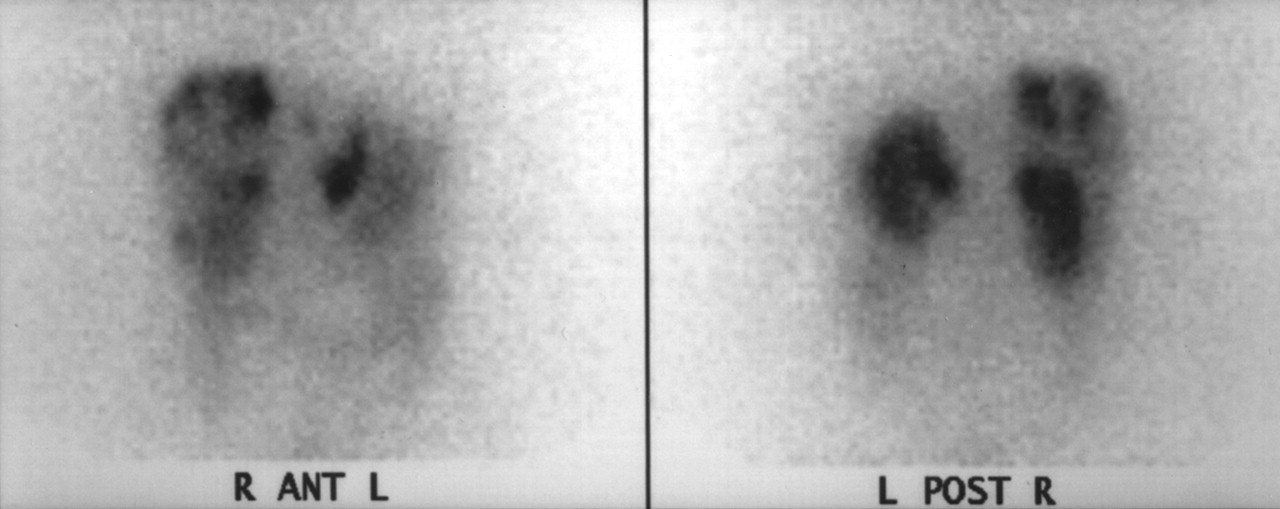
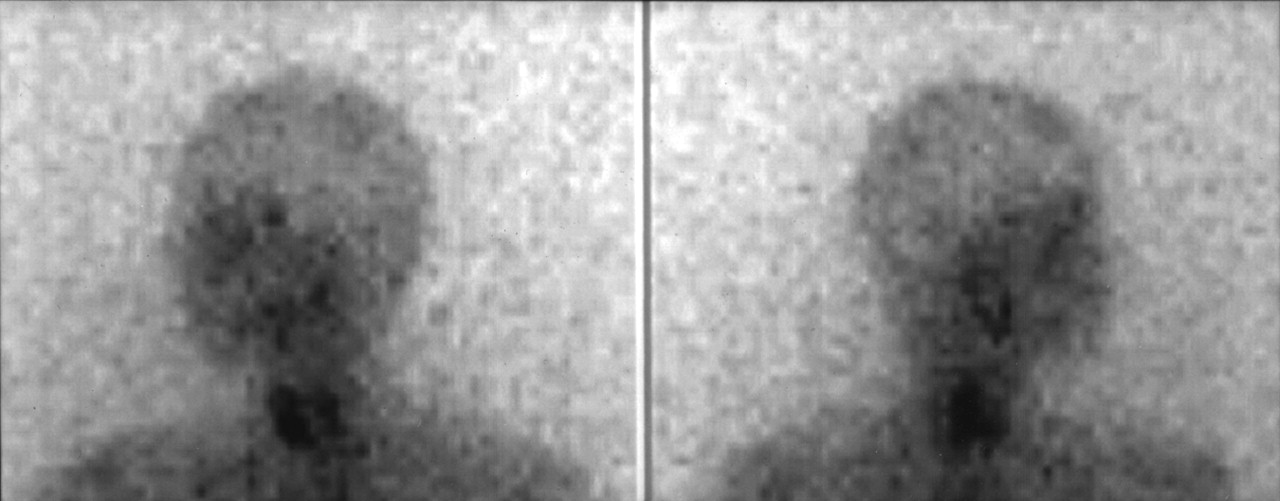
111In-DOTATOC scintigram of abdomen of 43-y-old woman with recurrence of EPT and multiple liver metastases before DOTATOC treatment. ANT = anterior; POST = posterior.

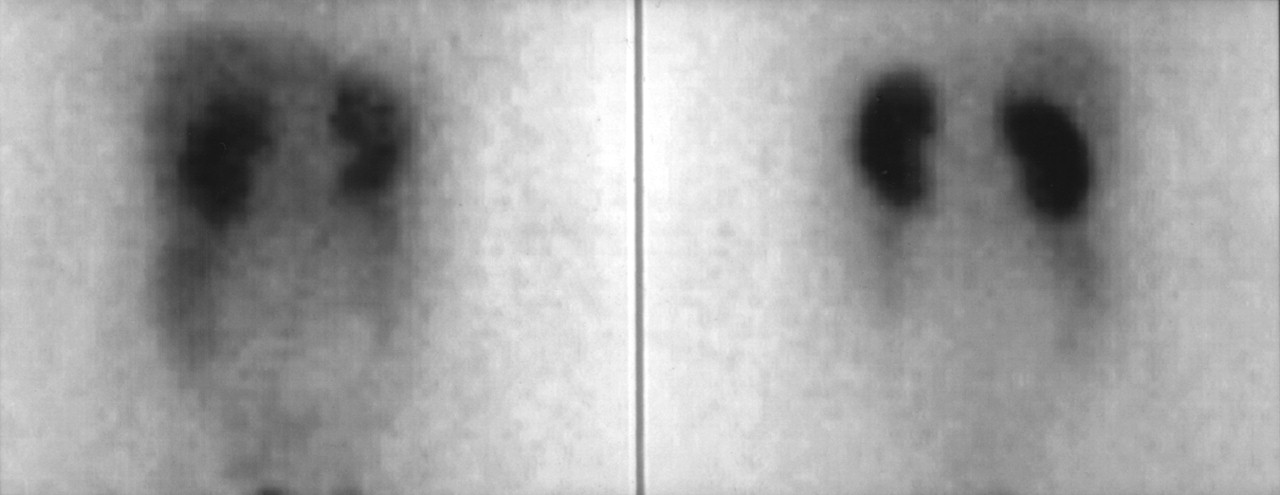
After DOTATOC treatment, 111In-DOTATOC scintigram (anterior [left] and posterior [right] images) of abdomen revealed no enhancement in pancreas region or in liver. MRI finding was complete remission.

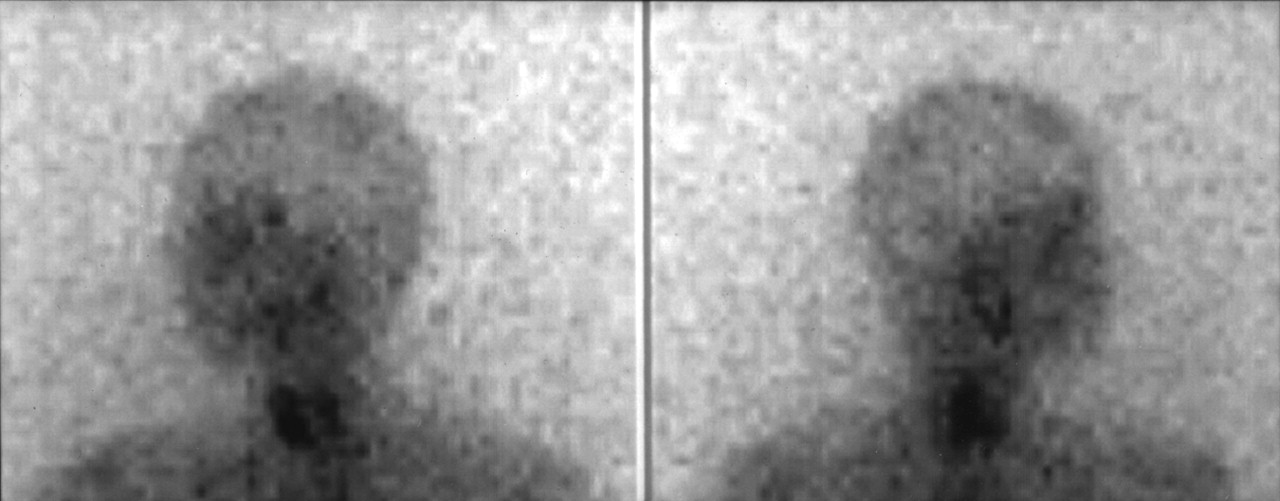
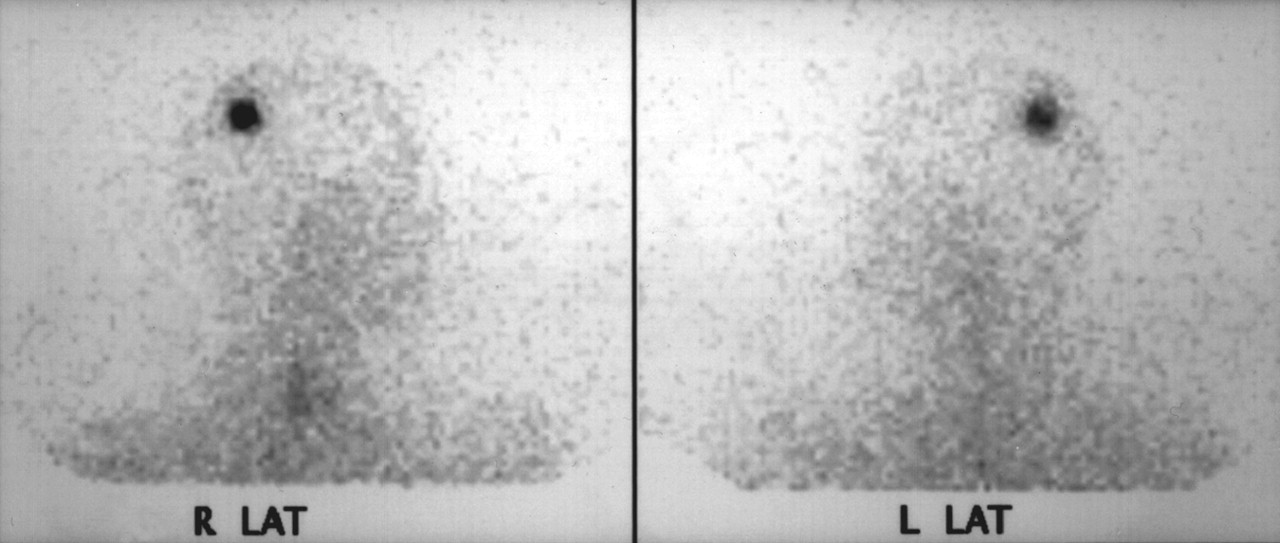
111In-DOTATOC scintigram of 43-y-old woman with neuroendocrine cerebral metastasis of EPT before DOTATOC treatment. LAT = lateral.
After DOTATOC treatment, 111In-DOTATOC scintigram (left and right lateral images) revealed no enhancement. CCT finding was partial remission.
Tumor Response (WHO Standard Criteria)
Complete remissions were found in 2 (5%) of 39 patients, partial remissions in 7 (18%) of 39 patients, stable disease in 27 (69%) of 39 patients, and tumor progression during or after treatment in 3 (8%) of 39 patients. The overall tumor response rate was 23%. For patients with EPT, the response rate was 38%. In 92% of patients, the disease could be stabilized (complete remission, partial remission, or stable disease).
Currently, 32 of 39 patients have no tumor progression and 4 patients have progressive disease. One patient died after the third treatment cycle because of hepatic failure caused by bacterial cholangiolitis. Two patients died within 3 mo after therapy because of tumor progression and hepatic decompensation.
Toxicity
During 90Y-DOTATOC injection, nausea occurred in 48% of patients and vomiting in 29%. After each cycle, 33% had grade 1–2 nausea; grade 3 nausea was experienced by 1 patient in 1 cycle. All cases of nausea and vomiting could be treated successfully with domperidone or ondansetron.
All patients had the lowest blood counts at the final treatment. At that time, 61% of the patients (24/39) had grade 1–4 lymphocytopenia: 8% had grade 4, 15% had grade 3, and 38% had grade 1 or 2. After 3–4 wk, the values returned to baseline and all patients could receive treatment according to the protocol. Reversible anemia developed in 51% of all patients, 3% of whom had grade 3 and 48%, grade 1 or 2. No blood transfusions were needed. In 15% of all patients, grade 1 thrombocytopenia was found. Thyroid-stimulating hormone levels were normal in all patients throughout the whole trial.
With a single exception, serum creatinine values remained normal during and after treatment (median follow-up, 6 mo). Five months after the fourth cycle, the serum creatinine level of 1 patient had increased from baseline (100 μmol/L before therapy and 230 μmol/L after therapy [reference range, 45–93 μmol/L], NCI-CTC grade 2). The serum creatinine remained at this level during follow-up.
Assessment of Clinical Benefit
Twenty-one consecutive patients completed a clinical benefit questionnaire (18 questions) about their disease history and their clinical features (symptoms of malignant carcinoid syndrome and tumor-associated pain). They scored all symptoms according to NCI-CTC before and after each treatment cycle. An example of scoring is shown in Table 3. Specific medical questions were translated into a language that patients understood.
Example of Scoring (6 of 18 Questions) According to National Cancer Institute Grading Criteria
Malignant Carcinoid Syndrome.
Fourteen (67%) of the 21 patients had malignant carcinoid syndrome despite receiving octreotide medication (Sandostatin or Sandostatin LAR; Novartis Pharmaceuticals Corp., East Hanover, NJ) before 90Y-DOTATOC-therapy. Six (43%) of the 14 patients with malignant carcinoid syndrome had diarrhea: grade 4 in 2, grade 3 in 1, grade 2 in 2, and grade 1 in 1. In 3 patients (50%), the diarrhea disappeared completely, and in 3 patients (50%), the diarrhea improved by at least 1 grade.
Fourteen (67%) of the 21 patients had intermittent flushes: grade 3 in 4, grade 2 in 6, and grade 1 in 4. The flushes disappeared completely in 3 patients (23%), improved by at least 1 grade in 6 patients (46%), and deteriorated during therapy in 2 patients (15%). Eight patients (38%) had wheezing or dyspnea: grade 3 wheezing in 3, grade 2 wheezing or dyspnea in 4, and grade 1 dyspnea in 1. In 2 patients (25%), the wheezing disappeared completely; in 5 patients (63%), the wheezing or dyspnea improved by at least 1 grade; and in no patients was the wheezing exacerbated during therapy. Four patients (19%) had pellagra: grade 2 in 1 and grade 1 in 3. In 3 patients (75%), the pellagra disappeared completely.
The overall clinical benefit rate was 63%.
Tumor-Associated Pain and Abdominal Pressure.
Nine of 21 patients had pain caused mainly by bone or liver metastases. Two had morphine-dependent pain; after 90Y-DOTATOC treatment, the medication of the first of these patients could be changed to nonsteroidal antiinflammatory drugs, and the second patient could discontinue analgesic drugs. In 5 (56%) of 9 patients, pain improved, and is still improved, by at least 1 grade. The level of pain improvement was independent of the degree of tumor reduction. Even patients who showed progression while undergoing therapy experienced a short-term clinical benefit of a few weeks or months.
DISCUSSION
The primary objective of this study was to compare the utility of 90Y-DOTATOC radionuclide therapy with that of standard treatment regimes. For advanced NET, the somatostatin analogue octreotide or lanreotide is the treatment of choice (6,23). Therapy with long-acting somatostatin analogues is reported to cause a tumor response in 12% of patients with EPT and a stabilization of disease in 25%–30% of patients (24). A Swedish research team found biochemical responses to a long-acting formulation in 40%–70% but an objective tumor response (WHO) in only 4%–10% (6). In a further study, in which NETs were treated with lanreotide, Ruszniewski et al. (24) showed subjective response rates of 50% and biochemical response rates of 42% but no objective tumor response. Alternatively, α-interferon is reported to have a biochemical response rate of 43% in patients with EPT and an objective response rate of 11% (6,24,25). In cases of tumor progression (clinical, biochemical, or objective) under the above-mentioned therapies, dose escalation of somatostatin analogues can be tried or, alternatively a combination of α-interferon and a somatostatin analog (1,2,6,24,25). If these treatments fail, patients are usually treated with chemotherapy (streptozotocin and 5-fluorouracil, or cisplatinum and etoposide) (6,23). Randomized trials have not established a standard chemotherapy protocol, and most evaluated chemotherapies have had response rates of <20% (6). Polychemotherapies in the treatment of NET have a high toxicity (23,25–30).
Compared with these standard regimes, treatment with 90Y-DOTATOC resulted in an objective response of 23% overall and a remarkable 38% for patients with EPT. Many of the patients in our trial were pretreated, and all had progressive disease. In these advanced malignancies, the tumors stabilized in 92% of the patients. Nevertheless, increasing the total dose from 6 GBq/m2, as used in our previous study, to 7.4 GBq/m2 did not improve the tumor response significantly, but our previous results were clearly confirmed in this trial. In general, 90Y-DOTATOC treatment was well tolerated and toxicity was mild; however, use of 7.4 GBq/m2 caused a case of renal toxicity. Importantly, there was a profound palliative effect both concerning the malignant carcinoid syndrome and concerning tumor-associated pain. This benefit seemed to be independent of an objective response.
CONCLUSION
Our study suggests that 90Y-DOTATOC is a remarkable therapeutic drug and an effective alternative to all chemo- and biotherapies known to us. Increasing the total dose from 6 to 7.4 GBq/m2 did not improve the outcome. To date, the dose-limiting toxicity of 90Y-DOTATOC has been renal insufficiency, starting at 7.4 GBq/m2 (19). The future goal is to further reduce renal toxicity so that significantly higher doses can be applied, hopefully resulting in higher response rates and better symptom control.
Acknowledgments
The authors thank Brigitte Leu and her staff for technical assistance and nursing. The authors are indebted to Daniela Biondo, Karin Hinni, Dr. Jörg Schmitt, and, especially, Pia Powell for nuclear pharmacy support. This study was supported by the Swiss National Science Foundation (grants 31-42516/94 and 31-452969/97) and the Regionale Krebsliga.
Footnotes
Received Mar. 5, 2001; revision accepted Oct. 25, 2001.
For correspondence or reprints contact: Jan Mueller-Brand, MD, Institute of Nuclear Medicine, University Hospital, Petersgraben 4, CH-4031 Basel, Switzerland.
E-mail: jmueller{at}uhbs.ch
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Peptide Receptor Radionuclide Therapy Is Effective for Clinical Control of Symptomatic Metastatic Insulinoma: A Long-Term Retrospective Analysis
- Safety of Peptide Receptor Radionuclide Therapy with 177Lu-DOTATATE in Neuroendocrine Tumor Patients with Chronic Kidney Disease
- NANETS/SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy
- Recombinant {alpha}1-Microglobulin Is a Potential Kidney Protector in 177Lu-Octreotate Treatment of Neuroendocrine Tumors
- Somatostatin Receptor 2-Targeting Compounds
- Dose Deposits from 90Y, 177Lu, 111In, and 161Tb in Micrometastases of Various Sizes: Implications for Radiopharmaceutical Therapy
- Metastatic Insulinoma: Current Molecular and Cytotoxic Therapeutic Approaches for Metastatic Well-Differentiated panNETs
- Somatostatin Receptor-Targeted Radiopeptide Therapy with 90Y-DOTATOC and 177Lu-DOTATOC in Progressive Meningioma: Long-Term Results of a Phase II Clinical Trial
- GEP-NETS UPDATE: Radionuclide therapy in neuroendocrine tumors
- Role of Somatostatin Analogues in the Treatment of Neuroendocrine Tumors
- PRRT: Defining the Paradigm Shift to Achieve Standardization and Individualization
- Targeted Radionuclide Therapy: Proceedings of a Joint Workshop Hosted by the National Cancer Institute and the Society of Nuclear Medicine and Molecular Imaging
- Long-Term Hematotoxicity After Peptide Receptor Radionuclide Therapy with 177Lu-Octreotate
- Molecular radiotherapy
- Cohort Study of Somatostatin-Based Radiopeptide Therapy With [90Y-DOTA]-TOC Versus [90Y-DOTA]-TOC Plus [177Lu-DOTA]-TOC in Neuroendocrine Cancers
- A New Era for the Systemic Therapy of Neuroendocrine Tumors
- Radiopeptide Imaging and Therapy in Europe
- Evaluation of 177Lu-DOTA-sst2 Antagonist Versus 177Lu-DOTA-sst2 Agonist Binding in Human Cancers In Vitro
- Therapeutic management of patients with gastroenteropancreatic neuroendocrine tumours
- Nuclear medicine techniques for the imaging and treatment of neuroendocrine tumours
- Therapeutic strategies for advanced neuroendocrine carcinomas of jejunum/ileum and pancreatic origin
- 177Lu-DOTATATE Molecular Radiotherapy for Childhood Neuroblastoma
- Altered Biodistribution of Somatostatin Analogues After First Cycle of Peptide Receptor Radionuclide Therapy
- Response, Survival, and Long-Term Toxicity After Therapy With the Radiolabeled Somatostatin Analogue [90Y-DOTA]-TOC in Metastasized Neuroendocrine Cancers
- Targeted Therapy in Advanced Well-Differentiated Neuroendocrine Tumors
- 68Ga-DOTATATE PET/CT for the Early Prediction of Response to Somatostatin Receptor-Mediated Radionuclide Therapy in Patients with Well-Differentiated Neuroendocrine Tumors
- In vivo targeting and growth inhibition of the A20 murine B-cell lymphoma by an idiotype-specific peptide binder
- 90Y-Edotreotide for Metastatic Carcinoid Refractory to Octreotide
- Somatostatin receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors
- Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients With Metastatic Neuroendocrine Midgut Tumors: A Report From the PROMID Study Group
- Midgut neuroendocrine tumours with liver metastases: results of the UKINETS study
- 68Ga-DOTA-Tyr3-Octreotide PET for Assessing Response to Somatostatin-Receptor-Mediated Radionuclide Therapy
- Treatment of Metastatic Carcinoid Tumors With Radiolabeled Biologic Molecules
- Carcinoid Tumors
- MIRD Pamphlet No. 20: The Effect of Model Assumptions on Kidney Dosimetry and Response--Implications for Radionuclide Therapy
- Treatment With the Radiolabeled Somatostatin Analog [177Lu-DOTA0,Tyr3]Octreotate: Toxicity, Efficacy, and Survival
- Utility of Radiolabeled Somatostatin Receptor Analogues for Staging/Restaging and Treatment of Somatostatin Receptor-Positive Pediatric Tumors
- Response to [90Yttrium-DOTA]-TOC Treatment is Associated with Long-term Survival Benefit in Metastasized Medullary Thyroid Cancer: A Phase II Clinical Trial
- [Lys40(Ahx-DTPA-111In)NH2]-Exendin-4 Is a Highly Efficient Radiotherapeutic for Glucagon-Like Peptide-1 Receptor-Targeted Therapy for Insulinoma
- Gastrointestinal neuroendocrine tumors: a role for targeted therapies?
- GLP-1 Receptor Expression in Human Tumors and Human Normal Tissues: Potential for In Vivo Targeting
- [Lys40(Ahx-DTPA-111In)NH2]Exendin-4, a Very Promising Ligand for Glucagon-like Peptide-1 (GLP-1) Receptor Targeting
- Predictive factors of efficacy of the somatostatin analogue octreotide as first line therapy for advanced pancreatic endocrine carcinoma
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- 177Lu-AMBA: Synthesis and Characterization of a Selective 177Lu-Labeled GRP-R Agonist for Systemic Radiotherapy of Prostate Cancer
- Anticancer Activity of Targeted Proapoptotic Peptides
- Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues
- Oral Versus Intravenous Administration of Lysine: Equal Effectiveness in Reduction of Renal Uptake of [111In-DTPA]Octreotide
- Megalin Is Essential for Renal Proximal Tubule Reabsorption of 111In-DTPA-Octreotide
- Evaluation of [99mTc/EDDA/HYNIC0]Octreotide Derivatives Compared with [111In-DOTA0,Tyr3, Thr8]Octreotide and [111In-DTPA0]Octreotide: Does Tumor or Pancreas Uptake Correlate with the Rate of Internalization?
- Treatment with 177Lu-DOTATOC of Patients with Relapse of Neuroendocrine Tumors After Treatment with 90Y-DOTATOC
- Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours
- Peptide Receptor Radionuclide Therapy for Non-Radioiodine-Avid Differentiated Thyroid Carcinoma
- A New Prostate Carcinoma Binding Peptide (DUP-1) for Tumor Imaging and Therapy
- Combination Radionuclide Therapy Using 177Lu- and 90Y-Labeled Somatostatin Analogs
- Long-Term Follow-Up of Renal Function After Peptide Receptor Radiation Therapy with 90Y-DOTA0,Tyr3-Octreotide and 177Lu-DOTA0, Tyr3-Octreotate
- Patient-Specific Dosimetry in Predicting Renal Toxicity with 90Y-DOTATOC: Relevance of Kidney Volume and Dose Rate in Finding a Dose-Effect Relationship
- 68Ga-Labeled Peptides in Tumor Imaging
- Therapeutic Efficacy of a 188Re-Labeled {alpha}-Melanocyte-Stimulating Hormone Peptide Analog in Murine and Human Melanoma-Bearing Mouse Models
- Overview of Results of Peptide Receptor Radionuclide Therapy with 3 Radiolabeled Somatostatin Analogs
- Practical Dosimetry of Peptide Receptor Radionuclide Therapy with 90Y-Labeled Somatostatin Analogs
- High Expression of Neuropeptide Y Receptors in Tumors of the Human Adrenal Gland and Extra-Adrenal Paraganglia
- Radiation Therapy of Small Cell Lung Cancer with 177Lu-DOTA-Tyr3-Octreotate in an Animal Model
- Quality of Life in Patients With Gastroenteropancreatic Tumors Treated With [177Lu-DOTA0,Tyr3]octreotate
- A Stylized Computational Model of the Rat for Organ Dosimetry in Support of Preclinical Evaluations of Peptide Receptor Radionuclide Therapy with 90Y, 111In, or 177Lu
- Inhomogeneous Localization of Radioactivity in the Human Kidney After Injection of [111In-DTPA]Octreotide
- Evaluating the Clinical Effectiveness of 90Y-SMT 487 in Patients with Neuroendocrine Tumors
- New Advances in Peptide Receptor Radionuclide Therapy