


Abstract
Therapy with [90Y-DOTA0, Tyr3]-octreotide (DOTATOC, where DOTA = tetraazacyclododecane tetraacetic acid and TOC = d-Phe-c(Cys-Tyr-d-Trp-Lys-Thr-Cys)-Thr(ol)) is established for the treatment of metastatic neuroendocrine tumors. Nevertheless, many patients experience disease relapse, and further treatment may cause renal failure. Trials with 177Lu-labeled somatostatin analogs showed less nephrotoxicity. We initiated a prospective study with 177Lu-DOTATOC in patients with relapsed neuroendocrine tumors after 90Y-DOTATOC treatment. Methods: Twenty-seven patients, pretreated with 90Y-DOTATOC, were included. The mean time between the last treatment with 90Y-DOTATOC and 177Lu-DOTATOC was 15.4 ± 7.8 mo (SD). All patients were injected with 7,400 MBq of 177Lu-DOTATOC. Restaging was performed after 8–12 wk. Hematotoxicity or renal toxicity of World Health Organization grade 1 or 2 was not an exclusion criterion. Results: Creatinine levels increased significantly, from 66 ± 14 μmol/L to 100 ± 44 μmol/L (P < 0.0001), after 90Y-DOTATOC therapy. The mean hemoglobin level dropped from 131 ± 14 to 117 ± 13 g/L (P < 0.0001) after 90Y-DOTATOC therapy. 177Lu-DOTATOC therapy was well tolerated. No serious adverse events occurred. The mean absorbed doses were 413 ± 159 mGy for the whole body, 3.1 ± 1.5 Gy for the kidneys, and 61 ± 5 mGy for the red marrow. After restaging, we found a partial remission in 2 patients, a minor response in 5 patients, stable disease in 12 patients, and progressive disease in 8 patients. Mean hemoglobin and creatinine levels did not change significantly. Conclusion: 177Lu-DOTATOC therapy in patients with relapse after 90Y-DOTATOC treatment is feasible, safe, and efficacious. No serious adverse events occurred.
Treatment options for metastatic neuroendocrine tumors are limited. Trials with long-acting somatostatin analogs (octreotide or lanreotide), interferon-α, or chemotherapy, mostly 5-fluorouracil based, have shown rather low response rates with regard to cytoreduction (1–3). However, somatostatin analogs inhibit flushing, diarrhea, and other symptoms of the carcinoid syndrome (4,5). A retrospective case series in 1996 suggested that survival has increased since the introduction of somatostatin analogs (6). In the last few years, treatment strategies with radiolabeled somatostatin analogs have shown more convincing results (7–13). The 3 most investigated radiopharmaceuticals in clinical trials are [111In-diethylenetriaminepentaacetic acid (DTPA)0]-octreotide, [90Y-DOTA0, Tyr3]-octreotide (DOTATOC, where DOTA = tetraazacyclododecane tetraacetic acid and TOC = d-Phe-c(Cys-Tyr-d-Trp-Lys-Thr-Cys)-Thr(ol)), and [177Lu-DOTA0, Tyr3, Thr8]-octreotide (DOTATATE) (7–13).
Initial studies with high activities of [111In-DTPA0]-octreotide were encouraging. Although partial remissions were not found, favorable effects on symptoms were reported. Many patients in poor clinical condition were included (12,13). For the other 2 radiopeptides, a high overall response rate and distinct improvement in quality of life could be demonstrated (10,14). Although the results with these radiolabeled somatostatin analogs seem promising, relapses occur after a certain time in many patients (15), and further treatment with 90Y-DOTATOC can cause renal failure (16). According to data in the literature, the median time to progression after treatment with 90Y-DOTATOC is 30 mo (17,18). For 177Lu-DOTATATE, the median time to progression had not been reached at 25 mo after the start of therapy (19).
In comparison to 90Y, which is a high-energy, pure β-emitter (Emax, 2.25 MeV), 177Lu is a low-energy β-emitter (maximum electron energy [Emax], 0.497 MeV) with a small γ-component that is suitable for scintigraphic imaging (133 keV [6.5%]; 208 keV [11%]) without using a radionuclide surrogate. Small peptides such as DOTATOC are reabsorbed by the proximal tubules of the kidneys (20). The damage that can occur after treatment with 90Y-DOTATOC is in the glomeruli. It is conceivable that the length of the β-particles influences kidney toxicity. This hypothesis is supported by animal experiments (21).
Renal toxicity has been identified as the dose-limiting factor of 90Y-DOTATOC therapy (9). In a study with [177Lu-DOTA0, Tyr3, Thr8]-octreotide, no nephrotoxicity was found (11). Although no long-term outcome data concerning nephrotoxicity after treatment with 90Y-DOTATOC or 177Lu-DOTATATE are available, we assumed that 177Lu might be less nephrotoxic than 90Y.
In vitro, a higher affinity to the somatostatin receptor subtype 2 was demonstrated for Y(III)-DOTATATE than for Y(III)-DOTATOC (22). However, because in humans a better tumor-to-kidney-ratio was found for 111In-DOTATOC than for 111In-DOTATATE (23), we decided to use DOTATOC as a DOTA-peptide conjugate labeled to 177Lu in patients with relapse.
We initiated a prospective feasibility study with 177Lu-DOTATOC in patients with relapse of neuroendocrine tumors after successful treatment with 90Y-DOTATOC. Because of the assumption that 177Lu-DOTATOC is less nephrotoxic than 90Y-DOTATOC, we did not consider World Health Organization (WHO) grade 1 or 2 renal toxicity, based on creatinine levels, to be an exclusion criterion, nor were patients with WHO grade 1 or 2 hematotoxicity excluded. Human data for 177Lu-DOTATATE show promising results and a tolerable toxicity for injected activities of around 22.2–29.6 GBq (600–800 mCi) in patients who are not pretreated with peptide receptor–mediated radionuclide therapy (11). But for 177Lu-DOTATOC, we could find no human data in the literature. Because our patients were pretreated with peptide receptor–mediated radionuclide therapy, and because no dosimetric data were available, we started with a relatively low injected activity. We treated all patients with a fixed activity of 7,400 MBq (200 mCi).
MATERIALS AND METHODS
The study was approved by the local ethical committee and the Swiss authorities. All patients gave written informed consent.
Patients
Twenty-seven patients (17 men and 10 women) were included. The mean age (± SD) was 58 ± 9 y. All patients had a histologically confirmed metastatic neuroendocrine tumor, which was progressive at the time of treatment. The progression was demonstrated by CT or ultrasound in all patients. All patients were pretreated with 90Y-DOTATOC and benefited from this treatment. Benefit was defined as complete remission, partial remission, minor response, or stable disease according to the WHO standard criteria. For the partial remissions in our collective, the mean time to progression was 15.4 ± 6.9 mo. Many patients were pretreated with surgery, chemotherapy, octreotide, or interferon as well. Details are listed in Table 1.
Patient Characteristics
Pretherapeutically, all patients underwent staging with CT, 111In-pentetreotide scintigraphy (OctreoScan; Mallinckrodt, Inc.), complete blood counts, and blood chemistry. The findings of 111In-octreotide scintigraphy were strongly positive in all patients. None of the patients had been treated with the long-acting somatostatin analogs octreotide (Sandostatin LAR; Novartis) or lanreotide (Somatuline; Ipsen) during at least the last 6 wk before receiving 177Lu-DOTATOC or with short-acting octreotide (Sandostatin s.c.; Novartis) during the last 3 d before receiving 177Lu-DOTATOC.
Radiotracer
DOTATOC was synthesized as previously described (24). For radiolabeling DOTATOC, we used lyophilized kits containing DOTATOC, gentisic acid, inositol, and sodium ascorbate (pH 5.0).
We added 7,400 MBq of 177LuCl3 (IDB Holland BV) to the lyophilized DOTATOC kits and heated them for 30 min at 95°C. After they had been cooled to room temperature, a quality control check was performed using an analytic high-performance liquid chromatograph (model 1050; Hewlett Packard) with a radiometric detector (model LB 506 C1; Berthold). Additionally, the labeling yield was determined by separation of bound and free 177Lu3+ using Sep-Pak C18 cartridges (Waters). After 177Lu-DOTATOC had been loaded onto the cartridge, the free 177Lu was eluted with sodium acetate buffer (0.4 mol/L, pH 5.0), and bound 177Lu-DOTATOC was then eluted with methanol. Each fraction was measured on a γ-counter.
Treatment
The patients were hospitalized for 3 d in accordance with the legal requirements for radioactivity control. A single, fixed-activity treatment protocol was used. The injected activity was 7,400 MBq of 177Lu-DOTATOC. An infusion of 2,000 mL of an amino acid solution (Ringer’s lactated Hartmann solution, Proteinsteril [B. Braun Medical AG] HEPA 8%, Mg 5-Sulfat [B. Braun Medical AG]) to inhibit tubular reabsorption of the radiopeptide was started 30 min before administration of the radiopharmaceutical and was continued until up to 3 h after administration of the radiopharmaceutical (20,25,26).
Imaging and Dosimetry
Imaging was performed with a dual-head Prism 2000 XP camera (Picker) using parallel-hole, medium-energy, general-purpose collimators. The windows were centered over both 177Lu photon peaks (113 and 208 keV) with a window width of 20%. In 4 patients, whole-body scans for dosimetry were obtained immediately and at 4, 24, and 28 h after injection. The acquisition time for the whole-body scans was 15 min. In all other patients, whole-body scans and spot images were obtained after 24 and 28 h for control of biodistribution.
To determine blood clearance, we drew blood samples from 4 patients at 5, 10, 30, and 60 min and at 12, 4, 24, and 28 h after injection. Radioactivity in blood was measured with a γ-counter (Cobra II; Canberra-Packard).
For dosimetric calculations, regions of interest were drawn manually on the whole-body scans from anterior and posterior projections. Those parts of the kidneys showing tumor infiltration or superimposition were excluded from the evaluation of organ uptake. The Odyssey XP program (Philips Electronics N.V.) was used. Background regions were placed close to the regions of interest for background correction. The geometric mean value between anterior and posterior was taken and corrected for attenuation and physical decay. Whole-body activity acquired immediately after injection was defined as 100% of the injected activity. Data were expressed as percentage injected activity as a function of time. The resulting time–activity data were fitted to a monoexponential curve for the whole-body clearance and to a biexponential curve for the kidneys to calculate residence time. Published radiation dose factors were used to calculate the absorbed doses (27).
The activity in blood was fitted to a biexponential curve to determine the residence time in blood. The dose to the red marrow was calculated from the residence time in blood, assuming no specific uptake, a uniform distribution of activity, and clearance from red marrow equal to that from blood. A correction factor of 1 was used as described by Cremonesi et al. (28).
Evaluation of Results and Assessment of Clinical Benefit
Pretherapeutically, patients underwent disease staging. Eight to 12 wk after peptide receptor–mediated radionuclide therapy, tumor growth and tumor response were monitored by CT or ultrasound. Tumor response was defined according to the WHO standard criteria. In addition, complete blood cell and platelet counts were obtained every 2 wk for at least 8 wk or until resolution of nadir. Side effects were scored according to the WHO criteria.
Statistics
Paired t testing was used to determine statistical significance. Differences at the 95% confidence level (P < 0.05) were considered significant.
RESULTS
The study included 27 patients with metastasized tumors, 11 of whom had neuroendocrine pancreatic tumors and 16, neuroendocrine tumors of other sites (7 of the small bowel, 4 of unknown primary, 2 of the rectum, 1 of the stomach, 1 of the bronchus, and 1 of the appendix). Detailed patient characteristics are listed in Table 1.
Evaluation of Long-Term Outcome After 90Y-DOTATOC Therapy
All patients had progressive disease before 90Y-DOTATOC therapy and before 177Lu-DOTATOC therapy. One criterion for inclusion into this study was benefit from 90Y-DOTATOC therapy. Of the 27 patients studied, we found a partial remission in 14, a minor response in 3, and stable disease in 10 at 3 mo after the last treatment with 90Y-DOTATOC.
The mean time between the last treatment with 90Y-DOTATOC and the treatment with 177Lu-DOTATOC was 15.4 ± 7.8 mo (range, 4–32 mo).
Before therapy with 90Y-DOTATOC, the mean hemoglobin level was 131 ± 14 g/L, the mean thrombocyte level was 306 ± 123 × 109/L, and the mean creatinine level was 66 ± 14 μmol/L. Before treatment with 177Lu-DOTATOC, the level of hemoglobin was significantly lower: 117 ± 13 g/L (P < 0.0001). The thrombocyte counts (263 ± 83 × 109/L) were lower as well but did not show significant changes. Creatinine levels increased to 100 ± 44 μmol/L. The difference was significant (P < 0.0001), although a high SD was seen. Details are listed in Table 2.
Blood Values and Clinical Results
Labeling of 177Lu-DOTATOC
The quality control testing of 177Lu-DOTATOC was done using 2 independent systems; the labeling efficiency was determined by analytic high-performance liquid chromatography and ranged from 99% to 100%. When the labeling yield was less than 99.5%, DTPA (1 mmol/L, pH 7.4) was added.
Dosimetry
Dosimetric calculations were performed on 4 patients and resulted in a mean whole-body absorbed dose of 413 ± 159 mGy. The mean absorbed dose to the kidney was 3.1 ± 1.5 Gy, and that to the red marrow was 61 ± 5 mGy.
Treatment with 177Lu-DOTATOC
The treatment was well tolerated. No severe adverse events occurred. Nausea and vomiting within the first 24 h after treatment occurred in 8 patients (30%). All cases of nausea and vomiting could be treated successfully with domperidone and ondansetron. Some increase of pain at the site of the tumor was experienced by 5 patients (19%) within the first 48 h after treatment. All cases could be controlled with analgesics. No other nonhematologic toxicity was found.
As expected. 177Lu-DOTATOC showed a high specific uptake in somatostatin receptor–positive tumors. The γ-component of 177Lu allowed acquisition of scintigraphic images of a high level of quality (Fig. 1A).

Anterior whole-body scans of patient 9. (A) Scan obtained 24 h after injection of 7,400 MBq of 177Lu-DOTATOC shows several abdominal metastases (liver, spleen, and lymph nodes). (B) Scan obtained 6 h after injection of 185 MBq 111In-Octreoscan 6 mo after treatment with 7,400 MBq of 177Lu-DOTATOC shows a decrease in tumor load. Especially, a reduction of liver metastases can be seen.
At the time of restaging, we found no change in creatinine levels. With these findings, late nephrotoxicity cannot be excluded definitely. But if nephrotoxicity arises, an increase in creatinine levels has usually been found 3 mo after treatment (16). Before treatment, 9 patients had grade 1 anemia and 1 had grade 2. Eight to 12 wk after treatment, 8 patients had grade 1 anemia, 1 had grade 2, and 1 had grade 3. The mean level of thrombocytes decreased significantly, from 263 ± 82 to 197 ± 70 × 109/L (P < 0.01). Details are listed in Table 2.
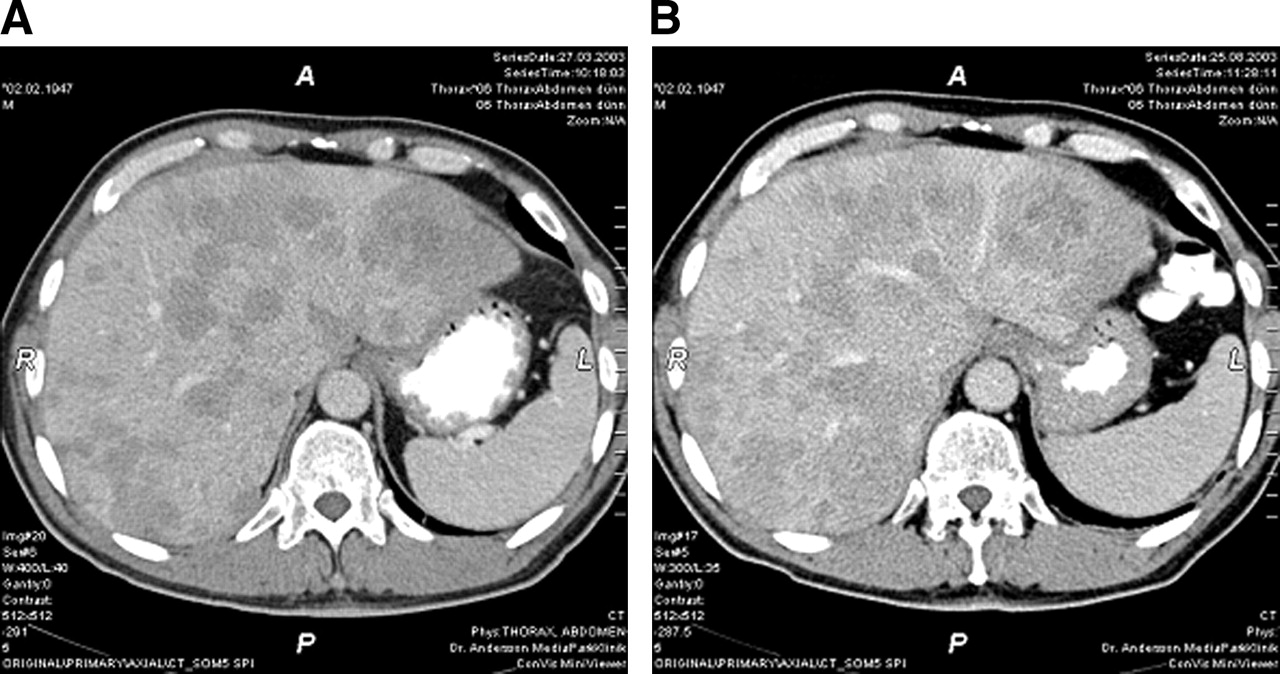
Eight to 12 wk after treatment, 8 patients did not show a benefit from peptide receptor–mediated radionuclide therapy and continued to have progressive disease. Nineteen patients (70%) showed a benefit: 12 with stabilization of the disease, 5 with a minor response, and 2 with partial remission. Scans of patient 9, with a minor response, are shown in Figure 1, and corresponding anatomic images are shown in Figure 2. According to the referring physicians, the general condition of the patients improved for 15 (56%), remained the same for 11 (41%), and decreased for only 1 (4%).

CT scans of patient 9. (A) Nine months after treatment with 90Y-DOTATOC and 4 wk before treatment with 177Lu-DOTATOC, CT scan shows multiple liver metastases. (B) Corresponding CT scan 4 mo after treatment with 177Lu-DOTATOC shows minor response.
The subgroup of patients who achieved partial remission after 90Y-DOTATOC (n = 14) included 2 with partial remission, 5 with a minor response, and 7 with stable disease after 177Lu-DOTATOC treatment. In no patient of this subgroup did the disease remain progressive.
The overall time of follow-up was 4–17 mo (mean, 11.0 ± 4.0 mo). The time of remission (stable disease, minor response, or partial remission) ranged from 4 to 13 mo (mean, 8.3 ± 3.4 mo). Presently, 8 patients are still without disease progression; therefore, the overall time to progression will increase further.
DISCUSSION
The labeling of 177Lu-DOTATOC was straightforward, and its application was safe. No serious adverse events occurred.
The group of 27 patients was selected from patients treated earlier with 90Y-DOTATOC; all showed stable disease, a minor response, or partial remission after treatment but experienced relapse rather early and a short time to progression (15 ± 7.8 mo) The time to progression after treatment with 90Y-DOTATOC in these patients was shorter than has been reported in the literature (18).
The absorbed doses to normal organs, especially to the kidneys, were low. In previous clinical trials, a cumulative absorbed dose to the kidneys of 23 or 27 Gy was taken as the maximum tolerated dose (11,26,29). But these values are controversial (30) because they are derived from external-beam radiation (31) with a potentially different mechanism. The low absorbed doses are compatible with the fact that no increase of creatinine levels was found.
When the clinical results after 177Lu-DOTATOC are correlated with the clinical results after 90Y-DOTATOC, a good response after 90Y-DOTATOC (partial remission in our patients) is obviously a positive prognostic factor for further radionuclide treatment. Some tumors seem to be especially suited for peptide receptor–mediated radionuclide therapy. Two reasons are possible: There could be a high density of somatostatin receptors leading to a high radiation-absorbed dose, or there could be some tumors that are more radiosensitive than others.
The general condition of the patients was not scaled before treatment with 177Lu-DOTATOC but was worse than before the first treatment with 90Y-DOTATOC because all patients had a longer history of illness and experienced progression after remission or stabilization after 90Y-DOTATOC therapy. The total amount of injected activity (fixed activity, 7,400 MBq of 177Lu-DOTATOC) was rather low because we included patients with an increased serum creatinine level or with a diminished hemoglobin level.
The toxicity in patients with increased creatinine or diminished hemoglobin levels was not different from that in patients with normal values. We found no severe toxicity and, especially, no increase of creatinine levels. Therefore, we conclude that the treatment with 177Lu-DOTATOC in cases of relapse after treatment with 90Y-DOTATOC is feasible and safe. Clinical improvement could be observed, and most patients benefited from the treatment.
With regard to the radiobiologic mechanisms of 177Lu and 90Y, the combination of the 2 radionuclides could improve the biologic efficiency. The high-energy β-emitter 90Y deposits high doses to tumors and also to areas with low target protein expression and to heterogeneous tumor tissue. Because of the strong crossfire effect, parts of the tumor that either are poorly differentiated and therefore have a low density of somatostatin receptors or are poorly vascularized can be reached. 177Lu, on the other hand, seems to have more favorable physical characteristics for the treatment of small tumors (32–34).
Another mechanism that is not well defined is the so-called low-dose hypersensitivity-inducible radioresistance hypothesis as described by Joiner et al. (35). The administration of only a low absorbed dose at a low dose rate might be more effective in inducing tumor cell death than are higher absorbed doses.
CONCLUSION
Treatment with 177Lu-DOTATOC of patients who were pretreated with 90Y-DOTATOC is feasible and appears to be safe even when patients present with grade 1 or 2 hematotoxicity or nephrotoxicity. Clinical response at a low injected activity is promising. A good response after treatment with 90Y-DOTATOC is a positive predictor for successful treatment with 177Lu-DOTATOC.
Acknowledgments
We thank all supporting personnel of the Division of Radiologic Chemistry and the Institute of Nuclear Medicine for their expert help and effort, and we gratefully thank Martin Speiser and Marlies Meury for technical assistance and nursing. We are indebted to Daniela Biondo, Priska Preisig, Nadia Mutter, Pia Powell, and Stefan Good for nuclear pharmacy support. This work was supported by the Swiss National Science Foundation (grant 31-452969/97) and was performed within the COST B12 action.
Footnotes
Received Dec. 20, 2004; revision accepted Apr. 7, 2005.
For correspondence or reprints contact: Flavio Forrer, MD, Institute of Nuclear Medicine, University Hospital Basel, Petersgraben 4, CH-4031 Basel, Switzerland.
E-mail: fforrer{at}uhbs.ch
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Reimbursement Approaches for Radiopharmaceutical Dosimetry: Current Status and Future Opportunities
- Twelve-Year Follow-up After Peptide Receptor Radionuclide Therapy
- Parametric Net Influx Rate Images of 68Ga-DOTATOC and 68Ga-DOTATATE: Quantitative Accuracy and Improved Image Contrast
- Dose Response of Pancreatic Neuroendocrine Tumors Treated with Peptide Receptor Radionuclide Therapy Using 177Lu-DOTATATE
- Targeted Radionuclide Therapy: Proceedings of a Joint Workshop Hosted by the National Cancer Institute and the Society of Nuclear Medicine and Molecular Imaging
- Radiopeptide Imaging and Therapy in Europe
- Nuclear medicine techniques for the imaging and treatment of neuroendocrine tumours
- Response and Long-Term Control of Bone Metastases After Peptide Receptor Radionuclide Therapy with 177Lu-Octreotate
- Dynamic and Static Small-Animal SPECT in Rats for Monitoring Renal Function After 177Lu-Labeled Tyr3-Octreotate Radionuclide Therapy
- Salvage Therapy with 177Lu-Octreotate in Patients with Bronchial and Gastroenteropancreatic Neuroendocrine Tumors
- 68Ga-DOTA-Tyr3-Octreotide PET for Assessing Response to Somatostatin-Receptor-Mediated Radionuclide Therapy
- Electron- and Positron-Emitting Radiolanthanides for Therapy: Aspects of Dosimetry and Production