


Abstract
68Ga-DOTATOC and 68Ga-DOTATATE are radiolabeled somatostatin analogs used for the diagnosis of somatostatin receptor–expressing neuroendocrine tumors (NETs), and SUV measurements are suggested for treatment monitoring. However, changes in net influx rate (Ki) may better reflect treatment effects than those of the SUV, and accordingly there is a need to compute parametric images showing Ki at the voxel level. The aim of this study was to evaluate parametric methods for computation of parametric Ki images by comparison to volume of interest (VOI)–based methods and to assess image contrast in terms of tumor-to-liver ratio. Methods: Ten patients with metastatic NETs underwent a 45-min dynamic PET examination followed by whole-body PET/CT at 1 h after injection of 68Ga-DOTATOC and 68Ga-DOTATATE on consecutive days. Parametric Ki images were computed using a basis function method (BFM) implementation of the 2-tissue-irreversible-compartment model and the Patlak method using a descending aorta image–derived input function, and mean tumor Ki values were determined for 50% isocontour VOIs and compared with Ki values based on nonlinear regression (NLR) of the whole-VOI time–activity curve. A subsample of healthy liver was delineated in the whole-body and Ki images, and tumor-to-liver ratios were calculated to evaluate image contrast. Correlation (R2) and agreement between VOI-based and parametric Ki values were assessed using regression and Bland–Altman analysis. Results: The R2 between NLR-based and parametric image–based (BFM) tumor Ki values was 0.98 (slope, 0.81) and 0.97 (slope, 0.88) for 68Ga-DOTATOC and 68Ga-DOTATATE, respectively. For Patlak analysis, the R2 between NLR-based and parametric-based (Patlak) tumor Ki was 0.95 (slope, 0.71) and 0.92 (slope, 0.74) for 68Ga-DOTATOC and 68Ga-DOTATATE, respectively. There was no bias between NLR and parametric-based Ki values. Tumor-to-liver contrast was 1.6 and 2.0 times higher in the parametric BFM Ki images and 2.3 and 3.0 times in the Patlak images than in the whole-body images for 68Ga-DOTATOC and 68Ga-DOTATATE, respectively. Conclusion: A high R2 and agreement between NLR- and parametric-based Ki values was found, showing that Ki images are quantitatively accurate. In addition, tumor-to-liver contrast was superior in the parametric Ki images compared with whole-body images for both 68Ga-DOTATOC and 68Ga DOTATATE.
Neuroendocrine tumors (NETs) are tumors derived from the disseminated system of endocrine cells in the body and have diverse biologic and clinical characteristics (1). Epidemiologic studies have shown that the NET incidence is rising, and according to an analysis of the North American Surveillance, Epidemiology, and End Results registry data the annual age-adjusted incidence increased from 1.09/100,000 in 1973 to 5.25/100,000 in 2004. The reason for this is assumed to be the improvements in imaging technology (2).
NETs are characterized by cellular overexpression of somatostatin receptors (SSTRs), allowing for the use of unlabeled and radiolabeled somatostatin analogs (SSAs) for imaging and therapy. SSTR scintigraphy with the 111In-labeled SSA 111In-DTPA-octreotide (OctreoScan; Mallinckrodt Inc.) remains the mainstay for functional NET imaging and continues to play an important role for NET imaging (3,4). However, PET using 68Ga-labeled SSAs, such as 68Ga-DOTATOC, 68Ga-DOTANOC, and 68Ga-DOTATATE, is gradually replacing SSTR scintigraphy and is expected to become the future gold standard for SSTR imaging of NETs (5). PET/CT with 68Ga-SSA shows a specificity and sensitivity well above 90%, exceeding that of OctreoScan and CT (6–11).
In disseminated disease, unlabeled SSA constitutes first-line therapy for low-grade NETs. During the last decade, peptide receptor radionuclide therapy (PRRT), with radiolabeled SSAs such as 177Lu-DOTATATE and 90Y-DOTATOC, has been shown to be effective and plays an increasingly important role in the treatment of NET patients (12–21). However, large interpatient variability in organ distribution and consequently radiation dose delivered to the lesions and normal organs calls for the development of methods for individualized radiotherapy planning (22). Conventional radiologic imaging techniques such as CT and MRI are well established for the evaluation of therapy response in the clinical routine by assessing changes in tumor size and diagnosing new lesions. The RECIST (23), are, however, not optimal to monitor systemic NET therapies because tumor shrinkage is seen only in a small fraction of patients and instead the treatments mainly induce tumor stabilization. Moreover, PRRT induces long-time effects due to β-emission of 177Lu and 90Y, resulting in continuously increasing necrosis and decrease of viable tumor although the tumor size may appear unchanged during the subsequent examinations (24). Also, with the new so-called targeted therapies tumor shrinkage is less common and the heterogeneous nature of tumors also adds uncertainty to such measurements. There is therefore a need for new methods to evaluate NET therapy response besides conventional morphologic size criteria (25).
In parallel with the increasing use of 18F-FDG PET/CT for therapy monitoring in conventional oncology, this application has also been suggested for NETs. However, because of the low proliferation and low metabolic activity of NET cells, they are generally not 18F-FDG–avid (26). By contrast, most NETs express SSTRs and show high 68Ga-SSA uptake. Consequently, 68Ga-DOTATOC and 68Ga-DOTATATE have been tested to assess NET therapy response (6,24,27). In 1 study (24), the authors found that the changes in tumor SUV between baseline and follow-up 68Ga-DOTATOC PET/CT did not correlate to the outcome of PRRT. This was also found in another study (27), although changes in the tumor-to-spleen SUV ratio between baseline and follow-up 68Ga-DOTATOC were shown to be more accurate than changes in tumor SUVmax to evaluate the response to PRRT. The problems of applying static tumor uptake measurements in these 2 therapy monitoring studies may be explained, at least partly, by the results in a recent study (6) on 68Ga-DOTATOC and 68Ga-DOTATATE. In this study, SUV saturated at a static value for high net uptake rate (Ki), especially for higher SUVs (>20–25). Hence, SUV does not appear to reflect SSTR density for tumors with high receptor expression. Consequently, changes in Ki may better reflect treatment response than changes in SUV.
To facilitate the clinical use of Ki, accurate and reliable computation of parametric images showing Ki at the voxel level is desirable. Moreover, information on Ki at the voxel level provides information on tumor heterogeneity that is lost when average tumor Ki is assessed. The aim of this study was to evaluate methods for computation of parametric Ki images by comparison to volume of interest (VOI)–based methods. A secondary aim was to explore the conditions for lesion detection in Ki images by assessing the image contrast in terms of tumor-to-liver ratios compared with those in static SUV images.
MATERIALS AND METHODS
Patients
Ten patients (6 men and 4 women; mean age ± SD, 65 ± 10 y) diagnosed with disseminated gastroenteropancreatic NETs, confirmed by histopathology, were included in the study. Five patients had small-intestinal NETs, 3 had pancreatic NETs, and 2 had lung carcinoids. The total number of tumors included in the study was 16; 5 patients had 1 tumor, 1 patient had 2 tumors, and 3 patients had 3 tumors. Only tumors with a diameter of more than 1 cm and high uptake (determined visually) were included. The study was approved by the Regional Ethical Review Board in Uppsala and the Radiation Ethics Committee at Uppsala University Hospital, and all patients signed a written informed consent form before inclusion in the study.
Image Acquisition and Reconstruction
Each patient underwent a 68Ga-DOTATOC and 68Ga-DOTATATE PET/CT examination on consecutive days, in random order. The patients received a bolus injection of 86.9 ± 16.4 MBq (range, 61–113 MBq) of 68Ga-DOTATOC and 91.4 ± 18.7 MBq (range, 67–121 MBq) of 68Ga-DOTATATE. Good manufacturing practice–compliant production of 68Ga-DOTATOC and 68Ga-DOTATATE was accomplished as previously described (6,28).
Images were acquired on a Discovery ST PET/CT scanner (GE Healthcare) with a transaxial and axial field of view of 70 and 15.7 cm, respectively. The image matrix size was 128 × 128, with a voxel size of 3.9 × 3.9 × 3.27 mm. The patients underwent a low-dose CT scan (140 kV; auto mA; 20–80 mA) followed by a 45-min dynamic PET examination of the abdomen to include the major tumor load. The dynamic PET examination started simultaneously with the intravenous injection of 68Ga-DOTATOC or 68Ga-DOTATATE and consisted of 22 time frames of increasing durations (6 × 10, 3 × 20, 3 × 60, 5 × 180, and 5 × 300 s). The dynamic examination was followed by a whole-body PET/CT scan ranging from the proximal femur to the base of the skull (3 min per bed position) starting at 60 min after injection after a second low-dose CT for attenuation correction of the whole-body images. Peripheral venous blood samples (∼1 mL) were taken at 5, 20, 45, and 60 min after injection to assess the whole-blood and plasma radioactivity concentrations, respectively. The PET data were normalized and corrected for dead time, random coincidences, scatter, and attenuation and were reconstructed using ordered-subsets expectation maximization with 2 iterations and 21 subsets applying a 5.4-mm gaussian postprocessing filter.
Image-Derived Input Functions
Because labeling with 68Ga-DOTATOC/DOTATATE is stable during the duration of the PET examination, the total radioactivity concentration in the arterial plasma was used as an input function (6). Circular regions of interest with a diameter of 1 cm were drawn over the descending aorta in 10 consecutive image planes in the time frame in which the first passage of the bolus was best visualized (typically frame 1–10). These regions of interest were then combined to form a single aortic VOI. The resulting aortic VOI was projected onto all time frames in the dynamic examination to produce an arterial time–activity curve. The image-derived input functions were calculated by multiplying the arterial time–activity curve with the mean plasma–to–whole blood ratio in venous blood (29,30).
VOI-Based Kinetic Analysis
Fifty percent isocontour tumor VOIs were drawn in the 20- to 45-min summation image of the dynamic data and were projected onto all time frames to generate tumor time–activity curves, using the NEDPAS software developed at VU University Medical Centre (Amsterdam) (31). The tumors were delineated similarly in the whole-body images, and the corresponding tumor SUVs were derived. To evaluate the tumor-to-liver contrast, a subsample of healthy liver was delineated in the whole-body images using a spheric 20-mL VOI.
It has previously been shown that the kinetics of 68Ga-DOTATOC/DOTATATE can be described by an irreversible 2-tissue-compartment model (32–36), which reflects internalization of the receptor–ligand complex. From this compartment model, the following differential equations can be defined: Eq. 1where C1(t) is the concentration of free tracer in tissue; CP(t) is the concentration in plasma; K1, k2, and k3 are rate constants; and:
Eq. 1where C1(t) is the concentration of free tracer in tissue; CP(t) is the concentration in plasma; K1, k2, and k3 are rate constants; and: Eq. 2where C2(t) is the concentration of tracer internalized into the tumor cell. The solution of this model, with the addition of a blood volume component, is given by the following equation:
Eq. 2where C2(t) is the concentration of tracer internalized into the tumor cell. The solution of this model, with the addition of a blood volume component, is given by the following equation: Eq. 3in which CPET(t) represents the measured concentration, VA the arterial blood volume, CA(t) the arterial blood concentration, and Ki the net uptake rate (37) defined as:
Eq. 3in which CPET(t) represents the measured concentration, VA the arterial blood volume, CA(t) the arterial blood concentration, and Ki the net uptake rate (37) defined as: Eq. 4By fitting Equation 3 to the measured PET data using nonlinear regression (NLR), Ki can be determined, which is assumed to reflect a combination of receptor density and the ability of the ligand to internalize in the tumors (6).
Eq. 4By fitting Equation 3 to the measured PET data using nonlinear regression (NLR), Ki can be determined, which is assumed to reflect a combination of receptor density and the ability of the ligand to internalize in the tumors (6).
Parametric Image Analysis
Parametric Ki images were generated first by a basis function method (BFM) implementation of the irreversible 2-tissue-compartment model (38,39) and second by application of the Patlak method (37,40) (t* = 15 min after injection) on the dynamic PET data 15–45 min after injection, using in-house–developed software in MATLAB. For the BFM implementation, 20 logarithmically spaced exponential clearance rates (α = k2 + k3) ranging between 0.1 and 0.8 min−1 were used in addition to an irreversible basis function to create a set of basis functions: Eq. 5The linear combination of the 3 terms in Equation 3, using BFi that resulted in the minimum sum of squared residuals, yielded K1-Ki, Ki, and VA for each voxel. Before parametric computations, a gaussian filter with a full width at half maximum of 5 mm was applied. Mean tumor Ki values were determined for 50% isocontour VOIs in the parametric images. Liver VOIs were drawn in the parametric Ki images (as described above for the whole-body images), and tumor-to-liver ratios were calculated.
Eq. 5The linear combination of the 3 terms in Equation 3, using BFi that resulted in the minimum sum of squared residuals, yielded K1-Ki, Ki, and VA for each voxel. Before parametric computations, a gaussian filter with a full width at half maximum of 5 mm was applied. Mean tumor Ki values were determined for 50% isocontour VOIs in the parametric images. Liver VOIs were drawn in the parametric Ki images (as described above for the whole-body images), and tumor-to-liver ratios were calculated.
Statistical Analysis
The agreement and correlation between the VOI-based and parametric-based Ki values were determined using Pearson correlation, Deming regression, and Bland–Altman analysis (Prism, version 6.04; GraphPad Software, Inc.).
RESULTS
VOI- and Parametric-Based Kinetic Analysis
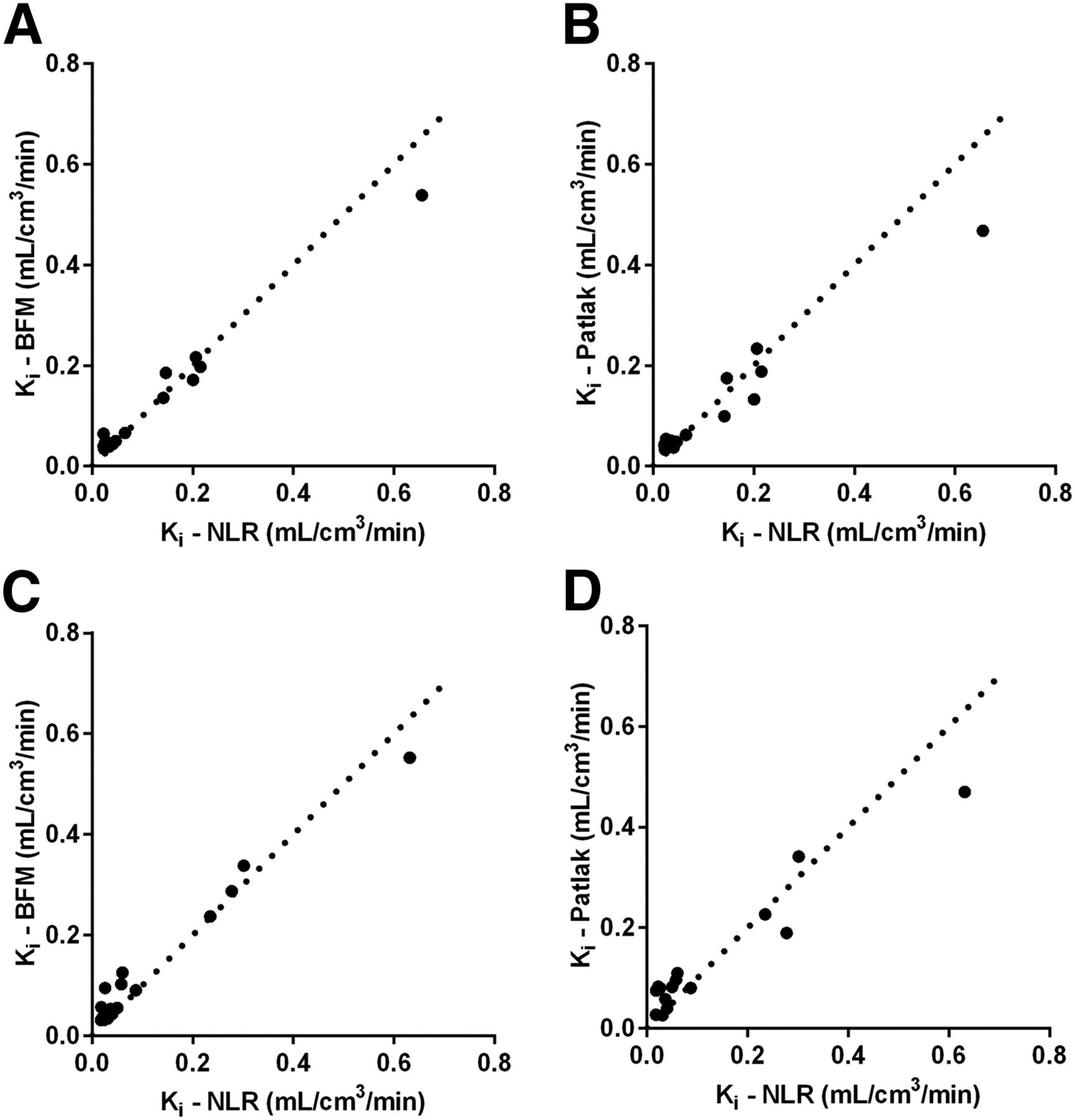
A linear relation was found between the VOI-based and parametric-based Ki values for both 68Ga-DOTATOC and 68Ga-DOTATATE. The relations between the VOI-based (NLR) and parametric-based (BFM and Patlak) Ki values for 68Ga-DOTATOC and 68Ga-DOTATATE are shown in Figure 1. Pearson correlation coefficients, Deming regression slope, and bias for the VOI- (NLR) and parametric-based (BFM and Patlak) Ki are listed in Table 1. For both tracers, the Pearson correlation coefficient was higher for BFM than for Patlak, the slope of regression line was higher for BFM than for Patlak (Table 1), and no significant bias was found for either parametric method or tracer.
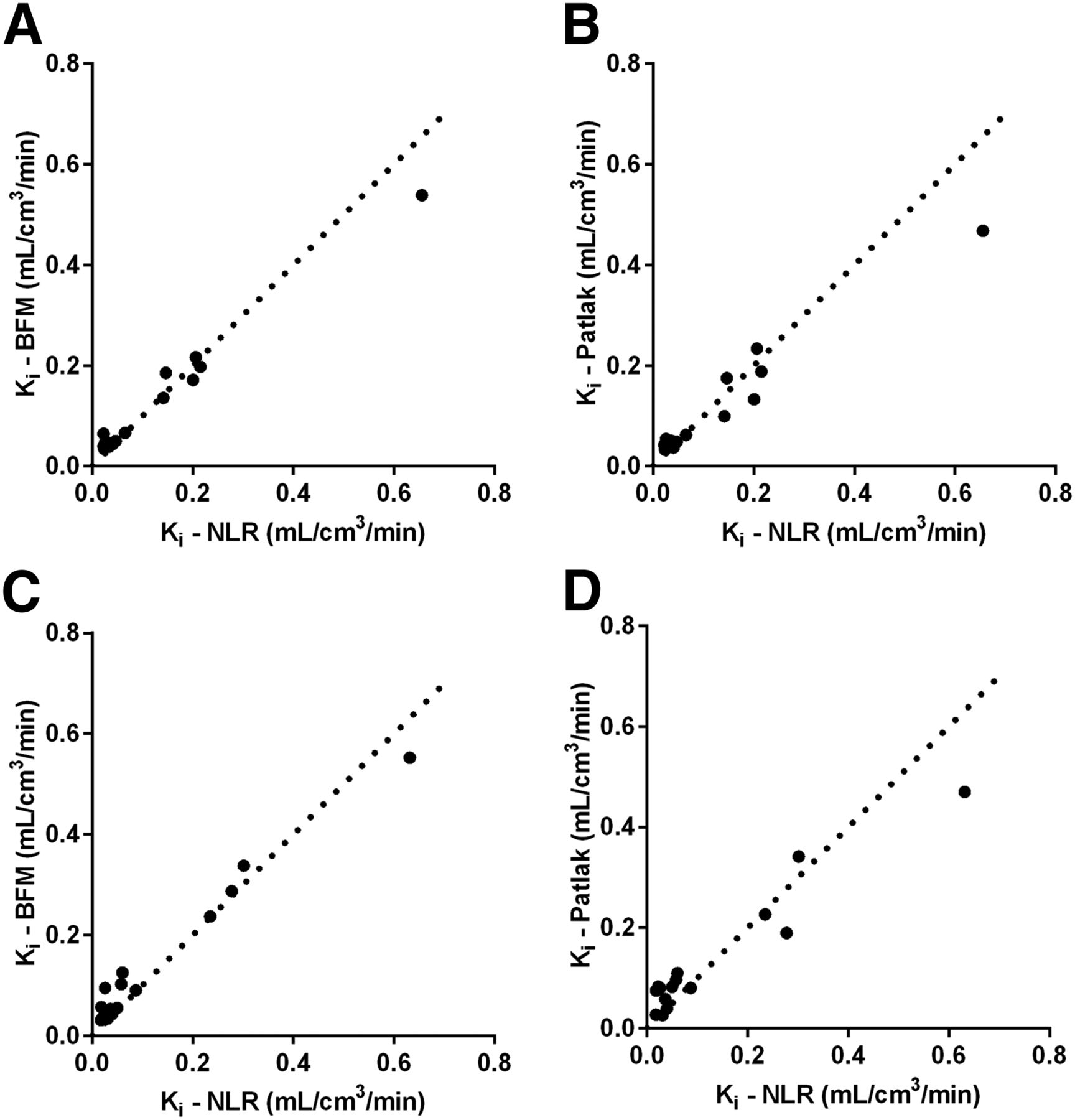
Correlation between NLR- and parametric-based (BFM and Patlak) Ki values for 68Ga-DOTATOC (A and B) and 68Ga-DOTATATE (C and D). Dashed lines represent lines of identity.
Pearson Correlation Coefficients (R2), Deming Regression Slope, and Bias Between Tumor VOI (NLR) and Parametric-Based (BFM and Patlak) Ki Values
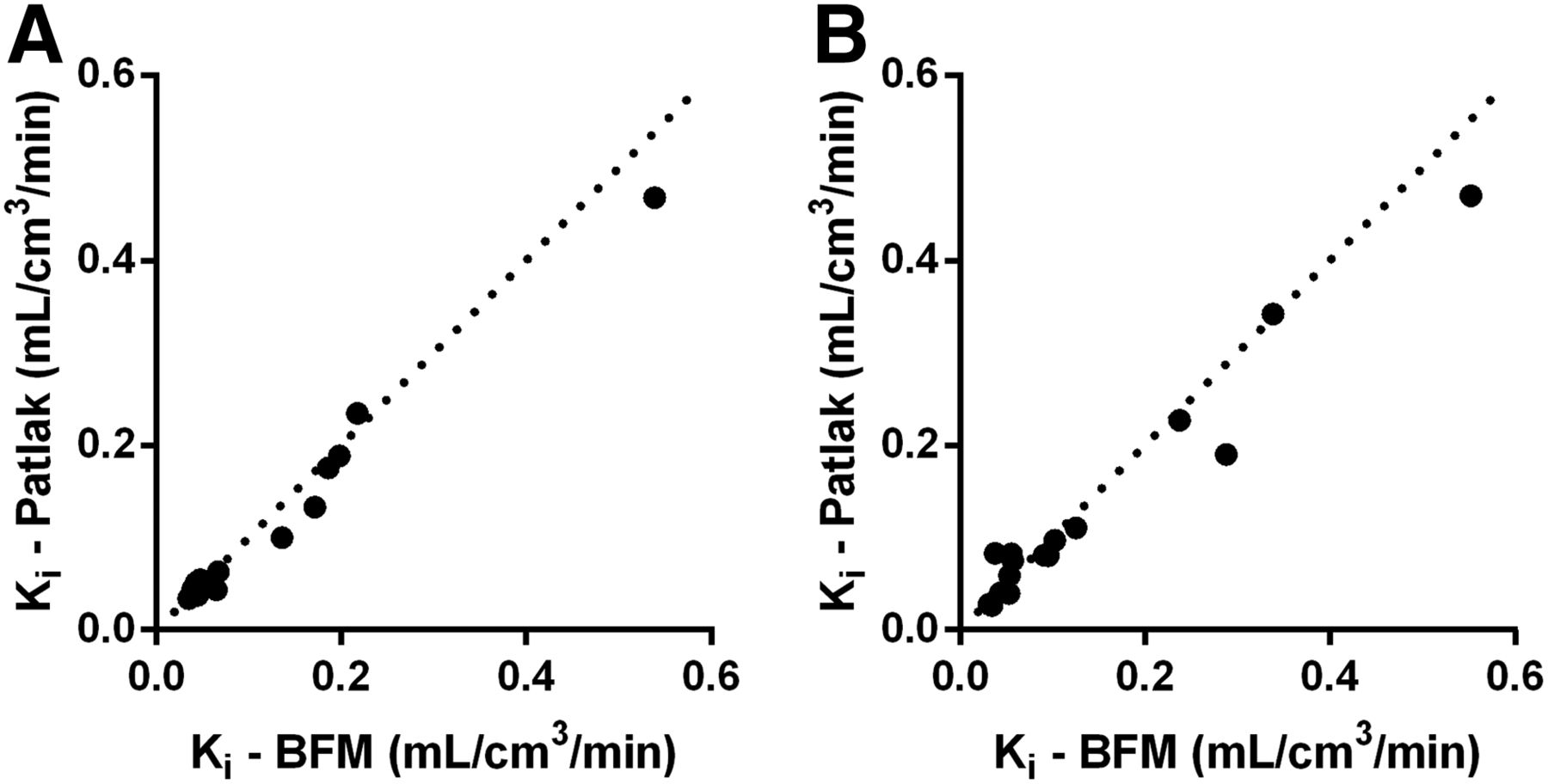
Parametric Ki values determined by BFM and Patlak for 68Ga-DOTATOC and 68Ga-DOTATATE are illustrated in Figures 2A and 2B, respectively. The Pearson correlation coefficient between BFM and Patlak Ki values was 0.99 for 68Ga-DOTATOC and 0.98 for 68Ga-DOTATATE. The Deming regression line slope between BFM and Patlak Ki values was 0.88 for 68Ga-DOTATOC and 0.85 for 68Ga-DOTATATE. The bias from the Bland–Altman plots was 0.01 (95% confidence interval, −0.05 to 0.03) and 0.01 (95% confidence interval, −0.08 to 0.06) for 68Ga-DOTATOC and 68Ga-DOTATATE, respectively.

Correlation between parametric Ki in tumor VOIs determined by BFM and Patlak analysis for 68Ga-DOTATOC (A) and 68Ga-DOTATATE (B). Dashed lines represent line of identity.
Tumor-to-Liver Contrast
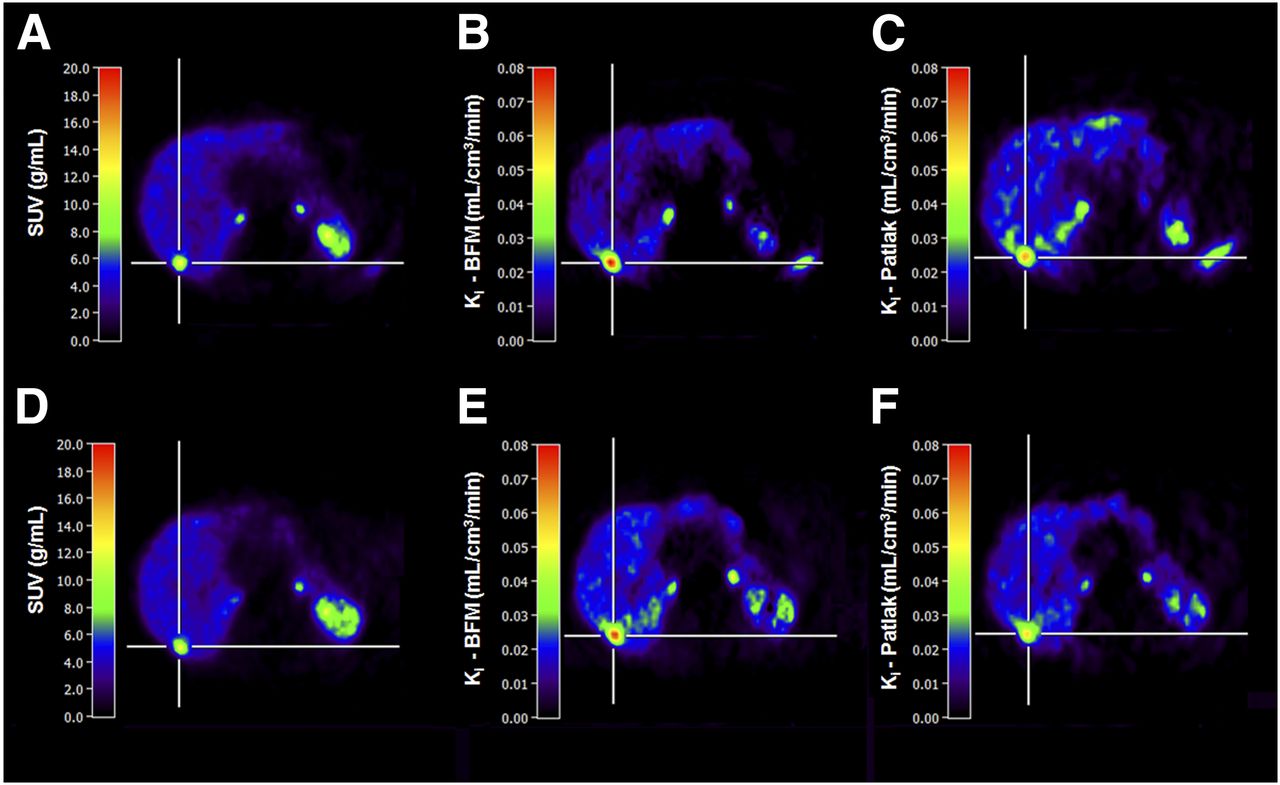
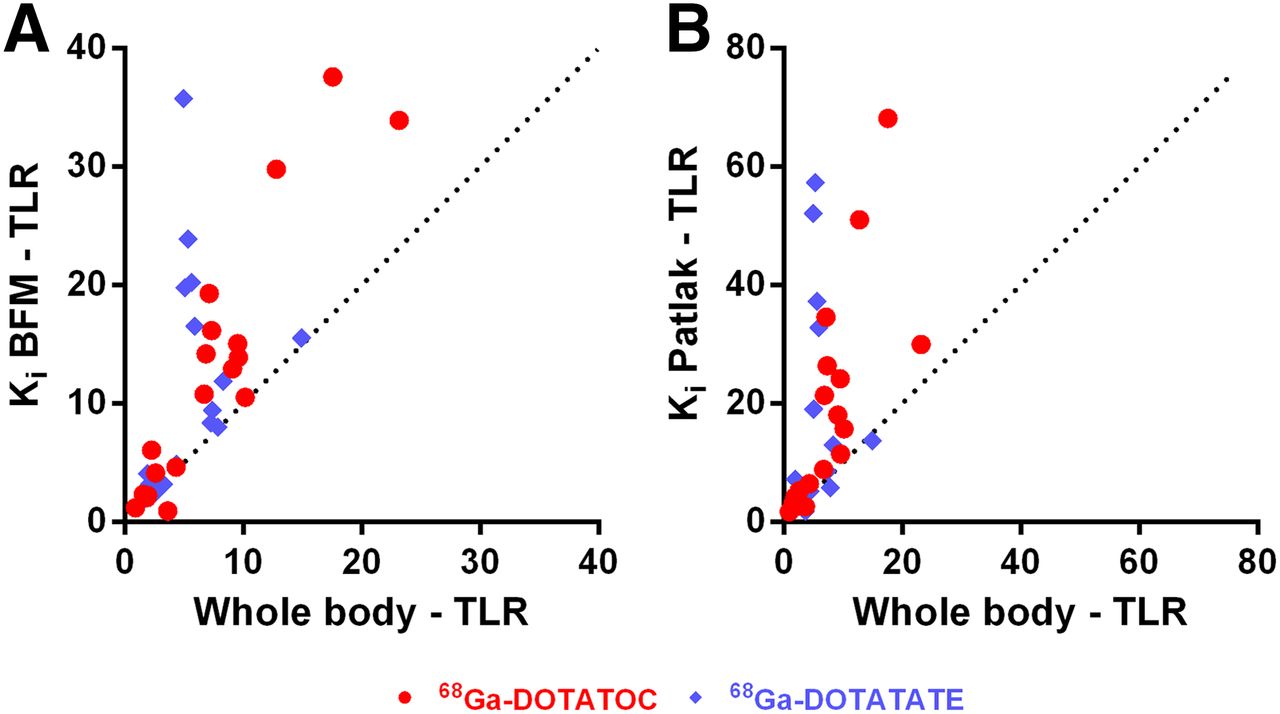
The image contrast visually improved in the parametric Ki images for both 68Ga-DOTATOC and 68Ga-DOTATATE (Fig. 3), and the tumor-to-liver ratio was generally higher in the parametric Ki images than in the whole-body images (Fig. 4). The tumor-to-liver ratio was 1.6 and 2.0 times higher in the parametric Ki images based on BFM than in the whole-body images for 68Ga-DOTATOC and 68Ga-DOTATATE (Fig. 4A), respectively. For the parametric Ki images based on the Patlak method, the tumor-to-liver ratio was 2.3 and 3.0 times higher than in the whole-body images for 68Ga-DOTATOC and 68Ga-DOTATATE (Fig. 4B), respectively. Generally, the image contrast was higher for 68Ga-DOTATATE than for 68Ga-DOTATOC (Fig. 4).

Representative transaxial images of liver obtained from static whole-body examination at 1 h after injection (A: 68Ga-DOTATOC; D: 68Ga-DOTATATE) and parametric Ki images based on BFM (B: 68Ga-DOTATOC; E: 68Ga-DOTATATE) and Patlak method (C: 68Ga-DOTATOC; F: 68Ga-DOTATATE), showing comparison of image contrast.

Tumor-to-liver ratio (TLR) for whole-body and parametric Ki images for BFM (A) and Patlak (B) both for 68Ga-DOTATOC and 68Ga-DOTATATE. Dashed lines represent lines of identity. Mean tumor to liver contrasts were 1.6 (A, red dot), 2.0 (A, blue diamond), 2.3 (B, red dot), and 3.0 (B, blue diamond) times higher in parametric Ki images than in whole-body images.
DISCUSSION
Early prediction of treatment response is essential to guide tumor therapy and avoid unnecessary side effects and costs from ineffective treatments. SUV has been proposed as a marker of SSTR density but changes of tumor SUV at 68Ga-DOTATOC PET/CT during PRRT have not been found to reliably correlate with the patient outcome (24,27,41–43). It was previously shown that Ki and SUV are not linearly correlated for NETs (especially for higher SUVs > 20–25), and the former may more adequately reflect the tumor SSTR density than SUV (6). However, in the present study, k3 was found to be much higher than k2 in patients with high Ki, indicating flow-limited delivery and an associated underestimation of both Ki and SUV, so this cannot explain the previously observed divergence between Ki and SUV. A more detailed analysis showed that the difference between SUV and Ki can rather be attributed to faster plasma clearance in patients with a high receptor burden, because the plasma radioactivity concentration at 45 min after injection in patients with high Ki values was considerably lower than in patients with low Ki values. This, in turn, would not affect the accuracy of Ki because plasma concentrations are considered when estimating Ki, but it does affect SUV because the absolute amount of tracer taken up into tissue is limited by the low plasma activity concentrations. Possibly, the total number of receptors in these patients is so high that nearly all peptide is cleared from the plasma during the scan, leading to the apparent saturation of SUVs.
The primary aim of this study was to develop a method to compute images that would incorporate the Ki parameter, allowing a more accurate determination of receptor density as well as a comparison of NLR- and parametric-based Ki values. Two sets of parametric Ki values were accordingly generated, and we presented a comparison between NLR-based and parametric-based Ki values for 68Ga-DOTATOC and 68Ga-DOTATATE. In a subset of 10 patients with 16 tumors, high correlation and agreement were found between the VOI- and parametric-based Ki values (Fig. 1), and no significant bias was found for the 2 methods, neither for 68Ga-DOTATOC nor for 68Ga-DOTATATE. Consequently, BFM and Patlak methods for computation of parametric images performed equally well and produced similar Ki values for both 68Ga-DOTATOC and 68Ga-DOTATATE. The agreement and correlation between the 2 parametric methods (BFM and Patlak) were also tested, and both methods were found to generate similar Ki values. However, parametric images appeared to show a considerable overestimation for low Ki values and a slight underestimation for high Ki values compared with NLR (Supplemental Figs. 1 and 2; supplemental materials are available at http://jnm.snmjournals.org). A possible explanation for this is that for low tumor uptake, the time–activity curves obtained from the 50% VOI in the dynamic images are a combination of the actual tumor uptake and spill-in from surrounding tissue. Because Ki in the surrounding liver tissue is much lower than in tumor tissue, VOI-based analysis using NLR will probably underestimate tumor Ki values. Because the liver background in the parametric images is much lower, the Ki values derived from the parametric images will to a much larger extent represent the actual tumor Ki and thus will be higher than the NLR values. In addition, VOIs were drawn independently in parametric and whole-body images. However, using the same VOIs in the dynamic and parametric images did not alter the conclusion—that is, parametric Ki values remained higher than NLR-based Ki values.
Many NET patients develop liver metastases but, because of the moderately high physiologic liver uptake of 68Ga-DOTATOC/DOTATATE, the detection of liver lesions may be jeopardized, especially when they are small. Also, this makes it challenging to evaluate therapy response because the physiologic liver background will affect the accuracy of the tumor uptake measurements. The tumor-to-liver ratios for whole-body SUV and parametric Ki images were therefore compared, and the latter were found to provide considerably better image contrast for both tracers (Figs. 3 and 4), although this was most apparent for 68Ga-DOTATATE. As previously shown (6), the uptake of 68Ga-DOTATOC/DOTATATE in both liver and tumors is more or less constant from 40 min after injection, with a possible small continuing increase for tumors. Therefore, using other uptake times for the SUV image in this comparison would not have affected contrast, but noise would increase for later time points. Consequently, the parametric Ki images can additionally be used to better visualize liver metastases. However, for its clinical implementation, automated methods for image-derived input function definition, such as previously presented, for example, for 15O-water myocardial blood flow imaging (44), need to be developed.
Because of the dynamic acquisition protocol required to generate the parametric Ki images, the whole abdomen or thorax may not be included for examination. The anatomic region that may be included for examination is therefore limited to the 15.5-cm axial field of view of the current PET/CT system, which reduces the clinical usefulness of the method. However, the recent generation of PET/CT and PET/MRI scanners, providing up to a 25-cm axial field of view, is a considerable improvement in this respect. Also, an alternative acquisition protocol may be applied to generate whole-body parametric Patlak Ki images, based on a short dynamic scan over the thorax followed by fast serial whole-body scanning. This alternative acquisition protocol will be the subject of future work.
CONCLUSION
Quantitatively accurate parametric Ki images, showing Ki of 68Ga-DOTATOC or 68Ga-DOTATATE at the voxel level, can be computed using the methods presented in the present work. In addition, the parametric methods reduced the signal from the liver for both tracers, providing better tumor-to-liver contrast in the parametric Ki images than in whole-body images. Further methodologic developments are necessary for clinical implementation of parametric Ki images to be feasible.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We express our gratitude to Mimmi Lindholm, Annie Bjurebäck, Maj Wiberg, Lars Lindsjö, and Marie Åhlman for their assistance in the PET/CT examinations.
Footnotes
Published online Oct. 27, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 29, 2016.
- Accepted for publication October 4, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantitative Assessments of Tumor Activity in a General Oncologic PET/CT Population: Which Metric Minimizes Tracer Uptake Time Dependence?
- In Vivo Instability of 177Lu-DOTATATE During Peptide Receptor Radionuclide Therapy
- Tumor-to-Blood Ratio for Assessment of Somatostatin Receptor Density in Neuroendocrine Tumors Using 68Ga-DOTATOC and 68Ga-DOTATATE