


Abstract
We aimed to evaluate 68Ga-DOTATATE PET/CT for the early prediction of time to progression and clinical outcome after a first cycle of peptide receptor radionuclide treatment (PRRT) in a cohort of patients with well-differentiated neuroendocrine tumors. Methods: Thirty-three consecutive patients (22 men and 11 women; mean age ± SD, 57.8 ± 12.1 y) were investigated at baseline and again 3 mo after initiation of the first cycle of PRRT. 68Ga-DOTATATE receptor expression was assessed using 2 measures of standardized uptake value (SUV): maximum SUV (SUVmax) and tumor-to-spleen SUV ratio (SUVT/S). Percentage change in SUV scores after PRRT relative to baseline (ΔSUV) was calculated. After completing 1–3 cycles of PRRT, patients entered the follow-up study, for estimation of time to progression. According to the Response Evaluation Criteria in Solid Tumors, progression was defined on the basis of contrast-enhanced CT. Clinical symptoms, as well as the tumor markers chromogranin A and neuron-specific enolase, were also recorded during regular follow-up visits. Results: The 23 of 31 patients with decreased SUVT/S after the first PRRT cycle had longer progression-free survival than did the 8 of 31 patients with stable or increased scores (median survival not reached vs. 6 mo, P = 0.002). For the 18 of 33 patients showing a reduction in SUVmax, there was no significant difference in progression-free survival (median survival not reached vs. 14 mo, P = 0.22). Multivariate regression analysis identified SUVT/S as the only independent predictor for tumor progression during follow-up. In the 17 of 33 patients with clinical symptoms before PRRT, ΔSUVT/S correlated with clinical improvement (r = 0.52, P < 0.05), whereas ΔSUVmax did not (r = 0.42, P = 0.10). Changes in the tumor markers (chromogranin A and neuron-specific enolase) did not predict ΔSUV scores, clinical improvement, or time to progression. Conclusion: Decreased 68Ga-DOTATATE uptake in tumors after the first cycle of PRRT predicted time to progression and correlated with an improvement in clinical symptoms among patients with well-differentiated neuroendocrine tumors; ΔSUVT/S was superior to ΔSUVmax for prediction of outcome.
In general, the medical treatment options for well-differentiated neuroendocrine tumors (NETs) are limited. Encouraging results have been reported for peptide receptor radionuclide treatment (PRRT) with somatostatin analogs targeting the somatostatin receptors, which are highly expressed in some NET lines (1–4). However, a study considering morphologic criteria for the identification of tumor response reported similar survival rates between NET patients with stable disease or minimal treatment response to PRRT and NET patients exhibiting a partial response (3). Other studies showed that despite a clear improvement in symptoms for most patients treated with PRRT, only a small percentage showed a significant decline in tumor size as measured by CT (1,5). Furthermore, improved quality of life after PRRT was not clearly associated with a discernible morphologic response to therapy (4). These mostly negative findings highlight the need for imaging methods of superior sensitivity for monitoring the response to treatment among NET patients.
PET with 18F-FDG has become established as an indispensable tool for diagnostics and as a surrogate marker in therapy-monitoring studies of various tumor types, such as malignant lymphoma (6) and diverse solid tumors (7–12). In such studies, 18F-FDG PET surpassed CT for assessing the response of gastrointestinal stromal tumors to treatment with tyrosine kinase inhibitors (13,14). In the course of such treatment, the 18F-FDG uptake decreased in these tumors, even though the tumor size remained constant for an extended period (15). However, the treatment response of NET is notoriously difficult to assess by imaging; these tumors are characterized mostly by a low metabolic activity, preventing their detection with 18F-FDG PET (16). However, the characteristically high levels of somatostatin receptor expression present an alternate approach for molecular imaging of NETs. A recent PET study has indicated sensitive detection of NETs with somatostatin analogs such as 68Ga-DOTATATE (17). These radiolabeled somatostatin analogs have shown a high uptake in NETs and organs such as the spleen (18).
Detection of NET therapy response is likewise difficult; the monitoring of functional parameters may be more reliable than morphologic measurements for assessing therapy response of NETs, as is the case for gastrointestinal stromal tumors. Indeed, Gopinath et al. showed that SPECT with the somatostatin analog 111In-pentetreotide was superior to CT for predicting the clinical outcome of patients with NETs (19). However, there have been no studies assessing the value of PET with 68Ga-DOTATATE for predicting therapy response of NETs. Therefore, we aimed in the present study to determine the capabilities of PET with 68Ga-DOTATATE for early prediction of clinical outcome and progression-free survival after the first cycle of PRRT in NET patients. To this end, we evaluated 2 measures of standardized uptake value (SUV)—maximum SUV (SUVmax) and tumor-to-spleen SUV ratio (SUVT/S)—as quantitative values for predicting time to progression (TTP) and clinical improvement in a series of 33 patients undergoing PRRT. We also compared the SUVs to the blood assays of the NET markers chromogranin A and neuron-specific enolase (NSE).
MATERIALS AND METHODS
Study Population
Thirty-three consecutive patients (22 men, 11 women; mean age ± SD, 57.8 ± 12.1 y; range, 20–72 y) with histologically proven, well-differentiated metastatic NET were included. The patients were treated with 1, 2, or 3 cycles of PRRT: either 3,700 MBq of 90Y-DOTATATE (n = 24), 7,400 MBq of 177Lu-DOTATATE (n = 7), or both (n = 2). Patients not eligible for PRRT were excluded. Patients’ clinical data are presented in Table 1. All patients underwent 68Ga-DOTATATE PET/CT before the radiotherapy and again at 3 mo after the first cycle of therapy. The median interval between pretherapeutic PET/CT and therapy was 7 ± 3.5 wk, and the median interval between the first cycle of therapy and posttherapeutic PET/CT was 13 ± 2.3 wk. Eight of 33 patients were pharmaceutically treated with long-acting somatostatin analogs during both the pre- and the posttherapeutic 68Ga-DOTATATE PET/CT (Table 2). Written informed consent was obtained from all patients before the PET examinations. Routine hematologic, liver, and kidney function tests were performed before each therapy, as well as during follow-up visits.
Patient Characteristics
Clinical Data and SUVs of Study Population
PET Scans
68Ga-DOTATATE was prepared as described previously (20). Whole-body PET scans were acquired in 3-dimensional mode (3 min per bed position) using a Gemini PET/CT scanner (Philips) or a Biograph 64 TruePoint PET/CT scanner (Siemens Medical Solutions). In all patients the pre- and posttherapeutic PET scans were performed with the same PET scanner. To validate the comparison between the SUVs obtained with the 2 different scanners, we performed multiple phantom measurements and defined a suitable correction factor for objects of different sizes on both scanners. The emission sequence was initiated at 60 min after intravenous injection of 200 MBq of 68Ga-DOTATATE, similar to the protocol in other studies using 68Ga-labeled somatostatin analogs (17,21,22). Emission data were reconstructed with attenuation correction based on low-dose CT (20 mA, 140 kV, 512 × 512 matrix). All scans were performed in combination with a diagnostic CT scan (100–190 mAs, depending on the region of the scanned organ; 120 kV; 2 × 5 mm collimation; pitch of 1.5) of the head, thorax, abdomen, and pelvis after a 2.5 mL/s intravenous injection of 120 mL of iodine-containing contrast agent (iopromide [Ultravist 300; Schering]). Initiation of this scan was delayed by 50 s in order to depict the venous contrast-medium phase.
Image Evaluation
Two nuclear medicine specialists working side by side in consensus evaluated the PET images using a dedicated software package (Hybrid Viewer; Hermes Medical Solutions). CT data were used for allocation of regions with increased uptake of the radiopharmaceutical to specific morphologic structures. Neither reader was aware of patients’ clinical or follow-up data. The peak SUV (SUVmax) corrected for body weight was calculated by automatically drawing—around tumors seen on the coregistered axial CT images—a region of interest having a threshold of 50% of the SUVmax. We also calculated the SUV of the tumors relative to the maximal splenic uptake by dividing the SUVmax of the tumors by the SUVmax of the spleen (SUVT/S) (Fig. 1). The SUVmax of the spleen was likewise calculated by drawing a splenic volume of interest having a threshold of 50% of the respective SUVmax. To evaluate the response to therapy, we calculated the percentage changes in ΔSUVmax and ΔSUVT/S relative to the corresponding baseline measurements of up to 3 tumors in 4 organs (liver, lung, lymph nodes, and bone), as well as the primary tumor. Any decrease in SUVmax and SUVT/S after the first cycle of therapy was considered a positive response to therapy. Furthermore, we evaluated the SUVmax of the most prominent lesion for each patient.

Coronal (A), sagittal (B), and axial (C) 68Ga-DOTATATE PET slices showing measurement of splenic SUVmax by drawing volume of interest with fixed 50% threshold of SUVmax. Inspection of coregistered CT images allows one to exclude the possibility that nonsplenic tissue has intruded into volume of interest.
TTP and Clinical Response Evaluation
Patients entered follow-up after completion of the PRRT (1, 2, or 3 cycles). For assessment of TTP, PET/CT follow-up examinations were performed at 3-mo intervals after therapy. A radiologist with 5 y of experience, who had not seen the PET scans or the patients’ clinical history, reviewed the contrast-enhanced CT images. For CT evaluation, the unidimensional measurement of the longest axis (or, in lymph nodes, the shortest diameter) was noted in order to assess progression of the primary tumor or the metastases. Every new metastasis noted, and any increase in tumor size of more than 20%, was considered progression, according to the Response Evaluation Criteria in Solid Tumors (23,24). Cystic liver metastases were excluded, according to the recommendations of the International Cancer Imaging Society (25).
For clinical outcome analysis, patients were asked to report tumor-related symptoms experienced during their inpatient stay immediately before PRRT and at 3 mo after completing PRRT. Any quantitative or qualitative improvement of these symptoms in the course of therapy was noted. We considered only those symptoms clearly related to hormone-secreting NETs, such as flush or diarrhea.
Tumor Marker
Venous blood samples were drawn within 3 d of the PET/CT study and were stored for subsequent analysis to measure plasma levels of the tumor markers chromogranin A and NSE. Chromogranin A was measured with a solid-phase 2-site immunoradiometric assay purchased from CISbio, and NSE was measured with an electrochemiluminescence immunoassay (Elecsys; Roche). The normal physiologic ranges are less than 98 ng/mL for chromogranin A and less than 16.3 ng/mL for NSE. Of 33 patients, 23 exhibited elevated chromogranin A values and 24 exhibited elevated NSE values. For these patients, the percentage change after therapy was calculated. A decrease of more than 50% or within the reference range was considered a therapy response.
Statistical Analysis
Statistical analyses were performed using the SPSS software package (version 15.0). The Kolmogorov–Smirnov test was performed to prove a gaussian distribution of the values. Pearson correlation coefficients were calculated for the correlations between the different SUV scores. The Kendall τ-test was used to measure the correlation between changes in these scores and clinical improvement. An uncorrected P value of less than 0.05 was assumed to be statistically significant. The t test was used to compare differences in SUV scores of the spleen and to compare the SUV scores of clinical responders. In addition, a receiver-operating-characteristic analysis was used to define a threshold of SUV changes predicting clinical outcome. The TTP of the different groups was compared by Kaplan–Meier analysis with log-rank test. The uni- and multivariate Cox proportional hazards model was used to estimate hazard ratios and 95% confidence intervals for number of PRRT cycles, SUVmax, ΔSUVmax, and ΔSUVT/S. For SUVT/S evaluation, 2 patients (patients 30 and 31) with a history of splenectomy were excluded. Quantitative data are presented as mean ± SD.
RESULTS
Tumor SUVmax ranged from 6.7 to 82.7 (mean, 28.5 ± 15.5) before PRRT and from 7.4 to 43.7 (mean, 22.9 ± 9.4) after PRRT. Summed SUVmax ranged from 22.9 to 314.9 (mean, 91.4 ± 58.2) before PRRT and from 25.9 to 147.9 (mean, 74.4 ± 34.5) after PRRT. Summed SUVT/S ranged from 1.21 to 18.54 (mean, 5.01 ± 3.4) before PRRT and from 1.02 to 10.48 (mean, 4.18 ± 2.5) after PRRT.
Splenic SUVmax ranged from 5.0 to 35.5 (mean, 18.4 ± 7.7). Mean splenic SUVmax was lower before therapy (range, 5.0–35.0; mean, 17.3 ± 7.4) than after therapy (range, 7.2–35.5; mean, 19.6 ± 8.0) (P = 0.05); individual pre- and posttherapeutic SUVmax correlated (r = 0.62; P < 0.001), and SUVmax correlated with SUVT/S (r = 0.64, P < 0.001).
TTP
Median follow-up time was 22.3 ± 5.1 mo (range, 13–34 mo). Fifteen patients showed disease progression, with a median TTP of 10.0 ± 4.4 mo (range, 3–16 mo). There was no significant difference in TTP between patients treated pharmacologically and those without such treatment (P = 0.70; log rank test). The 23 patients with decreasing SUVT/S after therapy had significantly longer TTP than did those without an SUVT/S decrease (median TTP not reached vs. 6 mo, P = 0.002) (Figs. 2 and 3). Differences in progression-free survival were also significant when the comparison was only between patients with (P < 0.05) and without (P < 0.05) octreotide treatment. Differences in TTP as predicted by ΔSUVmax were not significant (median TTP not reached vs. 14 mo, P = 0.22). According to the Cox proportional hazards model, we identified the ΔSUVT/S as the only predictor of TTP in both univariate (P = 0.006) and multivariate analyses (P = 0.03; Table 3). Additionally, the SUVmax was identified as a predictor of TTP in univariate analysis only (P = 0.04).

Pretherapeutic axial PET (A) and CT (B) slices, compared with posttherapeutic PET (C) and CT (D) slices, showing abdominal lymph node metastasis (arrow) of patient 6. Both SUVmax (−55%) and SUVT/S (−60%) decreased markedly after PRRT. This patient has been progression-free for 28 mo.

Kaplan–Meier progression-free survival curves as functions of ΔSUVT/S (P = 0.002) (left) and ΔSUVmax (P = 0.22) (right). P values were calculated with log-rank test.
Analysis of SUVs as Predictors of TTP
Clinical Outcome
Seventeen of 33 patients showed clinical symptoms of metastatic NET, notably flush or diarrhea. Among these 17 symptomatic patients, clinical improvement showed a slightly higher correlation with ΔSUVT/S (r = 0.52, P < 0.05) than with ΔSUVmax (r = 0.42, P = 0.10). Patients showing clinical improvement exhibited a significant decrease in SUVT/S (33% ± 32%; range, −82% to 17%; P = 0.02), with a concomitant significant decrease in SUVmax (19% ± 34%; range, −68% to 33%; P = 0.02) (Fig. 4). Patients without clinical improvement showed an 8% ± 25% increase (range, −21% to 54%) in SUVT/S, whereas SUVmax increased by 22% ± 21% (range, −6% to 47%). According to the receiver-operating-characteristic analysis, a ΔSUVmax threshold of −4% predicted an improvement in clinical symptoms with 75% sensitivity and 100% specificity, whereas a ΔSUVT/S threshold of −19% also had 75% sensitivity but only 87.5% specificity.
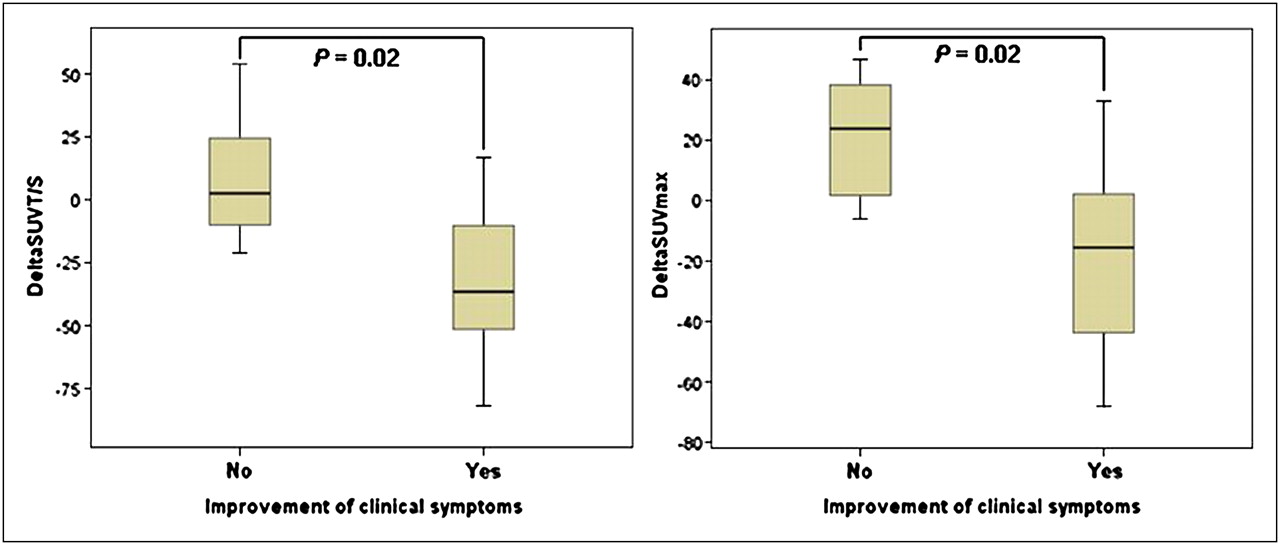
Distribution of ΔSUVT/S (P = 0.02) (A) and ΔSUVmax (P = 0.02) (B) of patients with reference to clinical improvement after PRRT. Boxes represent second and third quartiles. Bar within each box refers to mean value, and bars above and below each box indicate range.
Tumor Markers
There was no significant correlation between change in chromogranin A and either ΔSUVmax (r = 0.02, P = 0.93) or ΔSUVT/S (r = 0.12, P = 0.60), nor did the change in NSE levels significantly correlate (r = 0.31, P = 0.17, and r = 0.34, P = 0.15, respectively).
DISCUSSION
Early prediction of therapy response in tumors is essential to guide therapy and avoid the side effects and costs incurred by ineffective therapies. There is a particular need for a sensitive molecular imaging marker for patients with NET, because CT-based assessment of therapy response does not correlate well with progression-free survival, clinical outcome, or quality of life (3,4,19). Although the utility of 18F-FDG PET in assessing therapy response for many other tumors (6,7,9,10,26,27) does not generalize to NET, we anticipated that 68Ga-DOTATATE PET would target a specific NET marker, overexpression of somatostatin receptor.
To our knowledge, this was the first study evaluating 68Ga-DOTATATE PET/CT in the prediction of progression-free survival and clinical outcome in patients after PRRT. Patients with a decline in SUVT/S after finishing the first cycle of PRRT had a significant longer TTP than did patients without favorable SUVT/S changes, suggesting that this parameter has a potential role for the early prediction of outcome in patients with well-differentiated NET. Interestingly, ΔSUVmax did not emerge as a significant predictor of TTP, either through Kaplan–Meier statistics or the Cox regression hazard model. That finding is in line with recently published results by Gabriel et al. (28), who similarly found that the ΔSUVmax for 68Ga-DOTATOC PET was not useful for assessing therapy response in a series of 46 NET patients. Their ΔSUVmax fluctuated randomly after 2–7 cycles of PRRT. However, there was in our study a (not statistically significant) trend toward a longer TTP with decreasing SUVmax. A longer follow-up time might potentially have increased the level of significance also for SUVmax. In general, the validity of this method of calculating SUVmax is not clearly established for PET studies with 68Ga-DOTATATE or other somatostatin receptor ligands. Particularly in the context of PRRT, several cycles of which usually impairs renal function (29), SUVmax might be spuriously influenced by a therapy-related alteration of plasma tracer clearance, occurring independently of tumor progression. Furthermore, as there is almost no uptake of 68Ga-DOTATATE in the body except in tumors, the spleen, and a few other organs, a large percentage of the injected dose tends to concentrate in these tissues. If the treatment is successful in reducing uptake of tracer specifically in the tumor, more tracer will be available for physiologic uptake in the unaffected spleen and other organs. Under this circumstance, the calculation of SUV normalized to the injected dose and body weight is not exactly equivalent to normalizing to the dose available to any specific tumor or organ. Because of this potential confounding of estimates based on maximal uptake, we additionally defined a tumor-to-spleen ratio (SUVT/S), which proved to have only a moderate correlation with individual estimates of SUVmax, suggesting a certain pharmacodynamic invariance of our reference tissue index.
Despite the favorable properties of ΔSUVT/S for the prediction of TTP and clinical outcome, the possibility must be considered that this quantitative parameter was itself influenced by PRRT. Besides potential effects of PRRT on the expression and density of somatostatin receptors on the surface of the NET cells, we noted in the present study that PRRT increased 68Ga-DOTATATE uptake by the spleen. Partly because of this alteration, the number of responders was higher for ΔSUVT/S than for ΔSUVmax. Nonetheless, ΔSUVT/S proved to be superior to ΔSUVmax in predicting TTP and clinical outcome. We speculate that SUVmax might be corrected for the effects of PRRT on renal clearance of tracer by normalizing to the SUVmax of the spleen, resulting in greater prognostic value. Furthermore, decreased 68Ga-DOTATATE uptake in tumors could theoretically reflect dedifferentiation of NET cells, given that somatostatin receptor expression depends on the grade of differentiation of NET (30). In this scenario, rapid tumor growth could have led to shortened TTP. For early detection of dedifferentiation, combination PET/CT instead of PET alone is highly recommended.
Interestingly, univariate regression analysis identified pretherapeutic SUVmax as an accurate predictor for TTP, perhaps insofar as high receptor density may predispose to an optimal response to PRRT. This finding is in line with a previously published study that reported a higher response rate to PRRT in 310 NET patients exhibiting a high uptake in conventional somatostatin scintigraphy (2). This correlation has not been proved for 68Ga-DOTATATE PET.
In addition to the prediction of progression, a second major endpoint of the present study was the improvement of clinical symptoms, which is a major goal of the predominantly palliative therapies in metastatic NET. We found that a decline in SUVT/S correlated significantly (and slightly better than the SUVmax) with the improvement of clinical symptoms. The value of 68Ga-DOTATATE PET for prediction of clinical improvement during follow-up is consistent with an earlier report of Gopinath et al., who found a close correlation between the change in functional volume of NET assessed with 111In-pentetreotide SPECT and the improvement of clinical symptoms (19). Furthermore, 111In-pentetreotide SPECT proved to be clearly superior to CT in that study. We expect that 68Ga-DOTATATE PET imparts advantages over 111In-pentetreotide SPECT because of the higher affinity of the PET ligand for the constitutively expressed SSRT type 2, and given the superior spatial resolution of PET. Although the 2 ligands have not yet been compared directly, our finding that decreased 68Ga-DOTATATE uptake predicts clinical improvement emphasizes the link between decrease in SUV and improvement in NET symptoms.
In an animal study, chromogranin A secretion correlated strongly with the reduction of tumor volume after PRRT (31), but we did not find any relationship between chromogranin A or NSE levels and patient outcome. It might well be that the 3-mo follow-up after PRRT was too brief an interval for detecting true responses by tumor markers, especially given that there may have been a paradoxic elevation (i.e., due to treatment-related secretion) in the early posttreatment reassessment. Basically, the plasma chromogranin A level had low specificity for predicting changes in tumor size among human gastrinoma patients and varied considerably from day to day (32). In several previous clinical studies, chromogranin A levels failed to correlate with the NET mass (33–38). In fact, chromogranin A levels have been shown to reflect hepatic tumor burden (39). Thus, the serum chromogranin A level seems generally unsuited for assessing palliative therapy response in well-differentiated NET.
Regarding study limitations, it might be argued that a single, uniform PRRT protocol should have been assessed. However, the aim of this study was to evaluate the ability of 68Ga-DOTATATE PET to predict progression, not to evaluate the merits of a particular treatment. Despite the different treatment protocols, the TTP found in our study is in line with other studies (3,40). Furthermore, we found no significant correlation between the number of PRRT cycles and TTP.
Treatment of part of our patient group with long-acting somatostatin analogs may constitute a limitation of this study, given that this treatment may conceivably influence SUVmax both in tumors and in the spleen. However, we are unaware of any formal demonstration of the conjectural effect of somatostatin analogs on the SUV of 68Ga-DOTATATE. In any event, our patients were medicated during both the pre- and the posttherapeutic PET scans. Therefore, assuming that the effects of those somatostatin analogs were uniform over time, scores should have been influenced in the same way, with no bias on ΔSUVT/S scores.
CONCLUSION
This study suggests that 68Ga-DOTATATE PET/CT may contribute usefully to the early prediction of TTP and to the prediction of treatment outcome in patients with well-differentiated NET undergoing PRRT. ΔSUVT/S proved superior to baseline SUVmax and ΔSUVmax for the prediction of treatment outcome.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 2, 2010.
- Accepted for publication June 3, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Full-Body Tumor Response Heterogeneity of Metastatic Neuroendocrine Tumor Patients Undergoing Peptide Receptor Radiopharmaceutical Therapy
- Prediction of 177Lu-DOTATATE PRRT Outcome Using Multimodality Imaging in Patients with Gastroenteropancreatic Neuroendocrine Tumors: Results from a Prospective Phase II LUMEN Study
- 225Ac-MACROPATATE: A Novel {alpha}-Particle Peptide Receptor Radionuclide Therapy for Neuroendocrine Tumors
- Quantitative 68Ga-DOTATATE PET/CT Parameters for the Prediction of Therapy Response in Patients with Progressive Metastatic Neuroendocrine Tumors Treated with 177Lu-DOTATATE
- Somatostatin Receptor Imaging and Theranostics: Current Practice and Future Prospects
- Prognostic Value of 18F-FDG PET/CT in a Large Cohort of Patients with Advanced Metastatic Neuroendocrine Neoplasms Treated with Peptide Receptor Radionuclide Therapy
- Inflammation-Based Index and 68Ga-DOTATOC PET-Derived Uptake and Volumetric Parameters Predict Outcome in Neuroendocrine Tumor Patients Treated with 90Y-DOTATOC
- Safety, tolerability and clinical implementation of 'ready-to-use 68gallium-DOTA0-Tyr3-octreotide (68Ga-DOTATOC) (SomaKIT TOC) for injection in patients diagnosed with gastroenteropancreatic neuroendocrine tumours (GEP-NETs)
- Tumor-to-Blood Ratio for Assessment of Somatostatin Receptor Density in Neuroendocrine Tumors Using 68Ga-DOTATOC and 68Ga-DOTATATE
- A Prospective Observational Study to Evaluate the Effects of Long-Acting Somatostatin Analogs on 68Ga-DOTATATE Uptake in Patients with Neuroendocrine Tumors
- Twelve-Year Follow-up After Peptide Receptor Radionuclide Therapy
- SSTR-RADS Version 1.0 as a Reporting System for SSTR PET Imaging and Selection of Potential PRRT Candidates: A Proposed Standardization Framework
- Somatostatin Receptor 2-Targeting Compounds
- Parametric Net Influx Rate Images of 68Ga-DOTATOC and 68Ga-DOTATATE: Quantitative Accuracy and Improved Image Contrast
- 68Ga-DOTATATE PET/CT Interobserver Agreement for Neuroendocrine Tumor Assessment: Results of a Prospective Study on 50 Patients
- Predictors of Response to Radioligand Therapy of Metastatic Castrate-Resistant Prostate Cancer with 177Lu-PSMA-617
- Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors: Current Status and Future Directions
- A Delphic consensus assessment: imaging and biomarkers in gastroenteropancreatic neuroendocrine tumor disease management
- PET-Based Human Dosimetry of the Dimeric {alpha}v{beta}3 Integrin Ligand 68Ga-DOTA-E-[c(RGDfK)]2, a Potential Tracer for Imaging Tumor Angiogenesis
- The Impact of 68Ga-DOTATATE PET/CT Imaging on Management of Patients with Neuroendocrine Tumors: Experience from a National Referral Center in the United Kingdom
- Evaluating digestive neuroendocrine tumor progression and therapeutic responses in the era of targeted therapies: state of the art
- Quantitative and Qualitative Intrapatient Comparison of 68Ga-DOTATOC and 68Ga-DOTATATE: Net Uptake Rate for Accurate Quantification
- The use of biomarkers in neuroendocrine tumours
- Measured Human Dosimetry of 68Ga-DOTATATE
- The Role of 68Ga-DOTATATE PET/CT in Suspected Neuroendocrine Tumors
- Treatment with Octreotide Does Not Reduce Tumor Uptake of 68Ga-DOTATATE as Measured by PET/CT in Patients with Neuroendocrine Tumors
- Nuclear medicine techniques for the imaging and treatment of neuroendocrine tumours
- 177Lu-DOTATATE Molecular Radiotherapy for Childhood Neuroblastoma
- Therapeutic strategies for advanced neuroendocrine carcinomas of jejunum/ileum and pancreatic origin
- Imaging of Bilateral Neck Paragangliomas with 68Ga-DOTATATE Positron-Emission Tomography/CT