


Visual Abstract

Abstract
Our objective was to predict the outcome of peptide receptor radionuclide therapy (PRRT) using multimodality imaging and tumor dosimetry on gastroenteropancreatic neuroendocrine tumor (GEP-NET) lesions and patients. Methods: This prospective study included patients with progressive GEP-NETs. Treatment consisted of 4 cycles of 7.4 GBq of 177Lu-DOTATATE. Imaging parameters were measured on 68Ga-DOTATATE PET/CT (SUVmax/mean, somatostatin receptor [SSTR] tumor volume [TV], total lesion SSTR expression, and tumor-to-blood and tumor-to-spleen ratios), 18F-FDG PET/CT (SUVmax/mean, metabolically active TV, and total lesion glycolysis), and diffusion-weighted MRI (apparent diffusion coefficient) in a maximum of 5 target lesions per patient at approximately 10 wk after each injection. Tumor dosimetry was performed using SPECT/CT at 3 time points for every cycle. Baseline imaging parameters, their relative changes after PRRT cycle 1 (C1), and the tumor-absorbed dose at C1 were correlated with lesion morphologic outcome. The average values of the imaging parameters and the minimal, maximal, and mean C1 tumor-absorbed dose in each patient were tested for association with progression-free survival (PFS) and best objective response (RECIST 1.1). Results: In the 37 patients, the median PFS was 28 mo. Eleven of the 37 (30%) achieved a partial response (RECIST 1.1). After a median follow-up of 57 mo, the median time to lesion progression had not been reached in 84 morphologically evaluable lesions, with only 12 (14%) progressing (size increase ≥ 20% from baseline). Patients receiving a minimal C1 dose of 35 Gy in all target lesions exhibited a significantly longer PFS (48.1 vs. 26.2 mo; hazard ratio, 0.37; 95% CI, 0.17–0.82; P = 0.02). Volumetric 68Ga-DOTATATE PET parameters correlated with lesion and patient outcome: patients with an SSTR TV decrease of more than 10% after C1 had a longer PFS (51.3 vs. 22.8 mo; hazard ratio, 0.35; 95% CI, 0.16–0.75; P = 0.003). There was no statistical evidence of an association between other dosimetric or imaging parameters and the lesion or patient outcome. Conclusion: Minimal tumor-absorbed dose at C1 is predictive of outcome in patients with GEP-NETs treated with PRRT, providing a basis for personalized dosimetry-guided treatment strategies. An SSTR TV decrease after C1 could be used for early therapy response assessment as a predictor of PRRT outcome.
Neuroendocrine neoplasms represent a challenging clinical entity with marked heterogeneity in phenotype, prognosis, and evolution over time. Approximately 55%–70% of cases arise from gastroenteropancreatic structures (1). Neuroendocrine neoplasms can range from well-differentiated neuroendocrine tumors (NETs) to poorly differentiated neuroendocrine carcinomas (2). NET cells frequently have increased somatostatin receptor (SSTR) expression, predominantly of the somatostatin 2A subtype (3,4). This feature constitutes the basis for molecular imaging and therapy using SSTR-targeting radiopharmaceuticals. Peptide receptor radionuclide therapy (PRRT) with 90Y- and 177Lu-radiolabeled SSTR agonists (e.g., DOTATOC and DOTATATE) has been successfully used for more than 2 decades in NETs (5). The regulatory approval of 177Lu-DOTATATE PRRT followed the demonstration of significantly prolonged progression-free survival (PFS) compared with somatostatin analogs in patients with midgut NETs in the randomized phase 3 NETTER1 trial (6) and established a standard of care.
Maximizing the clinical benefit would require appropriate patient selection and adequate assessment of treatment response. In the last decade, PET/CT using 68Ga-radiolabeled SSTR agonists has almost completely replaced conventional SSTR scintigraphy as the fundamental step to assess SSTR status in vivo and evaluate the benefit likelihood for PRRT. Although PET/CT with 18F-FDG is generally reserved for imaging of high-grade NETs and neuroendocrine carcinomas (7,8), studies have shown that low-grade NETs can also be 18F-FDG–avid (9). Apart from assessing eligibility for PRRT, molecular imaging could potentially serve as a predictive biomarker of response to PRRT. Nevertheless, available data regarding the use of 68Ga-SSTR PET/CT to predict PRRT response are mainly retrospective and somewhat conflicting (10,11). Additionally, as the absorbed dose is fundamental to the antitumor effect of PRRT (12,13), dosimetry of the tumor lesions could be used for outcome prediction and treatment personalization.
We conducted a prospective study enrolling patients who had progressive gastroenteropancreatic NETs (GEP-NETs) and were eligible for treatment with 177Lu-DOTATATE PRRT. A series of multimodality imaging parameters derived from molecular imaging (i.e., 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT) and from diffusion-weighted MRI was followed after every treatment cycle. Tumor dosimetry after each injection was also performed. We aimed to assess the value of the pretreatment imaging parameters and their relative changes after PRRT cycle 1 (C1), as well as the tumor-absorbed dose in C1, in predicting lesion and patient outcome.
MATERIALS AND METHODS
Patients and Treatment
The LuMEn trial (NCT01842165) is a single-arm, prospective, phase II clinical-imaging study enrolling patients with advanced, histologically proven well-differentiated GEP-NETs, progressive within 12 mo before study inclusion. The complete list of patient selection criteria is available in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). All procedures performed in the study were in accordance with the Declaration of Helsinki. The study was approved by the Jules Bordet Institute Ethics Committee (CE2034), and written informed consent was obtained from all participants. Treatment consisted of 4 177Lu-DOTATATE injections of 7.4 GBq (±5%) each, administered intravenously 10–12 wk apart, with concomitant infusion of a nephroprotective amino acid solution and preceded by an antiemetic regime. 177Lu-DOTATATE was produced within the radiopharmacy facility of our nuclear medicine department as previously reported (14). All patients underwent baseline abdominopelvic MRI (or CT if MRI was contraindicated), 68Ga-DOTATATE PET/CT, and 18F-FDG PET/CT within 3 wk (± 1 wk) before the first PRRT injection. These imaging examinations were repeated approximately 10 wk after each 177Lu-DOTATATE injection. Detailed acquisition parameters are available in Supplemental Table 2. After the last PRRT cycle, patients were followed clinically and radiologically every 3 mo until disease progression according to RECIST 1.1 (15).
Image Analysis
On side-by-side evaluation of baseline MRI (or CT), 68Ga-DOTATATE PET/CT, and 18F-FDG PET/CT, a maximum of 5 target lesions was selected by a radiologist and nuclear medicine physician. Selection of a lesion required that it be unequivocally neoplastic, be RECIST 1.1-measurable, have uptake higher than physiologic liver uptake on 68Ga-DOTATATE PET/CT, and preferably be positive on 18F-FDG PET/CT (uptake above the threshold as defined below). The lesions had to represent the global tumor burden, ideally be spheric, and be outside any prior radiation fields of view. Confluent extensive lesions or lesions adjacent to each other on the 68Ga-DOTATATE PET/CT images were not included.
Tumors were delineated on 68Ga-DOTATATE PET/CT images using a gradient-based method (PETEdge tool in MIM Encore, version 6.9; MIM Software) to measure specific uptake (SUVmax, SUVmean, tumor-to-spleen ratio [tumor SUVmax/spleen SUVmean], tumor-to-blood ratio [tumor SUVmax/blood SUVmean]) and volumetric parameters (SSTR-expressing tumor volume [TV] and total lesion SSTR expression [SUVmean × SSTR TV]). Spleen parenchyma was delineated using a fixed threshold of 50% of maximum spleen uptake to calculate the spleen SUVmean, as previously defined by the group of Haug et al. (16). Blood SUVmean was measured in a 1-cm-diameter cylindric volume of interest in the center of the descending thoracic aorta. 18F-FDG–positive target lesions were delineated on 18F-FDG PET/CT images using a PERCIST-based threshold (17) to measure SUVmax, SUVmean, metabolically active TV, and total lesion glycolysis (SUVmean × metabolically active TV). The apparent diffusion coefficient (ADC) map of the MR images was used to obtain the ADC of the target lesions (automatically calculated by the MRI scanner). The mean ADC (mm2/s) was evaluated with a region of interest drawn inside the soft-tissue component of the lesion, avoiding necrosis or calcifications and without touching the borders. All parameters were measured for each lesion individually for the lesion-based analysis. The average values of the imaging parameters from the target lesions of one patient were used in a patient-based analysis.
For dosimetry purposes, SPECT/CT images were acquired 4, 24, and 168 h after each injection of 177Lu-DOTATATE. Target lesions were segmented on all 177Lu-DOTATATE SPECT/CT images using a region-growing tool (MIM Encore, version 6.9) to reach the same volume as the one obtained on the 68Ga-DOTATATE PET/CT images. Detailed data about the tumor dosimetry procedure are available in Supplemental Table 3. A conversion factor (previously assessed by our group (14)) was used to convert counts into activity concentrations, which were then corrected for partial-volume effect using a recovery coefficient curve obtained at our institute using a National Electrical Manufacturers Association phantom with infinite contrast. The mean activity inside tumors was converted into dose rate using the sphere model (OLINDA/EXM 1.1) (18). To calculate the absorbed dose, dose rate was time-integrated using the trapezoidal method up to 24 h, and monoexponential decay was derived from the last 2 time points.
Response Assessment
On a lesion level, morphologic progression was defined as a size increase of at least 20% from baseline. A size decrease of more than 30% from baseline was defined as a partial response, and the complete disappearance of a lesion (or size < 10 mm for lymph nodes) was defined as a complete response. Lesions showing neither a sufficient decrease nor a sufficient increase in size to qualify for progression or partial response were considered stable. For group comparisons, lesions with a complete or partial response were classified as responding lesions, whereas stable or progressive lesions were classified as nonresponding lesions. Morphologically evaluable lesions were those for which a response assessment after 4 PRRT cycles was available.
The patient-based response was assessed according to RECIST 1.1. Patients with a partial or complete response were classified as objective responders, whereas patients with stable or progressive disease were considered nonobjective responders.
Statistical Analysis
The primary endpoint of the study was lesion-based time to progression, calculated as the time between treatment initiation and the earliest documented lesion morphologic progression after completion of the treatment cycles. To get a power of 0.80 for a clinically relevant hazard ratio (HR) of 0.33, 37 progressive lesions needed to be documented. Differences in imaging parameters and tumor-absorbed dose between responding and nonresponding lesions were tested using the Wilcoxon signed-rank test. Correlations were analyzed using the Spearman correlation coefficient. PFS was defined as the time between treatment initiation and disease progression or death resulting from any cause. Kaplan–Meier survival curves and the Cox proportional-hazards regression model were used to compare PFS among different groups. The objective response rate was calculated as the proportion of subjects with a partial or complete response. Average values of the imaging parameters and the minimal, maximal, and mean tumor-absorbed dose per patient in C1 were tested for association with PFS and best objective response using the log-rank test. The optimal cutoff for a continuous explanatory variable was determined with the method of Contal and O’Quigley (19). A P value of less than 0.05 was considered statistically significant in all cases. Statistical analyses were performed using SAS 9.4 (SAS Institute Inc.) and Prism 7.04 (GraphPad Software).
RESULTS
Patients and Treatment Data
Between July 2013 and January 2020, 37 consecutive patients with advanced GEP-NETs were included in the study. Patient demographics and tumor characteristics are detailed in Table 1. Overall, 140 177Lu-DOTATATE cycles were administered, with a mean cumulated administered activity of 27.9 GBq (range, 7.5–36.9 GBq). Twenty-eight patients completed 4 cycles of PRRT, with a mean administered activity of 7.5 GBq (±0.2 GBq) per cycle. In the remaining 9 patients, different numbers of PRRT cycles were administered, the reasons for which are detailed in Supplemental Table 4. Safety analysis for the study cohort will be the subject of a separate publication.
Patients’ Demographics and Tumor Characteristics
Outcomes
At baseline, 116 target lesions were selected. Eighty-four were morphologically evaluable, of which 22 (26%) showed a partial response. They were mostly liver lesions (15/22), identified in 13 patients. There were no target lesions with a complete response. Fifty lesions (60%) were stable, and 12 (14%) progressed morphologically. The median follow-up time (data cutoff, July 2022) was 57 mo (95% CI, 50–71 mo), during which the median lesion-based time to progression was not reached. The objective response rate was 30% (11 patients with a partial response and no patients with a complete response), and the median PFS for the whole cohort was 28.1 mo. The association between PFS and potential prognostic factors is detailed in Supplemental Table 5. Patients with pancreatic primary NETs had a shorter PFS (median, 19.4 mo) than that of patients with intestinal NETs (29.5 mo) (P = 0.01; HR, 2.96; 95% CI, 1.25–7.02).
Imaging Parameters and Association with Lesion Outcome
68Ga-DOTATATE PET/CT
At baseline, 68Ga-DOTATATE PET/CT parameters were available for 110 of the 116 target lesions (6 excluded because of PET/CT artifacts) for SUVmax, SUVmean, tumor-to-blood ratio, SSTR TV, and total lesion SSTR expression and for 97 of the 116 target lesions for tumor-to-spleen ratio (additional 13 excluded because they were from 4 patients with prior splenectomy). Baseline SUVmax, SUVmean, tumor-to-blood ratio, SSTR TV, and total lesion SSTR expression were not associated with lesion morphologic outcome (Table 2). Baseline tumor-to-spleen ratio was significantly lower in the responding lesions than in the nonresponding ones (P = 0.03); however, the Spearman rank coefficient was not statistically significant, as detailed in Table 3.
Association Between Baseline 68Ga-DOTATATE PET/CT Parameters and Morphologic Lesion Outcome
Association Between Relative Change in 68Ga-DOTATATE PET/CT Parameters After C1 from Baseline and Morphologic Lesion Outcome
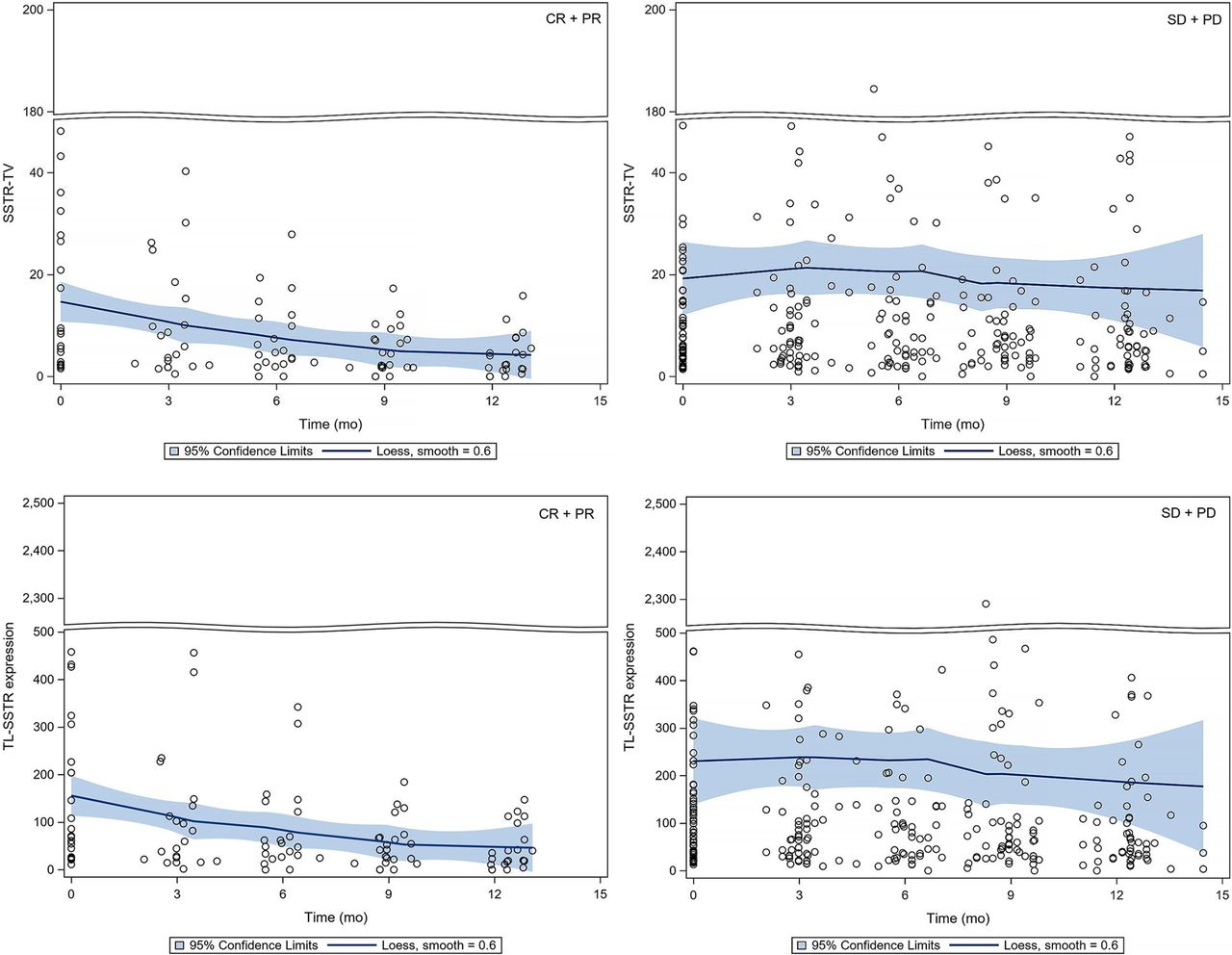
The changes in volumetric 68Ga-DOTATATE PET/CT parameters—that is, SSTR TV and total lesion SSTR expression—after C1 from baseline were significantly associated with lesion morphologic outcome (Fig. 1; Table 4). The specific uptake parameters decreased significantly after C1 from baseline in all lesions (responding and nonresponding) (Supplemental Fig. 1); however, this decrease was not associated with lesion morphologic outcome (Table 3).

Scatterplot with locally weighted scatterplot smoothing and 95% CI of SSTR TV and total lesion SSTR expression on baseline 68Ga-DOTATATE PET/CT and during subsequent treatment cycles. At left are morphologically responding lesions showing partial or complete response; at right are morphologically nonresponding lesions showing stable or progressive disease. CR = complete response; Loess = locally weighted scatterplot smoothing; PD = progressive disease; PR = partial response; SD = stable disease; TL = total lesion.
Correlation Between Tumor-Absorbed C1 Dose and Lesion Morphologic Outcome in All Lesions and in Size-Based Subgroups According to Primary NET Origin
18F-FDG PET/CT
At baseline, 21 target lesions from 12 patients were 18F-FDG–positive. Baseline values of SUVmax, SUVmean, metabolically active TV, and total lesion glycolysis showed no significant association with lesion morphologic outcome. A minor decrease in SUVmax was observed after C1 from baseline in all lesions (median, −10%; interquartile range [IQR], −20% to −8%; P = 0.03) but was not associated with lesion morphologic outcome, similarly to SUVmean, metabolically active TV, and total lesion glycolysis. Nevertheless, the small number of 18F-FDG–positive lesions prevents any meaningful statistical assessment.
Diffusion-Weighted MRI
Baseline ADC was available for 86 target lesions (6 excluded because of MR image artifacts; 24 were from patients followed by CT). The median value in all lesions was 859 (IQR, 718–1,002). ADC increased significantly after C1 from baseline in all evaluable lesions, with a median of 12% (IQR, 2%–27%; P < 0.001), and remained globally stable at the subsequent imaging time points. No statistically significant association was found between ADC (baseline or increase after C1) and lesion morphologic outcome (P = 0.58 and 0.71, respectively).
Imaging Parameters and Association with Patient Outcome
68Ga-DOTATATE PET/CT
An SSTR TV decrease of more than 10% from baseline after C1 discriminated patients with a significantly longer median PFS (51.3 mo) than that (22.8 mo) of patients for whom SSTR TV increased or decreased by less than 10% (P = 0.003; HR, 0.35; 95% CI, 0.16–0.75) (Fig. 2A). The same parameter remained significantly associated with PFS when patients with pancreatic primary NET were excluded, as presented in Figure 2B (median PFS of 51.3 mo compared with 27.6 mo: P = 0.008; HR, 0.32; 95% CI, 0.13–0.81). A decrease in total lesion SSTR expression of more than 10% from baseline after C1 discriminated patients with a median PFS of 32.2 mo, compared with 26.2 mo (P = 0.05; HR, 0.42; 95% CI, 0.17–1.0).

Kaplan–Meier curves of progression-free survival for SSTR TV change after C1 in all patients (A) and excluding patients with pancreatic primary NET (B), minimal absorbed dose per target lesion in C1 in all patients (C) and excluding patients with pancreatic primary NET (D), and combination of SSTR TV change after C1 and minimal absorbed dose per target lesion in C1 in all patients (E) and excluding patients with pancreatic primary NET (F). minC1 absorbed dose = minimal absorbed dose per target lesion in C1.
The changes in SSTR TV and total lesion SSTR expression after C1 remained significantly associated with the best objective response according to RECIST 1.1: a median decrease of −9% (IQR, −36% to 9%; P = 0.04) and −34% (IQR, −52% to −10%; P = 0.008) for SSTR TV and total lesion SSTR expression, respectively, in the responding patients, compared with 8% (IQR, 3% to 30%) and −3% (IQR, −19% to 10%) in the nonresponding patients.
Because the baseline tumor-to-spleen ratio was significant in a lesion-based analysis, the average values per patient were tested for association with patient outcome. An optimal cutoff of 1.25 demonstrated no significant association with PFS (P = 0.20) or with best objective response (P = 0.11).
18F-FDG PET/CT
Quantification of baseline 18F-FDG PET/CT was available for only 10 patients. Because of the low number of patients and events, no statistical analysis for association with patient outcome was performed.
Diffusion-Weighted MRI
In 29 patients followed by MRI, there was no statistical evidence of an association between baseline ADC or its relative change after C1 and patient outcome.
Tumor Dosimetry
Dosimetry was performed for 83 target lesions from 35 patients (33 lesions were excluded; Supplemental Fig. 2). The median absorbed dose in C1 was 33 Gy (IQR, 22–50 Gy) and declined from the first to the last treatment cycles, reaching significance between C1 and cycle 3 (P = 0.002), C1 and cycle 4 (P < 0.001), and cycles 2 and 4 (P = 0.01), as presented in Figure 3.

Tumor-absorbed dose as function of PRRT cycle across all target lesions. Whiskers indicate fifth and 95th percentiles.
The correlation between tumor-absorbed C1 dose and lesion outcome was tested for all target lesions treated with 4 PRRT cycles and in subgroups based on lesion size at baseline (inspired by a study by Ilan et al., in which accurate partial-volume effect correction was not possible for tumors < 22 mm in diameter, hence influencing the accuracy of activity measurement on SPECT images (13)) and on primary NET origin. As presented in Table 4, a significant correlation between tumor-absorbed C1 dose and lesion outcome was demonstrated for larger lesions (≥22 mm) and for the limited number of lesions of colorectal primary NET origin.
On a patient level, the minimal absorbed dose per target lesion in C1 ranged from 10 to 77 Gy. An optimal cutoff of 35 Gy (i.e., patients in whom all target lesions received at least a 35-Gy tumor-absorbed C1 dose) discriminated patients with a significantly longer median PFS (48.1 mo) than that of patients in whom at least 1 target lesion was treated with less than 35 Gy in C1 (26.2 mo) (P = 0.02; HR, 0.37; 95% CI, 0.17–0.82; P = 0.02) (Fig. 2C). The minimal absorbed dose per target lesion in C1 remained associated with PFS when patients with pancreatic primary NET were excluded, as presented in Figure 2D (median PFS of 48.1 compared with 27.6 mo: P = 0.05; HR, 0.40; 95% CI, 0.16–1.0).
Of the 26 patients who had a minimal absorbed dose of less than 35 Gy per target lesion in C1, 21 (81%) demonstrated an increase or decrease of less than 10% for SSTR TV on 68Ga-DOTATATE PET/CT after C1. Subsequently, the combination of these 2 parameters showed a stronger association with PFS in all patients (P < 0.001; HR, 0.32; 95% CI, 0.14–0.71) and when patients with pancreatic primary NET were excluded (P = 0.001; HR, 0.28; 95% CI, 0.10–0.77), as presented in Figures 2E and 2F, respectively. No association with PFS was found for the maximal or mean C1 doses.
DISCUSSION
We conducted a prospective study, unique to the best of our knowledge, aiming to assess the value of a series of multimodality imaging parameters and tumor-absorbed dose as potential predictive biomarkers of lesion and patient outcome after PRRT. Serial imaging (68Ga-DOTATATE PET/CT, 18F-FDG PET/CT, and diffusion-weighted MRI) and SPECT/CT-based tumor dosimetry at every cycle were performed in a standardized mode for each 177Lu-DOTATATE administration.
In 37 patients with advanced GEP-NETs, PRRT was confirmed to have high efficacy, with the median PFS reaching 28 mo and the best objective response rate being 30%, which line up with previous clinical trials (6,20). During a relatively long median follow-up (57 mo), our study’s primary endpoint of lesion-based time to progression was not reached. Only a small fraction (14%) of the prospectively followed target lesions progressed according to the morphologic criteria, questioning their suitability as reliable outcome measurements in PRRT. Although widely used, criteria based on morphologic measurements, such as RECIST 1.1, have several limitations that are significant in the particular setting of slow-growing NETs (21). In the NETTER1 trial, objective RECIST-based tumor response was reached in only 18% of the patients treated in the 177Lu-DOTATATE arm (6).
To our knowledge, this is the first report of the value of the lowest radiation dose received by tumors in C1 in predicting patient outcome. Patients receiving a minimum absorbed dose of 35 Gy in all measurable lesions showed a significantly longer median PFS than did patients in whom at least 1 target lesion received less than 35 Gy. This cutoff should ideally be confirmed in larger cohorts, especially in studies focusing on dose calculation for the entire tumor burden in the concept of personalized treatment regimes.
In a lesion-based analysis, our results demonstrate a correlation between absorbed dose in C1 and morphologic outcome only in the limited number of colorectal NET lesions but not for other primary NETs (i.e., pancreatic and small-intestinal). Direct comparison with previously published data, albeit scarce, on dose–response relationships in NETs treated with 177Lu-DOTATATE is impractical because of differences in study methods. Aiming to predict morphologic lesion outcome during treatment, we evaluated the absorbed dose received by the tumors only in C1. In contrast, in the study of Ilan et al., including only pancreatic NETs, the absorbed dose until the best response correlated with tumor shrinkage at any time during the treatment, especially in large lesions measuring at least 4 cm (13). In a study from the same group, evaluating only tumors of small-intestinal primary origin, no relationship between tumor shrinkage and absorbed dose was demonstrated (22). This follows our findings, again stressing the weakness of morphologic measurements (i.e., tumor shrinkage) as response criteria, especially in small-intestinal NETs.
Three-time-point SPECT/CT-based dosimetry after each 177Lu-DOTATATE injection revealed that the tumor-absorbed dose was higher in C1 and continuously decreased over the subsequent PRRT cycles. This observation supports the role of C1 and its impact on overall patient outcome. Furthermore, it could provide a basis for dosimetry-guided strategies in PRRT aiming at higher administered activities (to achieve higher tumor-absorbed doses) in the early therapy cycles. Several reports on the feasibility and safety of individualized dosimetry-based PRRT protocols in patients with NETs have been published so far. Two Swedish groups, using a similar study design, adjusted the number of PRRT cycles (each with a fixed injected activity of 7.4 GBq) to reach a maximum limit of absorbed dose to the kidneys. They achieved objective response rates of 24% (23) and 34% (24), without clinically significant toxicity. In contrast, Del Prete et al. personalized the administered activities in each cycle (median, 8.8 GBq) to deliver a prescribed absorbed dose to the kidneys over a fixed number of 4 PRRT cycles (25). They reported a high response rate of 59% and a significantly higher cumulative maximum tumor-absorbed dose, with a median 1.26-fold (maximum, 2.12-fold) increase compared with a simulated empiric regime. Because standard dosimetry protocols are generally burdensome for patients and personnel, implementing simplified procedures for such individualized tumor dosimetry is essential to expanding its availability in clinical routine. Methods of reducing the number of image acquisitions (single- or dual-time-point posttreatment SPECT/CT) are being explored by our group (26), as well as others (27,28), and they prove to be feasible and in agreement with standard dosimetry protocols.
SUV parameters measured on pretreatment SSTR PET/CT have been explored by many groups as predictors of PRRT outcome. In a study by Sharma et al., a baseline single-lesion SUVmax of more than 13 and an average SUVmax of more than 10.2 from up to 5 target lesions predicted RECIST 1.1 response to PRRT (11). Pauwels et al. found an SUVmean higher than 13.7 (derived from the whole-tumor burden on baseline 68Ga-DOTATOC PET/CT) to be associated with better overall survival (HR, 0.45; P = 0.024) (29). On a patient level, we could not identify any baseline 68Ga-DOTATATE PET parameters associated with outcome. In a lesion-based analysis, only the tumor-to-spleen ratio was significantly lower in responding than nonresponding lesions (P = 0.03). Nonetheless, its value in predicting response and thus guiding treatment decisions should be carefully assessed. The tumor-to-spleen difference between the 2 groups of lesions could be influenced by the higher radiotracer uptake in the spleen in patients showing a RECIST 1.1 partial response (data not shown). This observation is possibly related to differences in overall tumor burden and, thus, peptide biodistribution (30).
We assessed the evolution of serial 68Ga-DOTATATE PET/CT parameters after each treatment cycle with the intent to identify biomarkers of early outcome prediction using a rather complex design, which we do not recommend for implementation in clinical practice. Yet, this approach revealed that the changes in the volumetric 68Ga-DOTATATE PET/CT parameters observed already at 10–12 wk after C1 correlated significantly with both lesion outcome and patient outcome. An even stronger association with patient PFS was demonstrated when the SSTR TV decrease after C1 was combined with the minimal absorbed dose per target lesion in C1 (P < 0.001; Fig. 2E). Identifying these patients early during the treatment course is essential, as implementing optimization strategies such as combination therapies, or even using new α-emitting radiopharmaceuticals, might further improve patient outcome and survival.
Treatments inducing cancer cell death, such as PRRT, lead to an increase in ADC due to the development of cell swelling, tumor lysis, and necrosis (31). In our study, this increase in ADC after C1 was not associated with lesion morphologic response or patient outcome. Similarly, in a small population of 18 patients with NETs, Weber et al. saw no significant differences in diffusion-weighted MRI parameters between responders and nonresponders to PRRT (32).
Restricting the analysis to 5 target lesions, with the resulting incomplete assessment of SSTR expression, is perhaps the most limiting factor of the present study. We recognize that this limitation affects the comprehensiveness of our findings. We are currently analyzing the entire tumor burden on 68Ga-DOTATATE PET/CT in our prospectively followed cohort, aiming to evaluate how total tumor volumetric parameters and their change after C1 compare with the current methodology in predicting patient outcome. Additionally, target lesion selection can vary among observers, potentially affecting study results and their interpretation. Standardized criteria and involvement of more than one observer can significantly reduce intra- and interobserver variability. Enforcing these strategies minimized observer variability in our study.
Understanding the radiosensitivity of tumors is crucial in radiopharmaceutical therapies. Achieving this understanding involves various methods and techniques, including assessment of 18F-FDG PET parameters to evaluate changes in tumor metabolism in response to radiation. However, our study’s low number of 18F-FDG–positive lesions and patients prevents us from drawing any meaningful conclusions. At our center, all patients undergo dual-tracer PET/CT with 68Ga-DOTATATE and 18F-FDG to evaluate whether PRRT would be appropriate. Consequently, when there is a high 18F-FDG–positive tumor burden or 18F-FDG–positive/68Ga-DOTATATE–negative disease, other treatment modalities (e.g., chemotherapy) are preferred over PRRT.
Finally, the 68Ga-DOTATATE PET/CT segmentation method might be considered another limitation of our study. Customized thresholds based on physiologic liver SUVmax have been proposed, as compared with the frequently used 50% threshold of SUVmax that impacts the DOTATATE-avid TV in cases of intense radiotracer uptake (33). However, it is not uncommon for patients with metastatic NETs to have diffuse liver infiltration, restricting the use of physiologic liver uptake and stressing the need for standardized segmentation criteria on SSTR PET/CT imaging. An example of such a case from our study cohort is presented in Supplemental Figure 3.
CONCLUSION
In this prospective study, patients in whom all target lesions received an absorbed dose of at least 35 Gy in C1 demonstrated a longer PFS. This finding provides a basis for treatment strategies focusing on higher administered activities and higher tumor-absorbed doses in the early therapy cycles. Changes in SSTR TV and total lesion SSTR expression in selected target lesions after C1 correlated with lesion morphologic outcome, PFS, and best objective response. These findings support the use of volumetric parameters on 68Ga-DOTATATE PET/CT for early assessment of therapy response in GEP-NET patients treated with PRRT.
DISCLOSURE
A grant was provided by National Cancer Plan and Les Amis de l’Institut Bordet. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can molecular imaging and tumor dosimetry predict response to 177Lu-DOTATATE PRRT in patients with GEP-NETs?
PERTINENT FINDINGS: In a prospective study including 37 patients with advanced GEP-NETs, a decrease of more than 10% in volumetric parameters on 68Ga-DOTATATE PET/CT after C1, and a minimal tumor-absorbed dose of at least 35 Gy in C1, were significantly associated with a longer PFS.
IMPLICATIONS FOR PATIENT CARE: 68Ga-DOTATATE PET/CT and tumor lesion dosimetry could be used to predict patient outcome early in the course of PRRT, allowing implementation of strategies for further treatment optimization.
Footnotes
Published online Dec. 21, 2023.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 9, 2023.
- Revision received October 25, 2023.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Multicycle Dosimetric Behavior and Dose-Effect Relationships in [177Lu]Lu-DOTATATE Peptide Receptor Radionuclide Therapy
- Patient-Specific Dosimetry-Driven PRRT: Time to Move Forward!
- Dosimetry of [177Lu]Lu-DOTATATE in Patients with Advanced Midgut Neuroendocrine Tumors: Results from a Substudy of the Phase III NETTER-1 Trial
- Dosimetry Software for Theranostic Applications: Current Capabilities and Future Prospects
- The Translation of Dosimetry into Clinical Practice: What It Takes to Make Dosimetry a Mandatory Part of Clinical Practice
- Quantitative SPECT/CT Metrics in Early Prediction of [177Lu]Lu-DOTATATE Treatment Response in Gastroenteropancreatic Neuroendocrine Tumor Patients
- Absorbed Dose-Response Relationship in Patients with Gastroenteropancreatic Neuroendocrine Tumors Treated with [177Lu]Lu-DOTATATE: One Step Closer to Personalized Medicine