


Abstract
This study tested the principle that 68Ga-DOTATATE PET/CT may be used to select children with primary refractory or relapsed high-risk neuroblastoma for treatment with 177Lu-DOTATATE and evaluated whether this is a viable therapeutic option for those children. Methods: Between 2008 and 2010, 8 children with relapsed or refractory high-risk neuroblastoma were studied with 68Ga-DOTATATE PET/CT. The criterion of eligibility for 177Lu-DOTATATE therapy was uptake on the diagnostic scan equal to or higher than that of the liver. Results: Of the 8 children imaged, 6 had abnormally high uptake on the 68Ga-DOTATATE PET/CT scan and proceeded to treatment. Patients received 2 or 3 administrations of 177Lu-DOTATATE at a median interval of 9 wk and a median administered activity of 7.3 GBq. Of the 6 children treated, 5 had stable disease by the response evaluation criteria in solid tumors (RECIST). Of these 5 children, 2 had an initial metabolic response and reduction in the size of their lesions, and 1 patient had a persistent partial metabolic response and reduction in size of the lesions on CT, although the disease was stable by RECIST. One had progressive disease. Three children had grade 3 and 1 child had grade 4 thrombocytopenia. No significant renal toxicity has been seen. Conclusion: 68Ga-DOTATATE can be used to image children with neuroblastoma and identify those suitable for molecular radiotherapy with 177Lu-DOTATATE. We have shown, for what is to our knowledge the first time, that treatment with 177Lu-DOTATATE is safe and feasible in children with relapsed or primary refractory high-risk neuroblastoma. We plan to evaluate this approach formally in a phase I–II clinical trial.
- somatostatin receptor imaging
- childhood neuroblastoma
- 68Ga-DOTATATE
- 177Lu-DOTATATE
- targeted radionuclide therapy
- molecular radiotherapy
Neuroblastoma accounts for 6%–10% of all childhood cancers (1). Neuroblastomas show heterogeneity of behavior, with some regressing spontaneously and others progressing, despite intensive multimodality therapy. Current treatment for high-risk disease involves an intensive regime with induction chemotherapy, surgery, myeloablative chemotherapy with stem cell rescue, radiotherapy, and continuing therapy with 13-cis-retinoic acid and immunotherapy. Despite advances in the management of neuroblastoma, many children have primary refractory disease or relapse after initial treatment. The long-term survival rate remains under 40% (2–4). Improved therapeutic options are therefore required for these children.
For patients with relapsed or refractory neuroblastoma, treatment options include further chemotherapy or therapy with 131I-metaiodobenzylguanidine (131I-MIBG). Disease often becomes resistant to chemotherapy, and success is limited by poor bone marrow reserve in this heavily pretreated population.
Neuroblastomas derive from the neural crest and synthesize neurotransmitters, including somatostatin. Somatostatin receptors (particularly subtype 2) are expressed on the surface of some neuroblastomas, making molecular radiotherapy with somatostatin analogs an attractive therapeutic option in carefully selected patients (5–7).
Peptide receptor radionuclide therapy (PRRT) with radiolabeled somatostatin analogs is an established and effective treatment in somatostatin receptor–positive adult neuroendocrine tumors (8–10). The use of radiolabeled somatostatin analogs in neuroblastoma involves a distinct and separate cell surface molecular target different from the norepinephrine transporter molecule that takes up 131I-MIBG.
DOTATATE is the abbreviation used to describe a somatostatin analog, octreotate, linked with a chelator, 1,4,7,10-tetraazacyclotetradecane-N,N′,N′′,N′′′-tetraacetic acid (DOTA), that binds radionuclides. These include 68Ga, useful for imaging, and 177Lu for therapy. These agents have a high affinity for somatostatin receptor subtype 2.
68Ga-DOTATATE PET combined with CT has a higher sensitivity and improved spatial resolution for the detection of somatostatin receptor–positive tumors than somatostatin receptor scintigraphy with conventional SPECT γ-camera imaging using, for example, [111In-DTPA0]octreotide (Octreoscan; Mallinckrodt) (11–16). 68Ga-DOTATATE PET/CT enables the selection of patients for therapy with radiolabeled somatostatin analogs (17,18).
Here, using data on 6 children with neuroblastoma who were imaged with 68Ga-DOTATATE PET/CT and subsequently received molecular radiotherapy using 177Lu-DOTATATE, we provide proof of principle that children with neuroblastoma can be imaged and treated with somatostatin receptor–targeted agents.
MATERIALS AND METHODS
Patients
Between August 2008 and July 2010, 8 children with relapsed or primary refractory neuroblastoma were enrolled. All children were assessed for suitability for 177Lu-DOTATATE therapy by imaging with 68Ga-DOTATATE PET/CT. All 8 children were imaged with 68Ga-DOTATATE PET/CT according to the local protocol (19) on a Discovery STE PET/CT system (GE Healthcare). Patients were injected intravenously with at least 100 MBq for adequate image quality. Imaging took place at least 45 min but no longer than 1 h after injection. A low-dose scout projection (120 kVp; 10 mA; pitch, 1.75) was used to localize the region of head to thigh for transmission and emission imaging. CT was performed at 140 kVp and 40 mA for pediatrics. PET was performed in 3-dimensional mode with 4 min per bed position. Iterative reconstruction with 21 subsets was performed with attenuation correction.
If disease sites showed avid uptake of 68Ga-DOTATATE that was greater than uptake in the liver, then the child was considered eligible for therapy. Children were also imaged with 123I-MIBG to correlate uptake in disease sites.
Children had not been treated previously with other radiolabeled somatostatin analogs. Prerequisites for each treatment were adequate hematologic, renal, and hepatic function and adequate performance status. The parents or guardian, as well as comforters and caregivers, of each patient gave written informed consent for treatment. Each patient was treated on a compassionate basis when no other treatment options were available.
Methods
Children were admitted into one of the dedicated pediatric radionuclide inpatient treatment rooms for their 177Lu therapy, supported by specialized pediatric medical and nursing ward staff.
177Lu-DOTATATE was obtained commercially (IDB Holland, bv) and reconstituted in the in-house radiopharmacy.
Premedication consisted of ondansetron (5 mg m−2; maximum, 8 mg) twice daily orally for 5 d and dexamethasone (250 μg kg−1) daily orally in 2 divided doses for 5 d.
To reduce the radiation dose to the kidneys, an intravenous infusion of amino acids (2.5% L-lysine HCl and 2.5% L-arginine in water for injection) at the rate of 1 L over 4 h was commenced 30 min before the administration of the radiopharmaceutical. The 177Lu-DOTATATE was then administered intravenously via a second pump over 30 min.
The administered activity of 177Lu-DOTATATE was planned to be a fixed dose of 7.4 GBq per cycle. However, because of various problems with production and labeling it ranged from 4.04 to 7.5 GBq, with the median being 7.3 GBq, equating to administered activities of 0.1–0.5 GBq kg−1 (mean, 0.3 GBq kg−1). Repeated administrations were planned at 8- to 10-wk intervals to a maximum of 4 administrations. However, the patients’ condition precluded the full delivery of all fractions in most cases.
Whole-body planar scans and SPECT/CT scans were obtained after treatment to examine uptake of the therapeutic agent. All images were acquired on an Infinia Hawkeye 4 (GE Healthcare) dual-detector system. Whole-body planar scans were obtained with an emission window of 208 keV ± 10%. Bed speed was 10 cm/min. SPECT/CT was performed with an emission window of 208 keV ± 10%, with 120 projections and 30 s per projection; CT was performed at 140 kVp and 2.5 mA, with a slice thickness of 5 mm. Iterative reconstruction was used (20 subsets) with a 3-dimensional Butterworth filter and attenuation correction from the CT dataset.
After administration, weekly full blood counts, urea and electrolyte tests, and liver function tests were performed. Toxicity was graded using the Common Toxicity Criteria of the National Cancer Institute, version 3.0. Patients were examined in the outpatient clinic 2 wk after therapy, and 68Ga-DOTATATE PET/CT was performed again at 6–8 wk after treatment for reassessment. 123I-MIBG imaging and 18F-FDG PET were also used in response assessment, but not all of the patients were imaged with all of the modalities. Pre- and posttreatment bone marrow aspiration and trephine biopsy were not routinely performed.
RESULTS
Patient Characteristics
To assess suitability for therapy with 177Lu-DOTATATE, each patient underwent a 68Ga-DOTATATE PET/CT scan. Of the 8 children assessed, 2 had only faint uptake in disease sites on 68Ga-DOTATATE PET/CT and so were deemed unsuitable for 177Lu-DOTATATE therapy.
Six children were treated (Table 1). All of their scans showed known disease sites to have avid uptake of 68Ga-DOTATATE that was greater than uptake in the liver. Four children were female, and 2 were male. The children's ages ranged from 2 to 14 y, with a median of 7.5 y. All children had a confirmed histologic diagnosis of neuroblastoma. Five children had International Neuroblastoma Staging System stage 4 disease, and 1 had stage 3 disease (20). Three patients had primary refractory disease, and 3 had relapsed disease. One patient had MycN amplification. All of the children had had multiple previous lines of chemotherapy ranging from 2 to 5 different regimens. Four patients had had previous 131I-MIBG therapy ranging from 1 to 5 y prior. The time required from prior therapy to 177Lu-DOTATATE therapy was the time needed for adequate hematologic recovery.
Summary of Prior Therapies, Toxicity, and Response in 6 Patients Treated
Treatment Delivery
Fifteen administrations of 177Lu-DOTATATE were given in total. Three children had 3 administrations, and 3 had 2 administrations. The interval between treatments was 9–14 wk, with a median of 9 wk.
Inpatient stay for treatment was determined by the child's external radiation dose rate measured at chest level at a distance of 1 meter with a dose rate meter, compared with the standard 131I charts, per local guidelines (21). Patients retained only 10%–40% of the original administered activity 24 h after administration and could be discharged the following day from an external-dose-rate point of view. Dose rates measured the day after administration varied between discharge-on-public-transport level (∼19μSv/h [400 MBq 131I equivalent]) and discharge with no restrictions at all (1.5μSv/h [30 MBq 131I equivalent]). Patients’ admission ranged from 2 to 5 nights, with 10 of the 15 administrations requiring only a 2-night stay, 4 administrations a 3-night stay, and only 1 administration a 5-night stay, which was for practical logistic reasons.
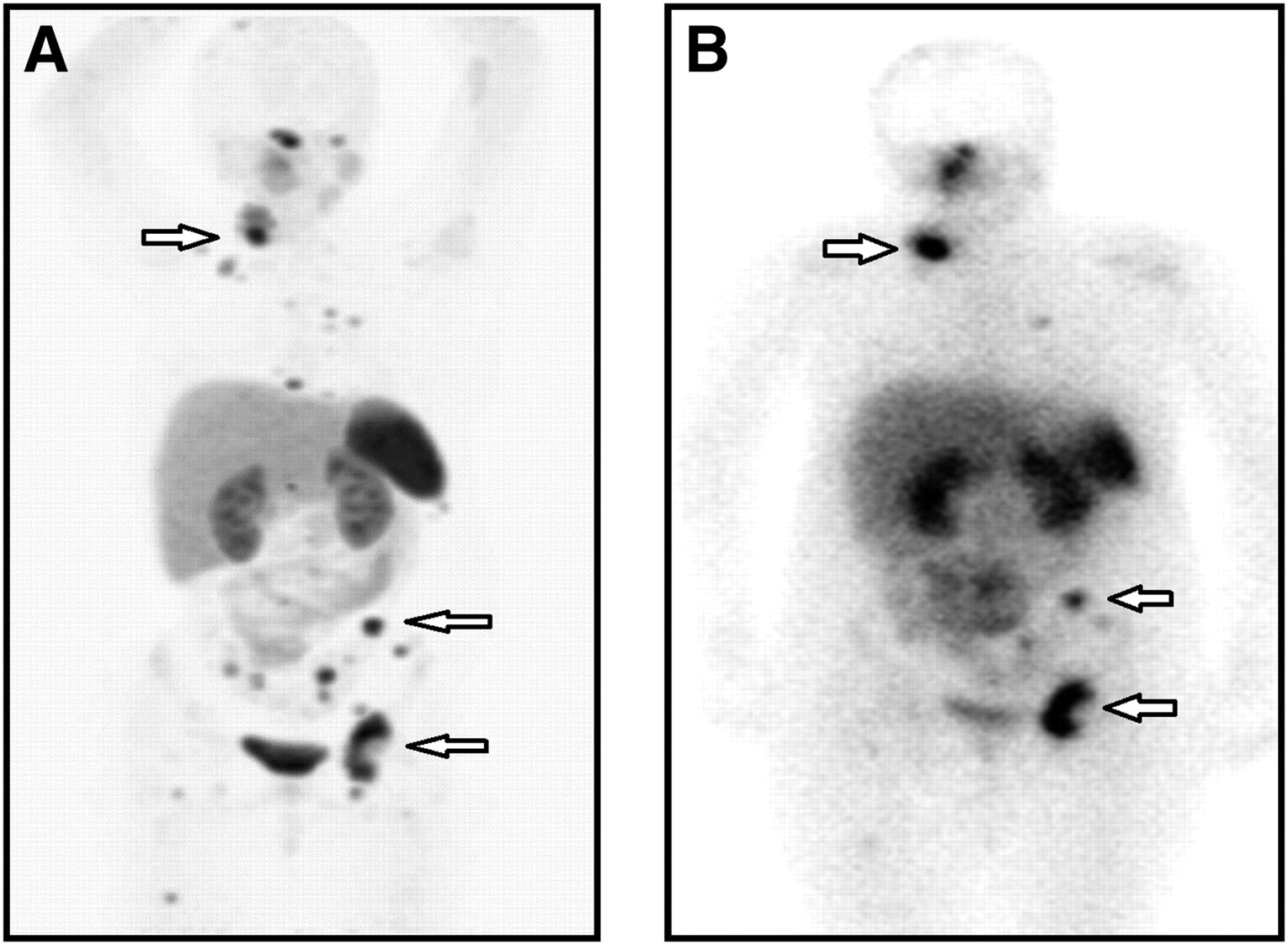
After administration of 177Lu-DOTATATE, whole-body planar scans and SPECT/CT scans were acquired to map the uptake of the therapeutic dose. Although the spatial resolution of SPECT/CT images is different from that of PET/CT images, uptake could be confirmed in the disease sites seen on the pretherapy PET/CT images (Fig. 1).
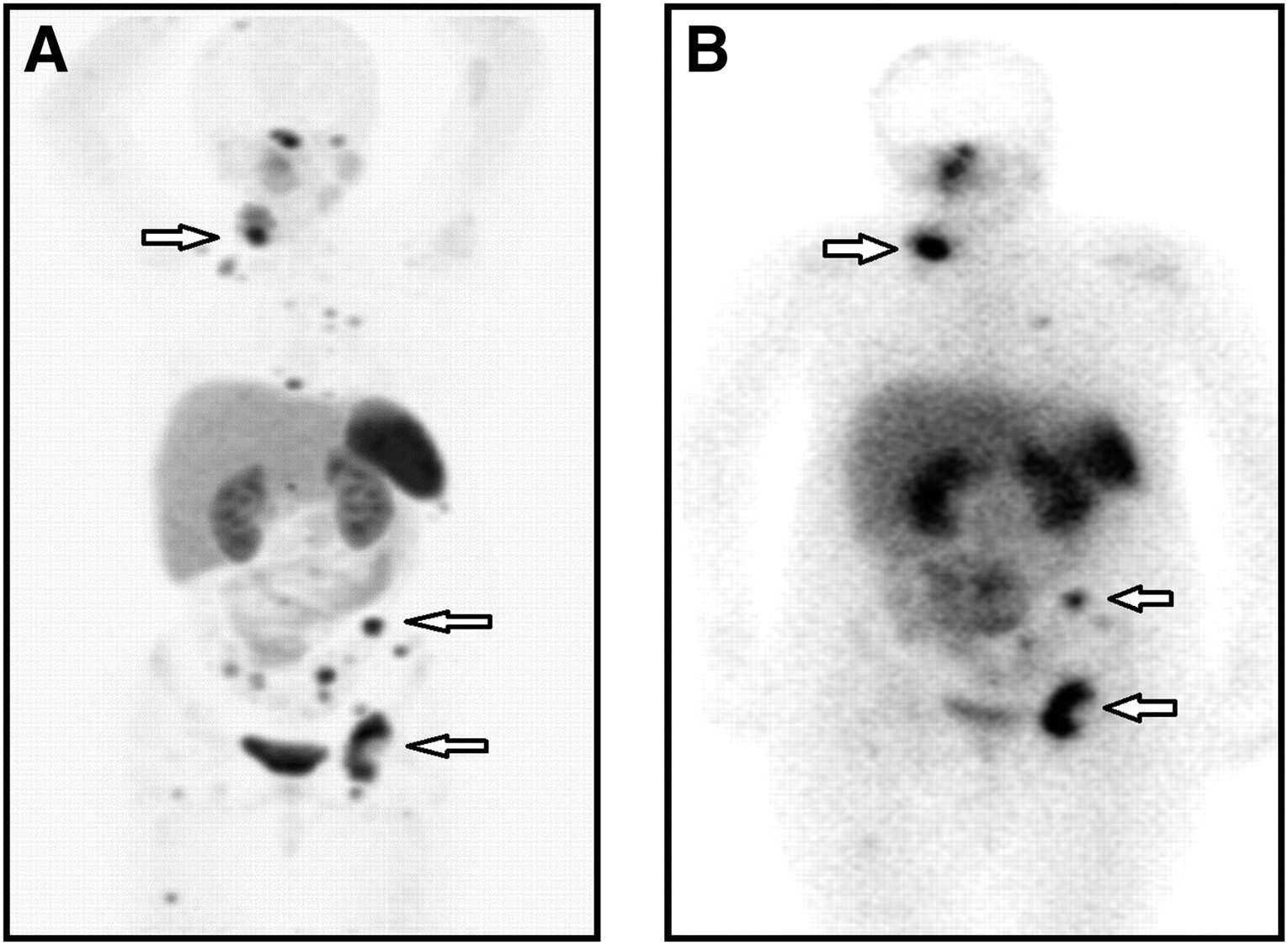
(A) Anterior maximum-intensity-projection image of diagnostic pretreatment 68Ga-DOTATATE PET/CT in child with relapsed neuroblastoma. Physiologic distribution of 68Ga-DOTATATE is seen in pituitary, liver, spleen, kidneys, and bladder. Uptake is also observed in disease sites in right posterior triangle and supraclavicular fossa (arrow); soft-tissue nodules anterior to the iliacus (arrow); left common, internal iliac, and obturator nodes (arrow); and multiple bone metastases. (B) Anterior maximum-intensity-projection image of SPECT/CT scan in same child with relapsed neuroblastoma after first administration of 177Lu-DOTATATE, confirming uptake of 177Lu-DOTATATE in same regions as on pretherapy 68Ga-DOTATATE scan (arrow).
Toxicity
Grade 1 nausea occurred in 3 patients. Two children had grade 3 thrombocytopenia after 2 administrations, and 1 patient had grade 3 thrombocytopenia after 3 administrations. One patient had grade 4 thrombocytopenia after the second administration of 177Lu. No further 177Lu was given to these patients, but 3 of 4 patients subsequently recovered their platelet counts. One patient was platelet-dependent before treatment with 177Lu and remains platelet-dependent but tolerated 3 administrations without any additional complications.
Two patients had grade 1 renal toxicity as determined by serial serum creatinine measurements. No other renal toxicity was seen. There were no life-threatening consequences or treatment-related fatalities.
Response to Therapy
The children in this study were a heterogeneous group with a poor prognosis. Treatment was given on a compassionate basis, and therefore not all patients were assessed with multimodality imaging and bone marrow aspirates or trephine biopsies were not performed. An individual account of each patient's response is given. If there was measurable soft-tissue disease then the RECIST were used (22), but if disease was only evaluable on 123I-MIBG or PET/CT then response by these imaging modalities was used.
Patient 1 had disease in the left lung invading the chest wall and had received prior 131I-MIBG and external-beam radiotherapy to this site as well as multiple lines of chemotherapy. Imaging before treatment was with 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT. After 1 cycle of 177Lu-DOTATATE, there was an initial partial metabolic response as judged by reduction in maximum standardized uptake value (SUVmax) scores on 18F-FDG PET/CT and 68Ga-DOTATATE PET/CT. The size of the chest lesion also reduced on CT but not enough to constitute a partial response according to RECIST. Two months after the second cycle of 177Lu-DOTATATE, there was progressive disease as judged by an increase in the size of the mass on 18F-FDG PET/CT.
Patient 2 had liver and bone disease and had received prior 131I-MIBG therapy and several lines of chemotherapy. The patient was imaged with 68Ga-DOTATATE PET/CT, 123I-MIBG, and 18F-FDG PET/CT before treatment. There was discordance between the imaging modalities: the lesions were not 18F-FDG–avid, and 123I-MIBG imaging showed a lesser extent of disease than did 68Ga-DOTATATE PET/CT. After 3 cycles of 177Lu-DOTATATE and on reassessment imaging 4 mo after completion of therapy, there was a partial metabolic response, with significant reductions in SUVmax scores on 68Ga-DOTATATE PET/CT in both the liver and the T4 lesions. On the CT scan, there was a reduction in the size of the liver lesions, but this did not qualify as a partial response according to RECIST. The disease remained nonavid for 18F-FDG, and there were no new lesions. 68Ga-DOTATATE imaging 1 y later confirmed the response (Fig. 2).
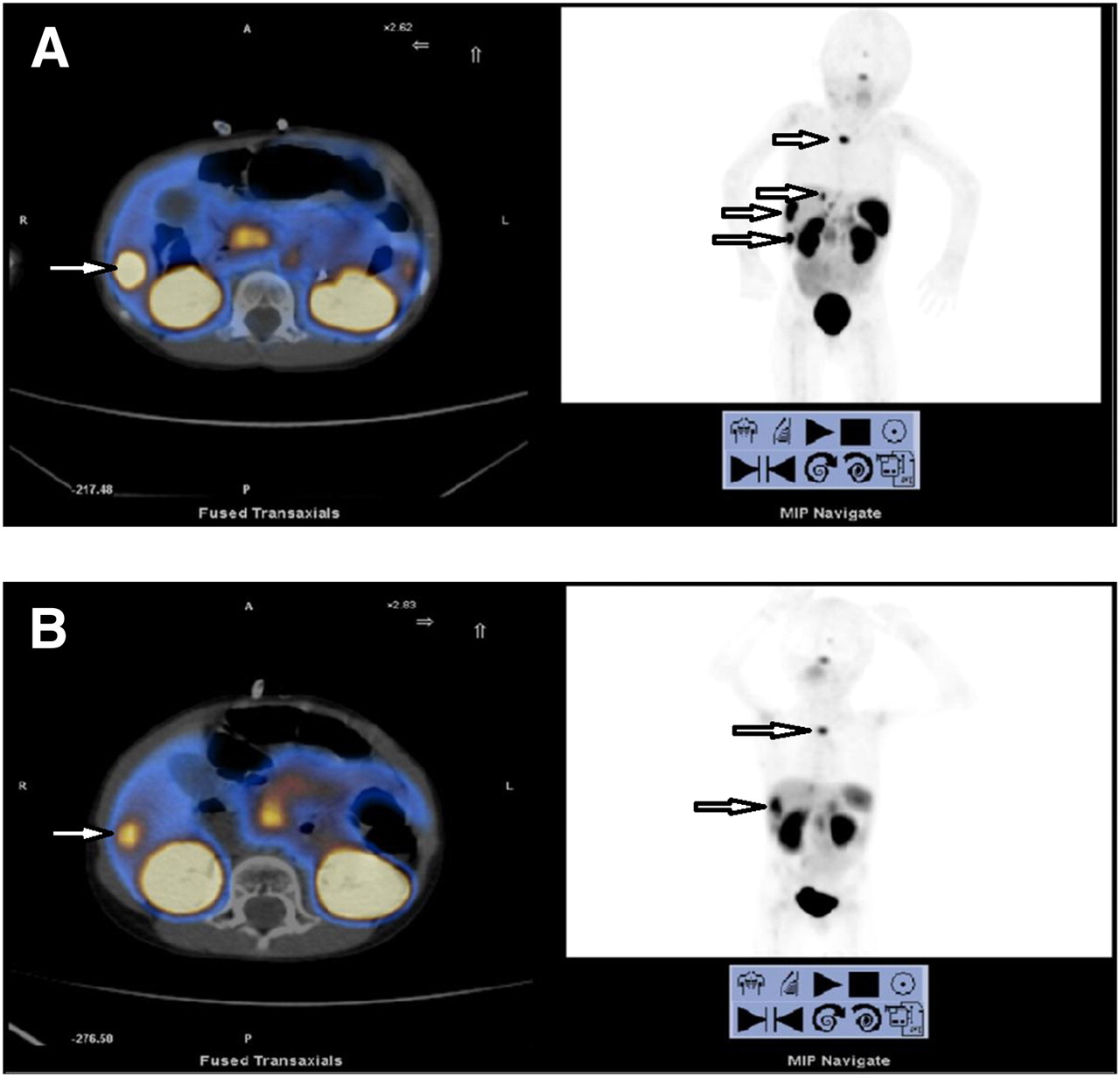
(A) Pretreatment 68Ga-DOTATATE PET/CT images showing 68Ga-DOTATATE–avid lesions in T4 vertebral body and 3 metastases in liver (arrow). Physiologic uptake is seen in pituitary, kidneys, bladder, stomach wall, liver, and spleen. (B) Images from repeated 68Ga-DOTATATE PET/CT 1 y later after 3 administrations of 177Lu-DOTATATE, showing metabolic partial response with reduction in SUVmax of lesion in T4 (SUVmax reduced from 13.2 to 9.9) and liver (lesion segment V, SUVmax reduced from 25.8 to 11) and no new lesions. Cross-sectional imaging shows reduction in size of liver lesions, although patient had stable disease by RECIST. MIP = maximum-intensity projection.
Patient 3 had localized soft-tissue disease only, with a large abdominal mass and no bone marrow disease. This patient's disease was negative for 123I-MIBG. Assessment was therefore with 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT. After treatment with 3 administrations of 177Lu-DOTATATE, patient 3 had stable disease by RECIST on CT. There was no significant change in SUVmax scores on either 68Ga-DOTATATE PET/CT or 18F-FDG PET/CT. The patient remains clinically well and off treatment 12 mo after the first administration of 177Lu-DOTATATE.
Patient 4 had a mixture of soft-tissue and bone disease. Assessment was with 68Ga-DOTATATE PET/CT. There was an initial metabolic response after 2 administrations of 177Lu-DOTATATE, with reductions in the SUVmax scores on 68Ga-DOTATATE PET/CT and a reduction in the size of the lesion on CT. The patient had stable disease by RECIST 8 wk after the final administration. Repeated imaging 5 mo after the last administration revealed progressive disease.
Patient 5 had diffuse bone and bone marrow disease and had received previous 131I-MIBG. On the reassessment 68Ga-DOTATATE PET/CT scan after 2 cycles of 177Lu-DOTATATE, there was no significant change in SUVmax scores and there was stable disease by RECIST on CT.
Patient 6 had widespread soft-tissue disease and bone metastases. Prior 131I-MIBG had been given. After 3 administrations of 177Lu-DOTATATE, there was progressive disease by RECIST as defined by the presence of new lesions on 18F-FDG PET/CT and 68Ga-DOTATATE PET/CT. Compared with 68Ga-DOTATATE PET/CT, 18F-FDG PET/CT underestimated the extent of the disease.
DISCUSSION
To our knowledge, this is the first published evidence of the use, in children with neuroblastoma, of 68Ga-DOTATATE PET/CT for therapy selection and response assessment and of 177Lu-DOTATATE for molecular radiotherapy. The established effectiveness of peptide receptor radionuclide imaging and therapy in adult neuroendocrine tumors provided the rationale to use this approach in children with neuroblastoma.
PRRT in adults with somatostatin-positive neuroendocrine tumors has resulted in improved symptoms, prolonged survival, and an enhanced quality of life (10,23–25). In studies of adults with neuroendocrine tumors, 177Lu-DOTATATE has been well tolerated, with little acute toxicity. The dose-limiting toxicities are renal and hematologic (10).
Neuroblastoma patients with somatostatin receptor–positive disease identified with 68Ga-DOTATATE PET/CT were deemed eligible for therapy with 177Lu-DOTATATE. 177Lu-DOTATATE offers a unique treatment target and differs from 131I-MIBG and chemotherapy in its mode of action. We recognize the success of 131I-MIBG therapy (26–29) and do not propose 177Lu-DOTATATE as a competitor but as a therapeutic option for those who have relapsed or have primary refractory disease and who may or may not have already received 131I-MIBG therapy. A combination of the 2 agents may be more effective than either used alone. Although both cause myelosuppression, they may complement each other in being able to deliver targeted radiation to different areas of the tumor, depending on the molecular target expressed. We have demonstrated in 1 patient in this series that diagnostic imaging with both 123I-MIBG and 68Ga-DOTATATE yielded nonconcordant results, another reason why combination therapies may be more effective.
All of the patients in this study had end-stage disease with few treatment options available and a poor prognosis. We aimed principally to assess 177Lu-DOTATATE as a feasible therapy, not its response. When disease was measurable, RECIST were used. Disease that was evaluable but not measurable was assessed on 123I-MIBG or PET/CT with either 68Ga-DOTATATE PET/CT or 18F-FDG PET/CT. An account of the metabolic response is also given, but we acknowledge that this is not yet a validated approach. Of the 6 children treated, 5 had stable disease by RECIST. Of these 5 children, 2 had an initial metabolic response and reduction in the size of their lesions, and 1 patient had a persistent partial metabolic response and reduction in size of the lesions on cross-sectional imaging, although the disease was stable by RECIST. One had progressive disease.
PRRT has minimal acute toxicities, and the main concern is renal and hematologic function. None of the children in our study have developed any significant renal toxicity (although follow-up duration is short). Hemotoxicity, however, has been observed, with grade 3 thrombocytopenia in 3 children and grade 4 thrombocytopenia in 1 child. The thrombocytopenia was transient in 3 of the 4 children. These children were heavily pretreated with multiple lines of chemotherapy and 131I-MIBG.
Dosimetry for PRRT is still developing (30,31) and will become an essential part of therapy with peptide receptor radionuclides because the same administered activity results in a variable absorbed radiation dose in grays to both the tumor and the dose-limiting organs at risk, especially the kidneys and bone marrow. Individual patient dosimetry becomes even more important in the pediatric population, in which there is a greater variation in body surface area, potentially requiring a modification of the administered activity, and individuals cured of their cancer may live for decades with late effects.
Menda et al. reported a phase I trial using 90Y-DOTATOC in children and young adults with tumors expressing somatostatin receptors, including 2 patients with neuroblastoma (32). From their dosimetry data, they found the maximum tolerable dose of 90Y-DOTATOC to be highly variable and proposed individualized dose administration as a preferred method to improve efficacy and reduce toxicity. 90Y is a pure β-emitter, and therefore dosimetry and imaging have historically required concurrent administration of 111In-DTPA-D-Phe1-octreotide whereas 177Lu-DOTATATE emits γ- and β-radiation, allowing essential dosimetry measurements and imaging to be performed from the same administration. There have been reports on the feasibility of 90Y PET/CT; the main limitation is the data acquisition time (33,34).
After this proof-of-principle study, we plan to evaluate 177Lu-DOTATATE formally in a phase I–II clinical trial to evaluate toxicity and response. Individualized patient dosimetry will form an essential part of this trial.
CONCLUSION
68Ga-DOTATATE can be used to identify patients with relapsed or primary refractory high-risk neuroblastoma who have somatostatin receptor–positive disease suitable for therapy with the radiolabeled somatostatin analog 177Lu-DOTATATE. Subsequent posttherapy 68Ga-DOTATATE scans can be used to assess response. Treatment with 177Lu-DOTATATE was feasible, practical, and well tolerated in this small group of patients with high-risk neuroblastoma. This approach will be evaluated further in a phase I–II clinical trial in relapsed or primary refractory high-risk neuroblastoma to formally assess response rate and toxicity.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This work was undertaken at UCLH/UCL, which received a proportion of funding from the Department of Health's NIHR Biomedical Research Centers funding scheme, Cancer Research U.K., the KCL/UCL CCIC, the University College London Hospitals Charity (Rays of Hope for Children with Cancer), and the Neuroblastoma Children's Cancer Alliance. No other potential conflict of interest relevant to this article was reported.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication November 8, 2010.
- Accepted for publication April 20, 2011.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preclinical Evaluation of 177Lu-OncoFAP-23, a Multivalent FAP-Targeted Radiopharmaceutical Therapeutic for Solid Tumors
- 68Ga-DOTATATE PET in Restaging and Response to Therapy in Neuroblastoma: A Case Series and a Mini Review
- 68Ga-DOTATATE PET in Restaging and Response to Therapy in Neuroblastoma: A Case Series and a Mini Review
- PET/MRI in Pediatric Neuroimaging: Primer for Clinical Practice
- 68Ga-DOTATATE PET/CT for Neuroblastoma Staging: Utility for Clinical Use
- NANETS/SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy
- Targeted Molecular Radiotherapy of Pediatric Solid Tumors Using a Radioiodinated Alkyl-Phospholipid Ether Analog
- 68Ga-DOTATOC and FDG PET Imaging of Preclinical Neuroblastoma Models
- Advances in Risk Classification and Treatment Strategies for Neuroblastoma
- Potential Pediatric Applications of PET/MR
- Radiopeptide Imaging and Therapy in the United States