


Abstract
During tumor therapy with radiolabeled somatostatin analogs, the kidneys are dose limiting. Renal uptake in patients can effectively be reduced by a 4- to 10-h intravenous infusion of a lysine/arginine solution, thereby increasing the maximum radiation dose to the tumor without renal side effects. Oral administration of amino acids could facilitate this labor-intensive procedure. Therefore, the effects of oral versus intravenous administration of d-lysine were compared in rats injected with [111In-diethylenetriaminepentaacetic acid (DTPA)]octreotide. Methods: Rats were intravenously injected with 3 MBq/0.5 μg [111In-DTPA]octreotide and also received d-lysine intravenously or orally in various concentrations and following various time schedules. Twenty-four hours after injection, a biodistribution study and renal ex vivo autoradiography were performed. Results: Renal uptake was reduced significantly—up to 40%—in all lysine-treated groups, without affecting the uptake in other organs. Conclusion: Renal uptake of this radiolabeled peptide can be reduced up to 40% both by oral and by intravenous administration of lysine in rats.
For years, stabilized somatostatin analogs have been used successfully in the clinic for peptide receptor scintigraphy of neuroendocrine tumors (1,2). These tumors overexpress somatostatin subtype 2 receptors on their cell membrane, to which somatostatin analogs (e.g., [diethylenetriaminepentaacetic acid (DTPA)]octreotide and [1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA),Tyr3] octreotate) bind with high affinity. [DTPA]octreotide also binds to somatostatin subtype 3 and somatostatin subtype 5 receptors, albeit with much lower affinity (3). Somatostatin analogs radiolabeled with therapeutic radionuclides, such as 177Lu and 90Y, are being used for peptide receptor radionuclide therapy (PRRT). This new form of targeted therapy has proven to be promising in preclinical and clinical studies (4–6). Other radiolabeled peptides frequently used in PRRT are [177Lu-DOTA,Tyr3]octreotate (4), [90Y-DTPA, Tyr3]octreotide (3,6), and 90Y-lanreotide (4). The results of these studies show high tumor response rates in patients.
However, the drawback of PRRT could be the total administered radioactivity to patients, which is limited by critical organs, such as the kidneys (3,7–9). The kidneys reabsorb part of the radiolabeled peptides in the proximal tubules after glomerular filtration (10). The peptide itself is degraded in the lysosomes of these cells, whereas the radionuclide–chelator complex is trapped inside the proximal tubular cells (9,10). A high dose to the kidneys could lead to nephrotoxicity, which in turn could lead to kidney failure (9). When this high renal radiation dose can be reduced, a higher dose to the tumor can be given, possibly leading to a higher success rate for PRRT.
Several researchers have shown that intravenous coadministration of lysine to rats results in a 40%–50% reduction of renal uptake of these radiolabeled peptides (11–13). In the clinic, the reduction of radioactivity in the kidneys is achieved by an infusion of lysine/arginine over a longer time (5,9,14–16). Radiolabeled somatostatin analogs are positively charged, favoring binding to negatively charged proximal tubular cells. Lysine and arginine are also positively charged and can, at high-enough concentrations, partly inhibit the renal reabsorption of somatostatin analogs. Recently, our group has shown that megalin is involved in the renal retention of these analogs and that new strategies can be developed to further decrease renal uptake (17).
It is preferred that lysine/arginine infusions in the clinic take place over 10 h (16); however, in practice most infusions are given in 4 h or less. Instead of this labor-intensive infusion method, a repeated oral administration of lysine/arginine solution could be more convenient both for the patients and for the hospital staff. Therefore, the aim of this work was to compare, in a rat model, oral versus intravenous administration of lysine with regard to reduction of renal uptake of [111In-DTPA]octreotide.
MATERIALS AND METHODS
Preparation of [111In-DTPA]Octreotide
Commercially available kits of [DTPA]octreotide and 111InCl3 were obtained from Tyco Health Care. The radiolabeling procedure was in accordance with standard procedures and previously published work (18).
Tissue Distribution of [111In-DTPA]Octreotide in Rats
Animal experiments were performed in compliance with the regulations of our institution and with generally accepted guidelines governing such work.
Adult male Lewis rats (Harlan) weighing 250–300 g were used for these experiments. All experimental groups are described in Table 1. d-lysine (Sigma-Aldrich) was diluted to a concentration of 400 mg/mL in saline. Groups that were treated with d-lysine received a dose of 400 or 800 mg/kg of this solution.
Description of Experimental Groups
At t = 0, [111In-DTPA]octreotide (3 MBq; 0.5 μg of peptide) was administered to all rats intravenously into the dorsal vein of the penis. The control group had no d-lysine administered. The intravenous group received 400 mg/kg coinjected with the radiolabeled peptide. To the groups receiving d-lysine orally (using an oral needle), 400 mg/kg were administered 30, 60, or 120 min before the radiolabeled peptide. An additional group had food withheld for 6–8 h before receiving a 400 mg/kg oral dose of d-lysine 30 min before the peptide. A final group received an 800 mg/kg oral dose of d-lysine 30 min before the peptide.
Twenty-four hours after injection of [111In-DTPA]octreotide, the following tissues were isolated: spleen, pancreas, adrenals, liver, stomach, muscle, femur, and 1 kidney. Radioactivity was measured in blood samples and in these isolated organs using a γ-counter (Wallac 1480 Wizard 3″; Perkin Elmer). The second kidney was immediately frozen using isopentane (Fluka Chemika) and liquid nitrogen and stored in a −80°C freezer, until processed for ex vivo autoradiography.
Ex Vivo Autoradiography
Frozen tissues were embedded in TissueTek (Sakura) and processed for cryosectioning. Tissue sections of 10 μm were mounted on SuperFrostPlus glass slides (Menzel) and exposed to phosphor imaging screens (Perkin Elmer) overnight in x-ray cassettes (Kodak). The screens were analyzed using a Cyclone phosphor imager and a computer-assisted OptiQuant 03.00 image-processing system (Perkin Elmer). Thereafter, an adjacent tissue section was stained with conventional hematoxylin and eosin.
Statistical Analysis
Data are expressed as mean ± SEM. Results were statistically analyzed using 1-way ANOVA. Differences were considered statistically significant when P was <0.05. If significance was found, a Dunnett multiple-comparison test was performed to compare all groups with the control group. All statistical analyses were performed with the Prism 4.0 program (GraphPad).
RESULTS
Preparation of [111In-DTPA]Octreotide
The labeling efficiency of [111In-DTPA]octreotide was determined with instant thin-layer chromatography and was >95%.
Tissue Distribution of [111In-DTPA]Octreotide in Rats
Figure 1 shows the results for the tissue distribution of [111In-DTPA]octreotide in blood and several somatostatin receptor–positive organs, such as pancreas and adrenals. No differences in these organs were seen between any treatment group and the control group. Slightly higher uptake in the adrenals was seen in the intravenous group and in the oral group from which food had been withheld; however, this increase was not statistically significant.

Radioactivity of [111In-DTPA]octreotide in blood (A), spleen (B), and 2 somatostatin subtype 2 receptor–positive organs (pancreas [C] and adrenals [D]) 24 h after injection of peptide, 3 MBq/0.5 μg. Data are expressed as percentage injected activity (%IA) per gram of tissue (mean ± SEM). Statistical analysis showed no significance (ns) between control bar and any other bar. con = control; iv = intravenous; Lys = d-lysine; nf = no food; po = by mouth/oral.
The uptake in the kidneys and the percentage reduction in kidney uptake are shown in Figure 2. All treatments resulted in a lower renal uptake than that of the control group. A renal reduction of about 41% (39%–43%) was seen in the intravenous group, in the group that received 800 mg/kg orally, and in the group that received 400 mg/kg orally 60 min before the peptide. These results were confirmed by the ex vivo autoradiography data (Fig. 3).
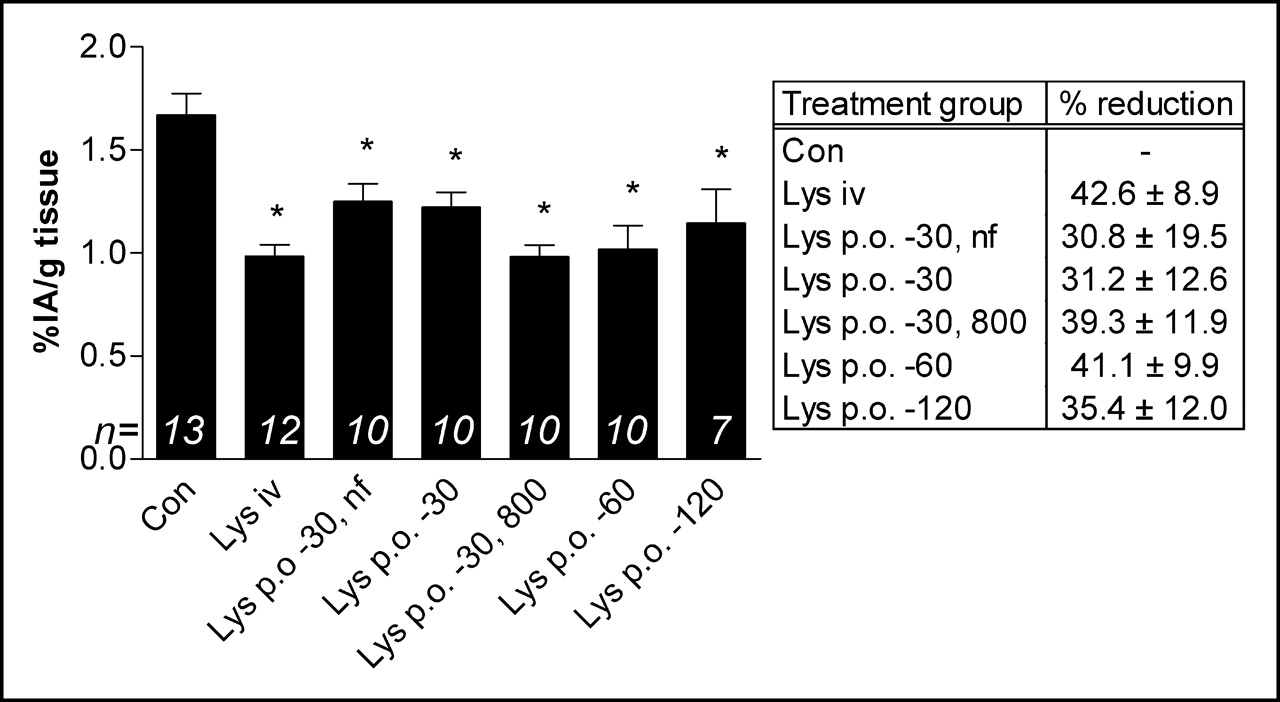
Uptake of [111In-DTPA]octreotide in kidney 24 h after injection of peptide, 3 MBq/0.5 μg, to all treatment groups. Data are expressed as percentage injected activity (%IA) per gram of tissue (mean ± SEM). Statistical analysis showed significant difference (P < 0.01) between control bar and each other treatment group. Also, percentage reduction of each treatment group is shown in adjacent table. Oral administration of lysine 30 min (800 mg/kg) or 60 min (400 mg/kg) before tracer produced renal reduction similar to that with intravenous administration. con = control; iv = intravenous; Lys = d-lysine; nf = no food; p.o. = by mouth/oral.
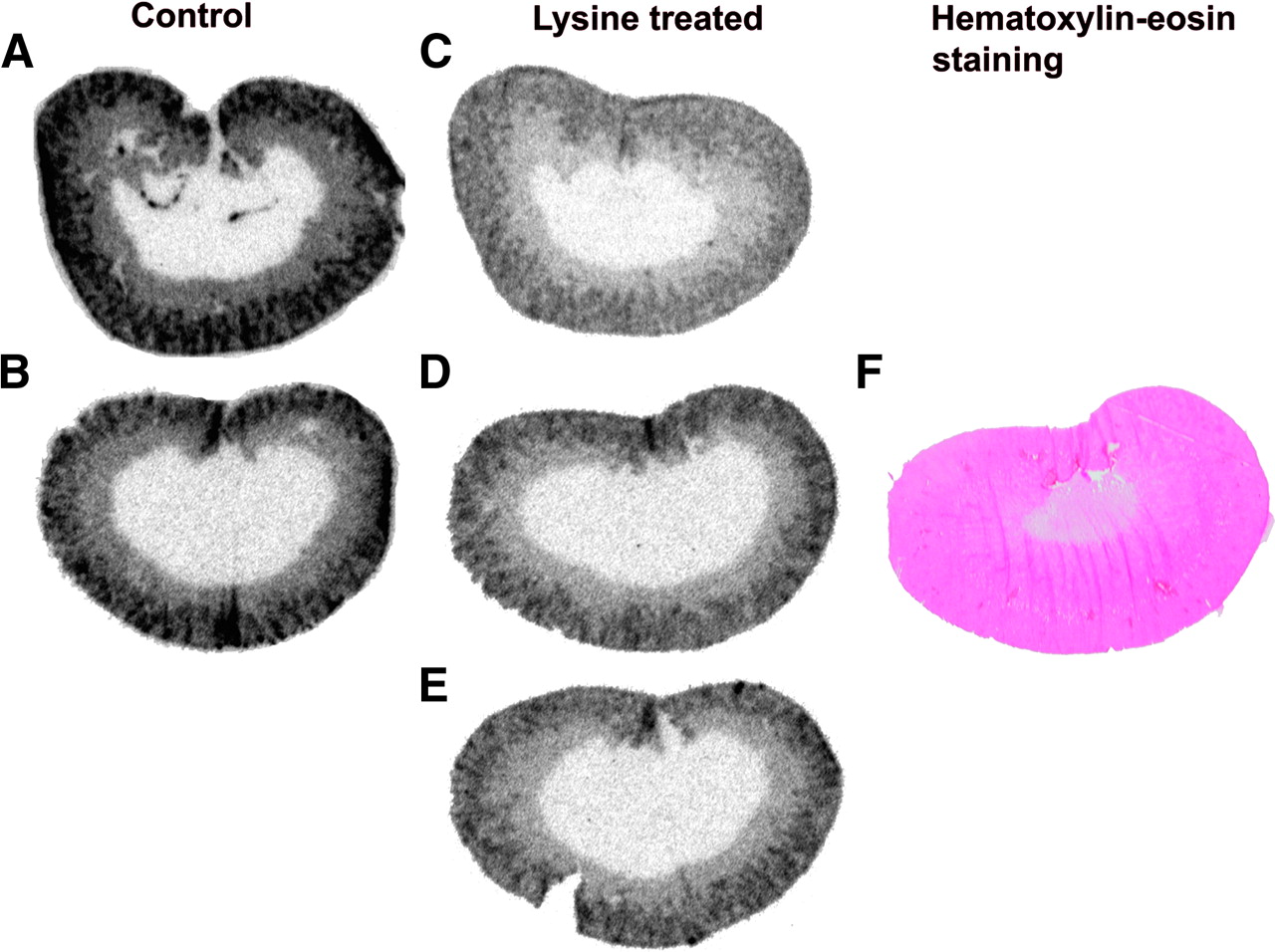
Ex vivo autoradiograms of renal tissue slices of control rats (A and B) and lysine-treated rats (C–E) 24 h after injection of [111In-DTPA]octreotide, 3 MBq/0.5 μg. Greatest reduction of renal radioactivity was seen in rats treated with intravenous lysine coinjected with tracer (C) or lysine (400 mg/kg) orally 60 min before tracer (D). Increasing the interval between oral lysine (400 mg/kg) and tracer to 120 min (E) did not lead to greater renal reduction. (F) Hematoxylin- and eosin-stained section adjacent to D shows high uptake of radioactivity in cortex and outer medulla but almost no uptake in inner medulla.
Ex Vivo Autoradiography
Autoradiograms of the control group and 3 experimental groups are shown in Figure 3. Histologic examination of hematoxylin- and eosin-stained sections adjacent to the autoradiography sections showed that radioactivity was taken up only in the cortex and outer medulla of the renal tissue.
DISCUSSION
In PRRT, the kidneys are the dose-limiting organ because of retention of radioactivity in the proximal tubules of the renal cortex (10). Based on external-beam radiation therapy data, an absorbed radiation dose to the kidneys of 23 Gy may lead to renal failure within 5 y in 5% of the patients. Therefore, the radiation dose limit to the kidneys in the various PRRT studies is mostly 23–27 Gy. By coinfusion of positively charged amino acids, such as lysine and arginine, the achieved radiation dose to the tumor can be higher without damaging the kidneys because of reduction of renal radioactivity (14). These infusions of an amino acid solution should take place over a 10-h period (16). Mostly, they are given within 4 h (14,15,19) because the procedure is highly labor intensive. Repeated oral administration of lysine/arginine would be more convenient for patients and hospital staff. We therefore investigated the effect of oral administration versus systemic administration of lysine on renal uptake of [111In-DTPA]octreotide in a rat model.
In this study, we administered d-lysine, 400 and 800 mg/kg, intravenously and orally. The maximum tolerated dose of this amino acid in mice is approximately 1.4-fold higher than the maximum tolerated dose of l-lysine (20) and could therefore safely be used in this study. Previous studies showed that d-lysine, 400 mg/kg, intravenously injected in rats led to about a 40% reduction in renal uptake (12,21) and that lysine/arginine combinations could not further the reduction of renal uptake in these rats (unpublished data). This study also confirmed this 40% renal reduction by comparing the control group and the intravenous group. Furthermore, this study showed that uptake of [111In-DTPA]octreotide in blood, spleen, pancreas, and adrenals was not significantly affected in rats treated orally with d-lysine, in comparison with those treated intravenously; however, renal uptake was reduced in all treated groups. The group that received 800 mg/kg orally and the group that received 400 mg/kg orally 60 min before the peptide showed a reduction of renal uptake comparable with that in intravenously treated rats. These results are confirmed by the ex vivo autoradiography images shown in Figure 3. The autoradiography data together with the hematoxylin- and eosin-stained sections showed that radioactivity was taken up only in the cortex and the outer medulla and that the reduction by lysine was therefore only in these sections of the kidney.
The group of Behr et al. (20) showed that lysine can effectively be used to reduce uptake of radioactivity in the kidneys when radiolabeled antibodies are applied and that this effect is not restricted to indium-labeled compounds. This group also showed that oral administration of l-lysine was as effective as intravenous administration at reducing renal uptake of these antibodies (20).
Several authors have reported that patients experienced nausea and vomiting when amino acids were infused (13,15,16,22). This adverse effect was related to the large amount of amino acids infused, the hyperosmolarity of the solution administered, and the rate of infusion (13).
Jamar et al. showed that infusion of amino acids over a period of up to 10 h could lead to a greater rate of reduction of renal uptake in patients (16) and that a large amount of amino acids could be given with relatively limited adverse effects (22). When an amino acid solution is administered orally, ingestion over a longer time can be realized more easily and, therefore, a greater renal reduction might be achieved.
CONCLUSION
The standard intravenous and oral methods of administering d-lysine equally reduce renal uptake of [111In-DTPA]octreotide in rats, with the oral administration preferably occurring 30–60 min before injection of the tracer. These results could offer a new clinical application for amino acid infusions before and during PRRT. The next step is to test this possibility in a clinical setting.
Footnotes
Received May 30, 2005; revision accepted Aug. 17, 2005.
For correspondence or reprints contact: Suzanne M. Verwijnen, BSc, Department of Nuclear Medicine, Erasmus MC, Dr. Molewaterplein 40, Room L208, 3015 GD Rotterdam, The Netherlands.
E-mail: s.m.verwijnen{at}erasmusmc.nl





{kind=link}
{kind=link}
{kind=link}