


Abstract
Small cell lung cancer (SCLC) is a tumor of neuroendocrine (NE) origin with very low survival rate. Somatostatin receptor scintigraphy using 111In-DTPA-octreotide (DTPA is diethylenetriaminepentaacetic acid) is a well-established method for the visualization of somatostatin receptor-expressing NE tumors. Recently, new combinations of radionuclides and somatostatin analogs have been investigated for therapeutic purposes. In this study, the somatostatin analog DOTA-Tyr3-octreotate (DOTA is 1,4,7,10-tetraazacyclododecane-N,N′,N″,N′″-tetraacetic acid), labeled with the medium-energy electron emitter 177Lu (maximal electron energy = 498 keV, half-life = 6.6 d), was used for radiation therapy of human SCLC in an animal model. Methods: Nude mice, bearing tumors from the human SCLC cell line NCI-H69, were injected intravenously with 177Lu-DOTA-Tyr3-octreotate. Groups of animals (n = 5 or 6) were injected with 45-, 60-, and 120-MBq fractions and two 45-MBq fractions 48 h apart. Furthermore, 1 control group was treated with unlabeled DOTA-Tyr3-octreotate and another control group was not treated. Results: In both control groups, the tumor volumes were increased 2-fold in approximately 5 d. Treatment with 177Lu-DOTA-Tyr3-octreotate resulted in marked tumor regression with statistically significant tumor volume reduction after 1 wk (P < 0.001). The tumor growth delay time was dependent on the amount of injected activity for the groups with single injections, 26 d for 60 MBq and 40 d for 120 MBq. The best therapeutic effect was obtained in mice injected with 2 fractions of 45 MBq. The relative tumor volume after 1 mo was 0.004 ± 0.004. Conclusion: Radiation therapy with 177Lu-DOTA-Tyr3-octreotate on SCLC-bearing mice was successful. Since the experiments were performed on a human SCLC cell line xenografted to nude mice, the results may be clinically relevant and treatment with 177Lu-DOTA-Tyr3-octreotate could be a treatment alternative in this tumor disease that normally has a dismal prognosis.
Systemic radiation therapy is an attractive modality to treat tumors because of the possibility to deliver high absorbed dose to the tumors, with tolerable radiation toxicity to normal tissues. Long-lived synthetic analogs to the peptide hormone somatostatin—for example, octreotide—bind to the somatostatin receptors (sstr). Five specific sstr subtypes, sstr1–sstr5, have been characterized, some of which may be overexpressed in different neuroendocrine (NE) tumor types—for example, carcinoid tumors (1,2). A high concentration of radiolabeled somatostatin analogs can thus be achieved in tumor tissue (3), which has been the basis for peptide receptor scintigraphy. Radiation therapy has been performed to date on patients with NE tumors using 131I-Tyr3-octreotide (4), 111In-DTPA-octreotide (DTPA is diethylenetriaminepentaacetic acid) (5–7), 90Y-DOTA-Tyr3-octreotide (DOTA is 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid) (7–12), 90Y-DOTA-lanreotide (13), or 177Lu-DOTA-Tyr3-octreotate (7,14).
Small cell lung cancer (SCLC) accounts for about 20% of all lung cancers (15). The tumor cells have a high proliferation rate and spread to lymph nodes and other organs—that is, brain, liver, and bone. The 5-y survival rate is <20% (15). There is an obvious need to find new therapeutic methods resulting in better survival. SCLC tumor cells express sstr (16), and 80%–100% can be visualized by octreotide scintigraphy (17–19). The established human SCLC cell line H69 has a high expression of sstr2 (20), and nude mice carrying H69 tumors can serve as an excellent experimental model for biodistribution and therapeutic studies using somatostatin analogs (21).
Since neither 90Y nor 111In is ideal for radiotherapy of small tumors (22), several biodistribution studies have recently been conducted in tumor-bearing animal models using different somatostatin analogs—for example, octreotide, Tyr3-octreotate, lanreotide, and vapreotide—labeled with low- or medium-energy electron emitters, such as 153Sm (maximal electron energy [βmax] = 808 keV, half-life [t1/2] = 46 h), 161Tb (βmax = 593 keV, t1/2 = 6.9 d), or 177Lu (βmax = 498 keV, t1/2 = 6.6 d) (23–26). Biodistribution studies in animal models have also been made for somatostatin analogs labeled with the high-energy electron emitter 188Re, the positron and electron emitter 64Cu, and the high-energy positron emitter 66Ga (27–29). The radionuclide pair 114mIn/114In is emitting both very low-energy Auger and conversion electrons and high-energy electrons and has been discussed for therapy of slowly growing sstr-positive tumors when bound to octreotide (30).
The somatostatin analog Tyr3-octreotate differs from octreotide by substitution of phenylalanine by tyrosine and threoninol is replaced by threonine. In this study, DOTA was used as bifunctional chelator because of its capability to bind to metal ions with extremely high stability (the metal ions bind to DOTA)—for example, Y(III) and lanthanides(III) (31). Furthermore, DOTA-Tyr3-octreotate has higher affinity to sstr2 than both DOTA-Tyr3-octreotide and DTPA-octreotide (32).
To our knowledge, no SCLC patient or animal model studies using 177Lu-DOTA-Tyr3-octreotate have been reported previously. Our biodistribution studies have shown high uptake of 177Lu-DOTA-Tyr3-octreotate in human SCLC xenografted to nude mice, making 177Lu-DOTA-Tyr3-octreotate a candidate radiopharmaceutical for therapy of SCLC (21). The aim of this study was to investigate the therapeutic response of 177Lu-DOTA-Tyr3-octreotate in male nude mice bearing SCLC tumors. We investigated the relationship between injected activity and tumor response and the difference in tumor response between 1 single injection and fractionated administration of the radiopharmaceutical.
MATERIALS AND METHODS
Radiopharmaceutical
DOTA-Tyr3-octreotate (synthesized by Jörg Schmitt, Institute of Nuclear Medicine, University Hospital, Basel, Switzerland) was dissolved in a solution containing sodium ascorbate, gentisic acid (2,5-dihydroxybenzoic acid), and 0.05 mol/L HCl (all chemicals from VWR International AB). The compound was stored in kits at −25°C until use. Each kit contained 40 μg DOTA-Tyr3-octreotate, 12.6 mg sodium ascorbate, 2.5 mg gentisic acid, and 0.1 mL HCl (21,25).
177LuCl3 was obtained from Missouri University Research Reactor with maximal specific activity of 740 MBq/μg. 177LuCl3 was diluted in 0.05 mol/L HCl to a concentration of 4.2–5.3 MBq/μL and incubated with the DOTA-Tyr3-octreotate solution for 30 min at 80°C to a specific activity of 29–33 MBq/μg DOTA-Tyr3-octreotate. Instant thin-layer chromatography (ITLC-SG; Gelman), with 0.1 mol/L sodium citrate (pH = 5.0; VWR International AB) as the mobile phase, was used to check the peptide-bound fraction. ITLC resulted in 96%–99% peptide-bound 177Lu.
The activity in the syringes was measured before and after administration of the radiopharmaceutical with a well-type ionization chamber (CRC-15R; Capintec), and the injected amount of activity was determined.
Animals
Four-week-old male BALB/c mice (Bommice; weight, 25 ± 0.5 g) were implanted subcutaneously in the neck with 2 × 107 cells of the human SCLC cell line NCI-H69 (ATCC HTB-119; American Type Culture Collection). Tumors were allowed to grow for 4 wk.
Therapeutic Study
Mice were each injected intravenously in a lateral tail vein with 177Lu-DOTA-Tyr3-octreotate in 0.1–0.2 mL isotonic saline. The first group (n = 5) was injected with 45 MBq, the second group (n = 5) with 60 MBq, and the third group (n = 6) with 120 MBq. The fourth group (n = 5) was injected with 2 fractions of 45 MBq each, given 48 h apart. One control group was treated with 4 μg unlabeled DOTA-Tyr3-octreotate (n = 7), which corresponds to the peptide amount given to the group treated with the highest activity. Another control group received no treatment (n = 5). Tumor volumes in different groups at the time of injection are shown in Table 1. The tumors in the groups treated with 45 or 2 × 45 MBq were approximately 1,000 mm3, and they were therefore compared with each other, whereas the tumors in the groups treated with 60 or 120 MBq were approximately 2,000 mm3.
Tumor Volume at Treatment Start
The Ethical Committee for Animal Research at Göteborg University approved the animal experiment. The animals were given autoclaved food and drinking water ad libitum. Tumor growth, animal condition, and body weight were determined at regular intervals. The mice were killed if they lost >10% of their original body weight or the tumor size was >20 mm in diameter.
The volume of the tumor, V, was determined, assuming an ellipsoid-shaped tumor:
 Eq. 1
Eq. 1
where the largest tumor diameter, a, and the perpendicular diameter, b, were measured with a ruler and the third diameter, c, was set to be similar to the smallest of the 2 measured diameters (i.e., b). The relative tumor volume was calculated as the ratio between the volume at time t and the volume at the time of injection (t = 0).
Biodistribution Study
The activity concentration Ctissue (percentage injected activity per gram [%IA/g]) was determined for 5 mice injected with 60 MBq and 3 mice injected with 120 MBq at 34 d after injection. The activity in the tumor and selected normal tissues were measured with a γ-counter (Wallac 1480, WIZARD 3″; Wallac Oy). Correction was made for detector background and for radioactive decay. The tumor-to-normal tissue activity concentration ratio, TNCtissue(t), was calculated. TNC values were also calculated at the time of minimal relative tumor volume. We assumed that the activity in the tumor and normal tissue was constant from this time to the time of measurement at 34 d after injection.
Dosimetry
Estimations of the absorbed dose in the tumor and normal tissue from 177Lu were made according to the MIRD formalism (33). The mean absorbed dose D̄tissue to a tissue with mass mtissue was estimated for various tissues as:
 Eq. 2
Eq. 2
with Ã, cumulated activity—that is, the total number of radioactive decays:
 Eq. 3
Eq. 3
where the product nE is the mean energy emitted per nuclear transformation and φ is the absorbed fraction. In these calculations, a uniform distribution of radioactivity was assumed and the product nE used was 147 keV (34). The absorbed fraction φ for bone marrow was set to be 0.5 because the thickness of the bone marrow was approximately 0.5 mm and the mean range of the 177Lu electrons was 0.3 mm (35). For all other organs the absorbed fraction used was 1. Only the absorbed dose contribution from electrons was included, and the absorbed dose originating from source organs other than the target organ was neglected. In these calculations, Atissue(t) from the study on the biodistribution of 177Lu-DOTA-Tyr3-octreotate 1–7 d after injection in a SCLC animal model (21) was used. A first-order exponential function was fitted to the measured activity at 1, 3, and 7 d after injection.
TNDtissue, the tumor-to-normal tissue absorbed dose ratio, was calculated as:
 Eq. 4
Eq. 4
Statistics
All results are expressed as mean ± SEM in each group. The Student t test was used to compare values between 2 groups, and ANOVA was used to compare the results between >2 groups. Probabilities of ≥95% (P ≤ 0.05) were considered statistically significant.
RESULTS
Therapeutic Study
The relative tumor volume values in control and treated groups are shown in Figure 1. For the group treated with unlabeled DOTA-Tyr3-octreotate, the tumor volume doubled in approximately 5 d. No difference was seen between the tumor growth for the group treated with unlabeled DOTA-Tyr3-octreotate and the untreated group. For the untreated tumors, no difference in the growth rate was observed between 100 and 3,000 mm3. All mice treated with 177Lu-DOTA-Tyr3-octreotate showed extensive tumor regression after 1 wk. None of the treated mice had weight loss or reduced physical activity.

Relative tumor volume in mice as function of time after 177Lu-DOTA-Tyr3-octreotate treatment with 45 MBq (▪) or 2 fractions of 45 MBq (○) (A) and as function of 60 MBq (•) or 120 MBq (□) (B) compared with control mice, either untreated (⋄) or given 4 μg unlabeled DOTA-Tyr3-octreotate (▴). Relative tumor volume was set to be 1 at treatment start. Data are given as mean ± SEM (n = 5–7). Note the logarithmic y-axis.
The tumors were most reduced in size at about 1–2 wk for the 45 MBq and 60 MBq groups, at about 3 wk for the group treated with 120 MBq, whereas the tumors in the 2 × 45 MBq group continued to decline during the period of study (34 d). Most of the treated tumors started to increase in volume 3–4 wk after treatment, and these animals were therefore sacrificed due to excessive tumor size after 34 d. The mean tumor growth delay time, defined as the time for the tumor volume to reach the same level as at the day of treatment, was shortest for the groups treated with 45 and 60 MBq, approximately 26 d. For the groups treated with 120 and 2 × 45 MBq the mean tumor growth delay time was extrapolated to about 40 and 50 d, respectively.
Statistically significant difference in relative tumor volume was obtained between the group treated with unlabeled DOTA-Tyr3-octreotate and all the 177Lu-treated groups after 7 d after injection and later (P < 0.001). Furthermore, statistically significant differences were obtained between the groups injected with 60 and 120 MBq at 19 d after injection and later (P < 0.05) and between the groups injected with 45 and 2 × 45 MBq at 31 d after injection (P < 0.05).
Biodistribution Study
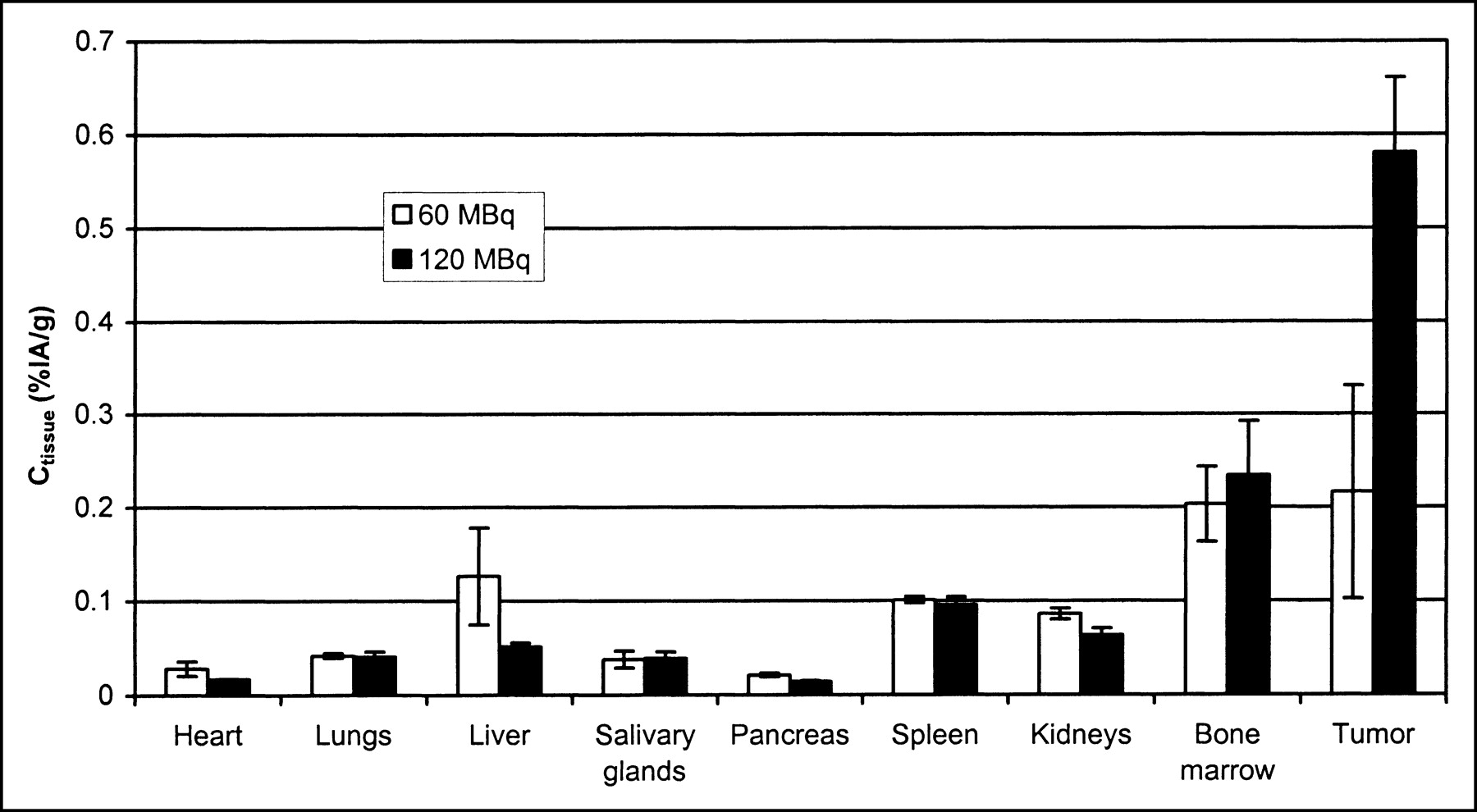
Figure 2 shows the results from the biodistribution study at 34 d after treatment. The activity concentration in the tumor at 34 d after injection was higher for the mice treated with 120 MBq (0.58 ± 0.08 %IA/g) than for the mice treated with 60 MBq (0.22 ± 0.07 %IA/g), P < 0.05. The tumors were larger at 34 d after injection in the 60 MBq group than in the 120 MBq group (relative volumes were 2.0 ± 0.1 and 0.42 ± 0.07, respectively).
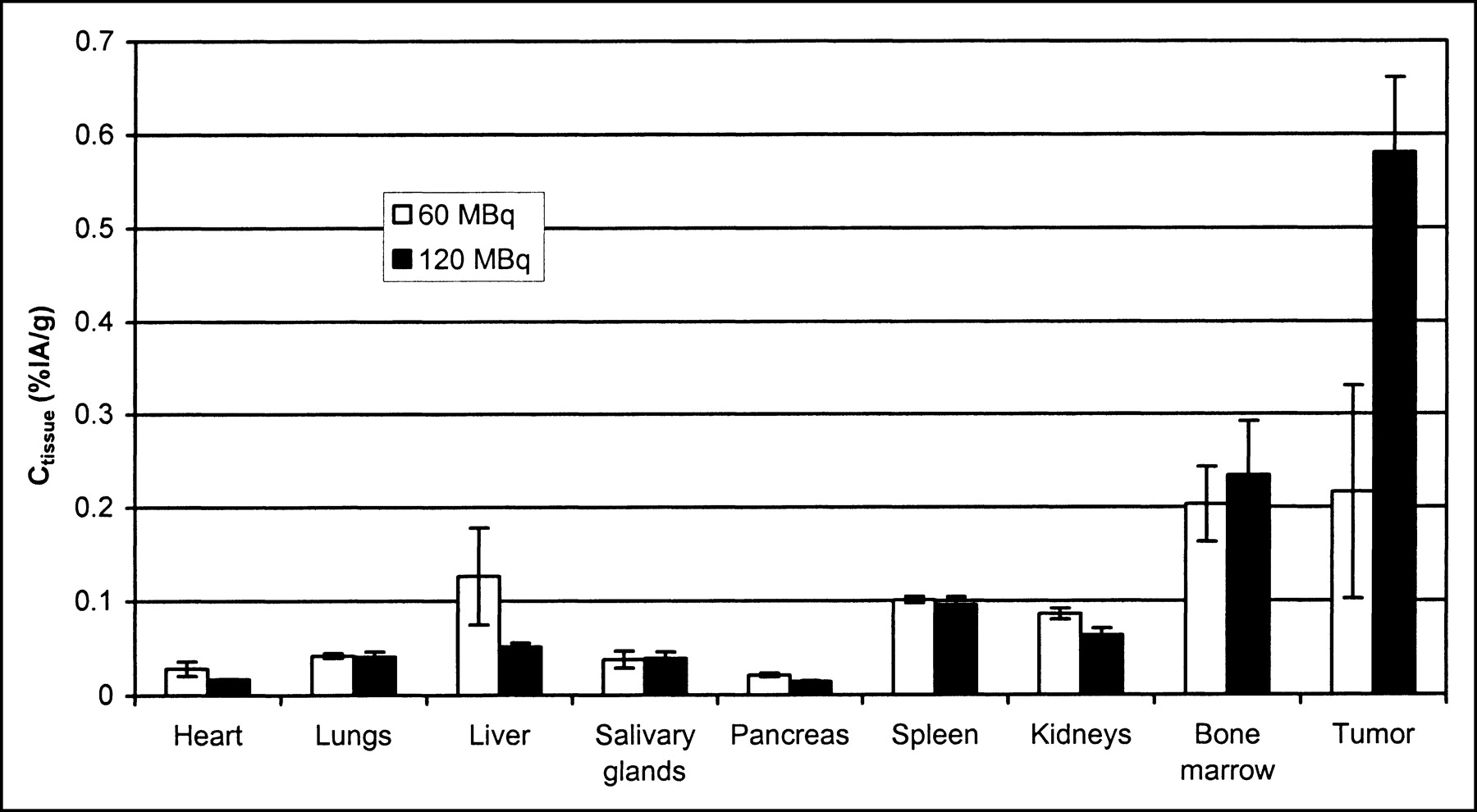
Activity concentration of 177Lu-DOTA-Tyr3-octreotate in tumor and normal tissue 34 d after injection. Data are expressed as mean ± SEM (n = 3–5).
TNC values at 34 d after injection are shown in Table 2. TNC values were higher for the 120-MBq group than for the 60-MBq group, with statistically significant differences found for all normal tissues, except bone marrow and the salivary glands. The calculated TNC values at the time of minimal relative tumor volume (15 d after injection for 60 MBq and 19 d after injection for 120 MBq) and TNC values for 1–7 d after injection, based on earlier published data in the same animal model (21), are also shown in Table 2. The tissues with the lowest TNC at 1–7 d after injection were the kidneys, lungs, bone marrow, pancreas, and adrenals. Note that TNC values at 1–7 d after injection were much higher for spleen, pancreas, liver, salivary glands, and bone marrow than TNC values at 34 d after injection. For the kidneys, lungs, and pancreas, TNC values were in the same range at 34 d after injection as at 1–7 d after injection. TNC values at 15 d after injection (60 MBq) and at 19 d after injection (120 MBq) were 5.0 and 3.3 times higher, respectively, than the corresponding values at 34 d after injection.
Figure 3A shows the relationship between activity concentration in tumor tissue at 34 d after injection and the start volume. The activity concentration at 34 d after injection was not correlated with the treatment volume at the start for the mice treated with 60 MBq. For the mice treated with 120 MBq, the highest activity concentration at 34 d after injection was found in the 2 tumors with the largest initial volumes, and the lowest activity concentration was found in the tumor with the smallest initial volume. Figures 3B and 3C show the activity concentration in tumor tissue versus tumor volume at 34 d after injection and versus relative volume, respectively. The best tumor regressions—that is, the lowest relative volumes at 34 d after injection—were found in the 2 tumors with the largest initial volumes, which were treated with 120 MBq.

Activity concentration of 177Lu-DOTA-Tyr3-octreotate in tumor tissue as function of tumor volume at treatment start (A), of tumor volume at 34 d after injection (dpi) (B), and of relative tumor volume 34 d after injection (C), with relative volume set to be 1 at treatment start.
Dosimetry
Dosimetric estimations of absorbed dose were made for organs with the highest uptake of 177Lu-DOTA-Tyr3-octreotate (Table 3). Tumor-to-normal tissue absorbed dose ratios (TND) were calculated according to Equation 4 and are also shown in Table 3. The absorbed dose per injected amount of activity to tumor tissue was determined earlier to be 290 mGy/MBq (21). If the mean activity concentration in the tumor at 34 d after injection was considered, this result was changed to 330 mGy/MBq. The absorbed dose to tumor was then 15, 20, and 40 Gy for the injected activity of 45, 60, and 120 MBq, respectively.
Absorbed Dose per Megabecquerel (MBq) Injected Activity and TND of 177Lu-DOTA-Tyr3-Octreotate
DISCUSSION
In this study, treatment with 177Lu-DOTA-Tyr3-octreotate resulted in marked tumor regression. When the groups with single injections were compared, the tumor volume response was better and the tumor growth delay time was longer for higher amounts of injected activity, indicating an absorbed dose–response relationship. However, the best tumor regression was obtained in the group given fractionated injections (2 × 45 MBq). The group treated with 120 MBq showed a less pronounced response than the group with fractionated therapy, even though the total injected activity was higher. This finding could be due to the larger amount of injected peptide in the group receiving 120 MBq (3.7 μg instead of 1.5 μg per fraction), which probably resulted in saturation of the sstr in the tumor tissue in accordance with previous studies (36,37). The difference between tumor volumes at the start can also affect the results. By using fractionation, saturation may be avoided, leading to an accumulated uptake of 177Lu in the tumor. Fractionation can effectively enhance therapeutic effects. One explanation for the increased effectiveness of such dose fractionation may be related to events after internalization of the receptor. After ligand binding, the ligand–receptor complex is internalized into the tumor cell. Intracellularly, the complex can be dissociated, and some receptors are recycled to the plasma membrane and are again available to the ligand (38). Furthermore, saturation of the sstr would lead to a somewhat lower activity concentration for the 120-MBq group, but the activity concentration was higher than that for the group treated with 60 MBq. Because of resumed tumor growth in the 60-MBq group 34 d after injection, the activity in the tumor was diluted, resulting in a reduced activity concentration. In this case, the saturation effect was surpassed by the therapeutic effect.
TNC values 1–7 d after injection, calculated from data in our earlier study (21), were evidently higher for the spleen, pancreas, liver, salivary glands, and bone marrow than the corresponding TNC values 34 d after injection, calculated from data in this study. This was due to a higher activity concentration in these tissues and a lower activity concentration in the tumor at 34 d after injection versus that at 1–7 d after injection. The activity concentration in the kidneys, lungs, and pancreas was also lower at 34 d after injection than that at 1–7 d after injection, resulting in TNC values in the same range at both time intervals. Different masses of peptide were used in the 2 studies, which could result in biodistribution differences. TNC values at the time of minimal relative tumor volume were higher than those at 1–7 d after injection for the lungs and kidneys. This finding is promising since the lungs and kidneys are at-risk organs. The activity concentration in the tumor was highest when the relative tumor volume was minimal, since no release of activity was assumed, resulting in higher TNC values for all organs, compared with the values at 34 d after injection. This assumed effect will be of therapeutic benefit and must be further evaluated in detail.
The dosimetric study by Lewis et al. (26) in rats with the rat pancreatic tumor CA20948 resulted in 91 mGy/MBq tumor dose after injection of 1.3 MBq 177Lu-DOTA-Tyr3-octreotate. In our model, the tumor dose per amount injected activity was higher, 330 mGy/MBq. A study by de Jong et al. (25) in the rat tumor model showed that 555 MBq 177Lu-DOTA-Tyr3-octreotate given as single injection resulted in 100% complete response. Because of the lower weight of the mice, 60 MBq (2 μg) given to a 25-g mouse is comparable to 555 MBq (24 μg) given to a 200- to 300-g rat. The 20-Gy tumor dose in the mouse model should be compared with 50 Gy in the rat model. To receive the same absorbed dose in our model and, hence, be able to compare the therapeutic response in the 2 animal models, therapy with several fractionations must be given in the SCLC mouse model.
The dosimetric calculations are based on the biodistribution study (21), in which each mouse received 0.7 μg peptide compared with 1.5–4.0 μg in this study. Saturation will result in a reduced tumor dose. The normal tissues at risk when administrating 177Lu-DOTA-Tyr3-octreotate in high amounts for radionuclide therapy are, above all, the kidneys and the bone marrow (7). In this study, the maximal absorbed doses to the kidneys and the bone marrow were calculated to be 13 and 1.9 Gy, respectively, in mice injected with 120 MBq. Because of the difficulty in determining the correct absorbed fraction for bone marrow, the calculated bone marrow dose remains uncertain. In a toxicity study by Lewis et al. (26), rats treated with up to 4.2 GBq/kg 177Lu-DOTA-Tyr3-octreotate showed a transient depression of white blood cell counts but no other significant hematologic changes. This level corresponds to 100 MBq given to a 25-g mouse.
Encouraging therapeutic results have also been obtained with Tyr3-octreotate labeled with other radionuclides such as 64Cu (28) and 153Sm (23) in different tumor-bearing animal models. The impressive results could be explained by very high affinity of sstr2 for Tyr3-octreotate (32). 177Lu-DOTA-Tyr3-octreotate has the highest tumor uptake of all somatostatin analogs tested so far and provides low-energy electrons appropriate for treatment of smaller tumor lesions. Furthermore, 177Lu has 2 low-abundance γ-emissions with energies optimal for imaging, which also allows dosimetric calculations.
CONCLUSION
This study shows that 177Lu-DOTA-Tyr3-octreotate can be an interesting alternative in the treatment of human SCLC. Other studies have shown promising results of 177Lu-DOTA-Tyr3-octreotate on other sstr2-positive NE tumors in both animals and patients (7,14,25). Since SCLC is difficult to cure with traditional therapy (i.e., external radiotherapy and chemotherapy), further evaluation of the use of 177Lu as an alternative radionuclide would be very interesting. Radiation from 177Lu-DOTA-Tyr3-octreotate can be delivered selectively to the primary tumor and smaller metastases. In patients with residual micrometastases, 177Lu-DOTA-Tyr3-octreotate could be given as completion radiation therapy in addition to the surgical treatment.
Acknowledgments
The authors thank Ann Wikström and Siw Tuneberg for excellent technical assistance. This study was supported by the Swedish Cancer Society (grants 3911 and 3427) and the Swedish Medical Research Council (grant 5520) and was done within the European Cooperation in the field of Science and Technology (COST B12 and D18). The support of one author by The Swiss National Foundation (grant 3100-100390) is acknowledged.
Footnotes
Received Nov. 12, 2003; revision accepted Feb. 25, 2004.
For correspondence or reprints contact: Anneli Schmitt, MSc, Department of Radiation Physics, Sahlgrenska University Hospital, S-413 45 Göteborg, Sweden.
E-mail: anneli.schmitt{at}radfys.gu.se





{kind=link}
{kind=link}
{kind=link}