


Abstract
A new treatment modality for inoperable or metastasized gastroenteropancreatic tumors is the use of radiolabeled somatostatin analogs. Initial studies with high doses of [111In-diethylenetriaminepentaacetic acid (DTPA)0]octreotide in patients with metastasized neuroendocrine tumors were encouraging, although partial remissions were uncommon. Another radiolabeled somatostatin analog that is used for peptide receptor radionuclide therapy (PRRT) is [90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA)0,Tyr3]octreotide. Various phase 1 and phase 2 PRRT trials have been performed with this compound. Despite differences in the protocols used, complete and partial remissions in most of the studies with [90Y-DOTA0,Tyr3]octreotide were in the same ranges, 10%–30%; these ranges were higher than those obtained with [111In-DTPA0]octreotide. Treatment with the newest radiolabeled somatostatin analog, [177Lu-DOTA0,Tyr3]octreotate, which has a higher affinity for the subtype 2 somatostatin receptor, resulted in complete or partial remissions in 30% of 76 patients. Tumor regression was positively correlated with a high level of uptake on OctreoScan imaging, a limited hepatic tumor mass, and a high Karnofsky performance score. Treatment with radiolabeled somatostatin analogs is a promising new tool in the management of patients with inoperable or metastasized neuroendocrine tumors. Symptomatic improvement may occur with all 111In-, 90Y-, or 177Lu-labeled somatostatin analogs that have been used for PRRT. The results obtained with [90Y-DOTA0,Tyr3]octreotide and [177Lu-DOTA0,Tyr3]octreotate are very encouraging in terms of tumor regression. Also, if kidney protective agents are used, the side effects of this therapy are few and mild, and the duration of the therapy response for both radiopharmaceuticals is more than 2 y. These data compare favorably with those for the limited number of alternative treatment approaches.
Neuroendocrine gastroenteropancreatic (GEP) tumors, which comprise pancreatic islet cell tumors, nonfunctioning neuroendocrine pancreatic tumors, and carcinoids, are usually slow growing. When these tumors have metastasized, treatment with somatostatin analogs results in reduced hormonal overproduction and symptomatic relief in most cases. Treatment with somatostatin analogs, whether or not in combination with α-interferon, however, is seldom successful in terms of CT- or MRI-assessed tumor size reduction (1).
A new treatment modality for inoperable or metastasized GEP tumors is the use of radiolabeled somatostatin analogs. The majority of GEP tumors possess somatostatin receptors and therefore can be visualized in vivo with the radiolabeled somatostatin analog [111In-diethylenetriaminepentaacetic acid (DTPA)0]octreotide (OctreoScan; Mallinckrodt Medical). A logical extension of this tumor visualization in patients therefore is to try to treat these patients with radiolabeled somatostatin analogs.
STUDIES WITH [111In-DTPA0]OCTREOTIDE
Initial studies with high doses of [111In-DTPA0]octreotide in patients with metastasized neuroendocrine tumors were encouraging, although partial remissions (PRs) were uncommon. Two of 26 patients who had GEP tumors, who were treated with high doses of [111In-DTPA0]octreotide, and who received total cumulative dosages of more than 20 GBq (550 mCi) had decreases in tumor size of 25%–50%, as measured on CT scans (2). None, however, had PRs (Table 1). In another study of patients with GEP tumors, PRs were reported in 2 of 26 patients with measurable disease (Table 1) (3). Both series included relatively high numbers of patients who were in poor clinical condition on study entry. Also, many had progressive disease (PD) on study entry. The most common type of toxicity in both series was bone marrow suppression (Table 2). Serious side effects consisted of leukemia and myelodysplastic syndrome (MDS) in 3 patients who had been treated with total cumulative dosages of >100 GBq (2.7 Ci) (and an estimated bone marrow radiation dosage of about 3 Gy) (2). One of these patients had also been treated with chemotherapy, which may have contributed to or caused this grave complication. Anthony et al. (3) reported renal insufficiency in 1 patient; this effect probably was not treatment related but likely was attributable to preexisting retroperitoneal fibrosis. Transient liver toxicity was observed in 3 patients with widespread liver metastases. Although in both series favorable effects on symptomatology were reported, CT-assessed tumor regression was observed only in rare cases. This finding is not surprising, as 111In-coupled peptides are not ideal for peptide receptor radionuclide radiotherapy (PRRT) because of the small particle range and therefore the lower tissue penetration range.
Tumor Responses in Patients with GEP Tumors and Treated with Various Radiolabeled Somatostatin Analogs
Side Effects in Patients with GEP Tumors and Treated with Various Radiolabeled Somatostatin Analogs
STUDIES WITH [90Y-DOTA0,Tyr3]OCTREOTIDE
Another radiolabeled somatostatin analog that is used for PRRT is [90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA)0,Tyr3]octreotide. Various phase 1 and phase 2 PRRT trials have been performed with this compound.
Otte et al. (4) and Waldherr et al. (5,6) reported on various phase 1 and phase 2 studies in patients with neuroendocrine GEP tumors. In their first reports, with a dose-escalating scheme of 4 treatment sessions up to a cumulative dosage of 6 GBq (160 mCi)/m2 and without renal protection with amino acid infusion for half of the patients, renal insufficiency developed in 4 of 29 patients (Table 2). The overall response rate in GEP tumor patients who were treated either with 6 GBq (160 mCi)/m2 (5) or, in a later study, with 7.4 GBq (200 mCi)/m2 in 4 doses (6), was 24% (Table 1). In a subsequent study, with the same dosage of 7.4 GBq (200 mCi)/m2 administered in 2 sessions, complete remission (CRs) and PRs were found in 33% of 36 patients (Table 1) (7). It should be emphasized, however, that this trial was not a randomized trial comparing 2 dosage schemes.
Chinol et al. (8) described dosimetric and dose-escalating studies with [90Y-DOTA0,Tyr3]octreotide with and without the administration of kidney-protective agents. No major acute reactions were observed up to an administered dose of 5.6 GBq (150 mCi) per cycle. Reversible grade 3 hematologic toxicity was found in 43% of patients injected with 5.2 GBq (140 mCi), which was defined as the maximum tolerated dose per cycle. None of the patients developed acute or delayed kidney nephropathy, although follow-up was short. PRs and CRs were reported by the same group for 28% of 87 patients with neuroendocrine tumors (9).
In a more detailed publication, Bodei et al. (10) reported the results of a phase 1 study of 40 patients with somatostatin receptor–positive tumors, of whom 21 had GEP tumors. Cumulative total treatment dosages ranged from 5.9 to 11.1 GBq (from 160 to 300 mCi) given in 2 treatment cycles. Six of 21 patients (29%) had tumor regression (Table 1). The median duration of the response was 9 mo.
Another study with [90Y-DOTA0,Tyr3]octreotide was a multicenter phase 1 study performed in Rotterdam, The Netherlands; Brussels, Belgium; and Tampa, Florida, in which 60 patients received escalating doses of up to 14.8 GBq (400 mCi)/m2 in 4 cycles or up to 9.3 GBq (250 mCi)/m2 in a single dose, without the maximum tolerated single dose being reached (11). The cumulative radiation dosage to the kidneys was limited to 27 Gy. All patients received amino acids concomitantly with [90Y-DOTA0,Tyr3]octreotide for kidney protection. Three patients had dose-limiting toxicity: 1 had liver toxicity, 1 had grade 4 thrombocytopenia (<25 × 109/L), and 1 had MDS. Four of 54 patients (8%) who received their maximum allowed dose had PRs, and 7 patients (13%) had minor responses (MRs) (25%–50% tumor volume reduction) (Table 1). The median time to progression in the 44 patients who had stable disease, MRs, or PRs was 30 mo.
Bushnell et al. (12) reported a favorable clinical response, as determined by a scoring system that included weight, a patient-assessed health score, a Karnofsky performance score, and tumor-related symptoms, for 14 of 21 patients who were treated with a total cumulative dosage of 13.3 GBq (360 mCi) of [90Y-DOTA0,Tyr3]octreotide in 3 treatment cycles.
Despite differences in the protocols used, CRs and PRs in most of the studies with [90Y-DOTA0,Tyr3]octreotide were in the same ranges, 10%–30%; these ranges were higher than those obtained with [111In-DTPA0]octreotide.
STUDIES WITH [177Lu-DOTA0,Tyr3]OCTREOTATE
The somatostatin analog [DTPA0,Tyr3]octreotate differs from [DTPA0,Tyr3]octreotide only in that the C-terminal threoninol is replaced with threonine. Compared with [DTPA0,Tyr3]octreotide, it shows improved binding to somatostatin receptor–positive tissues in animal experiments (13). Also, its DOTA-coupled counterpart, [DOTA0,Tyr3]octreotate, labeled with the β-and γ-particle–emitting radionuclide 177Lu, was reported to be very successful in terms of tumor regression and animal survival in a rat model (14). Reubi et al. (15) reported a 9-fold increase in the affinity for the subtype 2 somatostatin receptor of [DOTA0,Tyr3]octreotate compared with [DOTA0,Tyr3]octreotide and a 6- to 7-fold increase in affinity in a similar comparison of their yttrium-loaded counterparts.
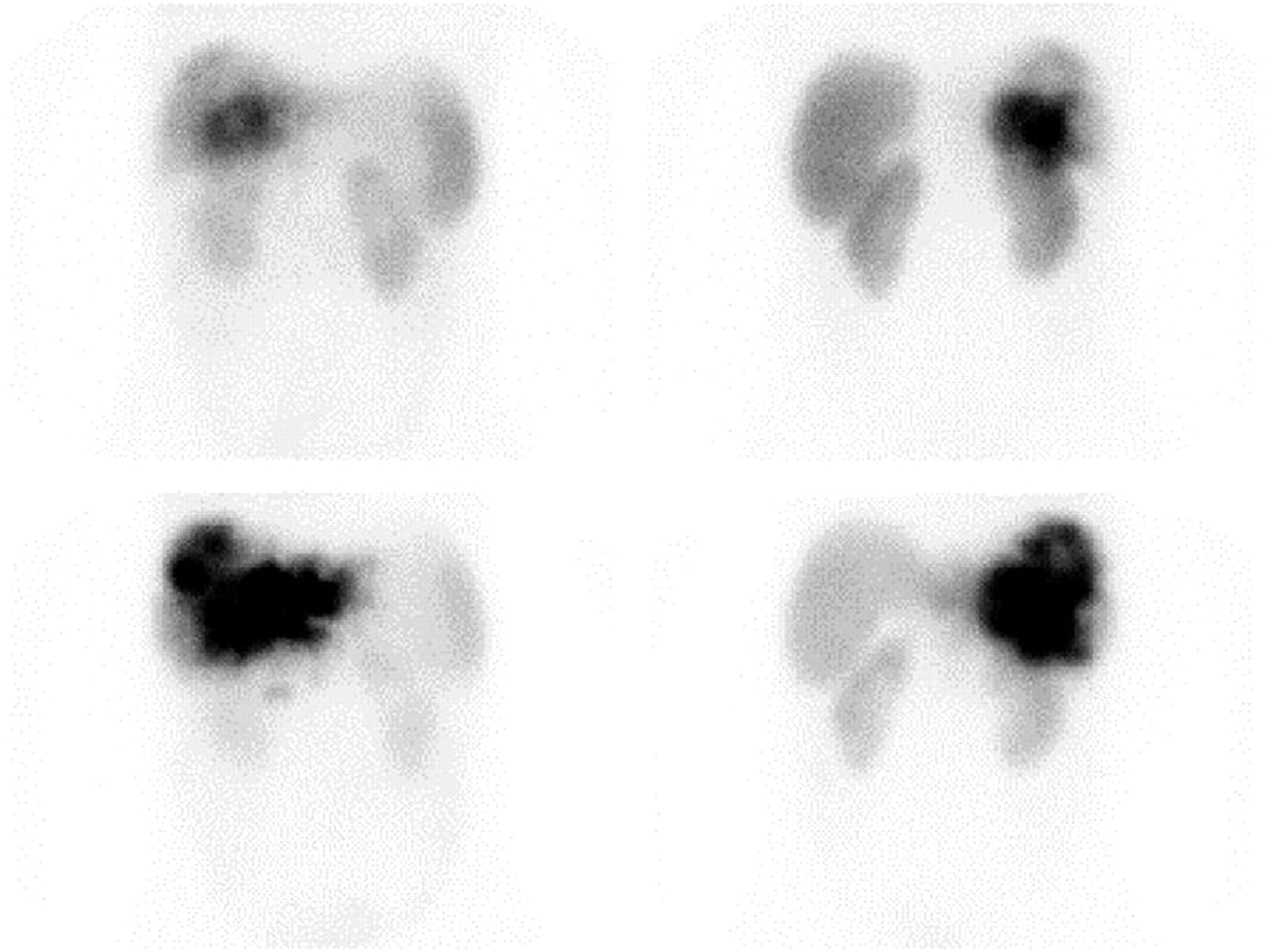
In a comparison in patients, it was found that the uptake of radioactivity, expressed as a percentage of the dose of [177Lu-DOTA0,Tyr3]octreotate injected, was comparable to that after [111In-DTPA0]octreotide injection in the kidneys, spleen, and liver but was 3- to 4-fold higher in 4 of 5 tumors (Fig. 1) (16). Therefore, [177Lu-DOTA0,Tyr3]octreotate potentially represents an important improvement because of the higher absorbed doses that can be achieved for most tumors with about equal doses to potentially dose-limiting organs and because of the lower tissue penetration range of 177Lu than of 90Y, a feature that may be especially important for small tumors.

Anterior abdominal images in a patient with liver metastases from a neuroendocrine pancreatic tumor. (Upper row) OctreoScan images 24 h after injection of 222 MBq (6 mCi) of [111In-DTPA0]octreotide; anterior (left) and posterior (right) abdominal views are shown. (Lower row) Posttherapy scans 1 d after injection of 7.4 GBq (200 mCi) of [177Lu-DOTA0,Tyr3]octreotate. Note the higher uptake in the metastases after [177Lu-DOTA0,Tyr3]octreotate injection. Physiologic uptake in the liver, spleen, and kidneys was seen on all scans.
The first treatment effects of [177Lu-DOTA0,Tyr3]octreotate therapy were described for 35 patients who had neuroendocrine GEP tumors and who had a follow-up at 3–6 mo after receiving the final dose (17). Patients were treated with 3.7, 5.6, or 7.4 GBq (100, 150, or 200 mCi) of [177Lu-DOTA0,Tyr3]octreotate, up to a final cumulative dosage of 22.2–29.6 GBq (600–800 mCi), at treatment intervals of 6–9 wk.
The effects of the therapy on tumor size could be evaluated for 34 patients. At 3 mo after the final administration, CR was found in 1 patient (3%), PRs were found in 12 patients (35%), stable disease was found in 14 patients (41%), and PD was found in 7 patients (21%), including 3 patients who died during the treatment period. The side effects of therapy with [177Lu-DOTA0,Tyr3]octreotate were few and mostly transient, with mild bone marrow suppression being the most common finding.
In a more recent update of this treatment in 76 patients with GEP tumors (18), CR was found in 1 patient (1%), PRs were found in 22 patients (29%), MRs were found in 9 patients (12%), stable disease was found in 30 patients (40%), and PD was found in 14 patients (18%) (Table 1). Six of 32 patients who had initially stable disease or tumor regression after therapy and who were also evaluated after 12 mo (mean from the start of therapy, 18 mo) had PD; in the other 26 patients, the tumor response was unchanged. The median time to progression was not reached at 25 mo from the start of therapy. Serious side effects in the entire group of patients who had been treated or who were being treated up to that time consisted of MDS in a patient who had had chemotherapy with alkylating agents 2 y before study entry and renal insufficiency in another patient who had had unexplained rises in serum creatinine concentrations in the year preceding the start of therapy and who had a urinary creatinine clearance of 41 mL/min at study entry.
Tumor regression was positively correlated with a high level of uptake on OctreoScan imaging, a limited hepatic tumor mass, and a high Karnofsky performance score.
COMPARISON OF VARIOUS TREATMENTS
Treatment with radiolabeled somatostatin analogs is a promising new tool in the management of patients with inoperable or metastasized neuroendocrine tumors. The results obtained with [90Y-DOTA0,Tyr3]octreotide and [177Lu-DOTA0,Tyr3]octreotate are very encouraging, although a direct, randomized comparison of the various treatments is lacking. Also, the reported percentages of tumor remission after [90Y-DOTA0,Tyr3]octreotide treatment vary, for several possible reasons. The administered doses and dosage schemes differ; some studies use dose-escalating schemes, whereas others use fixed doses. Alternatively, several patient and tumor characteristics determine treatment outcome; these include amount of uptake on OctreoScan imaging, estimated total tumor burden, and extent of liver involvement. Therefore, differences in patient selection may play an important role in determining treatment outcome.
This situation can be illustrated with 3 examples. In the combined data from 2 studies by Waldherr et al. (5,6) with 4 cycles of [90Y-DOTA0,Tyr3]octreotide treatment, the tumor response rate (CRs and PRs) was 24%. In their report on 33 patients to whom they administered 2 cycles of treatment, the response rate was 33% (Table 1) (7). In their first series of patients, 30 of 74 had either intestinal or bronchial carcinoids, which showed a response rate of 10%, whereas the other patients had either endocrine pancreatic tumors or neuroendocrine tumors of unknown origin, which regressed after therapy in 34%. In their second series, the response rates for endocrine pancreatic tumors and neuroendocrine tumors of unknown origin were the same (10/29 patients, or 34%), but because only 4 patients with carcinoids were included, the results seemed much more promising (Table 3). In a series of patients treated with [177Lu-DOTA0,Tyr3]octreotate, the response rate reported for the first group of 34 patients was 38% (17); in a later update with 76 patients, the response rate fell to 30% (18). Much of this change can be accounted for by the fact that in the first report, 3 gastrinoma patients (9% of total) who all had PRs were included, whereas in the later update, 5 gastrinoma patients (7% of total) who had PRs were included. Also, the relatively high percentage of tumor regression reported by the Milan group (G. Paganelli, written communication, April 2004) can be explained mainly by the large number of patients with endocrine pancreatic tumors whom they treated (Table 3). Other factors that may have contributed to the different results that were found in trials with the same compounds at various centers include differences in tumor response criteria and centralized versus decentralized follow-up CT scoring. Therefore, to establish which treatment scheme and which radiolabeled somatostatin analog or combination of analogs is optimal, randomized trials are needed.
Tumor Responses According to Tumor Type in Patients with GEP Tumors and Treated with Various Radiolabeled Somatostatin Analogs
OPTIONS FOR IMPROVING PRRT
From animal experiments it can be inferred that 90Y-labeled somatostatin analogs may be more effective for larger tumors, whereas 177Lu-labeled somatostatin analogs may be more effective for smaller tumors, but their combination may be the most effective (19). Therefore, in addition to comparisons between radiolabeled octreotate and octreotide and between somatostatin analogs labeled with 90Y or 177Lu, PRRT with combinations of 90Y- and 177Lu-labeled analogs should be evaluated.
In addition to combinations of analogs labeled with various radionuclides, future directions for improving this type of therapy should include efforts to upregulate somatostatin receptor expression on tumors as well as studies of the effects of the use of radiosensitizers.
CONCLUSION
Treatment with radiolabeled somatostatin analogs is a promising new tool in the management of patients with inoperable or metastasized neuroendocrine tumors. Symptomatic improvement may occur with all 111In-, 90Y-, or 177Lu-labeled somatostatin analogs that have been used for PRRT. The results obtained with [90Y-DOTA0,Tyr3]octreotide and [177Lu-DOTA0,Tyr3]octreotate are very encouraging in terms of tumor regression. Also, if kidney-protective agents are used, the side effects of this therapy are few and mild, and the duration of the therapy response for both radiopharmaceuticals is more than 2 y. These data compare favorably with those for the limited number of alternative treatment approaches.
Footnotes
Received May 11, 2004; revision accepted Aug. 13, 2004.
For correspondence or reprints contact: Dik J. Kwekkeboom, MD, Department of Nuclear Medicine, Erasmus Medical Center, University Hospital Rotterdam, Dr. Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.
E-mail: d.j.kwekkeboom{at}erasmusmc.nl
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Bicyclic Peptides as a New Modality for Imaging and Targeting of Proteins Overexpressed by Tumors
- Quality of Life in Patients with Metastatic Gastroenteropancreatic Neuroendocrine Tumors Receiving Peptide Receptor Radionuclide Therapy: Information from a Monitoring Program in Clinical Routine
- A Modular Dual-Labeling Scaffold That Retains Agonistic Properties for Somatostatin Receptor Targeting
- Parametric Net Influx Rate Images of 68Ga-DOTATOC and 68Ga-DOTATATE: Quantitative Accuracy and Improved Image Contrast
- Comparison of the Therapeutic Response to Treatment with a 177Lu-Labeled Somatostatin Receptor Agonist and Antagonist in Preclinical Models
- Dose Response of Pancreatic Neuroendocrine Tumors Treated with Peptide Receptor Radionuclide Therapy Using 177Lu-DOTATATE
- Endocrine Tumours: Epidemiology of malignant digestive neuroendocrine tumours
- Study of the Impact of Tissue Density Heterogeneities on 3-Dimensional Abdominal Dosimetry: Comparison Between Dose Kernel Convolution and Direct Monte Carlo Methods
- Response and Long-Term Control of Bone Metastases After Peptide Receptor Radionuclide Therapy with 177Lu-Octreotate
- Altered Biodistribution of Somatostatin Analogues After First Cycle of Peptide Receptor Radionuclide Therapy
- Phase I Trial of 90Y-DOTATOC Therapy in Children and Young Adults with Refractory Solid Tumors That Express Somatostatin Receptors
- 68Ga-DOTATATE PET/CT for the Early Prediction of Response to Somatostatin Receptor-Mediated Radionuclide Therapy in Patients with Well-Differentiated Neuroendocrine Tumors
- Functional Imaging of Neuroendocrine Tumors: A Head-to-Head Comparison of Somatostatin Receptor Scintigraphy, 123I-MIBG Scintigraphy, and 18F-FDG PET
- 68Ga-DOTANOC PET/CT Clinical Impact in Patients with Neuroendocrine Tumors
- Somatostatin receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors
- A Comparison of 68Ga-DOTATATE and 18F-FDG PET/CT in Pulmonary Neuroendocrine Tumors
- High-resolution genomic profiling reveals gain of chromosome 14 as a predictor of poor outcome in ileal carcinoids
- Treatment of Metastatic Carcinoid Tumors With Radiolabeled Biologic Molecules
- Tumor Receptor Imaging
- Utility of Radiolabeled Somatostatin Receptor Analogues for Staging/Restaging and Treatment of Somatostatin Receptor-Positive Pediatric Tumors
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- Renal Uptake of Radiolabeled Octreotide in Human Subjects Is Efficiently Inhibited by Succinylated Gelatin
- Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues
- Long-Term Follow-Up of Renal Function After Peptide Receptor Radiation Therapy with 90Y-DOTA0,Tyr3-Octreotide and 177Lu-DOTA0, Tyr3-Octreotate
- Patient-Specific Dosimetry in Predicting Renal Toxicity with 90Y-DOTATOC: Relevance of Kidney Volume and Dose Rate in Finding a Dose-Effect Relationship