


Abstract
Peptide receptor–mediated radiotherapy of neuroendocrine and other somatostatin receptor–positive tumors with radiolabeled somatostatin analogs has been applied in several experimental settings. The kidneys are the organs responsible for dose-limiting toxicity attributable to the retention of radiolabeled octreotide in the renal cortex, leading to a relatively high radiation dose that may result in irreversible loss of kidney function. The administration of basic amino acids reduces renal uptake but does have significant side effects. We observed that gelatin-based plasma expanders induced tubular low-molecular-weight proteinuria in healthy volunteers, suggesting that components in these solutions can interfere with the tubular reabsorption of proteins and peptides. Here, we studied the effects of infusion of low doses of the plasma expander succinylated gelatin (GELO) on the renal uptake of 111In-labeled octreotide (111In-OCT). Methods: Five healthy volunteers were given 111In-OCT, first in combination with normal saline and 2 wk later in combination with GELO. Scintigraphic images of the kidneys as well as blood and urine samples were analyzed. To exclude a nonspecific hemodynamic effect of the plasma expander, the procedure was repeated with 5 other volunteers who received the carbohydrate-based plasma expander hydroxyethyl starch (HES). Results: Low doses of GELO were able to effectively reduce the kidney retention of 111In-OCT. The renal radiation dose was significantly reduced by 45% ± 10% (mean ± SD) (P = 0.006), whereas HES showed no significant effect (0% ± 12%). The infusion of GELO did not cause any side effects. Conclusion: GELO effectively reduces the renal uptake of 111In-OCT. In contrast to currently used mixtures of amino acids, GELO does not cause any side effects.
Radiolabeled somatostatin derivatives, such as 90Y-(1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid [DOTA])0-Tyr3-octreotide (DOTATOC) and 177Lu-DOTA0-Tyr3-octreotate (DOTATATE), are used for experimental peptide receptor–mediated radiotherapy (PRRT) in patients with somatostatin receptor–positive tumors (1). These hydrophilic radiolabeled peptides are cleared from the body predominantly by the kidneys. As most peptides demonstrate a relatively high level of retention in the renal cortex, the kidneys consequently receive a relatively high radiation dose, and chronic renal damage can occur. In some cases, bone marrow toxicity is observed, but in most cases, radiation nephritis is responsible for dose-limiting toxicity in PRRT (1–3).
Radiolabeled octreotide is filtered through glomeruli and partly reabsorbed in proximal tubular cells (4). The reabsorption recently was shown to be mediated by megalin receptors (5,6). To enhance the therapeutic window, solutions of lysine or arginine are coinfused to block the reabsorption of octreotide (2,7). The positive charges on these basic amino acids interfere with the interaction of peptides with the receptor on the proximal tubular cells and thus block receptor-mediated endocytosis. However, large amounts of these amino acids in hyperosmolar solutions are needed to effectively achieve lower levels of renal uptake, resulting in side effects such as hyperkalemia, vomiting, volume overload, and local irritation at the injection site (8). Furthermore, lysine itself can cause renal tubular toxicity (9,10).
We recently demonstrated that the infusion of a low dose of the polypeptide-based succinylated gelatin (GELO) plasma expander Gelofusine (Braun) or Haemaccel (Hoechst) increased the urinary excretion of the small peptide β2-microglobulin (11). The data indicated that the effect was caused by competitive inhibition of the tubular reabsorption of low-molecular-weight proteins (11). In the present study, we assessed whether the coinfusion of GELO also influences the renal uptake of 111In-octreotide (111In-OCT) in healthy volunteers.
MATERIALS AND METHODS
Subjects
Ten healthy volunteers were recruited for the present study. Inclusion criteria were age of 18 y or over and normal renal function, defined as a creatinine clearance of >90 mL/min by the formula of Cockcroft and Gault (12). Exclusion criteria were hypertension, the use of any medication affecting renal function, known hypersensitivity to any of the substances used, pregnancy, and lactation. The present study was approved by the institutional review board of the Radboud University Nijmegen Medical Centre. Written informed consent was obtained from all volunteers.
GELO Group
To assess the effect of GELO (Gelofusine) on the renal uptake of [111In-diethylenetriaminepentaacetic acid-d-Phe1]-octreotide (111In-OCT; Octreoscan; Tyco Mallinckrodt), 2 series of measurements were obtained for 5 subjects (2 men and 3 women; age [mean ± SD], 48 ± 5 y; creatinine clearance, 100 ± 3 mL/min). Baseline renal uptake and blood and urine 111In-OCT concentrations were measured during and after infusion with normal saline (0.9% NaCl). Two weeks later, the procedure was repeated with GELO.
Subjects were pretreated with a bolus infusion of either saline or GELO (1 mL per kilogram of body mass over 10 min). Next, 111In-OCT (50 MBq, 5 μg of peptide) was administered. Infusion of normal saline or GELO was continued at a rate of 0.02 mL/kg/min over 3 h. Blood pressure and heart rate were monitored during infusion. During the 48 h after the injection of 111In-OCT, posterior planar images of the kidney region were recorded in a 128 × 128 matrix with a γ-camera (ECAM; Siemens) equipped with medium-energy collimators by use of both 111In photon peaks (172 and 245 keV) with 20% symmetric energy windows. Images were recorded immediately and at 4, 24, and 48 h after injection (15 min per image). A sample containing a known fraction of the injected dose was placed in the field of view for reference purposes.
Blood samples were drawn through an indwelling intravenous cannula in the contralateral arm at 2, 10, 20, 40, 60, and 90 min and at 2, 4, and 24 h after injection.
Urine was collected during the 24 h after the injection in two 3-h intervals, followed by 6- and 12-h intervals. Radioactivity in blood and urine samples was measured with an automatic γ-counter (Wizard 1480; Wallac).
Hydroxyethyl Starch (HES) Group
As GELO is a pharmaceutical agent registered for plasma expansion in hypovolemia and therefore may induce changes in hemodynamics, a nongelatin plasma expander (HES; Voluven; Fresenius) was studied with a group of 5 healthy volunteers (5 women; age [mean ± SD], 31 ± 15 y; creatinine clearance, 104 ± 9 mL/min). The procedure described above also was used for this group, except that at 2 wk after the baseline measurements, HES was infused instead of GELO.
Image Analysis
Regions of interest were drawn around the kidneys and the reference sample. The kidney regions of interest were copied and placed adjacent to the kidneys to determine background activity. The percentage injected dose (%ID) in both kidneys was calculated as previously described (13): {[counts in the left kidney – (0.66 × counts in the left background)] + [counts in the right kidney – (0.66 × counts in the right background)]}/(counts in the reference/%ID in the reference). A graph of %ID in both kidneys against time was plotted. The areas under the curve at up to 48 h after injection were calculated by use of the Prism 4 software package (GraphPad Software).
Statistical Analysis
Data were analyzed with paired and unpaired t tests by use of the Prism 4 software package. The level of significance was set at 0.05.
RESULTS
Less than 420 mL of normal saline, GELO, or HES was infused into each subject. GELO contains 40 g of succinylated gelatin per liter; the total amount administered averaged 12.9 g (SD, 2.3). Normal saline, GELO, and HES did not induce any significant changes in blood pressure or heart rate and did not cause any other clinical side effects.
As shown in Figure 1, compared with the infusion of normal saline, the infusion of GELO significantly reduced the renal uptake of 111In-OCT. The area under the curve decreased by 45% (SD, 10%) (P = 0.006). Baseline renal 111In-OCT uptake over time in the GELO group was similar to that in the HES group (P = 0.36). However, in sharp contrast to the observations for the GELO group, HES did not alter the renal uptake of 111In-OCT, as shown in Figure 2. No difference in the area under the curve was observed after infusion of either normal saline or HES (mean, 0%; SD, 12%) (P = 0.85). Figure 3 shows the effects of GELO and HES on renal uptake.
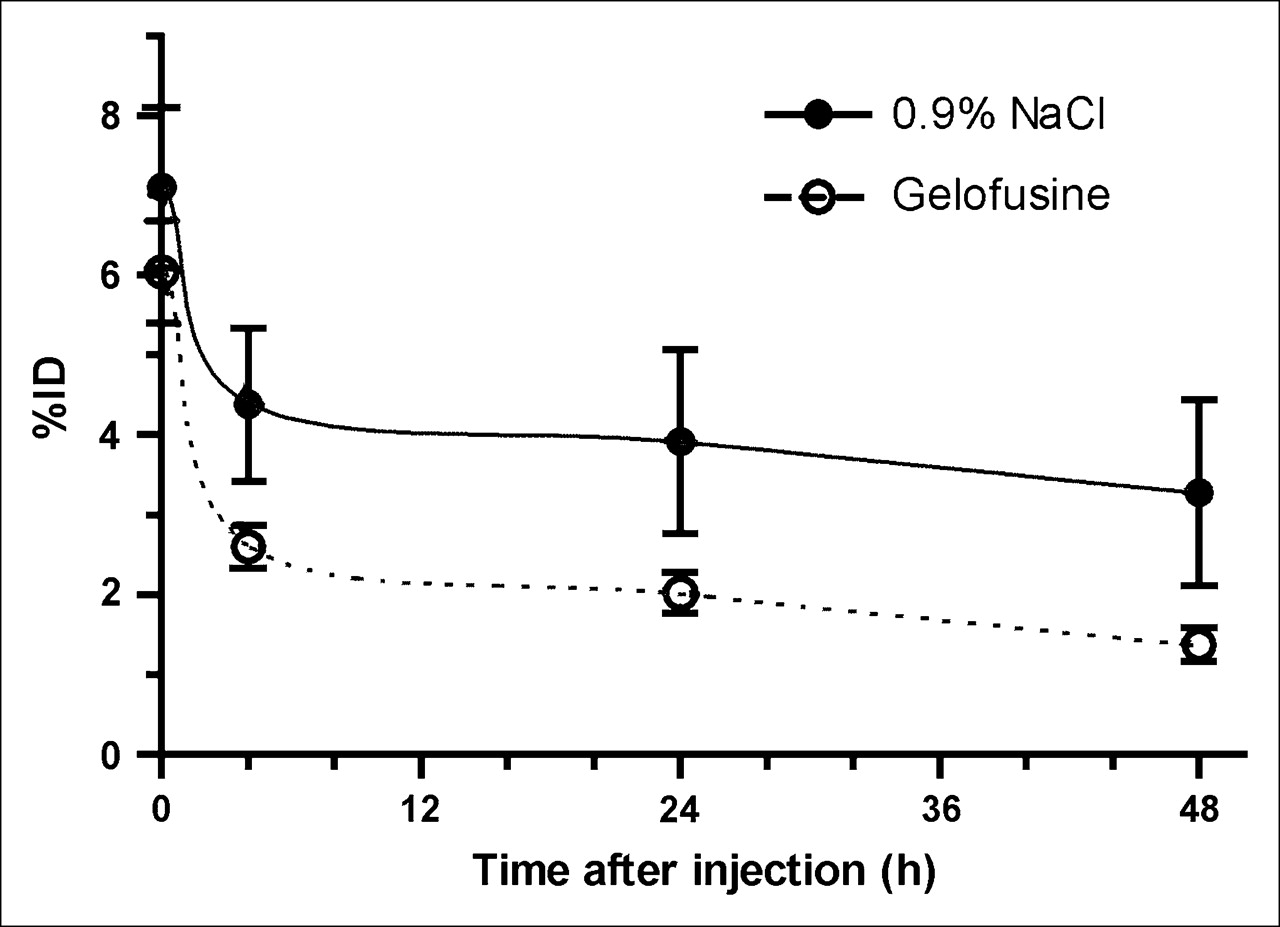
%ID (mean ± SD) of 111In-OCT over time in kidneys at baseline or after infusion of GELO. Significantly less 111In-OCT was retained in kidneys after GELO infusion than after normal saline infusion (P = 0.006 for difference in areas under curves).
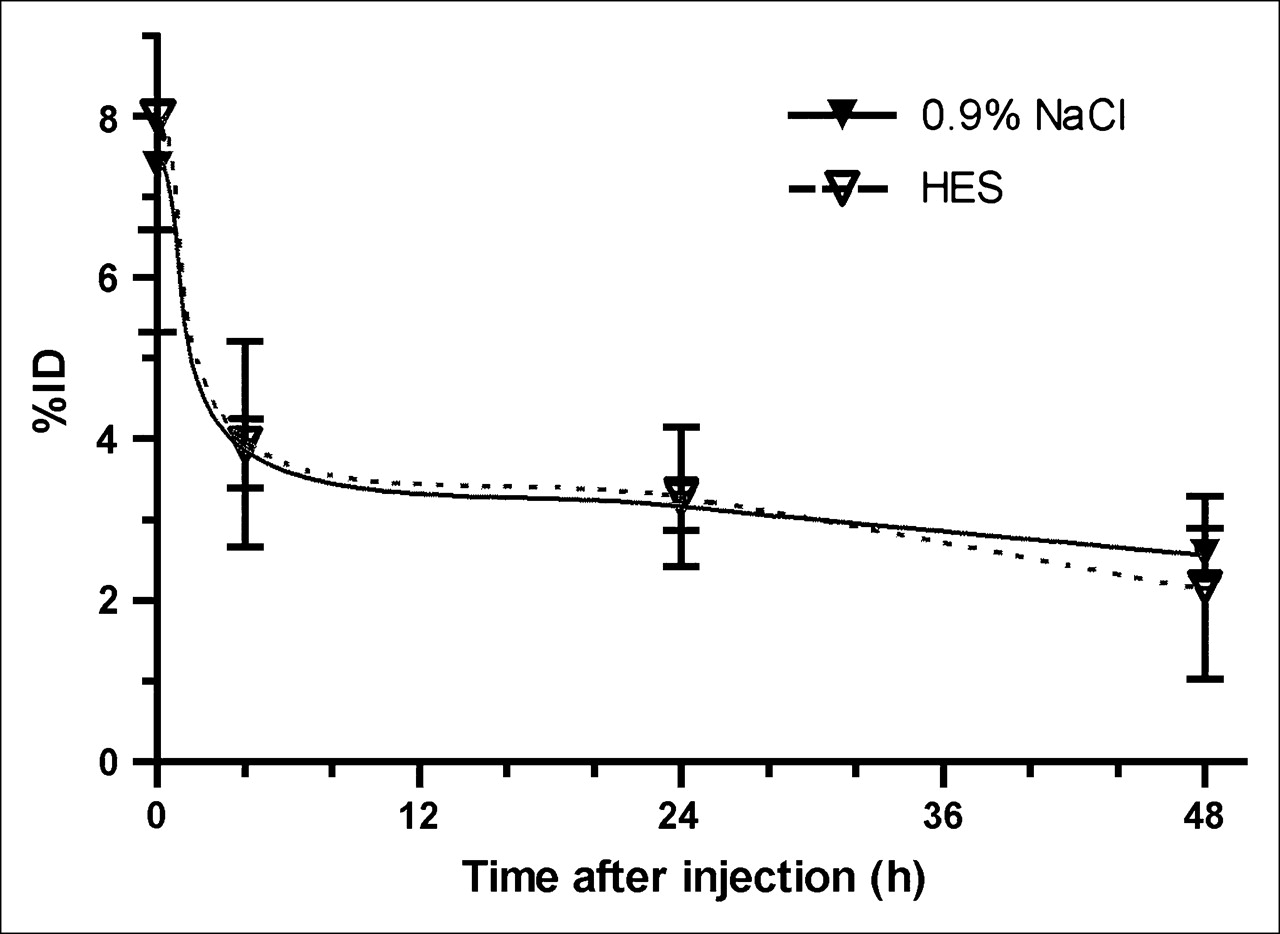
%ID (mean ± SD) of 111In-OCT over time in kidneys at baseline or after infusion of HES. No statistically significant difference was observed between infusion of normal saline and infusion of HES.
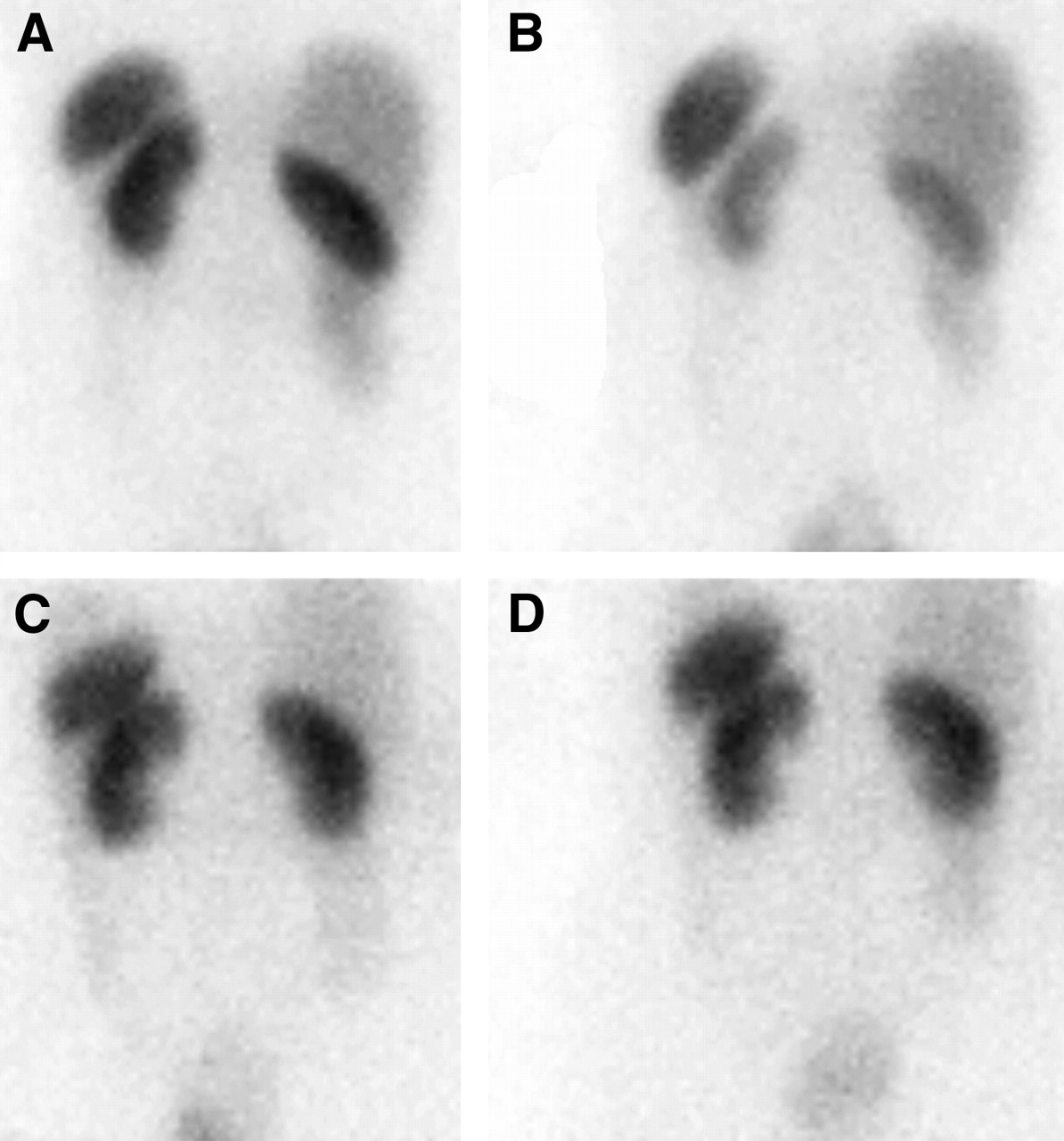
Posterior images of kidney region 24 h after injection of 111In-OCT at baseline (A) and after GELO infusion (B) and at baseline (C) and after HES infusion (D). GELO resulted in renal uptake levels lower than those at baseline, whereas HES had no effect.
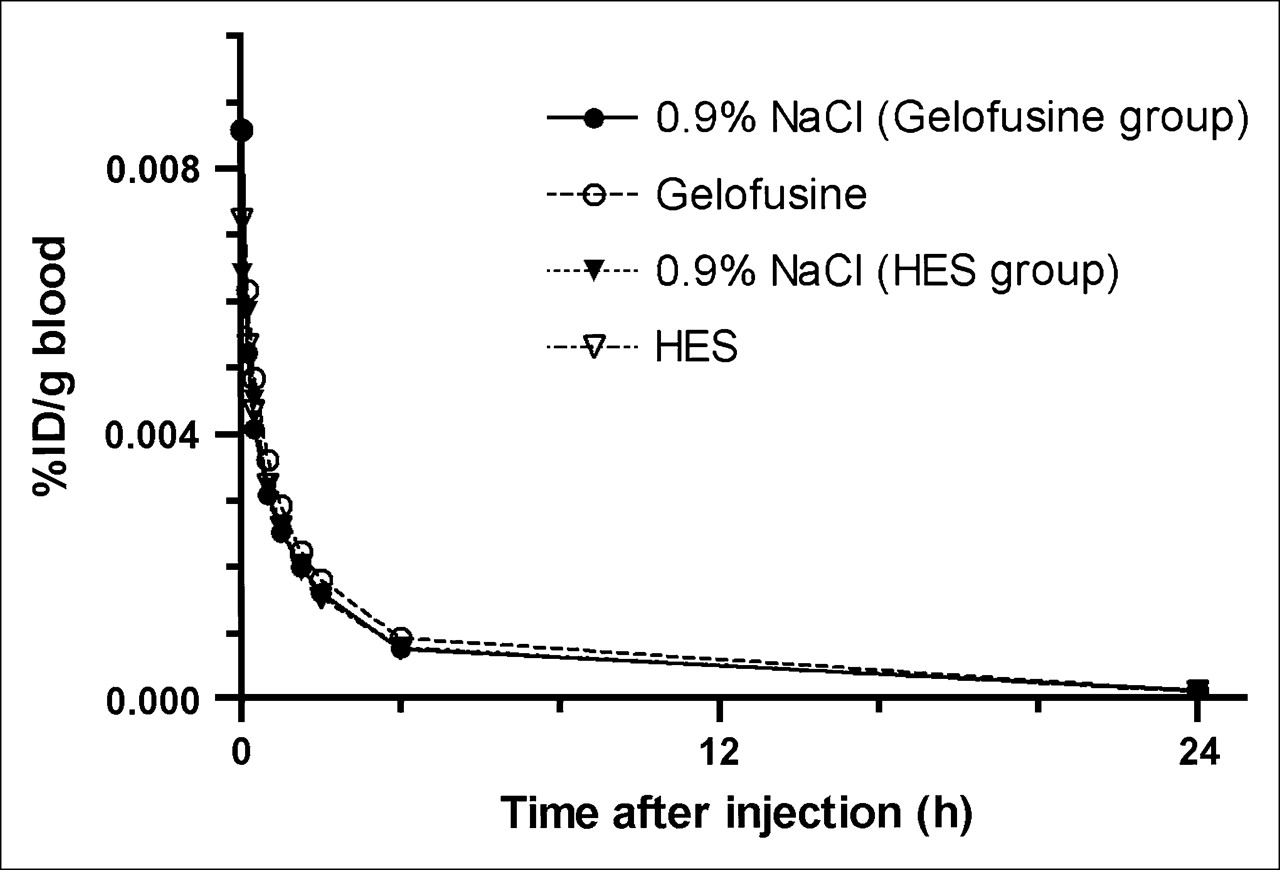
111In-OCT was cleared rapidly from the blood. After 4 h approximately 5% and after 24 h approximately 0.6% of the initial radioactivity was still present in the circulation. As shown in Figure 4, compared with the infusion of normal saline, the administration of GELO or HES did not affect the clearance of 111In-OCT from the blood.
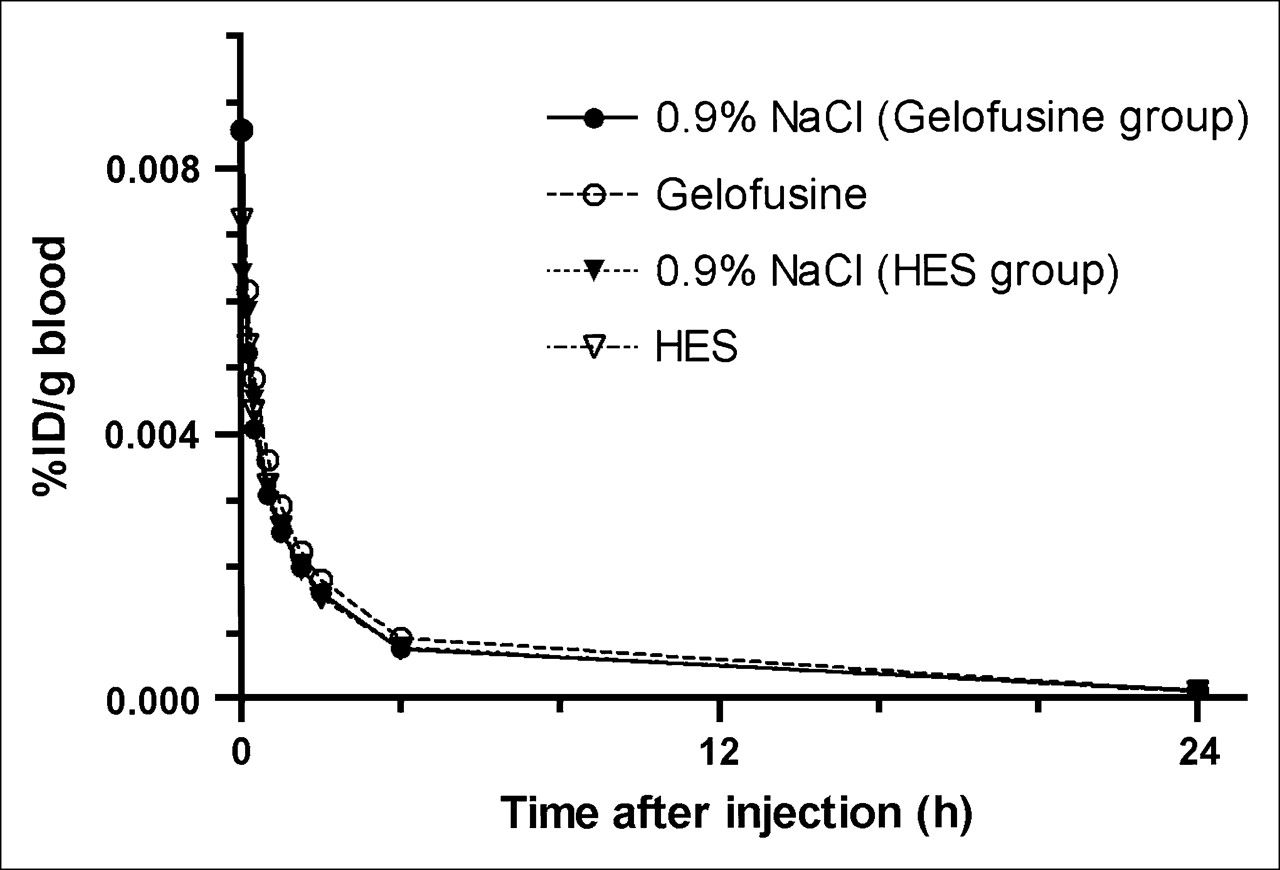
Clearance of 111In-OCT from blood over time. No statistically significant differences were observed between groups.
The excretion of 111In-OCT in urine ranged from 40 to 50 %ID (SD, 8–10 %ID) in the first 3 h after injection and from 76 to 87 %ID (SD, 7–15 %ID) in the first 24 h. No statistically significant differences in urine excretion attributable to infusion of GELO or HES were observed.
DISCUSSION
In the present study, the infusion of relatively small amounts of GELO (<420 mL) effectively reduced the renal retention of 111In-OCT by 45%. Because the infusion of similar amounts of the carbohydrate-based plasma expander HES did not affect the renal retention of 111In-OCT, the reduction cannot be attributed to nonspecific renal or vascular effects as a result of plasma expansion. The absence of a hemodynamic effect is supported further by the absence of changes in blood pressure.
Neither GELO nor HES altered clearance from the blood or 24-h renal excretion of 111In-OCT. Because renal retention was reduced after the infusion of GELO, one would have expected increased urinary excretion. The absence of a significant effect on the excreted fraction probably was attributable to the relatively small %ID retained in the kidneys at any given time point (approximately 5 %ID) compared with the large fraction of total excreted activity and its relatively large SD (approximately 85 ± 11 %ID in the first 24 h). The latter may have been caused by volunteers who failed to collect all urine over 24 h.
The mechanism of retention of radiolabeled peptides in the kidneys after intravenous administration is relatively well understood. In general, peptides with a molecular weight of less than 20 kDa are filtered readily in the glomeruli and subsequently reabsorbed effectively in the cells of the proximal renal tubules. Peptides are reabsorbed by the tubular cells via receptor-mediated endocytosis and pinocytosis. After internalization, the labeled peptides are degraded in the lysosomes, and the metabolites are transferred mainly back into the bloodstream. However, the radioactive metabolite of peptides labeled with radiometals, the radiolabeled diethylenetriaminepentaacetic acid- or DOTA-conjugated amino acid, cannot leave the lysosomes and remains trapped in the proximal tubular cells. de Jong et al. recently showed that 111In-OCT reuptake in kidney proximal tubular cells is mediated by megalin receptors (6). This receptor is involved in the reuptake of several low-molecular-weight proteins, including β2-microglobulin.
Preclinical studies have shown that the infusion of lysine or arginine can block the tubular reabsorption of radiolabeled peptides, thereby reducing the renal retention of these peptides (14–16). Studies with patients have confirmed that this approach is also clinically feasible, and it has become part of standard PRRT protocols for patients (4,7,8,17). However, most of these protocols have significant side effects. The infusion of large amounts of cationic amino acids may induce vomiting as well as metabolic changes leading to hyperkalemia, which can cause serious cardiac problems. To prevent the administration of solutions with potentially dangerous high osmolarity, large volumes need to be infused. The resulting high-volume load may cause cardiac problems, especially in patients with cardiac compromise (8,18). Current studies are focusing on reducing these side effects and selecting a protocol that is clinically acceptable.
Although a decrease in 111In-OCT activity in the kidneys is of minor importance to diagnostic procedures, the current findings are of importance for therapeutic doses of somatostatin derivatives and other peptides labeled with metallic radionuclides. Earlier studies showed that octreotide and octreotate labeled with different radioactive metal ions have similar biodistribution characteristics (19). In most studies, 111In-labeled analogs (111In-DOTATOC and 111In-OCT) are used as surrogates to predict the biodistribution of 90Y- or 177Lu-labeled compounds, despite the fact that the nature of the conjugate may affect the affinity of octreotide for its receptor and consequently its in vivo biodistribution (20,21). PET with 86Y-DOTATOC has been applied to estimate the radiation dose of 90Y-DOTATOC to the kidneys (7,22). However, the mean residence times for 111In-DOTATOC and 90Y-DOTATOC in the kidneys are similar.
It has been shown that the renal uptake of, for example, 90Y-DOTATOC or 177Lu-DOTATATE can be decreased by coinfusion of amino acid mixtures. Kidney dose reductions in the range of 20%–50% have been reported (7,8,19). Nevertheless, the currently optimal amino acid mixture of 25 g of lysine and 25 g of arginine still causes hyperkalemia (8). Our study shows that coinfusion of GELO results in a reduction in the renal uptake of 111In-OCT of 45%, similar to the maximum effect reached with amino acid infusions, without any side effects. It appears that gelatin-derived peptides more effectively attenuate the reabsorption of octreotide than do basic amino acids. GELO is a plasma expander that is widely used clinically at high doses with few or no side effects. In particular, the infusion of GELO is not associated with hyperkalemia. To achieve a reduction in the renal uptake of 111In-OCT, only a limited amount of gelatin, on average, 12.9 g, was needed.
The exact composition of GELO is unknown. Gelatin, which mainly consists of type I collagen, is rich in the amino acids proline and glycine but also contains lysine residues. We expect that the coinfusion of GELO also will decrease the renal uptake of therapeutic doses of 90Y-DOTATOC or 177Lu-DOTATATE, similar to the observed effects on 111In-OCT uptake.
CONCLUSION
The present study shows that the infusion of a relatively small amount of GELO effectively reduces the renal uptake of 111In-OCT and therefore may limit the nephrotoxicity of PRRT, without any of the side effects associated with amino acid infusions. Further in vitro and in vivo studies are in progress to characterize the active substances and their exact mechanisms of action.
References
- Received for publication October 13, 2005.
- Accepted for publication December 15, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Safety and Efficacy of Para-Aminohippurate Coinfusion for Renal Protection During Peptide Receptor Radiotherapy in Patients with Neuroendocrine Tumors
- Glypican-3-Targeting F(ab')2 for 89Zr PET of Hepatocellular Carcinoma
- Renal Toxicity of Radiolabeled Peptides and Antibody Fragments: Mechanisms, Impact on Radionuclide Therapy, and Strategies for Prevention
- Reducing Renal Uptake of Radiolabeled Peptides Using Albumin Fragments
- Bispecific Antibody Pretargeting of Radionuclides for Immuno-Single-Photon Emission Computed Tomography and Immuno-Positron Emission Tomography Molecular Imaging: An Update
- Indication for Different Mechanisms of Kidney Uptake of Radiolabeled Peptides
- Inhibition of Kidney Uptake of Radiolabeled Somatostatin Analogs: Amino Acids or Gelofusine?
- Reply: Inhibition of Kidney Uptake of Radiolabeled Somatostatin Analogs: Amino Acids or Gelofusine?