


Abstract
Because of the presence of cell membrane somatostatin receptors (SSTRs), many neuroendocrine tumors will bind analogs of somatostatin. 90Y-Dodecanetetraacetic acid-Phe1-Tyr3-octreotide (SMT 487) is an SSTR radiopharmaceutical currently under investigation as a therapeutic option for neuroendocrine tumors. Although there are a variety of methods for evaluating response to a given cancer therapy, an important indicator of success is the impact on the clinical status of the patient. The purpose of this work was to develop a semiquantitative method and assess the clinical effectiveness of 90Y-SMT 487 therapy in patients with neuroendocrine tumors. Methods: A scoring system was developed to evaluate clinical response that included the following parameters: weight, health status score (determined by the patient), Karnofsky score, and tumor-related symptoms. Results: We applied this scoring system to 21 patients who had completed 3 cycles of therapy with 90Y-SMT 487. Fourteen of the 21 showed a favorable clinical response, whereas 5 were clinically stable after treatment and 2 showed evidence of clinical progression. There was also a significant reduction in the amount of octreotide being used after completion of 90Y-SMT 487 therapy in the 20 patients who were on this medication. Conclusion: Using this scoring method, 90Y-SMT 487 appears effective in improving the clinical status of patients with 111In-pentetreotide-positive neuroendocrine tumors.
Neuroendocrine tumors share a common tissue of origin and typically synthesize and secrete a variety of bioactive monoamines and peptides, which can cause debilitating symptoms. Therapy of metastatic neuroendocrine tumors was enhanced dramatically with the introduction of the somatostatin analog octreotide (Sandostatin; Novartis). Although having only a modest ability to control tumor growth, this agent nevertheless has a dramatic impact on the elaboration of the bioactive substances responsible for many of the symptoms (1). Unfortunately, nearly all such tumors will eventually become resistant to the effects of octreotide (1).
Because of the presence of somatostatin receptors (SSTRs), especially subtype 2, on the cell surface membrane, many types of neuroendocrine tumors will bind analogs of somatostatin. 90Y-Dodecanetetraacetic acid-Phe1-Tyr3-octreotide (SMT 487 [OctreoTher; Novartis]) is an SSTR radiopharmaceutical currently under investigation as a therapeutic agent for patients with SSTR-positive neuroendocrine tumors. It differs from the imaging agent 111In-pentetreotide (OctreoScan; Mallinckrodt Medical) by substituting tyrosine for phenylalanine at the 3 position and by replacing the chelator diethylenetriaminepentaacetic acid with dodecanetetraacetic acid. In addition, and critical for therapeutic application, the β-emitter 90Y takes the place of 111In on this molecule. Early clinical studies have produced encouraging results for targeted radiotherapy of SSTR-positive tumors with this agent (2,3).
CT measurement of tumor size is a well-accepted method for assessing response to therapy. However, CT examination is not without limitations when one is attempting to determine the effectiveness of a particular cancer treatment (4). Ultimately, the most important indicator of treatment response is the impact on clinical status. Improvement in survival is easiest to measure and clearly vital, but an extended time may be required to complete the analysis. Assessment of the treatment impact on morbidity is more difficult but of great importance. The purpose of this work was to develop a clinical response scoring system and use it to assess the initial clinical effectiveness of 90Y-SMT 487 therapy.
MATERIALS AND METHODS
The study group represented a subset of patients with neuroendocrine tumors who were enrolled as part of a phase II trial of the efficacy and safety of 90Y-SMT 487 in patients with SSTR-positive metastatic tumors, as determined by SPECT or planar 24-h 111In-pentetreotide imaging. The eligibility criterion was greater 111In-pentetreotide uptake in at least 1 measurable tumor site than in normal liver. Patients were required to discontinue octreotide before imaging with 111In-pentetreotide or therapy with 90Y-SMT 487, and they signed an institutional review board-approved consent document before participation.
The trial design called for 3 treatment cycles of 4,400 MBq (120 mCi) each of 90Y-SMT 487 every 6–9 wk. With each treatment cycle, 2 L of an amino acid solution containing arginine and lysine (Aminosyn II 7%; Abbott Laboratories) was infused over 4 h to reduce renal uptake of 90Y-SMT 487. 90Y-SMT 487 was administered intravenously over approximately 15–20 min, concurrent with the amino acid infusion through a separate intravenous line.
A scoring system was developed that included the following parameters evaluated at baseline and 6 wk after the third cycle of therapy: weight, health status score, Karnofsky score, and tumor-related symptoms. Tumor-related symptoms and Karnofsky score were determined by either the study nurse or the physician. Symptoms that were evaluated included fatigue, abdominal pain, diarrhea, nausea/vomiting, and flushing. These were assessed without knowledge of biochemical or CT follow-up results. The health status score was determined by the individual patients, who were asked to rate the state of their health on a scale of 1–100 by marking a point along a 100-mm line.
Table 1 summarizes the scoring system used to determine each patient’s clinical response status. An overall clinical response score was obtained for each patient by summing the individual scores described in Table 1. Consequently, the maximum clinical response score was +4 and the minimum was −4. A patient was considered to have a favorable clinical response to therapy if the clinical response score was +2 or greater; was considered stable if the score was −1, 0, or +1; and was considered to have clinical progression if the score was −2 or less.
Scoring System for Clinical Response Score
Finally, to better assess the clinical validity of our response score, we determined the tumor-related medication requirements for each patient before and after therapy with 90Y-SMT 487. To discern whether medication use had significantly decreased after treatment, pretherapy daily octreotide doses were compared with the doses 6–10 wk after the third cycle of therapy, using a paired t test with P = 0.05 defined as significant.
RESULTS
The baseline and posttherapy assessments were completed for 21 patients with metastatic neuroendocrine tumors (20 of which were known to be enteropancreatic in origin) who successfully completed all 3 cycles of 90Y-SMT 487 therapy. Seventeen individuals had carcinoid tumors, 2 had nonfunctional islet cell tumors of the pancreas, 1 had a glucagonoma, and 1 had metastases from a neuroendocrine tumor of unknown origin. There were 9 women and 12 men, ranging in age from 41 to 76 y. One other patient with a neuroendocrine tumor was excluded from the analysis because of inadequate clinical follow-up. We excluded 3 other individuals because of their different tumor types (small cell lung cancer, meningioma, and cranial hemangiopericytoma). Three additional patients were excluded because they did not complete the full 3 cycles of therapy.
Baseline and posttherapy body weights, health state scores, and Karnofsky scores and the response status of each clinical symptom for each patient are summarized in Table 2. On the basis of our scoring system, 14 patients (67%; 95% confidence interval, 43%–85%) showed a favorable clinical response, 5 patients (24%) were clinically stable, and 2 patients (10%) showed clinical progression.
Clinical Response Indicators
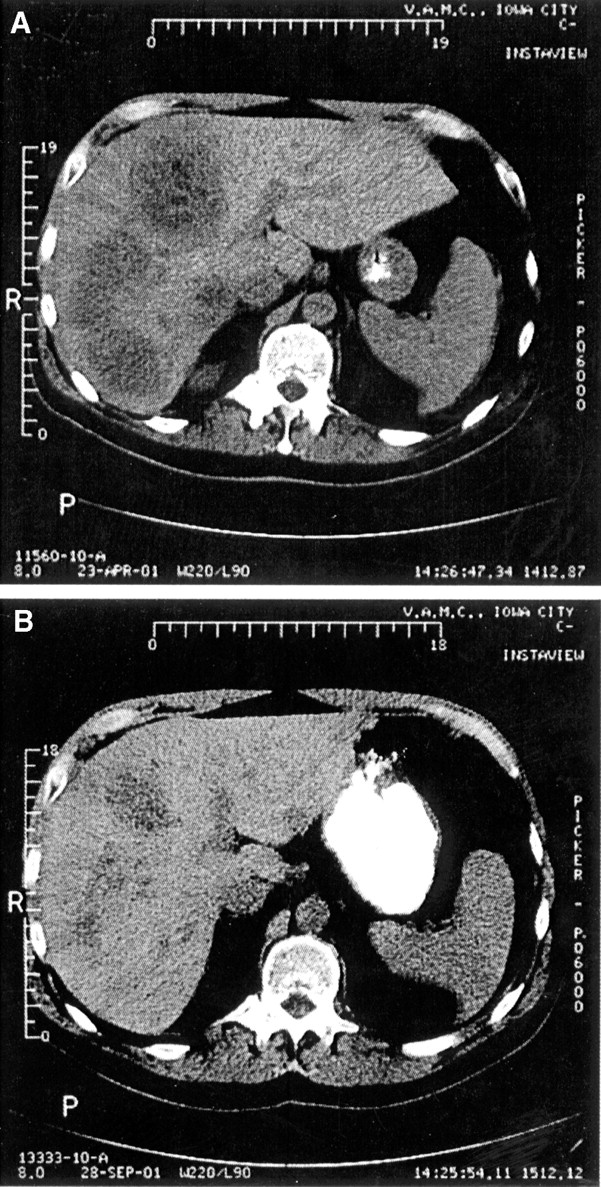
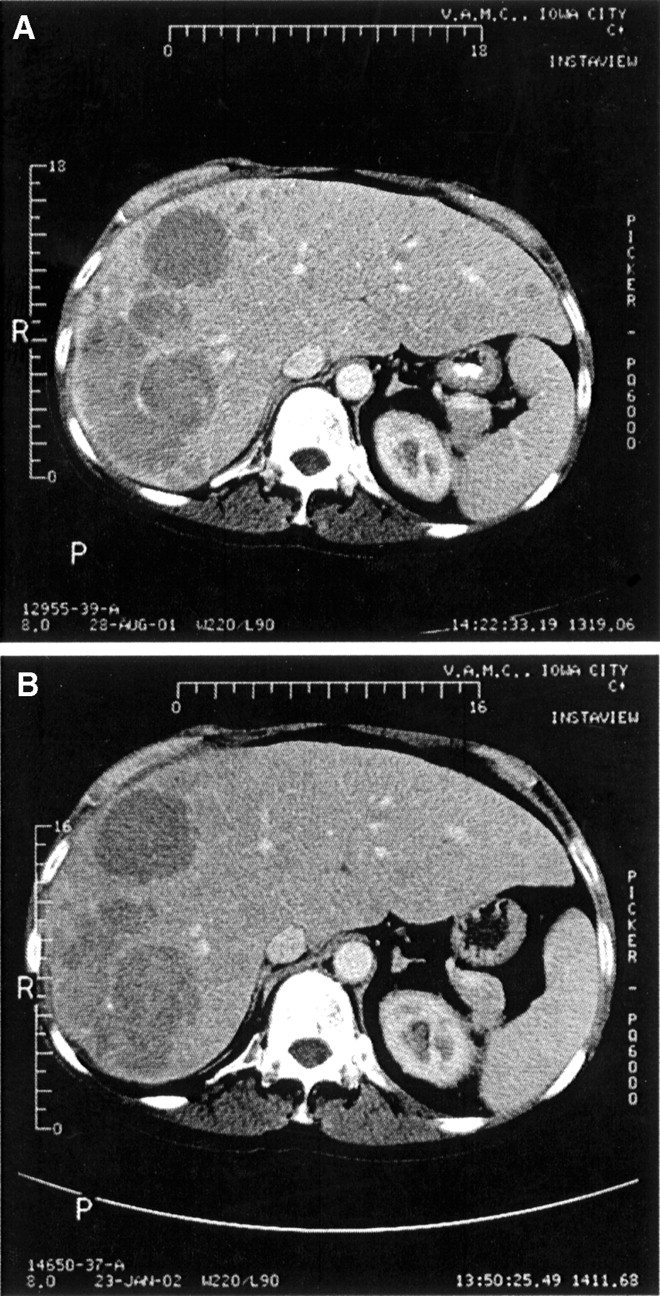
Figures 1A and 1B are examples of baseline and posttherapy CT scans revealing substantial shrinkage in numerous large hepatic metastases. The patient (patient 7) had a favorable clinical response. However, not all of the 14 individuals with a favorable clinical response showed CT evidence of tumor shrinkage. Figures 2A and 2B show little change in the hepatic metastases on the pre- and posttherapy CT scans of patient 10, who nevertheless had a favorable clinical response.
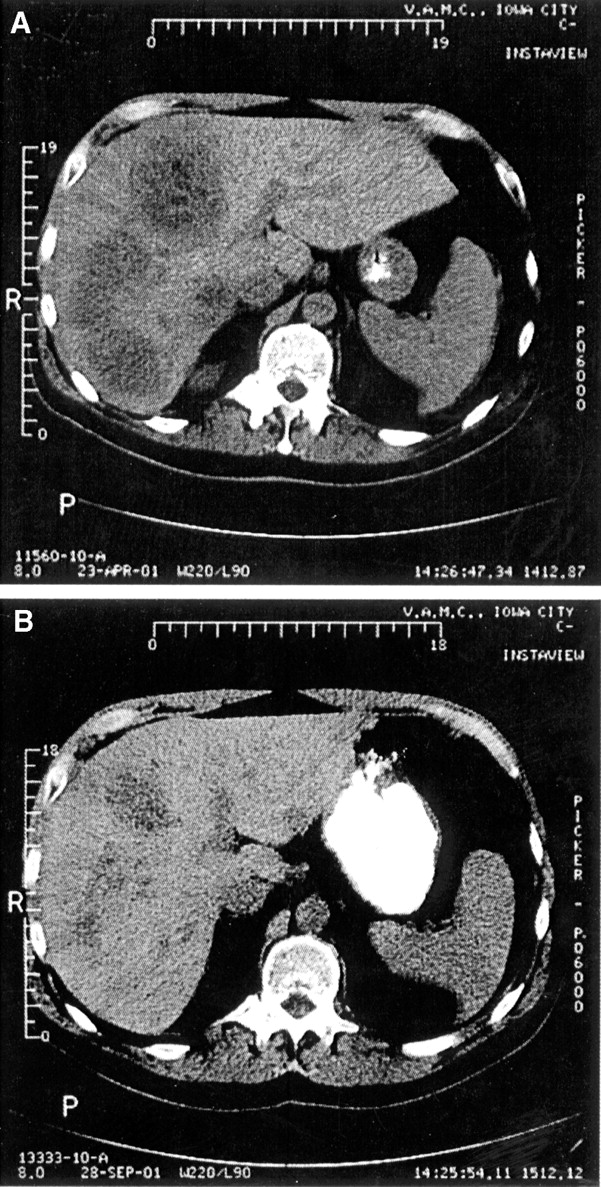
Pretherapy (A) and posttherapy (B) CT images of liver of patient 7 show that multiple large, hypodense lesions seen at baseline were significantly smaller on posttherapy CT.
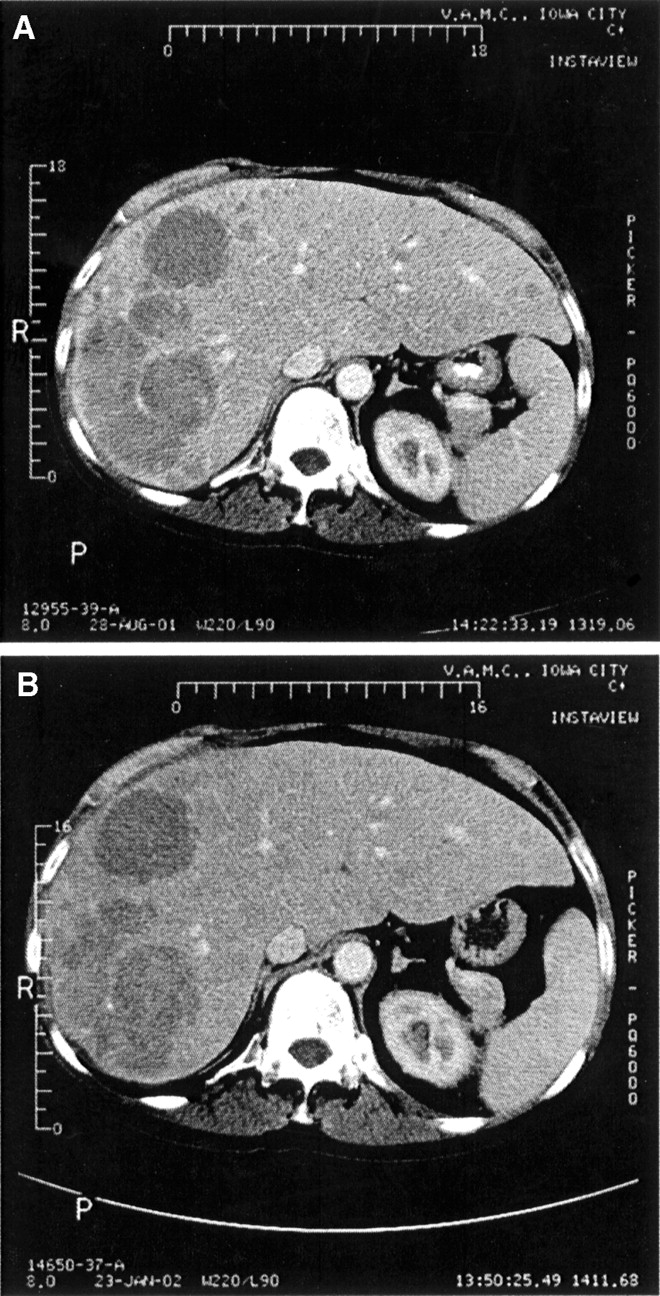
Pretherapy (A) and posttherapy (B) CT images of liver of patient 10 show that multiple large, hypodense lesions seen at baseline did not change significantly after therapy.
Table 3 summarizes the pre- and posttherapy daily octreotide requirements along with the final clinical response status for each patient. One individual was not taking octreotide before treatment with 90Y-SMT 487. For the other 20 patients, there was a significant reduction in octreotide dosage after treatment with 90Y-SMT 487 (P = 0.044). Of the 18 clinically stable or improved patients who were using octreotide before therapy with 90Y-SMT 487, 13 were taking a reduced dosage of this medication after completing cycle 3.
Daily Octreotide Doses Before and After 90Y-SMT 487 Therapy
DISCUSSION
Early results with 90Y-SMT 487 in patients with neuroendocrine tumors have been promising. However, not all studies address the issue of clinical response. For example, Paganelli et al. reported on a group of 20 patients participating in a dose escalation trial consisting of 3 treatment cycles with 90Y-SMT 487 beginning at 1.1 GBq (30 mCi)/cycle in the first group of 5 individuals and ending at 2.2 GBq (60 mCi)/cycle in the last group of 5 (3). Using World Health Organization (WHO) response criteria with CT or MRI, they found an overall response rate of 25%, with 55% showing stable disease and 20% showing progressive disease. Otte et al. treated a group of 29 patients with 4 or more cycles of 90Y-SMT 487 in ascending administered activities (2). The mean cumulative administered activity for their group was 6.1 GBq (165 mCi)/m2. They used a combination of CT and 111In-pentetreotide imaging to define response. Of the 9 patients followed with CT, 2 showed partial remission, 4 showed stable disease, and 3 showed progressive disease. Clinical response data were not reported for either of these studies.
More recent reports have included limited data on the clinical effectiveness of this treatment. Waldherr et al. published results from a phase II study finding similar efficacy to the aforementioned studies in a larger group of patients with neuroendocrine tumors (5). Patients in this study received a total of 7.4 GBq (200 mCi)/m2 administered over 4 therapy cycles. In addition, these authors assessed clinical effectiveness using a patient-scored questionnaire given before and after treatment to 21 of their patients. They found that, overall, 63% of these individuals reported improvement in at least 1 of 4 symptom categories, which included diarrhea, flushing, wheezing, or pellagra. Valkema et al. reported symptomatic improvement in 18 of 38 patients with neuroendocrine tumors, including 2 individuals with insulinomas (6). The administered activity of 90Y-SMT 487 in this study was based on renal dosimetry estimates, with patients limited to a total of 27 Gy to the kidneys over multiple therapy cycles with 90Y-SMT 487. Consequently, our finding of a 67% favorable clinical response is very consistent with what has been reported to date.
Because our study was not masked or placebo-controlled, there was, of course, the potential for bias in assessing symptom response. It may be beneficial if future applications of this methodology use WHO grading criteria for evaluation of the 4 symptoms listed in Table 1. Our scoring system did include an important objective measure (weight change) as well as the subjective assessments described. Additionally, we required a +2 overall score for classification as a favorable response to enhance the certainty of correctly identifying individuals who did in fact benefit from this therapy.
CONCLUSION
On the basis of the results from our clinical response scoring system and the finding of reduced medication requirements, therapy with 90Y-SMT 487 appears to improve the clinical status of a substantial fraction of patients withSSTR-positive neuroendocrine tumors. Further data are needed to determine, among other things, the duration of clinical benefit and possible impact on survival. This multicenter phase II trial is ongoing, and the final results may change as additional data are received and analyzed from the other institutions.
Acknowledgments
We thank the personnel of the University of Iowa Clinical Research Center for their assistance with this project. We also thank John Bricker, Wayne Walkner, and James Ponto for their important contributions to this work. Funding for this work was provided by Novartis.
Footnotes
Received Jan. 21, 2003; revision accepted Jun. 13, 2003.
For correspondence or reprints contact: David Bushnell, MD, Diagnostic Imaging and Radioisotope Therapy Service, Iowa City Veterans Administration Hospital, Highway 6 West, Iowa City, IA 52240.
E-mail: david-bushnell{at}uiowa.edu
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Management of neuroendocrine tumors
- Role of Somatostatin Analogues in the Treatment of Neuroendocrine Tumors
- Molecular radiotherapy
- Radiopeptide Imaging and Therapy in the United States
- Phase I Trial of 90Y-DOTATOC Therapy in Children and Young Adults with Refractory Solid Tumors That Express Somatostatin Receptors
- 90Y-Edotreotide for Metastatic Carcinoid Refractory to Octreotide
- Somatostatin receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors
- Treatment of Metastatic Carcinoid Tumors With Radiolabeled Biologic Molecules
- Utility of Radiolabeled Somatostatin Receptor Analogues for Staging/Restaging and Treatment of Somatostatin Receptor-Positive Pediatric Tumors
- Potential Increased Tumor-Dose Delivery with Combined 131I-MIBG and 90Y-DOTATOC Treatment in Neuroendocrine Tumors: A Theoretic Model
- Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues
- Evaluation of [99mTc/EDDA/HYNIC0]Octreotide Derivatives Compared with [111In-DOTA0,Tyr3, Thr8]Octreotide and [111In-DTPA0]Octreotide: Does Tumor or Pancreas Uptake Correlate with the Rate of Internalization?
- Preclinical Evaluation of New and Highly Potent Analogues of Octreotide for Predictive Imaging and Targeted Radiotherapy
- Overview of Results of Peptide Receptor Radionuclide Therapy with 3 Radiolabeled Somatostatin Analogs
- 68Ga-Labeled Peptides in Tumor Imaging
- Combination Radionuclide Therapy Using 177Lu- and 90Y-Labeled Somatostatin Analogs
- Patient-Specific Dosimetry in Predicting Renal Toxicity with 90Y-DOTATOC: Relevance of Kidney Volume and Dose Rate in Finding a Dose-Effect Relationship