


Abstract
Radiopharmaceutical therapy, traditionally limited to refractory metastatic cancer, is being increasingly used at earlier stages, such as for treating minimal residual disease. The aim of this study was to compare the effectiveness of 90Y, 177Lu, 111In, and 161Tb at irradiating micrometastases. 90Y and 177Lu are widely used β−-emitting radionuclides. 161Tb is a medium-energy β− radionuclide that is similar to 177Lu but emits a higher percentage of conversion and Auger electrons. 111In emits γ-photons and conversion and Auger electrons. Methods: We used the Monte Carlo code CELLDOSE to assess electron doses from a uniform distribution of 90Y, 177Lu, 111In, or 161Tb in spheres with diameters ranging from 10 mm to 10 μm. Because these isotopes differ in electron energy per decay, the doses were compared assuming that 1 MeV was released per μm3, which would result in 160 Gy if totally absorbed. Results: In a 10-mm sphere, the doses delivered by 90Y, 177Lu, 111In, and 161Tb were 96.5, 152, 153, and 152 Gy, respectively. The doses decreased along with the decrease in sphere size, and more abruptly so for 90Y. In a 100-μm metastasis, the dose delivered by 90Y was only 1.36 Gy, compared with 24.5 Gy for 177Lu, 38.9 Gy for 111In, and 44.5 Gy for 161Tb. In cell-sized spheres, the dose delivered by 111In and 161Tb was higher than that of 177Lu. For instance, in a 10-μm cell, 177Lu delivered 3.92 Gy, compared with 22.8 Gy for 111In and 14.1 Gy for 161Tb. Conclusion: 177Lu, 111In, and 161Tb might be more appropriate than 90Y for treating minimal residual disease. 161Tb is a promising radionuclide because it combines the advantages of a medium-energy β− emission with those of Auger electrons and emits fewer photons than 111In.
The main advantage of radiopharmaceutical therapy over conventional external-beam radiotherapy is the ability to reach metastases and tumor cells scattered in multiple body locations (1). Radiopharmaceutical therapy uses tumor-targeting radiopharmaceuticals, such as 131I-metaiodobenzylguanidine for neural crest-derived tumors, 131I- or 90Y-labeled anti-CD20 antibodies for lymphoma, the somatostatin analogs 90Y-DOTATOC and 177Lu-DOTATATE for neuroendocrine tumors, or prostate-specific membrane antigen–targeting molecules for prostate cancer (2–5).
Radiopharmaceutical therapy is not limited anymore to palliative care in patients with relapsed or refractory disease but now includes early treatment of metastatic disease, adjuvant therapy, and consolidation after remission, as, for example, in non-Hodgkin lymphomas (6,7). Indeed, adjuvant 131I therapy is known to prevent recurrence after thyroidectomy (8). Also, radiopharmaceutical therapy achieves better results when the metastases are small (4,9). Large metastases are difficult to irradiate effectively because they often include areas of stromal, fibrous, or necrotic tissues as well as tumor areas with loss of target expression, resulting in heterogeneous distribution of the absorbed dose. Moreover, hypoxia increases resistance to radiation. Experimental data in rodents also showed better efficacy on microscopic metastases (10,11).
In many cancers, prognosis is linked to metastatic relapse, which may occur years after primary surgery (12). Relapse can be predicted from various parameters, including the initial locoregional extension, tumor grade, response to neoadjuvant treatment, and tumor marker levels. Moreover, metastatic spread can now be diagnosed at a very early stage, for example, by detecting tumor cells in the bone marrow or blood (13,14). Therefore, radiopharmaceutical therapy may play an important role to eradicate occult micrometastases in high-risk patients.
It is, however, unclear which isotopes would be the most appropriate for adjuvant or consolidation therapy, in which tumor targets are undetectable by radiologic examinations and presumably very small (ranging from isolated tumor cells to lesions of 5–10 mm in diameter). Although 90Y showed encouraging results for treating occult residual disease after remission of ovarian cancer (15) and lymphoma (6,7), isotopes with lower energy might be a better choice.
90Y (high-energy β−) and 177Lu (medium-energy β−) are the 2 most widely used isotopes for labeling therapeutic radiopharmaceuticals (2–5). 111In is a γ-emitting isotope mainly used for imaging. However, it also emits Auger and conversion electrons (CEs) and might be used to target micrometastases and single cells (16–18). The radiolanthanide 161Tb is a medium-energy β− emitter similar to 177Lu but emits a higher percentage of conversion and Auger electrons. Some in vivo studies suggested that 161Tb might outperform 177Lu (19,20). The aim of this Monte Carlo simulation study was to compare the effectiveness of 90Y, 177Lu, 111In, and 161Tb at irradiating micrometastases of various sizes.
MATERIALS AND METHODS
The Monte Carlo code CELLDOSE was used to assess electron dose from a uniform distribution of 90Y, 177Lu, 111In, or 161Tb in spheres of water density whose diameters ranged from 10 mm to 10 μm. The decay characteristics of these isotopes are shown in Table 1. The full data on electron emissions (β-spectra, CE, Auger and Coster–Kronig electrons) were obtained from the International Commission on Radiological Protection publication ICRP-107 (21). The electron emission spectra used in the Monte Carlo simulation are shown in Figure 1. Photons were neglected.
Characteristics of the 4 Radionuclides

Electron emissions of 90Y, 177Lu, 111In, and 161Tb. β-spectra are in red, CEs are in blue, and Auger electrons are in green. CEs and Auger electrons with probability of less than 0.0001 were neglected (21).
CELLDOSE is based on electron–water molecule interaction cross sections and takes into account all ionizations, excitations, and elastic scatterings to produce an event-by-event electron track simulation (22). The full slowing-down histories for primary and secondary electrons are described until an energy value of 7.4 eV is reached (electronic excitation threshold of the water molecule) (23). The residual energy below this cutoff was considered to be absorbed locally. Figure 2 shows the energy deposits along the paths of 2 CEs (1 from 111In and 1 from 161Tb) and 2 Auger electrons.

Tracks of representative electrons from 111In and 161Tb as obtained with CELLDOSE. (A) 111In CE-K (144.6 keV; frequency, 8.5%; magenta) and 161Tb CE-L (39.9 keV; frequency, 38%; blue). (B) 111In Auger LMM transition (2.61 keV; frequency, 82%; red) and 161Tb Auger MNN transition (1.02 keV; frequency, 184%; green). ● = ionizing interactions induced by primary electrons; ○ = ionizing interactions induced by secondary electrons.
For each isotope and sphere, we assessed the absorbed energy as well as the relative contribution of β− particles and CE and Auger electrons (as we previously described for 131I (22)).
In addition to the dose resulting from a single decay (S values), we also calculated in all spheres the absorbed dose resulting from a uniform concentration (1 decay per μm3). Moreover, because the 4 isotopes have a different electron energy emitted per decay, absorbed doses were compared after normalizing by a fixed amount of electron energy released per unit of volume (1 MeV per μm3). This concentration would yield 160 Gy if totally absorbed.
Finally, to assess the ability of each isotope to deliver a cross-dose outside labeled structures, we studied the spatial profile of energy deposit around a point source.
RESULTS
Absorbed Energy and Contribution of Different Electron Emissions
For each isotope, Table 2 reports the energy absorbed in each sphere and the relative contribution of the various electron emissions. The absorbed energy decreases along with the decrease in sphere size. This decrease was more pronounced in the case of 90Y (Table 2).
Retained Energy (Percentage and Absolute Value) and Contribution of Different Electronic Emissions
For 177Lu, the combined contribution of CE and Auger electrons to absorbed energy was 10% in the 10-mm sphere and reached 33.9% in the 10-μm sphere (Table 2). The contribution of CE and Auger electrons was much higher in the case of 161Tb and was 24.9% of the energy deposit in the 10-mm sphere and 88.3% in the 10-μm sphere (Table 2). Considering 111In, the relative contribution of Auger electrons increased compared with that of CEs when the sphere size decreased.
S Values for 90Y, 177Lu, 111In, and 161Tb in Spheres of Various Sizes
S values obtained with the Monte Carlo code CELLDOSE are reported in Table 3. There was good agreement with S values previously reported for 90Y and 177Lu using scaled dose point kernel (24) and for 90Y and 111In using range-energy expressions for electrons (25). The largest differences were found for 90Y in the 5,000-μm sphere: the S value reported by Goddu et al. was 11% lower, whereas that reported by Bardiès and Chatal was 5.4% higher, than the value obtained with CELLDOSE (24,25). 161Tb data were not available in the literature for comparison.
Comparison of Electron Dose Deposit for the 4 Isotopes (Figure 3)
Absorbed Doses from 90Y, 177Lu, 111In, and 161Tb After Normalization
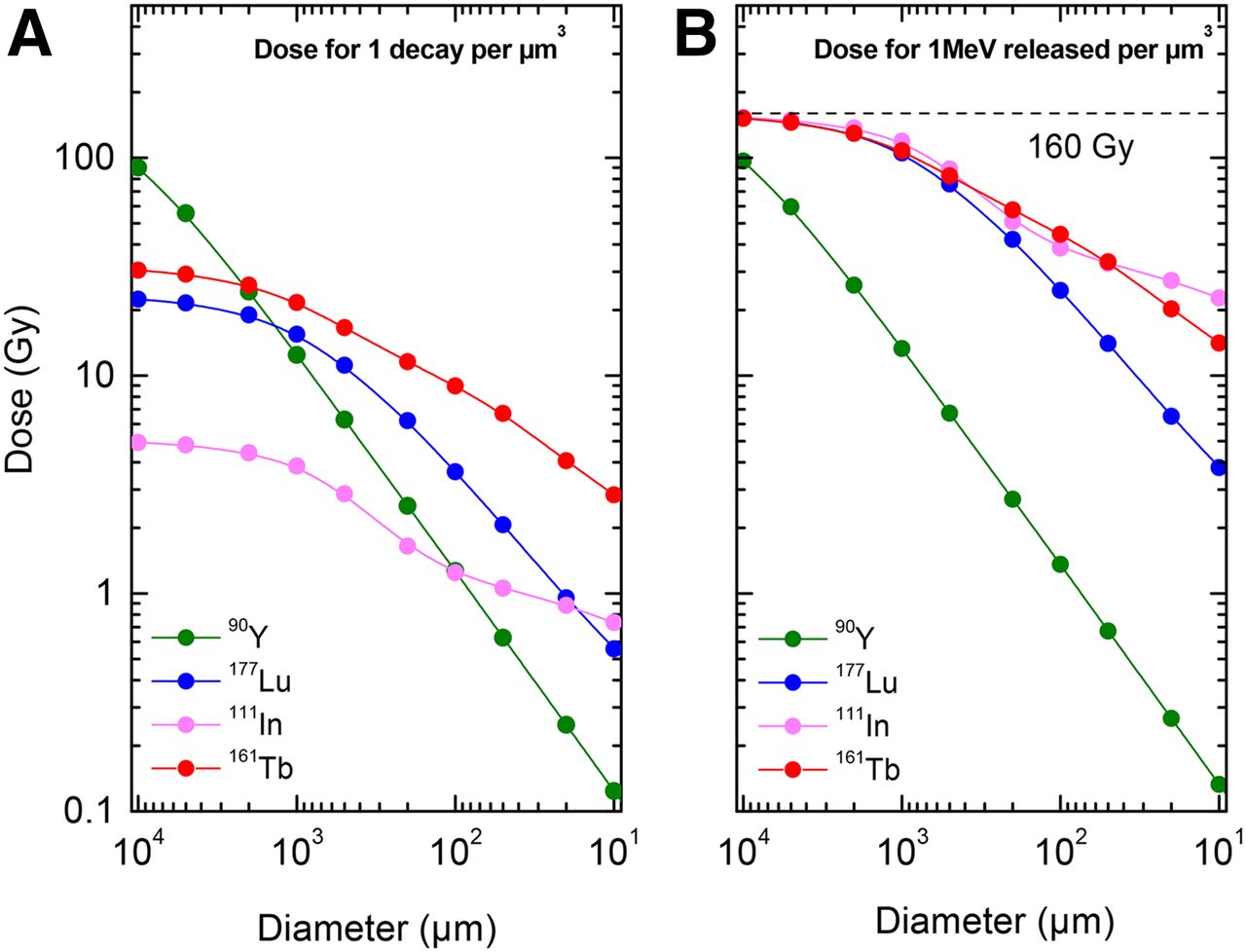
Table 3 and Figure 3 show, for each isotope and sphere, the absorbed dose from 1 decay per μm3 and the absorbed dose from 1 MeV released per μm3 (i.e., normalization for differences in electron energy per decay). On the basis of the total electron energy released per decay (Table 1), the average number of decays per cubic micrometer (N) that corresponds to 1 MeV released per cubic micrometer is 1.07 for 90Y, 6.76 for 177Lu, 28.74 for 111In, and 4.94 for 161Tb. Also, assuming complete decay and no biologic excretion or redistribution over time, and a tissue density of 1 g/cm3, this corresponds to an activity concentration within tumor tissue (A0 = N × ln2/T) of 3.22 MBq/g for 90Y, 8.16 MBq/g for 177Lu, 82.19 MBq/g for 111In, and 5.74 MBq/g for 161Tb.

Electron dose from 90Y (green), 177Lu (blue), 111In (magenta), and 161Tb (red) as a function of sphere size. (A) Electron dose considering 1 decay per μm3. (B) Electron dose considering 1 MeV released per μm3. 160 Gy/MeV/μm3 corresponds to total absorption.
When 1 MeV was released in every μm3, the absorbed dose for a 10-mm metastasis was 96.5 Gy with 90Y, 152 Gy with 177Lu, 153 Gy with 111In, and 152 Gy with 161Tb (Table 3). However, in a 1-mm metastasis, the dose delivered by 90Y fell to 13.3 Gy as compared with 104 Gy with 177Lu, 118 Gy with 111In, and 108 Gy with 161Tb. For a 100-μm micrometastasis, the absorbed dose was only 1.36 Gy with 90Y but 24.5 Gy with 177Lu, 38.9 Gy with 111In, and 44.5 Gy with 161Tb (Table 3; Fig. 3).
In cell-sized spheres, 111In and 161Tb delivered significantly higher doses than 177Lu. For instance, in a homogeneously labeled single cell of 10-μm diameter, the absorbed dose was 3.92 Gy for 177Lu, 22.8 Gy for 111In, and 14.1 Gy for 161Tb (Table 3; Fig. 3).
Energy Deposit Around Point Source
Figure 4 shows the pattern of energy deposit after normalization (1 MeV released). The radius within which 90% of the energy is deposited is 5.82 mm for 90Y, 0.62 mm for 177Lu, 0.37 mm for 111In, and 0.63 mm for 161Tb. The radius within which 99% of the energy is deposited is 8.19 mm for 90Y, 1.07 mm for 177Lu, 0.49 mm for 111In, and 1.06 mm for 161Tb. At a distance beyond 0.8 mm, 90Y deposited more energy (per MeV released) than 177Lu or 161Tb.

(A and B) Energy deposit (per MeV released) within concentric shells of 10-μm thickness around point source: 90Y (green), 177Lu (blue), 111In (magenta), and 161Tb (red). (C and D) Comparisons of energy deposit in first 700 μm: 111In vs. 177Lu (C), 161Tb vs. 177Lu (D). Energy deposit is in logarithmic scale in A and B and in linear scale in C and D.
The complex profile of energy deposit from 111In shows a high peak, 4 times higher than that of 177Lu (per MeV released), in the first 10-μm-thick shell surrounding the point source (Fig. 4C).
The pattern of energy deposit of 161Tb and 177Lu markedly differed in proximity of the source. The energy deposited by 161Tb (per MeV released) was higher than that deposited by 177Lu up to 30 μm around the point source, and particularly so in the first 10 μm (Fig. 4D).
DISCUSSION
Most currently used radiopharmaceuticals were designed to be administered to patients with advanced disease, and the choice of the radionuclide had been made accordingly. However, the same radiopharmaceuticals might not be equally effective to treat both large tumor masses and minimal residual disease. For example, anti-CD20 antibodies, labeled with 90Y, have been used to treat patients with relapsed or refractory lymphomas (2) but are now also used for consolidation after successful chemotherapy (6,7). In radionuclide therapy, there is an optimal tumor size for cure, which differs from one radionuclide to another (26,27). Thanks to the high energy of 90Y β− particles, 90Y-labeled radiopharmaceuticals may compensate for uptake heterogeneity within large tumors and effectively irradiate nonlabeled targets, such as liver malignancies after intraarterial radioembolization (28). At a distance beyond 0.8 mm, 90Y deposited more energy (per MeV released) than 177Lu (Fig. 4). However, our results clearly suggest that 90Y is not an adequate isotope for eradicating micrometastases, because most of the energy was deposited outside the tumor (Table 2). This is expected to reduce efficacy and increase toxicity. 177Lu irradiated smaller spheres more effectively than 90Y.
To facilitate the comparison between isotopes, the energy released was normalized for 1 MeV per μm3 of tumor tissue. If totally absorbed, this energy would yield 160 Gy. The normalized dose in a 1-cm metastasis was 96 Gy with 90Y (vs. 152 Gy with 177Lu). However, the dose delivered by 90Y steeply decreased when sphere size decreased (Table 3; Fig. 3B). In a 1-mm metastasis, the dose from 90Y was 13.3 Gy (vs.104 Gy with 177Lu). In a 100-μm micrometastasis, the dose from 90Y was only 1.36 Gy, whereas 177Lu delivered 24.5 Gy.
These results are in line with experimental data by Michel et al., who showed that the rate of eradication of single cells and micrometastases was higher with 177Lu than with 90Y (29). By contrast, 1 study assessed anti-CD20 pretargeted radioimmunotherapy on lymphoma xenografts and found a higher efficacy with 90Y (30). However, the treatment was given when the size of tumor xenografts exceeded 8 mm (which is higher than the size of a typical micrometastasis). Radioactivity distribution within the tumor was highly heterogeneous (30). Also, because tumor uptake (percentage injected dose per gram) decreased over time (11.8% at 4 h; 3.7% at 120 h), the longer half-life of 177Lu was here a drawback. Finally, 90Y and 177Lu were compared using the same activity (37 MBq), although the amount of energy released differs.
Although 177Lu performed better than 90Y in small metastases, 111In and 161Tb outperformed 177Lu in very small metastases (<100 μm) and single cells (Table 3; Fig. 3B).
The dose delivered by 111In (considering 1 MeV released per μm3) was 1.6 times higher than that from 177Lu in a 100-μm micrometastasis (38.9 vs. 24.5 Gy) and 5.8 times higher than that from 177Lu in a 10-μm cell (22.8 vs. 3.92 Gy) (Table 3). Studies have shown that the rate of eradication of micrometastases and single cells is higher with 111In than with either 90Y (16) or 177Lu (29). By consequence, many teams actively work on developing 111In-labeled radiopharmaceuticals aimed at targeting micrometastases or cancer stem cells (17,18). 111In has, however, a large proportion of photon emission (92% of the total energy per decay) (Table 1). Photon emission adds to the total-body dose and in many countries requires patient hospitalization for radiation protection purposes. The alternatives offered by 161Tb are then of major interest.
161Tb has a β− spectrum similar to that of 177Lu but emits a larger number of Auger electrons and CEs (Fig. 1). Most 161Tb CEs are in the low-energy domain (<50 keV) and deposit their dose over relatively short distances (Figs. 1 and 2). The dose delivered by 161Tb (considering 1 MeV released per μm3) is 1.8 times higher than that delivered by 177Lu in a 100-μm micrometastasis (44.5 vs. 24.5 Gy) and 3.6 times higher than 177Lu in a 10-μm cell (14.1 vs. 3.9 Gy) (Table 3). 161Tb deposits a larger amount of energy per MeV than 177Lu over a distance of 30 μm (Fig. 4D). Thus, 161Tb would likely deliver a higher dose than 177Lu, not only to the targeted cell but also to its immediate neighbors.
Our Monte Carlo simulation provides a mechanistic rationale to the studies that found a good tumor-control efficacy of 161Tb-labeled molecules. For example, 161Tb-anti-L1CAM antibodies were more effective than 177Lu-anti-L1CAM at inhibiting the growth of subcutaneous xenografts of ovarian cancer (19). In another study, the radioactivity concentration necessary to achieve half-maximal inhibition of tumor cells was lower with 161Tb-labeled than with 177Lu-labeled radiofolate conjugates (20).
The most suitable radioisotope can be appropriately chosen if the subcellular distribution of the targeting molecule is known. Techniques such as high-resolution autoradiography or secondary ion mass spectrometry can quantitatively depict the distribution at the cellular level (31). This distribution may be used as input to derive the absorbed dose with Monte Carlo codes (32,33). Uniform distribution, as considered in the present study, is an acceptable model for some molecules, which are internalized via receptor-mediated endocytosis and partly trafficked to the nucleus. Examples include growth factors such as epidermal growth factor or agonist analogs of somatostatin and bombesin (4,17,34). By contrast, neuropeptide antagonists are not internalized (34). Again, some antibodies are internalized after binding to their membrane receptor (e.g., antibodies targeting CD22, prostate-specific membrane antigen, epidermal growth factor receptor, human epidermal growth factor receptor 2), whereas others (e.g., anti-CD20 and anti–carcinoembryonic antigen) are less internalized. Many research projects aim at facilitating the routing of Auger-emitting radiopharmaceuticals to the nucleus (18,35). For DNA irradiation, internalization in the nucleus is indeed necessary to get the full benefit from Auger electrons (Fig. 2B). Auger electrons may also effectively irradiate other targets, such as cell membranes (36).
Our study may help in predicting the effectiveness of adjuvant therapy in clinical trials. We ran our simulation by assuming that 1 MeV was released per μm3. If totally absorbed, this energy would yield 160 Gy using any isotope. Notably, this value is within the range of tumor-absorbed doses that were measured in metastases of neuroendocrine tumors in patients who showed good response to 177Lu-DOTATATE therapy (37). If the same activity of 177Lu-DOTATATE that is used for treating radiologic metastases was given as adjuvant therapy, and assuming that the uptake in occult metastases is the same (1 MeV released per μm3), the radiation dose would decrease along with the size of targeted metastases. The predicted dose would be 104 Gy in a 1-mm metastasis, 24.5 Gy in a 100-μm micrometastasis, and 3.9 Gy in a 10-μm single tumor cell. Although small tumors are more radiosensitive than macrometastases (10,11), the low dose delivered by 177Lu to isolated cells might not be sufficient to destroy them all. However, the dose delivered by a hypothetical 161Tb-labeled somatostatin analog (with the same tumor affinity) would be 1.8 times higher in a 100-μm micrometastasis (44.5 Gy) and 3.6 times higher in a 10-μm single cell (14.1 Gy) (Table 3).
Similarly to 177Lu, 161Tb can be stably linked to various targeting molecules (19,20). 161Tb has a small percentage of photons that would enable posttherapy imaging (Table 1). Moreover, 2 isotopes of terbium (152Tb: half-life, 17.5 h, β+ emitter; and 155Tb: half-life, 5.32 d, γ-emitter) offer the possibility for pretherapy imaging and dosimetry with PET or SPECT.
161Tb can be produced as no-carrier-added in large amounts, using, for example, a 160Gd target (160Gd(n,γ)161Tb), and with good radionuclide purity (160Tb–to–161Tb activity ratio < 0.0001) (38). The cost for large-scale production was estimated to be comparable to that of no-carrier-added 177Lu (38).
CONCLUSION
Radiopharmaceutical therapy can effectively target disseminated tumor cells and occult micrometastases, provided that the optimal radionuclide is used. 177Lu, 111In, and 161Tb might be more appropriate than 90Y for treating minimal residual disease. 161Tb combines the classic advantages of a medium-energy β− isotope and those specific to Auger emitters. In addition, 161Tb emits fewer photons than 111In. These promising characteristics warrant the use of 161Tb in clinical trials.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was funded by the Institut National de la Santé et de la Recherche Médicale (INSERM) under contract PhysiCancer “MICRONAUTE project” and by the French Investment for the Future program within LabEx TRAIL ANR-10-LABX-57. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Keith Eckerman for helpful discussions regarding the ICRP-107 data files.
Footnotes
Published online Feb. 9, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 25, 2015.
- Accepted for publication January 26, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Localized In Vivo Prodrug Activation Using Radionuclides
- Localized in vivo prodrug activation using radionuclides
- Clinical Trial Protocol for VIOLET: A Single-Center, Phase I/II Trial Evaluation of Radioligand Treatment in Patients with Metastatic Castration-Resistant Prostate Cancer with [161Tb]Tb-PSMA-I&T
- Comparison of the tolerability of 161Tb- and 177Lu-labeled somatostatin analogues in the preclinical setting
- Is 161Tb Really Happening?
- Gadolinium-Based Nanoparticles Sensitize Ovarian Peritoneal Carcinomatosis to Targeted Radionuclide Therapy
- Albumin-Binding and Conventional PSMA Ligands in Combination with 161Tb: Biodistribution, Dosimetry, and Preclinical Therapy
- Membrane and Nuclear Absorbed Doses from 177Lu and 161Tb in Tumor Clusters: Effect of Cellular Heterogeneity and Potential Benefit of Dual Targeting--A Monte Carlo Study
- Membrane and Nuclear Absorbed Doses from 177Lu and 161Tb in Tumor Clusters: Effect of Cellular Heterogeneity and Potential Benefit of Dual Targeting--A Monte Carlo Study
- 161Tb-DOTATOC Production Using a Fully Automated Disposable Cassette System: A First Step Toward the Introduction of 161Tb into the Clinic
- First-in-Humans Application of 161Tb: A Feasibility Study Using 161Tb-DOTATOC
- Therapeutic Efficacy Evaluation of Pegylated Liposome Encapsulated With Vinorelbine Plus 111In Repeated Treatments in Human Colorectal Carcinoma With Multimodalities of Molecular Imaging
- Expression of Gastrin-Releasing Peptide Receptor in Breast Cancer and Its Association with Pathologic, Biologic, and Clinical Parameters: A Study of 1,432 Primary Tumors