


Abstract
The challenge for internal therapy is to deliver the highest possible dose to the tumor while sparing normal organs from damage. Currently, the potential risk of kidney and red marrow toxicity limits the amount of radioactivity that may be administered. An accurate dosimetry method that would provide reliable dose estimates to these critical organs and to tumors before therapy would allow the clinician to plan a specific therapeutic regimen and also select those patients who would benefit the most from treatment. The dosimetry for 90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid-d-Phe1-Tyr3-octreotide is usually based on quantitative imaging at different time points that provides information on activity retention in organs over time and on stylized models representing average individuals. Because the therapeutic agent labeled with 90Y is not suitable for quantitative imaging, the peptide surrogate labeled with the positron emitter 86Y can be considered the most appropriate tracer for measuring distribution and retention of the radiopharmaceutical over time. Dose calculations in target organs are generally performed using the MIRDOSE program, in which S values from source to target are integrated. Significant improvement of dose estimates may be achieved by introducing patient-specific adjustments to the standard models. The use of individual kidney volumes assessed by CT instead of the use of a fixed volume for males and females may significantly improve the determination of kidney radiation doses. The use of actual CT-derived tumor volumes has also shown a dose–efficacy relationship. Additional improvements in this field include the validation and use of an 111In surrogate to avoid the complexity of 86Y use and the consideration of radiobiologic parameters, such as fractionation effects and the specific biologic efficacy of internally deposited radiation, which are probably underestimated using currently available methods.
The recent availability of radiolabeled somatostatin analogs opened a new avenue for therapy of several tumor types bearing a high density of somatostatin receptors (SSR). Until now, the attention has been mainly focused on tumors expressing SSR2, such as neuroendocrine tumors. In the near future, other radiolabeled analogs binding to other receptor subtypes or to other hormone receptors will become available (1).
The challenge of this type of therapy is to deliver the highest possible radiation-absorbed dose to the tumor(s) while sparing normal organs from radiation damage. In the case of neuroendocrine tumors, clinical trials have been conducted with several compounds, including 90Y-[DOTA]-d-Phe1-Tyr3-octreotide (90Y-DOTATOC, OctreoTher) and 111In-diethylenetriaminepentaacetic acid (DTPA)-d-Phe1-octreotide (111In-DTPA-OC; OctreoScan111, or SomatoTher). Satisfactory therapeutic results were noted with objective tumor responses or stabilization in patients with progressive disease. However, significant toxicity was also noted. Acute toxicity remained limited, but delayed toxicity was observed, leading to substantial morbidity. In the case of administration of very high activities of 111In-DTPA-OC, bone marrow toxicities in the form of myelodysplastic syndromes and leukemia were reported (2). With 90Y-DOTATOC, reported toxicity was mainly renal, with a significant impairment of renal function and some patients evolving to end-stage renal failure and hemodialysis (3–5). This was particularly true in the phase of early human use, when no attempts at dosimetry were made. Infusion of large amounts of amino acids was proposed to reduce the radiation dose to kidneys by a factor of 20%–40% (6). With dose escalation, however, bone marrow irradiation levels may become critical and also may lead to delayed myelotoxicity.
An accurate knowledge of actual radiation doses to tumor tissues as well as to normal organs would be of great help in planning for therapy. Such knowledge might also aid in predicting which patients might better benefit from the treatment and in identifying those with unfavorable dosimetry. To be optimal, such estimations require time-consuming and sophisticated methods, including pharmacokinetic, biodistribution, and washout studies using the pharmaceutical and the radionuclide to be used for therapy. This may be impossible for practical reasons related to the patient’s status and for physical reasons. In the case of 90Y-DOTATOC, the β-emission of 90Y does not allow appropriate quantification from the brehmsstrahlung emission. Alternative approaches are therefore envisioned, including imaging with similar analogs or using the same analog labeled with a positron emitter used as a surrogate for the therapeutic radionuclide (e.g., 86Y).
This article reviews experience by several investigators in the estimation of radiation doses to tissues and tumors during therapy with 90Y-labeled somatostatin analogs. Methodologic aspects are emphasized, such as the choice of the radiopharmaceutical, acquisition and processing of data, and dosimetry calculations, usually based on the MIRD formula. Also included is an overview of results reported on radiation doses to kidney, bone marrow, and tumors, as well as to other potential target organs.
CHOICE OF RADIOPHARMACEUTICAL
Because 90Y cannot be imaged accurately to ensure correct quantification of organ activity, different approaches are used to mimic the biodistribution of 90Y-DOTATOC and predict its dosimetric parameters.
The chemical structure (hydrophilicity of the molecule and charge) of the radiolabeled analog is important, because it influences tumor uptake, urinary clearance, renal retention, and residence times in tissues (7,8). The ideal method for mimicking 90Y-DOTATOC is to use the same compound labeled with the positron-emitter 86Y. In this case, the chemical structure of the compound is totally preserved. In 24 patients who were candidates for therapy with 90Y-DOTATOC, we studied the pharmacokinetics and biodistribution of 86Y-DOTATOC (9). Using the same methodology, Förster et al. (10) reported data on 3 patients. However, this application is limited, because it requires a PET facility and a high-energy cyclotron. Moreover, the short half-life of 86Y (14.3 h) does not enable delayed acquisitions beyond 48–72 h after tracer administration. To overcome this problem, biodistribution studies were performed using the commercially available 111In-DTPA-OC to predict the behavior of 90Y-DOTATOC. Results were contradictory. Förster et al. (10) showed an overestimation of renal radiation doses using 111In-DTPA-OC when compared with 86Y-DOTATOC, but they observed a good correlation between both radiopharmaceuticals in individual patients. In our experience, 111In-DTPA-OC clearly underestimates 90Y-DOTATOC renal dose compared with 86Y-DOTATOC, and we found a weak correlation between dose estimates for 90Y-DOTATOC with both tracers as a result of intrapatient variation (11). The differences between the 2 studies were probably related to the acquisition method for 111In-DTPA-OC (SPECT vs. planar) and to the use of amino acid infusion.
The last approach used to mimic 90Y-DOTATOC was reported by Cremonesi et al. (12), who used DOTATOC labeled with 111In. This radiopharmaceutical allows γ-camera imaging, which is accessible everywhere, although the chemical behavior of the analog labeled with 111In is not identical to that of the analog labeled with 90Y.
DOSE CALCULATION METHODOLOGY
In internal radiotherapy the dose (Dt) to a target tissue (t) is defined as:
 where Ns = number of decays occurring in the source tissue s, and S factor St←s = energy transported per decay from the source tissue s to a unity mass of the target tissue t.
where Ns = number of decays occurring in the source tissue s, and S factor St←s = energy transported per decay from the source tissue s to a unity mass of the target tissue t.
Thus, patient-specific dosimetry requires quantitative patient imaging at different time points to evaluate the retention of activity in various organs over time. After integration of the measured activities, these time integrals of activity are multiplied by energy transport factors to obtain radiation dose estimates in target organs.
Because continuous patient imaging is not feasible, the determination of source organ activities over time is usually achieved by interpolation between the data collected at specific time points and further extrapolation to infinity beyond the last measurement. For generation of such time–activity curves, a set of linear and exponential segments or a smooth curve derived from a compartment model can be used. To minimize the risk of an inaccurate extrapolation that could lead to significant under- or overestimation of the dose to target organs, it is recommended that data points be collected to cover 3 effective half-lives of the therapeutic compound (13). Alternatively, a conservative approach may be chosen by assuming that, beyond the last measurable time point, the compound is retained in the organ and that the activity is declining only by radioactive decay.
As previously discussed, the therapeutic compound DOTATOC labeled with 90Y, a pure β-particle emitter, is not suitable for quantitative imaging. The substitution of an isotope of yttrium (86Y, a positron emitter) emitting an in vivo detectable particle provides an appropriate surrogate to predict the in vivo behavior of the therapeutic compound 90Y-DOTATOC. Positron emitters allow the use of PET imaging that provides increased quantitative accuracy and spatial resolution. Unfortunately, the decay characteristics of 86Y also involve 2 drawbacks requiring careful attention. First, 86Y also emits a high number of prompt γ-rays responsible for overestimations of activity that may reach 100% and 80% in the background and kidneys, respectively, when not properly accounted for. This is particularly true in 3-dimensional-mode acquisition. Several correction methods have been described, including a simple background subtraction or a sinogram tail subtraction (14,15). We proposed a patient-dependent correction method based on sinogram tail fitting using an 86Y point spread function library, which was shown to significantly improve the accuracy of quantification (16). Second, the relatively low branching (33%) and short physical half-life of 86Y (14.6 h) result in a very low counting rate at 48 h after injection, which implies that beyond this time point activities can be estimated only by extrapolation.
Two somatostatin analogs labeled with 111In, a single-photon emitter, were used in dosimetry studies (10,12). Despite the lower sensitivity of SPECT compared with PET, the longer physical half-life (67.4 h) of this radionuclide allows collection of data up to at least 72 h. In addition to the fact that minor structural changes (metal or metal chelator) may lead to significant changes in biodistribution characteristics, it remains an arduous task to obtain accurate quantitative measurements with single-photon imaging (7,17). Planar acquisitions should be avoided, because they do not allow the actual delineation of organs of interest. The major drawback of quantification with SPECT arises from the important contribution (up to 40%) of scattered γ-rays. No accurate correction has been proposed, especially when the 2 energy peaks must be recorded to preserve the counting rate. The use of an effective attenuation coefficient or the subtraction of events acquired in a lower energy window are the most widely used techniques for scatter correction (18). When the attenuation coefficient map is known, an exact attenuation correction theoretically can be performed with SPECT using an iterative algorithm. Despite all these drawbacks, the use of an 111In-labeled surrogate remains attractive, because it is commercially available and does not require PET technology.
Once the time integrals of activities in organs of interest are measured, absorbed dose calculations in target organs are generally performed using dedicated software, such as the MIRDOSE program, in which S values from any source to any target are integrated (13,19). Although age- and sex-specific reference data for human anatomy are included in the program, the estimated doses derived are far from patient-specific or even accurate, because they take into account neither patient-specific differences in organ shape or size nor nonuniform distribution of activity within the source organs. It is also important to remember that when the absorbed dose in a target is mainly related to self-irradiation (source = target), the S factor highly depends on the target volume. Because of the short range of 90Y decay particles, S factors for targets with a mass greater than 1 cm3 are almost inversely proportional to the target volume. A good approximation is to measure the volume of the patient tissue and rescale the dose obtained from standard man or woman S factors (13). Significant improvement in the accuracy of measured doses may thus be achieved by precise organ volume measurement with use of high–spatial-resolution techniques such as CT or MR imaging.
Finally, it should be remembered that toxicity results from a competition between DNA damage and enzymatic repair mechanisms (20,21). This is related to the ratio between the dose rate and the DNA repair half-time and can be described by the linear–quadratic model (20). Although correlation between biologic effects and radiation doses can be estimated in healthy people after radiation accidents or in patients treated by external beam radiotherapy, the dose rate with 90Y internal radiotherapy (with a half-life of 62 h) may vary significantly and must be considered for estimation of the biologic effects (21–23). Recent data on low-dose hyperradiosensitivity-inducible radiation repair could also have significant implications for the understanding of the relationship between toxicity and absorbed dose. Studies by Joiner et al. (24) identified a region of high sensitivity in the radiation survival response of mammalian and human cells at doses lower than 0.5 Gy with low dose rates. This hypersensitivity phenomenon is observed with low linear energy transfer (LET) radiation (e.g., x- and γ-rays) but not with high-LET radiation (e.g., neutron beams). Studying the survival of CA20948 rat pancreatic tumor cells incubated with increasing amounts of 131I leading to doses of 1–10 Gy, Verwijnen et al. (25) found no hypersensitivity effects. Additional studies are needed to evaluate whether and to what extent low-dose hypersensitivity occurs in human tissues during internal therapy using peptide analogs labeled with a β-particle emitter such as 90Y.
KIDNEY DOSIMETRY
The kidney is the major critical organ during therapy with 90Y-DOTATOC. Once filtered by glomeruli, radiolabeled peptides are reabsorbed and retained in proximal tubular cells (6,26). Although kidney uptake is limited, renal toxicity can occur because of irradiation of the radiosensitive glomeruli by activity present in the radioresistant tubular cells (3–5). Thrombotic microangiopathy is the main histologic finding related to sublethal endothelial cell irradiation (4). With external beam radiotherapy, it is recommended that a kidney absorbed dose of 23 Gy not be exceeded. This is the absorbed dose that has been shown to induce a 5% risk of nephrotoxicity at 5-y follow-up (23). Whether this holds true for internal irradiation remains unclear.
In vivo studies showed a wide inter-patient variability of 86Y-DOTATOC kidney uptake, supporting the need to perform direct individual measurements. In 4 patients, no uptake could be delineated in the kidney on PET imaging. These patients were assumed to be able to receive high activities without a risk of renal side effects. In others, the renal uptake, mean residence times (MRTs), and, therefore, radiation doses varied by a factor of 4 (range, 1.2–5.1 mGy/MBq) (9). The same variability in renal absorbed doses (range, 2.9–5.7 mGy/MBq) was reported by Bodei et al. (27) in a series of 6 patients who underwent dosimetry studies with 111In-DOTATOC without amino acid infusion.
We treated a series of 60 patients after individual kidney dose estimation using 86Y-DOTATOC imaging and the MIRDOSE3.1 model. Despite the fact that the activities administered to each patient were calculated so that the expected doses delivered to the kidneys would not exceed a fixed limit of 27 Gy, various degrees of nephropathy were experienced by 5 patients, with 1 patient on hemodialysis at 5-y follow-up. We investigated possible factors that could affect the accuracy of pretherapeutic dose estimates. The most important of these seems to be the actual kidney volume. Indeed, the MIRDOSE model refers to standard kidney volumes for males and females (288 and 264 mL, respectively). Retrospective determination of individual kidney volumes on pretherapeutic CT images in 25 patients showed high interindividual variability (range, 231–503 mL), indicating that individual kidney volume determination might be crucial to improve the determination of kidney radiation doses. Taking the actual renal volume measured by CT into account resulted in a median undercorrection of the absorbed dose by 11%. However, patients who developed renal toxicity had significantly smaller kidneys as assessed by CT and, in fact, received significantly higher kidney doses compared with patients who experienced no renal toxicity.
Methods usually proposed to estimate organ-absorbed doses require the assumption of a homogeneous activity distribution over the entire organ. In a recent improvement of the MIRD model, Bouchet et al. (28) proposed a multiregion model for the kidney, including 4 main homogeneous regions as source/target: cortex, medulla, pelvis, and papillae. The kidney dose estimates could be made more patient-specific by rescaling the 4 kidney regions on the basis of the actual kidney volume measured by CT or MR imaging. To make use of this model, it is essential to know the activity distribution inside the kidney. Unfortunately, this can not be achieved by quantitative radionuclide imaging because of the lack of spatial resolution of PET and SPECT cameras. However, a more precise pattern of activity distribution inside the kidney has been established by ex vivo studies. Autoradiography of a human kidney obtained after in vivo injection of 111In-labeled somatostatin analog showed radioactivity to be concentrated predominantly in the juxtamedullary region of the cortex (29,30). Transposing this heterogeneous pattern of activity in a voxel-based model, the authors showed a 2-fold increase in the dose estimates in 29% of the cortex volume compared with the estimates produced by a single-region model assuming a homogeneous organ activity distribution.
Other factors that may influence the radiobiologic effects of internal irradiation should also be taken into consideration. As noted previously, in fractionated external beam therapy, the dose limit causing a 5% probability of radiation nephropathy within 5 y has been found to be 23 Gy. This dose is typically given at a high dose rate in fractions of 1.5–2 Gy. In contrast, during 90Y-DOTATOC therapy, radiation exposure is continuous and exponentially decaying with an effective half-life of 48 h. It was recently suggested that the linear–quadratic model could be used to transpose the external beam therapy dose limit (23 Gy) to a corresponding limit for radionuclide therapy with 90Y-DOTATOC. According to this model, which takes into account the rate and fractionation of the dose, the 5% level of probability of nephrotoxicity shifts from the 23 Gy threshold for external beam therapy to 35 ± 7 Gy for 90Y-DOTATOC (31).
Thus, the actual dose to the glomeruli may be twice that estimated with the classic MIRD model based on fixed kidney size and homogeneous activity distribution within the whole organ. On the other hand, the maximum tolerable kidney dose for internal radiotherapy with 90Y-DOTATOC therapy is significantly higher than the dose limit for external beam therapy.
RED MARROW
Assessment of red marrow dosimetry in internal radiotherapy is of great importance (32). With red marrow irradiation, we are entering another world in terms of dose assessment. For most organs, significant toxicity may occur for delivered doses of some 10s of Gy, whereas doses as low as 3 Gy to the red marrow induce 1% of leukemia within 10 y after exposure, and the probability of survival decreases rapidly beyond 4 Gy to reach an LD50 (death of 50% of individuals) between 5 and 6 Gy (33). This implies that the red marrow maximal tolerated dose will be reached for a specific uptake much lower than the uptake in other organs. Another hurdle in estimating the red marrow absorbed dose is its nonhomogeneous nature, with a complex mixture of trabecular bone, cortical bone, active red marrow, and inactive marrow. Improvements to the MIRD model were proposed to take this microstructure into account in S factor computation (34).
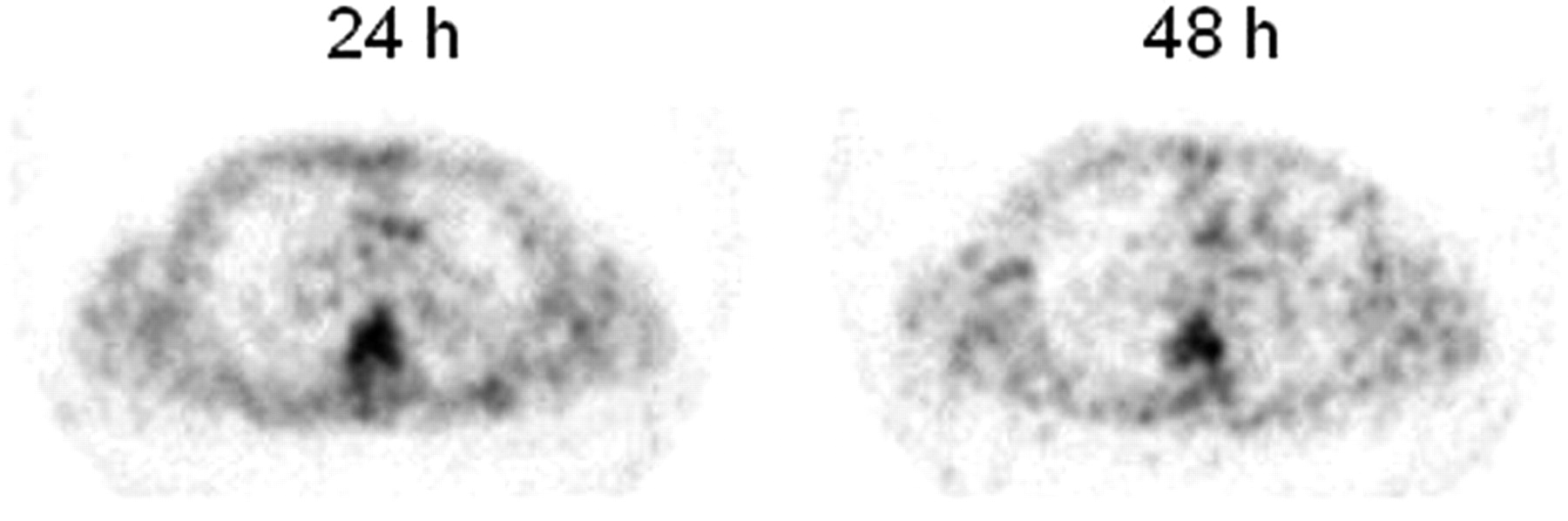
It was originally reported that no specific uptake in red marrow was noted on 111In-DTPA-OC scan, and red marrow activity was assumed to be a fraction of plasma activity or equal to the remainder of the body (10,12). Recent studies using 86Y-DOTATOC and PET showed that somatostatin analogs are also taken up in the red marrow but not in the trabecular or cortical bone (Fig. 1) (35). The mechanisms of uptake are not entirely elucidated and may include specific binding to SSR, transchelation of the metal label to transferrin, or plasma activity.
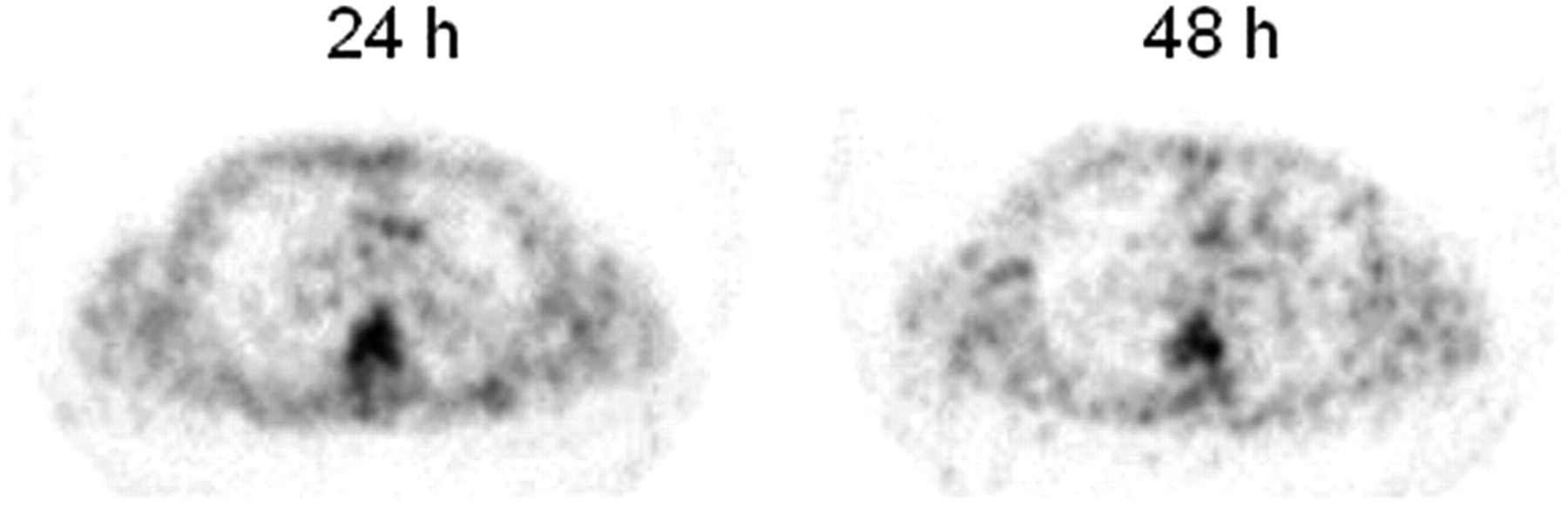
Transverse PET slices through the chest obtained 24 and 48 h after injection of 0.4 GBq of 86Y-DOTATOC. Note the clear uptake over the spine area, whereas areas without active red marrow, such as the humerus, were not visualized.
To avoid direct superimposition of organ activity or cross-contamination by scatter γ-rays, it is recommended that the red marrow be measured over a segment of the thoracic spine region and rescaled to the whole red marrow mass using the standard fraction of active red marrow present in the thoracic spine (32,35). The delivered dose can than be computed using the correction of the MIRDOSE program using MRTs as input (36).
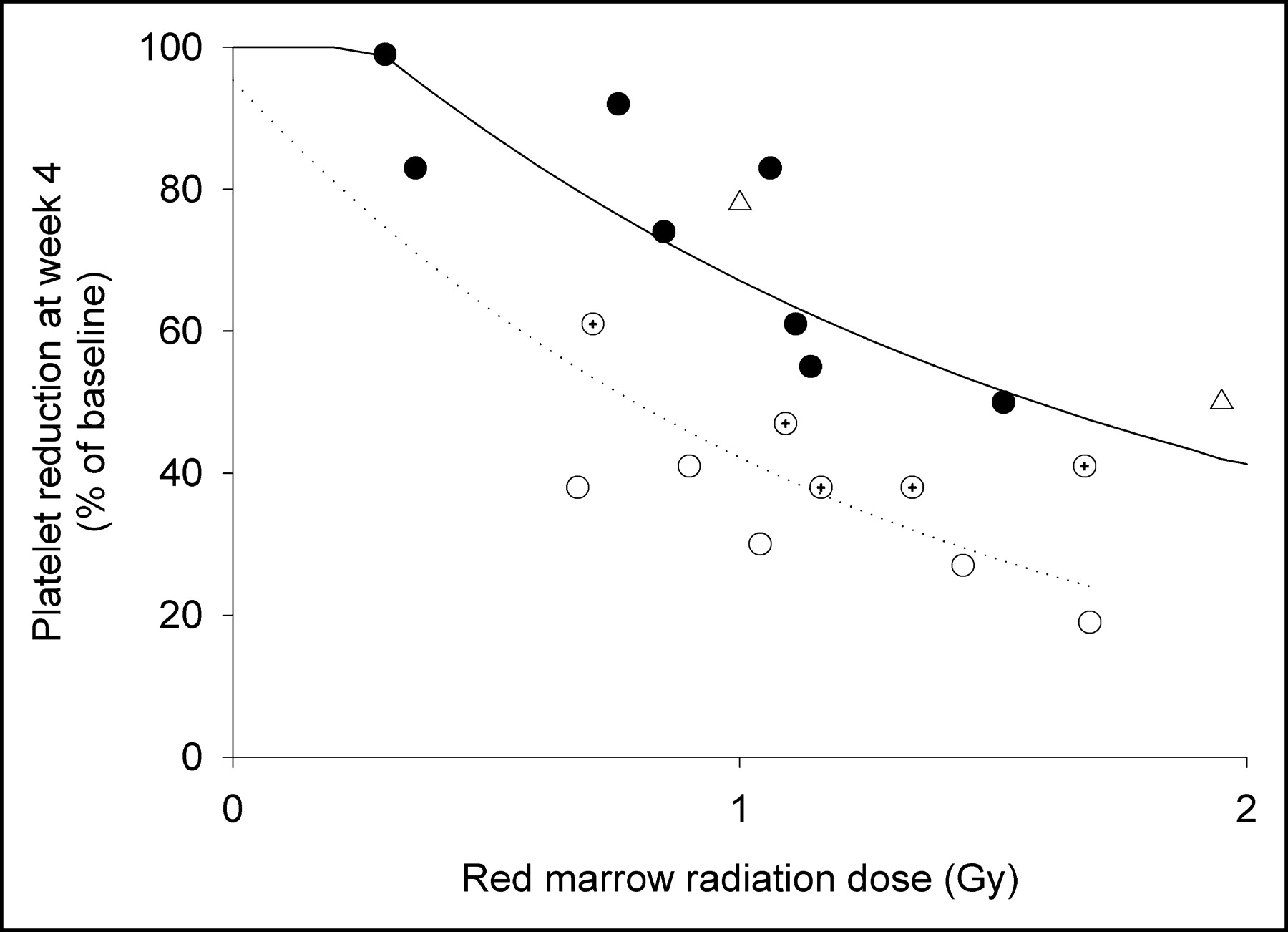
Studies showed that planar imaging techniques for 90Y-labeled antibodies binding to red marrow improved the correlation between myelotoxicity and estimated dose delivered to red marrow (32,37). Some authors suggested that, to predict the myelotoxicity as a function of the delivered dose to the red marrow, patients should first be sorted into populations with different red marrow sensitivities (Fig. 2) (37–40).
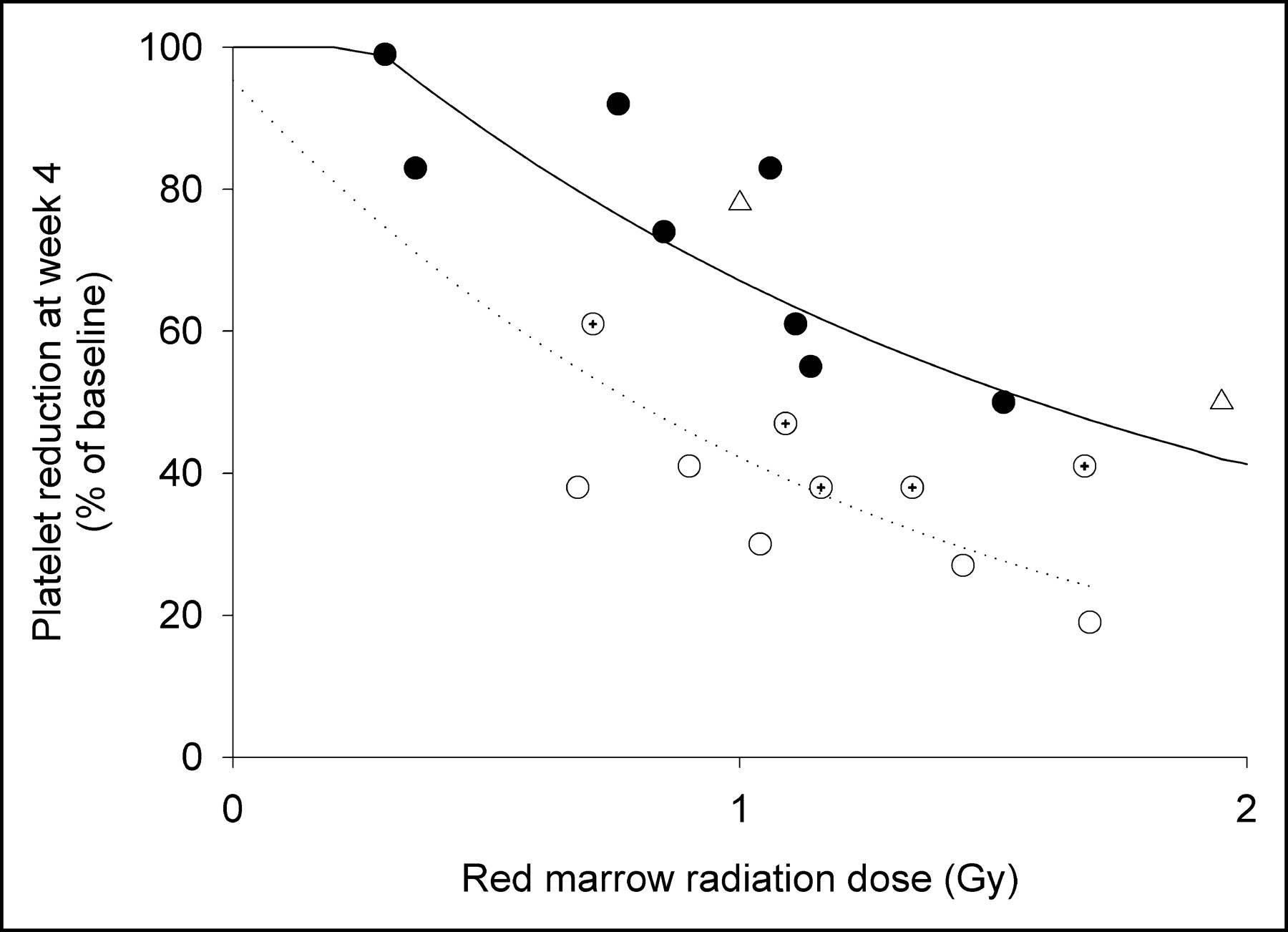
Correlation between the platelet count nadir observed after 90Y-DOTATOC therapy and the red marrow radiation doses estimated using 86Y-DOTATOC. • = patients with subsequent complete platelet count recovery; ○ = patients with a partial platelet count recovery; ⊕ = patients who previously underwent chemotherapy but did not completely recover their platelet counts; ▵ = platelet count nadir observed in radiation accident in healthy individuals.
Investigations after radiation accidents in healthy people showed that for sublethal doses the platelet count recovery (PCR) 6 wk after irradiation was almost complete (21,22). In 90Y-DOTATOC therapy, the platelet count nadir (PCN) for patients with a normal PCR as a function of the red marrow dose, estimated using 86Y-DOTATOC PET, was in good agreement with observations in radiation accidents (Fig. 2) (35). In contrast, patients with an incomplete PCR already presented an abnormally low PCN. Half of those patients had undergone chemotherapy, known to alter the red marrow reserve. No patients with normal PCRs had undergone chemotherapy.
OTHER ORGANS
For technical reasons, quantification of other organs using the methodology described here is not feasible. Accurate estimation of liver exposure to internal irradiation is hampered by the almost constant and often bulky presence of liver metastases. Absorbed doses to the pituitary and thyroid cannot be precisely measured because of the small size of the organs. However, scintigraphic images show lower uptakes in all these organs than in the kidneys, probably resulting in an absorbed dose far below 20 Gy. Such doses should not be deleterious to these organs. This may not be the case for the testes, which probably receive a substantial radiation dose as illustrated by the drop in inhibin B levels after treatment with 90Y-DOTATOC (41).
TUMOR DOSE–RESPONSE RELATIONSHIPS
Despite differences in the protocols used, tumor size reduction of at least 25% (range, 10%–30%) has been reported in most studies with 90Y-DOTATOC (27,42–44). This relatively low rate of complete or partial response is a result of the fact that neuroendocrine gastroenteropancreatic tumors are usually radioresistant and also because there is a limit to the therapeutic activities that can be delivered safely. There is a need for predictive parameters that could help the clinician select more appropriate candidates for treatment and, conversely, identify those patients who would not benefit from such treatment.
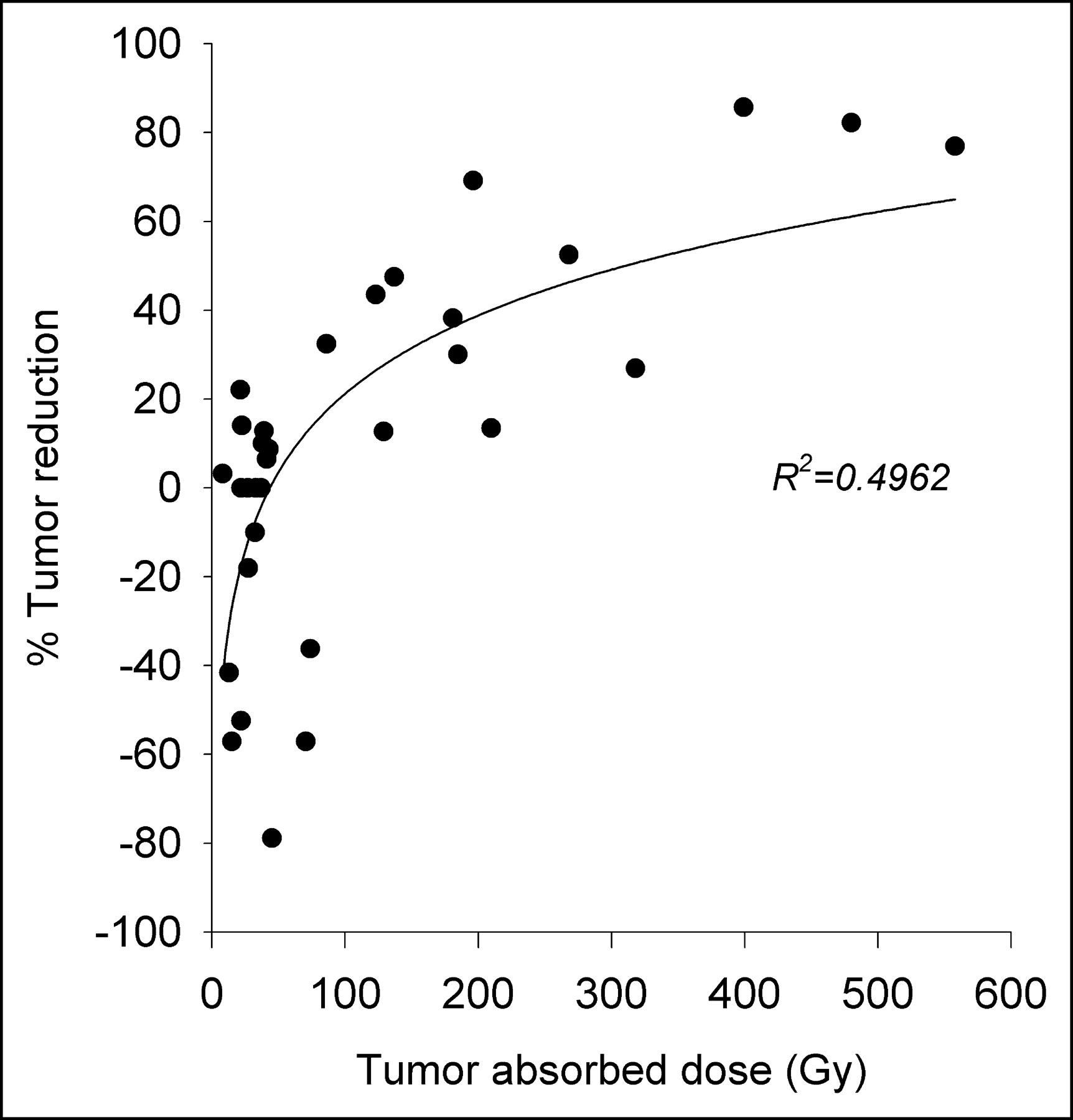
In a subset of 13 patients treated with 90Y-DOTATOC, we found a significant correlation between dose estimates to the tumors and the tumor size reduction measured at the end of the treatment (Fig. 3) (45). A similar correlation between tumor dose and response was still present 1 y after end of treatment. Dose estimates were derived from quantitative PET with 86Y-DOTATOC, and the MIRDOSE spheric model was refined by using the actual tumor sizes measured by CT. The median absorbed dose was 6-fold higher in responding tumors (232 Gy) than the median value in nonresponding tumors (37Gy). It is noteworthy that in only 20% of the nonresponding tumors, dose estimates were in the range of those in responding tumors. Although obtained in a limited number of patients, these dose–response relationships suggest the potential usefulness of tumor dosimetry in the management of patients with neuroendocrine tumors.
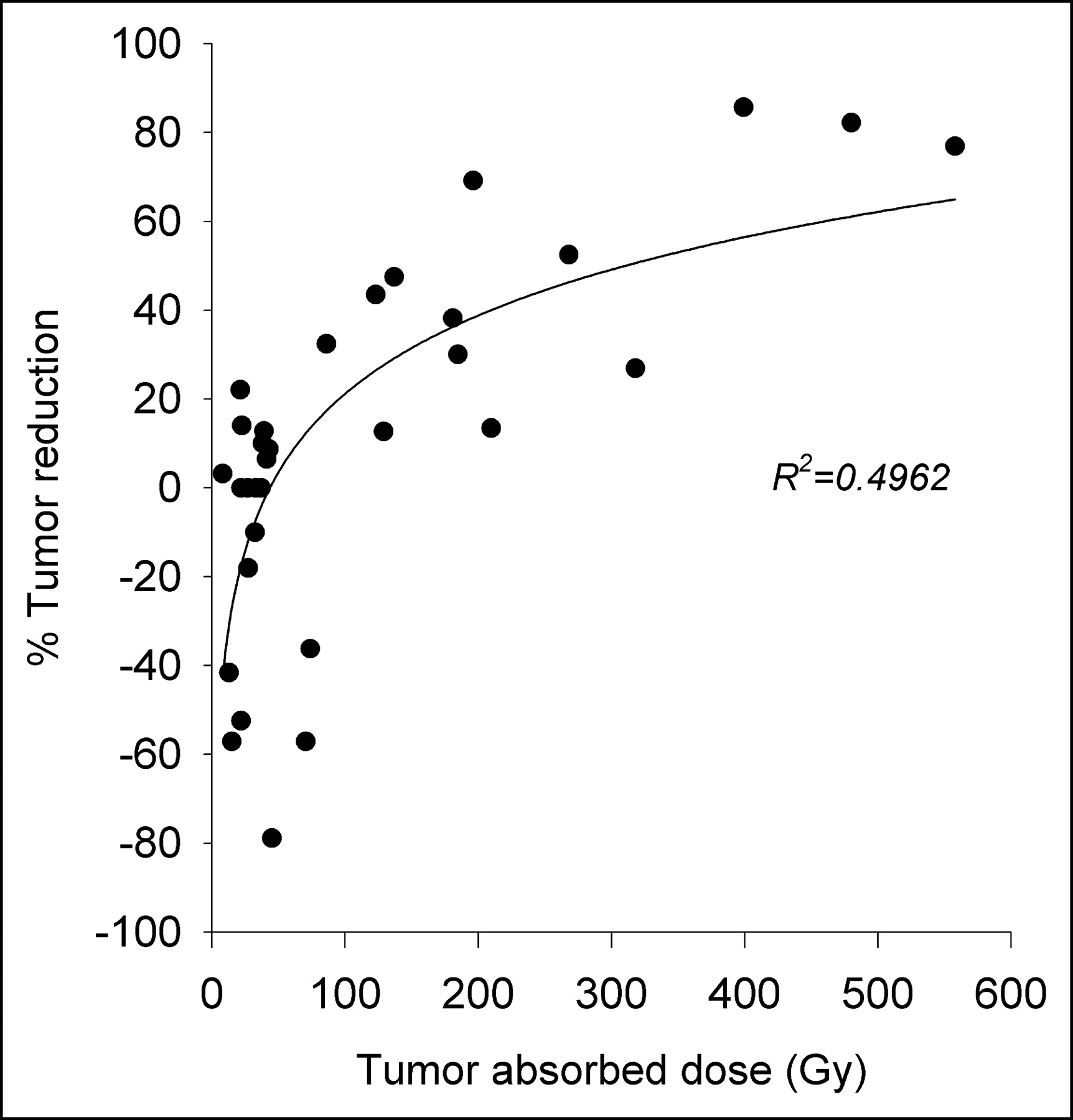
Tumor dose–response relationship in 13 patients treated with 90Y-DOTATOC. Tumor volumes were assessed by CT before and after treatment. Tumor dose estimates were derived from CT scan volume measurements and quantitative 86Y-DOTATOC imaging performed before treatment. Data were further computed using the MIRDOSE spheric model.
CONCLUSION
Although it is clear that accurate prediction of absorbed doses is required for internal radiotherapy, methods developed up to now do not enable a simple approach. Even with sophisticated techniques, inaccuracies can occur and result in overestimation of the absorbed doses, resulting in undertreatment, or in underestimation, resulting in overtreatment and unpredicted toxicity. One of the major unknowns in internal dosimetry is the effect on cells of very low dose rates and of low-energy γ- and x-ray emissions. Additional research is needed in this field.
Footnotes
Received May 19, 2004; revision accepted Sept. 13, 2004.
For correspondence or reprints contact: Stanislas Pauwels, MD, PhD, Centre de Médecine Nucléaire, Université Catholique de Louvain, UCL 54.30, Avenue Hippocrate, 54, B-1200 Brussels, Belgium.
E-mail: stanislas.pauwels{at}mnuc.ucl.ac.be
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prediction of 177Lu-DOTATATE PRRT Outcome Using Multimodality Imaging in Patients with Gastroenteropancreatic Neuroendocrine Tumors: Results from a Prospective Phase II LUMEN Study
- Dosimetric Quantities in Neuroendocrine Tumors over Treatment Cycles with 177Lu-DOTATATE
- Reimbursement Approaches for Radiopharmaceutical Dosimetry: Current Status and Future Opportunities
- Tumor Response to Radiopharmaceutical Therapies: The Knowns and the Unknowns
- 64Cu-SARTATE PET Imaging of Patients with Neuroendocrine Tumors Demonstrates High Tumor Uptake and Retention, Potentially Allowing Prospective Dosimetry for Peptide Receptor Radionuclide Therapy
- Technical Advances in Image Guidance of Radionuclide Therapy
- Clinical History of the Theranostic Radionuclide Approach to Neuroendocrine Tumors and Other Types of Cancer: Historical Review Based on an Interview of Eric P. Krenning by Rachel Levine
- Red Marrow-Absorbed Dose for Non-Hodgkin Lymphoma Patients Treated with 177Lu-Lilotomab Satetraxetan, a Novel Anti-CD37 Antibody-Radionuclide Conjugate
- Dose Response of Pancreatic Neuroendocrine Tumors Treated with Peptide Receptor Radionuclide Therapy Using 177Lu-DOTATATE
- Hepatic arterial infusion enhances DOTATOC radiopeptide therapy in patients with neuroendocrine liver metastases
- RADAR Commentary: Evolution and Current Status of Dosimetry in Nuclear Medicine
- 4-Step Renal Dosimetry Dependent on Cortex Geometry Applied to 90Y Peptide Receptor Radiotherapy: Evaluation Using a Fillable Kidney Phantom Imaged by 90Y PET
- 131I-Tositumomab Radioimmunotherapy: Initial Tumor Dose-Response Results Using 3-Dimensional Dosimetry Including Radiobiologic Modeling
- MIRD Pamphlet No. 20: The Effect of Model Assumptions on Kidney Dosimetry and Response--Implications for Radionuclide Therapy
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- Potential Increased Tumor-Dose Delivery with Combined 131I-MIBG and 90Y-DOTATOC Treatment in Neuroendocrine Tumors: A Theoretic Model
- Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues
- 89Zr as a PET Surrogate Radioisotope for Scouting Biodistribution of the Therapeutic Radiometals 90Y and 177Lu in Tumor-Bearing Nude Mice After Coupling to the Internalizing Antibody Cetuximab
- Patient-Specific Dosimetry in Predicting Renal Toxicity with 90Y-DOTATOC: Relevance of Kidney Volume and Dose Rate in Finding a Dose-Effect Relationship
- Dosimetry of Internal Emitters
- Long-Term Follow-Up of Renal Function After Peptide Receptor Radiation Therapy with 90Y-DOTA0,Tyr3-Octreotide and 177Lu-DOTA0, Tyr3-Octreotate
- Molecular Imaging as In Vivo Molecular Pathology for Gastroenteropancreatic Neuroendocrine Tumors: Implications for Follow-Up After Therapy