


Abstract
Radiopharmaceutical therapy (RPT) is defined as the delivery of radioactive atoms to tumor-associated targets. In RPT, imaging is built into the mode of treatment since the radionuclides used in RPT often emit photons or can be imaged using a surrogate. Such imaging may be used to estimate tumor-absorbed dose. We examine and try to elucidate those factors that impact the absorbed dose–versus–response relationship for RPT agents. These include the role of inflammation- or immune-mediated effects, the significance of theranostic imaging, radiobiology, differences in dosimetry methods, pharmacokinetic differences across patients, and the impact of tumor hypoxia on response to RPT.
Treatment for almost all patients with metastatic cancer is a balance between preventing or mitigating cancer progression and managing often severe, treatment-induced toxicity. One way to achieve this balance is to modulate delivery of treatment. Typically, a treatment course of cytotoxic drugs is administered over multiple cycles, spanning weeks to months. A treatment cycle is defined as drug administration followed by a rest period to recover from treatment toxicity. If, after the initial treatment course, disease progresses, oncologists offer subsequent lines of cytotoxic drugs, usually with diminishing therapeutic benefit for the patient and significant toxicity. It is unsurprising, then, that we have devoted substantial resources to developing new cancer drugs. The failure rate of cancer medication from first-in-humans trial to Food and Drug Administration approval is 97% (1). These trials are largely dominated by targeted agents. Among the factors contributing to this high failure rate is the misunderstanding of mechanism of action; remarkably, the observed therapeutic effect of many targeted investigational biologic agents is through off-target effects (2). Efforts to push the limit on patient treatment with these agents has shifted the balance to conclude that stable disease, as measured by axial CT of an index lesion, is a desirable goal despite significant toxicities. The result, then, is a treatment paradigm focused largely on managing toxicity. Treatment toxicity cannot be predicted for an individual patient. To manage potential toxicity, treatment is protracted and typically delivered in cycles over several weeks to months. The interval between cycles allows an assessment of toxicity in each patient and dose adjustment for the subsequent cycle to avert treatment-induced morbidity. This empiric approach to individual-patient therapy has been adopted as the mainstay for the management of cancer patients and is appropriate for a treatment modality that is untargeted or cannot quantify tumor–versus–normal-tissue targeting. Radiopharmaceutical therapy (RPT) is defined by the delivery of radioactive atoms to tumor-associated targets. Cell killing is achieved by delivering ionizing radiation, a treatment modality that has been used for almost 100 years and whose mechanism of action (i.e., induction of DNA damage) is well understood and potentially less sensitive to compensatory cell-signaling networks that are activated when perturbed by small-molecule inhibitors, for example. This long history and understanding make it possible to focus on characterizing the interplay between immune-mediated or tumor microenvironmental effects and overall tumor or normal-organ response. In external-beam radiotherapy (EBRT), significant improvements in efficacy without increasing toxicity arose with the adoption of image-guided radiotherapy (3). In RPT, imaging is built into the mode of treatment since the radionuclides used in RPT often emit photons. Photon emissions may be imaged by nuclear medicine modalities (e.g., SPECT or PET) to assess the distribution of the RPT in each patient. RPT agents that exclusively emit β-particle radiation (e.g., 90Y), which were once thought not to be imageable, have been imaged by SPECT via Bremsstrahlung photon emissions (associated with high-energy β-particle photon radiation emitted during particle deacceleration) and by PET (using the very low positron yield of 90Y) and are used for treatment verification (4–6). Efforts to image and quantify the distribution of α-particle–emitting RPT are ongoing (7,8). Alternatively, a theranostic approach may be adopted wherein a radiotracer is used to demonstrate that the patient’s tumor sites express the RPT target adequately. Such imaging information may be used for dosimetry-driven treatment planning (9–14) and patient selection (the process by which the absorbed dose to tumors or normal tissues is considered in selecting the most appropriate RPT treatment for a given patient or population of patients).
The evidence demonstrating that patient outcomes are improved (or predicted) when dosimetry is included in RPT delivery continues to accumulate (15–22). Notably, quality of life (23) can be better with RPT agents than with conventional treatment modalities (24–29).
Despite these key distinctions, RPT is currently being delivered using traditional paradigms that are driven by managing toxicity rather than fully leveraging the modality’s unique features that make it more than just radioactive chemotherapy. In this work, we focus on tumor response to RPT. We start with a review of current knowledge (the knowns) and then identify those areas that require further research (the unknowns). Such a review is particularly appropriate for RPT since many RPT patients are undertreated and it is imperative that we leverage the unique quantitative tools available for RPTs to yield precision dosing that can improve the therapeutic index for patients with late-stage cancers.
TECHNICAL FACTORS IMPACTING TUMOR-ABSORBED DOSE VERSUS RESPONSE IN RPT
The 4 pillars of the paired diagnostic and therapeutic radiopharmaceuticals are personalized treatment planning, accurate verification of treatment delivery, adaptive treatment optimization, and treatment response evaluation. This aim is achieved through better patient selection by molecular imaging phenotyping (stratification), radiopharmaceutical dose optimization by predictive dosimetry (capability for predicting target engagement at disease sites and off-target toxicities), posttreatment absorbed dose deposition mapping by imaging and dosimetry, and augmentation of therapeutic targeting by adjunct therapies (locoregional such as EBRT or systemic such as additional RPT or adjuvant chemotherapy). These inherent features of RPTs represent opportunities for molecular imaging to broaden the understanding of tumor biology beyond morphologic imaging and pave the way for personalized and precision medicine. The dominant technical factors impacting tumor-absorbed dose versus response in RPT include the accuracy of quantitative imaging, the region delineation process, and uncertainties in the overall dosimetry procedure chain (30,31).
The importance of the verification of target expression by whole-body imaging as a patient-selection criterion for RPT was established in neuroendocrine tumors (NETs) by Kwekkeboom et al. (32). In that study, high tumor uptake, assessed qualitatively by pretreatment planar 111In‐pentetreotide (OctreoScan; Mallinckrodt, Inc.), was one of the independent predictive markers of a favorable treatment outcome after peptide receptor radionuclide therapy (PRRT). Increasing use of PET tracers, with the inherent quantitative ability of PET imaging, has allowed reliable and reproducible measurement of biologic target expression, which in turn has demonstrated the predictive ability of pretreatment molecular imaging in NETs and prostate cancer (33,34). Violet et al. has demonstrated a positive correlation between lesion SUV on pretreatment 68Ga-prostate-specific membrane antigen (PSMA) PET/CT and absorbed dose (estimated by posttreatment 177Lu-PSMA SPECT/CT) that resulted in a biochemical (prostate-specific antigen) response (34). The short half-life of the most commonly used radiotracers, such as 68Ga or 18F, or the uncertain in vivo stability of the longer-half-life radiopharmaceutical has been the main limitation in deriving a meaningful pretreatment dosimetry assessment (35). However, longer-half-life radiotracers such as 124I have made it possible to perform pretreatment (PET-based) dosimetry and, in RPT of thyroid cancer, has been used to confirm successful restoration of NaI symporters after targeting of the driver mutations in radioiodine-refractory thyroid cancer, thereby allowing radioiodine therapy of otherwise non–iodine-avid lesions (36,37). New imaging modalities, such as total-body PET (38), and advances in SPECT instrumentation (39,40) will likely further enhance the utility of pre- and posttherapy imaging in RPT and increase the ability to image the RPT agent itself. In addition, new advances in radiochemistry using longer-half-life radiolabels such as 64Cu (12.7 h) and 89Zr (78.4 h) bound to stable bioconjugates, in vivo, have demonstrated the feasibility of imaging the biologic targets beyond 24 h with PET, further facilitating the pretreatment dosimetry for personalized RPT (41–43).
Tumor heterogeneity and tissue-sampling uncertainties are known limitations of increasingly biomarker-driven treatments in precision oncology (44). These limitations have become apparent by the observation that even in highly selected patient populations (e.g., basket trials) (45), the response rates in patients with a targetable alteration in their tumors was less than 10% (46). Molecular imaging provides a whole-body assessment of the biologic target expression and also its intra- and interlesional nonuniformity. This is of particular interest given the short pathlength (millimeters for β-particles and submillimeter for α-particles) of radiation particles used in RPTs, leading to nonuniform absorbed dose distributions. The prognostic significance of intralesional and interlesional somatostatin receptor expression on pretreatment somatostatin receptor PET in patients undergoing PRRT, and PSMA expression in those undergoing PSMA RPT, has underscored the fundamental role of molecular imaging in therapeutic decisions (47–49). The combination of different radiotracers enables a comprehensive assessment of various target expressions and molecular imaging–derived tumoral heterogeneity, with significant implications for the feasibility and choice of RPTs (50). Screening patients with dual-tracer imaging, including somatostatin receptor and 18F-FDG PET in NETs or PSMA and 18F-FDG and 18F-NF PET in prostate cancer, has significant implications for patient selection for RPT. These implications include guiding selection of biopsy sites, measuring the disease burden of different phenotypes, and eventually providing prognostications (51–56). Molecular imaging has become an integral component of RPT in guiding therapeutic decisions based on imaging phenotype, optimizing RPTs through prospective dosimetry, and avoiding possibly futile therapeutic interventions.
BASIC BIOLOGY FACTORS IMPACTING TUMOR-ABSORBED DOSE VERSUS RESPONSE IN RPT
Although the variability in response to RPT may depend on the RPT itself and the tumor type, the variability is just as likely derived from intrapatient or interpatient variability in tumor size and tumor location (such as bone vs. soft tissue). The microenvironment of the lesion and the tissue within which the lesion is located play a critical role. For example, skeletal metastases of thyroid cancer generally require higher administered activities of radioiodine than do soft-tissue lesions (57,58). Vascular supply to the tumor is critical for ensuring optimal delivery of the RPT to the lesion. Large, solid tumors have necrotic cores as they outgrow the vascular supply, which is mostly limited to the periphery of the tumor. Larger tumors therefore will have limited specific targeting related to receptor or target binding while requiring more of the cross-fire effect for radiation to kill tumor cells located distal from blood vessels. For this reason, combination therapy using radionuclides with short- and long-range emissions or tumors with a mixed vascular supply is consistent with radiobiologic principles. Clinical trial data are needed to confirm that it is a suitable strategy to improve tumor-absorbed dose distribution and response. Certain tumors are inherently more vascular, such as renal and lung cancers and melanoma. Neovascular targeting agents can be combined with RPT to better treat tumors by enhancing their radiosensitivity (59). Combinations of tyrosine kinase inhibitors with girentuximab have been used for renal carcinoma (60) and have potential to be used with RPT to enhance efficacy (61). Bevacizumab targets the neovasculature and is also thought to normalize the vasculature, and although RPT delivery in areas of normal vasculature may be retained or enhanced, overall tumor vasculature may be decreased, leading to lower targeted delivery (62). Radiolabeled bevacizumab has been used to target vascular endothelial growth factor–expressing tumors, but data on combination therapy with RPT are lacking (63–65).
The tumor microenvironment plays a key role in regulating radiation response, in addition to regulating cancer growth and progression. Tumors comprise the cellular component and stroma, which includes the extracellular matrix, vascular cells, fibroblasts, and leukocytes, among others. Cancer-associated fibroblasts are known to play a role in radiation resistance mediated via secretion of various signal factors leading to contact-mediated signaling or potentiating prosurvival signal pathways (66,67). In addition, these factors may promote stem cell generation and cause immune modulatory effects (68). Besides, secretory factors such as growth factors, cytokines, and chemokines in the extracellular matrix also lead to complex interactions with cellular components. Cancer-associated fibroblasts regulate adaptive and innate immune cell–mediated effector functions, including CD8-positive T-cell anergy, release of transforming growth factor-β and vascular endothelial growth factor cytokines, and expression of programmed death-ligand 1 (69). The overall response to radiation therefore depends on this complex interaction between the cellular and extracellular environments (70). Radiation leads primarily to cellular DNA damage. However, it is known that radiation effects can be noted on distant sites or areas that are outside the radiation field, known as abscopal effects. These are thought to be a result of radiation-induced immunogenic cell death and induction of subsequent cancer neoantigen-specific immune responses (71,72). Radiation-related abscopal effects are enhanced when used in combination with checkpoint inhibitors (73). CD8-positive cells play a key role in immune modulation, and the presence of CD8-positive T cells is an important prognostic marker. Given this radiation–host immune system interplay, several studies are examining combination EBRT and immune-oncology treatments, though results from randomized trials have been negative to date (74,75), suggesting we still have much to learn. Studies using RPT and immune-oncology have been initiated (NCT03805594, NCT04261855, NCT03658447).
The inherent radiation sensitivity of the tumor is one of the prime factors that impacts response to radiation. Breast cancer, neuroblastoma, lymphoma, head and neck tumors, and lung tumors are generally radiosensitive. Although not fully understood, the intrinsic radiation sensitivity of a tumor is impacted primarily by the activity of DNA repair pathways. Tumors vary considerably in radiosensitivity, which, in turn, is affected by several factors related to DNA damage and repair, apoptosis, and cellular proliferation. Oncogenes and tumor suppressor genes considerably influence the radiosensitivity. Defects in DNA damage repair and DNA repair signaling mechanisms such as the cell-cycle checkpoint determine radiosensitivity. Several candidate genes associated with deletion or loss of function are implicated in affecting the radiosensitivity of cells. Examples are BRCA1, BRCA2, ATM, ATR, DNA-PK, POLE, mismatch repair deficiencies, and p53. Tumors harboring such mutations may show altered radiosensitivity. Hypoxia in the tumor microenvironment is also a key factor in radiosensitivity. It increases radioresistance, making hypoxic tumors resistant to radiation therapy (76). However, the effect of hypoxia specifically on RPT has not been studied. Although the radiosensitivity is more widely characterized for radiation therapy, RPTs are currently limited to only a few tumor types. Inherent interpatient differences in RPT are likely to be more pronounced, as related to pharmacokinetic factors not operative in EBRT, including the clearance and targeting kinetics of the RPT. The differences in hematologic toxicities provide an example: whereas bone-targeting agents may be expected to cause increased toxicity with greater tumor burden (223RaCl2, PSMA targeting osseous disease, 131I-metaiodobenzylguanidine in neuroblastoma), toxicity may also be related to target expression on hematologic cells (e.g., 177Lu-DOTATATE). The impact of genetic factors (i.e., genes involved in DNA damage repair) versus physiologic factors (pharmacokinetics) on tumor-absorbed dose versus response in RPT has not yet been elucidated. Genomic and proteomic analyses and their correlation with RPT tumor response are ongoing (77,78).
ABSORBED DOSE VERSUS TUMOR RESPONSE IN EBRT
Since RPT is fundamentally a radiation delivery modality, knowledge of tumor-absorbed dose versus response in EBRT is a useful starting point for evaluating absorbed dose versus tumor response in RPT. The traditional approach to radiation delivery in EBRT has been to deliver the total dose in daily 2-Gy fractions. Fractionation in radiotherapy is based on the observation that cells making up nonproliferating normal organs repair radiation-induced DNA damage more quickly than do most cancer cells. In radiobiologic terms, late-responding tissues (e.g., normal tissues) with a typical α/β of less than 4.5 Gy are less susceptible to fractionated radiation delivery than are most cancer cells (typical α/β, >10 Gy) (α and β are parameters of the linear-quadratic model widely used to describe response to radiation [the linear quadratic model is reviewed in a number of publications, such as the MIRD Primer and International Commission on Radiation Units and Measurements report 96 (79,80)]). This approach is important when radiation targeting is suboptimal, delivering substantial radiation to normal tissues during tumor targeting. The reduction in normal-organ radiation exposure with advanced techniques has led to hypofractionation protocols—total dose delivered in fewer fractions, with each fraction greater than 2 Gy.
The response of tumors to a particular absorbed dose delivered by EBRT depends on a host of factors, including tumor histology and stage, tumor volume, fraction of tumor volume irradiated, and fractionation schedule applied. Tumor response itself is reported as locoregional (e.g., tumor volume change, absence of recurrence if given adjuvantly) or global (e.g., reduction in imaging or serum markers or, most importantly for patients, improvement in quality of life or overall survival). Accordingly, Table 1 provides the typical range of doses used in radiation oncology for different cancers. In the selected cases for which response is provided, it is a substantial simplification of the actual anticipated response. In several cases, the absorbed dose is expressed as the biologically effective dose or as the 2-Gy equivalent dose. Both formalisms are intended to account for differences in how the total prescribed tumor-absorbed dose is fractionated. The former yields the absorbed dose to achieve a particular biologic effect if it were delivered in infinitesimally small dose fractions. The latter yields biologic effects seen with a traditional 2-Gy/fraction delivery of radiotherapy. Normal-organ dose limits are described in another paper (81) included in this supplement to The Journal of Nuclear Medicine.
Summary of Tumor-Absorbed Dose vs. Response from EBRT
Table 1 lists typical prescribed radiation doses for different cancer types. Consistent with genomic-based approaches to introducing precision medicine to medical oncology, genomic analysis of individual-patient tumor samples has been explored to assess tumor radiosensitivity in radiotherapy patients, with the intent of using this information to adjust the prescribed dose (82). Although promising, prospective evaluations of such approaches are needed.
CANCER CELL RESPONSE BY CATEGORY
Beyond the specific cancer types listed in Table 1, it is possible to broadly categorize tumors by tumor target and compartment. These broad categories and corresponding tumor characteristics are listed below.
Liquid Tumors (Leukemias, Lymphomas)
Liquid tumors exist within the intravascular, lymphatic, and marrow space and are generally rapidly accessible to intravenously administered RPT. They are radiosensitive because of a short cell-doubling time, tend to be clonal, and often harbor genomic lesions, increasing their susceptibility to DNA damage. These cancers are treatable with RPT absorbed doses in the range of 5–15 Gy (83).
Solid Tumors
Perhaps the most relevant tumor characteristic for RPT is the variable vascularity of, and absence of lymphatic drainage from, solid malignancies (84–86). The interstitial pressure associated with these characteristics impedes uniform penetration of systemically administered RPT. The reduced vasculature and reduced nutrient supply lead to hypoxia and induction of hypoxia-related signaling pathways. Cancer cells with elevated hypoxia-inducible factors are more aggressive, are less sensitive to therapy, and exhibit a greater propensity for metastatic dissemination. These factors give rise to highly nonuniform intratumoral dose distributions from most RPT agents. Tumor-volume–averaged absorbed dose estimates for response to different RPT agents range from 40 to 200 Gy. In addition to all the biologic variables, this large range in absorbed doses needed for a response may also reflect the impact of absorbed dose nonuniformities. Efforts to account for this possibility using the equivalent uniform dose (EUD) formalism have been developed; however, continued rigorous evaluation of its applicability is warranted (87–89).
Metastatically Disseminated Cancer Cells
Metastatically disseminated cancer cells are the cell population perhaps most relevant for RPT. Distant metastases to bone and other viscera typically occur via hematogenous spread. It is thought that RPT may be most effective for low-volume metastases. However, given the known radiosensitivity to leukocytes, the risk of marrow toxicity is real and warrants caution.
RPT TUMOR DOSE–RESPONSE EXPERIENCE
At the most basic level, response to RPT is impacted by 2 factors: the intrinsic radiation sensitivity of the tumor, and the absorbed dose to the tumor. Although not fully understood, the intrinsic radiosensitivity of a tumor cell is impacted primarily by doubling time and ability to address genomic lesions caused by ionizing radiation. The dose to the tumor is dependent on the target expression, the residence time of the RPT once it binds to the target, and the physical properties of the radiopharmaceutical (e.g., isotope half-life and emission characteristics).
Establishing the tumor-absorbed dose–versus–response relationship in RPT has yet to be prioritized. In addition to the scarcity of studies acquiring multiple-time-point imaging data for dosimetry, tumor dosimetry is associated with the added challenge of segmentation. Although fully automatic or semiautomatic tools based on thresholding, atlas libraries, and—more recently—machine learning are available for organ segmentation, accurate tumor segmentation typically requires a radiologist either to perform the task manually or to refine outlines from emission imaging thresholding or gradient-based tools. Furthermore, standardized tumor dosimetry can be more challenging than organ dosimetry because imaging-related factors such as PET and SPECT resolution, reconstruction parameters, and partial-volume correction methods have a substantially increased impact on objects with small volumes relative to the system resolution. The criteria and timing used for response assessment will impact the tumor-absorbed dose–versus–outcome relationships. Although morphologic response on CT or MRI using criteria such as RECIST has traditionally been used to assess tumor response in dose–response studies, use of metabolic response based on PET SUV or biochemical response (e.g., chromogranin A levels for NETs or prostate-specific antigen levels for prostate cancer) has also been reported. In some cases, implementation of proposed tumor-specific radiologic response criteria has been attempted, such as the European Association for the Study of the Liver criteria for hepatocellular carcinoma (90).
Most studies reporting a statistically significant association between absorbed dose and tumor response have been on 90Y microsphere radioembolic therapy of hepatic malignancies (Table 2). The most extensive of these evaluations has been performed by the group of Garin et al., using 99mTc-macroaggregated albumin SPECT/CT-based estimates as a surrogate for 90Y (91). In their initial studies, they demonstrated that the overall survival was significantly higher at 6 mo after treatment in patients who received a mean tumor-absorbed dose of at least 205 Gy than in those who received less than 205 Gy (18 mo vs. 9 mo; P = 0.032) (92)—a finding that was independently validated in a prospective study with 85 patients (91). Their findings were subsequently used to design the DOSISPHERE-01 trial, a prospective clinical trial to compare response and survival in patients receiving a personalized tumor dosimetry–guided treatment to deliver more than 205 Gy to the index lesion, compared with those receiving the standard treatment protocol for 90Y glass microspheres. Recently published results from this trial show that personalized dosimetry significantly improved the objective response rate (71% vs. 36%; P = 0.0074) and survival (median 27 mo vs. 11 mo; P = 0.0096) over radioembolization using a standard dosimetry approach (92). Literature reports on non–hepatocellular carcinoma intrahepatic radioembolization targets—colorectal metastases, NET metastases, cholangiocarcinoma, and metastatic melanoma—also demonstrate statistically significant dose–response relationships, but with differing response thresholds (22,93–100).
Studies Reporting on Tumor-Absorbed Dose vs. Response in Microsphere Radioembolization of Hepatic Malignancies
A recent study on 177Lu-PSMA radioligand therapy in low-volume hormone-sensitive metastatic prostate cancer patients reported a statistically significant correlation between absorbed dose to the index lesion and treatment response, defined as a prostate-specific antigen drop of more than 50% (101).
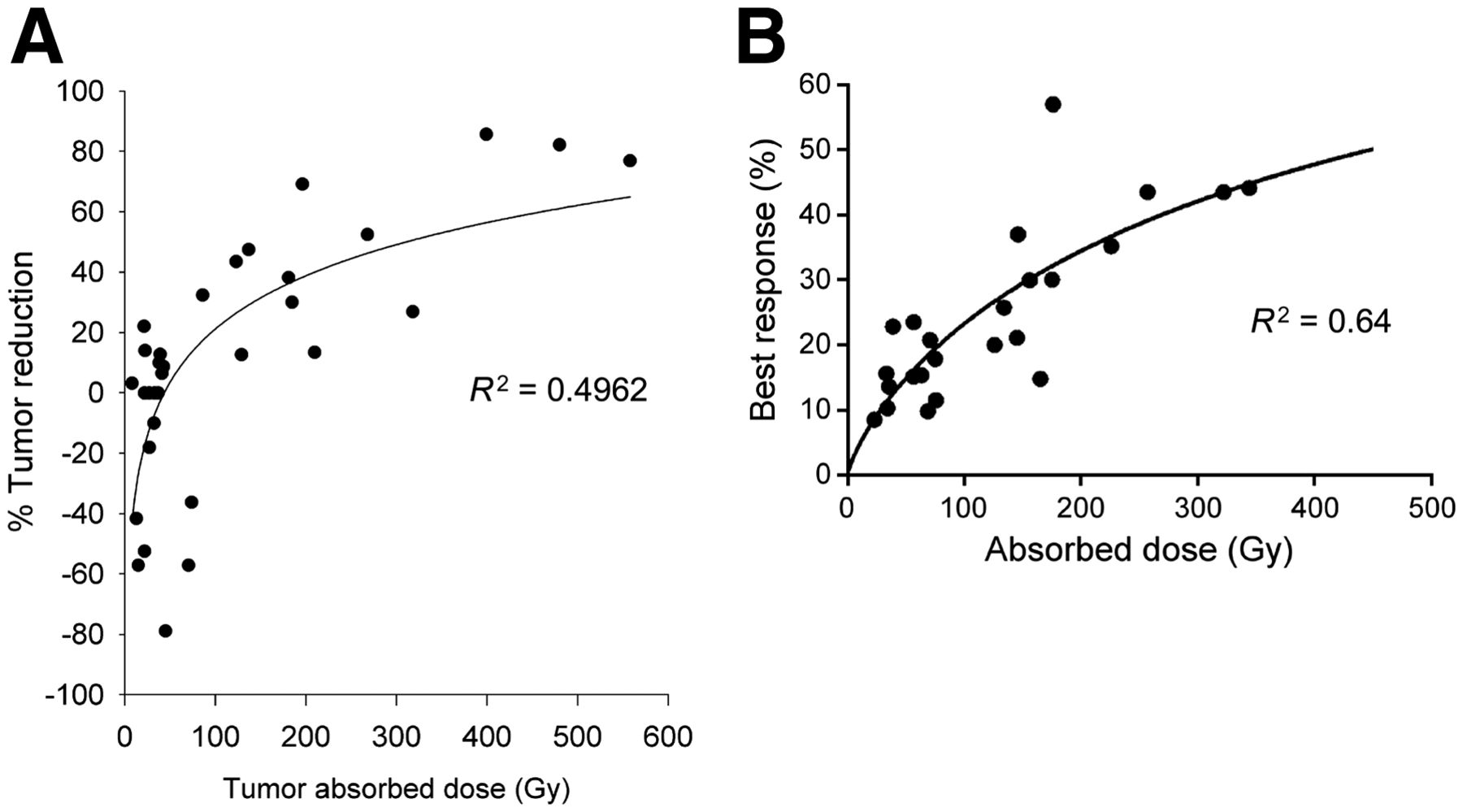
In radioiodine therapy, PRRT, and radioimmunotherapy, there have been a few studies investigating tumor dose–response relationships (Table 3). For PRRT, these data have been summarized in a recent review article (17). For NETs, the dose–response curve published in 2005 by Pauwels et al. (102) for 90Y-DOTATOC therapy is remarkably similar to the results published by Ilan et al. (103) a decade later for 177Lu-DOTATATE (Fig. 1). As the figure shows, in both cases, a 30% tumor shrinkage was achieved at approximately a 150-Gy mean absorbed dose to the tumor (over multiple cycles). Unlike the study by Ilan et al. for pancreatic NETs, a similar dose–response study on small intestinal NETS by the same group failed to demonstrate a statistically significant relationship (104). They reported mean tumor-absorbed doses of 51–487 Gy (median, 140 Gy) that showed no association with tumor reduction or biochemical response. Because of the very high radiosensitivity of lymphomas, reported absorbed doses to achieve a response in non-Hodgkin lymphoma treated with radioimmunotherapy have been about 100-fold lower than in NETS treated with PRRT. Tumor-absorbed doses reported by Sgouros et al. for a study of 131I-tositumomab RPT in non-Hodgkin lymphoma were in the range of 37–1,760 cGy (median, 300 cGy) (105). In a study of 39 patients (130 tumors) treated with 131I-tositumomab RPT, Dewaraja et al. reported longer progression-free survival in patients receiving mean tumor-absorbed doses greater than 200 cGy than in those receiving 200 cGy or less (median progression-free survival, 13.6 vs. 1.9 mo for the 2 dose groups; P < 0.0001) (16). The tumor-absorbed doses in this study ranged from 94 to 711 cGy (median, 275 cGy), with 62% of patients classified as responders and 46% as complete responders. In a study of 16 patients with non-Hodgkin lymphoma treated with 177Lu-lilotomab satetraxetan, the reported absorbed doses were of the same order of magnitude as reported in the studies by Dewaraja et al. and Sgouros et al. for 131I-tositumomab RPT, ranging from 35 to 859 cGy (median, 330 cGy) (106). Although most patients demonstrated a metabolic response on 18F-FDG PET, there was no overall correlation between tumor-absorbed dose and response assessed on the basis of either PET or CT measurements. This diversity of dose–response data may reflect the importance of standardizing dosimetry methods and performing rigorous trials that incorporate dosimetry to help evaluate variability in absorbed dose versus tumor response more definitively.
Studies Reporting Tumor Dose–Response Relationship in Other RPTs

The importance of radiobiologic dosimetry in accounting for the effects of dose-rate and spatial nonuniformity in absorbed dose is evident when comparing the threshold tumor-absorbed doses for achieving a response reported in clinical studies with resin microspheres versus glass microspheres (Table 2). In hepatocellular carcinoma, the reported mean tumor-absorbed dose thresholds for glass are generally in the range of 200–400 Gy, whereas for resin this value is in the range 100–150 Gy. This difference has been attributed to the differences in the uniformity of microsphere distribution on a microscopic scale—uniformity that varies with the number of injected particles per gigabecquerel (107). However, this difference is difficult to resolve with PET or SPECT imaging capabilities. The higher specific activity of glass than of resin microspheres leads to a less uniform dose deposition and, hence, a lower biologic effect per gray. d’Abadie et al. (108) have attempted to use the tumor EUD to reconcile the approximately 2-fold difference in efficacy per gray between resin and glass microspheres reported in clinical studies. For hepatocellular carcinoma treated with glass microspheres, Chiesa et al. reported that responding versus nonresponding lesions were well separated regardless of the dose metric used, but the equivalent uniform biologically effective dose gave significantly better separation than what was achieved with mean absorbed dose (AUC, 0.87 vs. 0.80) (109). Two other studies used logistical regression models for describing dose–response data for 90Y glass microspheres showed a strong association between dose metrics and the probability of response regardless of whether mean absorbed dose or radiobiologic dose metrics were used. Although the statistical models used in these studies have no radiobiologic basis, they use a variable function to approximate the sigmoidal response function potentially caused by tumor variations in radiosensitivity, clonogen number, experimental uncertainty, and other factors (110,111). In RPT, Roberson et al. expanded their tumor radiobiologic model for non-Hodgkin lymphoma to include the effect of the cold antibody (unlabeled tositumomab) that is coadministered with both the tracer and the therapy administration of 131l-labeled tositumomab (16,112). Facilitated by access to multiple-time-point SPECT/CT imaging, they demonstrated substantial lesion shrinkage during the 7 d of imaging after the tracer and therapy administration; this shrinkage was attributed to the therapeutic effect of the cold antibody and the high radiosensitivity of lymphomas. The use of EUD for dose–response correlations using early response as the outcome resulted in an improvement over the use of mean absorbed dose. However, regarding progression-free survival, both mean tumor-absorbed dose and EUD showed a similar statistically significant association (16). Image-derived EUDs are constrained by the resolution of the SPECT or PET system. Although image-derived EUD may be valuable for tumor regions that broadly exhibit variable uptake (e.g., necrotic zones), accounting for millimeter-scale patterns of retention that could drive some degree of differential radioresistance among patients is not possible unless supplemented with a priori knowledge of the expected distribution (e.g., as may be obtained from preclinical studies).
SUMMARY AND TABLE OF UNKNOWNS
The biologic characteristics of radiation have been extensively characterized, both in vitro and in vivo, and numerous factors are known to impact biologic response. These include total absorbed dose, dose rate, timing of sequential doses of radiation, spatial uniformity in the absorbed dose, tissue type, radiation type, and chemical factors such as tissue oxygen saturation. Dose and treatment fractionation in particular have been tools of radiation oncology to help increase the therapeutic ratio—that is, by increasing tumor control probability relative to normal-tissue complication probability. Despite the limitations associated with extrapolating from controlled experiments (e.g., clonogenic cell survival assays) to heterogeneous patient populations, mathematic models describing these relationships, such as the linear quadratic model, have been highly influential in radiation therapy practice patterns.
Conventional (∼2 Gy per fraction) EBRT practice has benefitted from landmark publications, including the Emami paper (113) and the QUANTEC (Quantitative Analysis of Normal Tissue Effects in the Clinic) papers (114,115). These publications—written on the basis of available data or, when data were lacking, expert opinion—have guided the field of radiation oncology toward standardization of how normal-tissue doses affect measurable adverse events, such as fibrosis or neuropathy. As the practice of radiation oncology has evolved since 2010, hypofractionation (in which high doses of radiation are delivered in fewer fractions) has become a routine part of clinical care. As such, additional guidelines regarding normal-tissue dose tolerances have been developed, such as the HyTEC (High Dose per Fraction, Hypofractionated Treatment Effects in the Clinic) project (116). No comprehensive or authoritative resource currently exists regarding tumor control probability as a function of EBRT dose and treatment schedule. Rather than deriving the ideal treatment schedule from fundamental radiobiologic models and preclinical studies, current treatment patterns are often a reflection of historic norms, through which safety and efficacy are supported by existing data. With the exception of palliative therapy and the small subset of cases in which local control is close to 100% at moderate dose levels, historic prescribing patterns reflect a dose level that typically does not exceed normal-tissue tolerances. The intent with this approach is to maximize the therapeutic ratio in a typical patient. Radiobiologic modeling via the concept of biologically effective dose and equivalent dose in 2 Gy per fraction is often used clinically for extrapolation from conventional fractionation to other treatment schedules that are isoeffective but have reduced toxicity, isotoxic but have increased efficacy, or some combination of the two. To the extent that it has been developed, the radiobiology of low-dose-rate brachytherapy may be more relevant to RPT tumor response for a given total tumor-absorbed dose. Incorporating novel approaches, such as Decipher or genomic-adjusted radiation dose, may improve classic models by incorporating genomic data from patients (82,117). Table 4 summarizes the list of unknowns.
List of Unknowns
CONCLUSION
Within the context of RPT, direct adoption of guidelines and tumor control probability models developed for the field of EBRT may be impractical; however, the history of external-beam dosimetry refinement and optimization of treatment plans may guide similar advances with RPT. At a given average tumor-absorbed dose, RPT may lead to very different biologic effects from those of EBRT because of a reduced dose rate, a much greater nonuniformity in the spatial absorbed dose distribution at the microscopic level, differing relative biological effectiveness (via α-emitting RPTs), or differences in the total treatment time. Increased DNA repair during low-dose-rate therapy, as well as repair and proliferation between treatments, is generally expected to increase organ dose tolerance and thresholds for tumor control. As with conventional radiation therapy, though, it is critical that we combine expert opinion with clinical experience whereby the absorbed dose to tumors and healthy structures is well estimated within conventional treatment paradigms, and radiobiologic models are subsequently used to refine treatment practice. Such efforts can help standardize the treatment of patients with RPT and improve the therapeutic index on a patient-specific basis. Importantly, we need well-designed prospective clinical trials to validate the hypothesis that, like external radiotherapy, absorbed doses to tumors and organs relate to tumor control and toxicity, respectively. Admittedly, arriving at a standardized model to test and implement is challenging, but the potential benefit is well worth the effort.
DISCLOSURE
George Sgouros is a founder of, and holds equity in, Rapid. He serves as a member of Rapid’s Board of Directors. This arrangement has been reviewed and approved by the Johns Hopkins University in accordance with its conflict-of-interest policies. Yuni Dewaraja is a consultant for MIM Software and has a grant from Varian. Thomas Hope is a consultant for Curium and Rayze Bio, has a grant from Clovis Oncology, and is on the advisory board of Blue Earth Diagnostics and Ipsen. He is also a participant on a AAA/Novartis clinical trial. The opinions expressed in this publication are the author(s)’ own and do not reflect the view of the National Institutes of Health, the Department of Health and Human Services, or the United States government. No other potential conflict of interest relevant to this article was reported.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.
- 11.
- 12.
- 13.
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.
- 19.
- 20.
- 21.
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.
- 27.
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.
- 53.
- 54.
- 55.
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.
- 86.↵
- 87.↵
- 88.
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.
- 128.
- 129.
- 130.
- 131.
- 132.
- 133.
- 134.
- 135.
- 136.
- 137.
- 138.
- 139.
- 140.
- 141.
- Received for publication July 26, 2021.
- Revision received October 18, 2021.
In this issue





{kind=link}
Jump to section
- Article
- Abstract
- TECHNICAL FACTORS IMPACTING TUMOR-ABSORBED DOSE VERSUS RESPONSE IN RPT
- BASIC BIOLOGY FACTORS IMPACTING TUMOR-ABSORBED DOSE VERSUS RESPONSE IN RPT
- ABSORBED DOSE VERSUS TUMOR RESPONSE IN EBRT
- CANCER CELL RESPONSE BY CATEGORY
- RPT TUMOR DOSE–RESPONSE EXPERIENCE
- SUMMARY AND TABLE OF UNKNOWNS
- CONCLUSION
- DISCLOSURE
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Theranostic GPA33-Pretargeted Radioimmunotherapy of Human Colorectal Carcinoma with a Bivalent 177Lu-Labeled Radiohapten
- Assessing Response to PSMA Radiopharmaceutical Therapies with Single SPECT Imaging at 24 Hours After Injection
- Quality Assurance Considerations in Radiopharmaceutical Therapy Dosimetry Using PLANETDose: An International Atomic Energy Agency Study
- Lesion Dosimetry for [177Lu]Lu-PSMA-617 Radiopharmaceutical Therapy Combined with Stereotactic Body Radiotherapy in Patients with Oligometastatic Castration-Sensitive Prostate Cancer
- Tumor Control Probability and Small-Scale Monte Carlo Dosimetry: Effects of Heterogenous Intratumoral Activity Distribution in Radiopharmaceutical Therapy
- Dosimetry in Radiopharmaceutical Therapy
- Reply: Single-Time-Point Tumor Dosimetry Assuming Normal Distribution of Tumor Kinetics
- Single-Time-Point Tumor Dosimetry Assuming Normal Distribution of Tumor Kinetics
- Normal-Tissue Tolerance to Radiopharmaceutical Therapies, the Knowns and the Unknowns
- Radiopharmaceutical Dosimetry for Cancer Therapy: From Theory to Practice