


Abstract
The expression of prostate-specific membrane antigen (PSMA) is increased in prostate cancer. Recently, 68Ga-PSMA (Glu-NH-CO-NH-Lys-(Ahx)-[68Ga(HBED-CC)]) was developed as a PSMA ligand. The aim of this study was to investigate the detection rate of 68Ga-PSMA PET/CT in patients with biochemical recurrence after radical prostatectomy. Methods: Two hundred forty-eight of 393 patients were evaluable for a retrospective analysis. Median prostate-specific antigen (PSA) level was 1.99 ng/mL (range, 0.2–59.4 ng/mL). All patients underwent contrast-enhanced PET/CT after injection of 155 ± 27 MBq of 68Ga-PSMA ligand. The detection rates were correlated with PSA level and PSA kinetics. The influence of antihormonal treatment, primary Gleason score, and contribution of PET and morphologic imaging to the final diagnosis were assessed. Results: Two hundred twenty-two (89.5%) patients showed pathologic findings in 68Ga-PSMA ligand PET/CT. The detection rates were 96.8%, 93.0%, 72.7%, and 57.9% for PSA levels of ≥2, 1 to <2, 0.5 to <1, and 0.2 to <0.5 ng/mL, respectively. Whereas detection rates increased with a higher PSA velocity (81.8%, 82.4%, 92.1%, and 100% in <1, 1 to <2, 2 to <5, and ≥5 ng/mL/y, respectively), no significant association could be found for PSA doubling time (82.7%, 96.2%, and 90.7% in >6, 4–6, and <4 mo, respectively). 68Ga-PSMA ligand PET (as compared with CT) exclusively provided pathologic findings in 81 (32.7%) patients. In 61 (24.6%) patients, it exclusively identified additional involved regions. In higher Gleason score (≤7 vs. ≥8), detection efficacy was significantly increased (P = 0.0190). No significant difference in detection efficacy was present regarding antiandrogen therapy (P = 0.0783). Conclusion: Hybrid 68Ga-PSMA ligand PET/CT shows substantially higher detection rates than reported for other imaging modalities. Most importantly, it reveals a high number of positive findings in the clinically important range of low PSA values (<0.5 ng/mL), which in many cases can substantially influence the further clinical management.
In biochemical recurrence after radical prostatectomy (RP), an increase of the prostate-specific antigen (PSA) level precedes a clinically detectable recurrence by months to years (1). However, it cannot differentiate between local, regional, or systemic disease with the necessary precision that is essential for further disease management (2). Furthermore, PSA kinetics such as PSA velocity (PSAvel) and PSA doubling time (PSAdt) play an important role, with high PSA kinetics facilitating disease detection (3).
Morphologic imaging methods exhibit considerable limitations: sensitivity ranges between 25% and 54% for the detection of local recurrence by transrectal ultrasound or CT and is moderately improved using functional MR imaging techniques (2,4). The sensitivity for detection of lymph node metastases of CT or MR imaging is reported to be 30%–80% (5). Ultra-small particles of iron oxides proved to be effective; however, they have not been approved by regulatory authorities so far (6).
Various targets have been addressed by molecular imaging to improve the detection of recurrent prostate cancer (PC). For PET imaging, mainly 11C- and 11F-labeled choline derivates have been used in the past (7–9). However, especially in patients with PSA values below 3 ng/mL, the detection rate is only 40%–60% (3,4,7). Recently, a new molecular probe targeting, for example, the gastrin-releasing peptide receptor or the prostate-specific membrane antigen (PSMA), has been developed (10–12). PSMA is a membrane-bound enzyme with significantly elevated expression in PC cells in comparison to benign prostatic tissue (13). The localization of the catalytic site of PSMA in the extracellular domain allows the development of small specific inhibitors that are internalized after ligand binding (14). Older agents targeting the intracellular domain of PSMA showed disappointing results due to low image contrast, low sensitivity, or high background signal (15). The recent development of 68Ga-PSMA (Glu-NH-CO-NH-Lys-(Ahx)-[68Ga(HBED-CC)]) as an extracellular PSMA inhibitor for PET imaging demonstrated a high specificity for PSMA tumor–expressing cells as well a high and specific uptake in a mouse model (16). A first preliminary study in PC patients revealed a higher image contrast and detection rate for 68Ga-PSMA than 18F-choline (17). In addition, further preliminary data in primary PC back the high specificity of 68Ga-PSMA ligand PET imaging, ranging more than 95% at both patient- and field-based analysis for lymph node staging validated by extended pelvic lymph node dissection (18). Most recently, a large study including patients with different primary treatment was published encompassing patients with recurrent PC, supporting high detection rates (19). Consequently, PSMA targeting holds promise in being a superb biomarker for the early detection of recurrent disease allowing adequate stratification of patients for optimal treatment planning.
Thus, the purpose of our study was to assess the value of 68Ga-PSMA ligand PET/CT for the detection and localization of recurrent disease in a large homogeneous series of patients after RP. Specifically, we aimed to describe the detection rate as a function of the absolute PSA level and PSA kinetics and the evaluation of the diagnostic performance, compared with primary histologic differentiation and antihormonal treatment.
MATERIALS AND METHODS
Patients
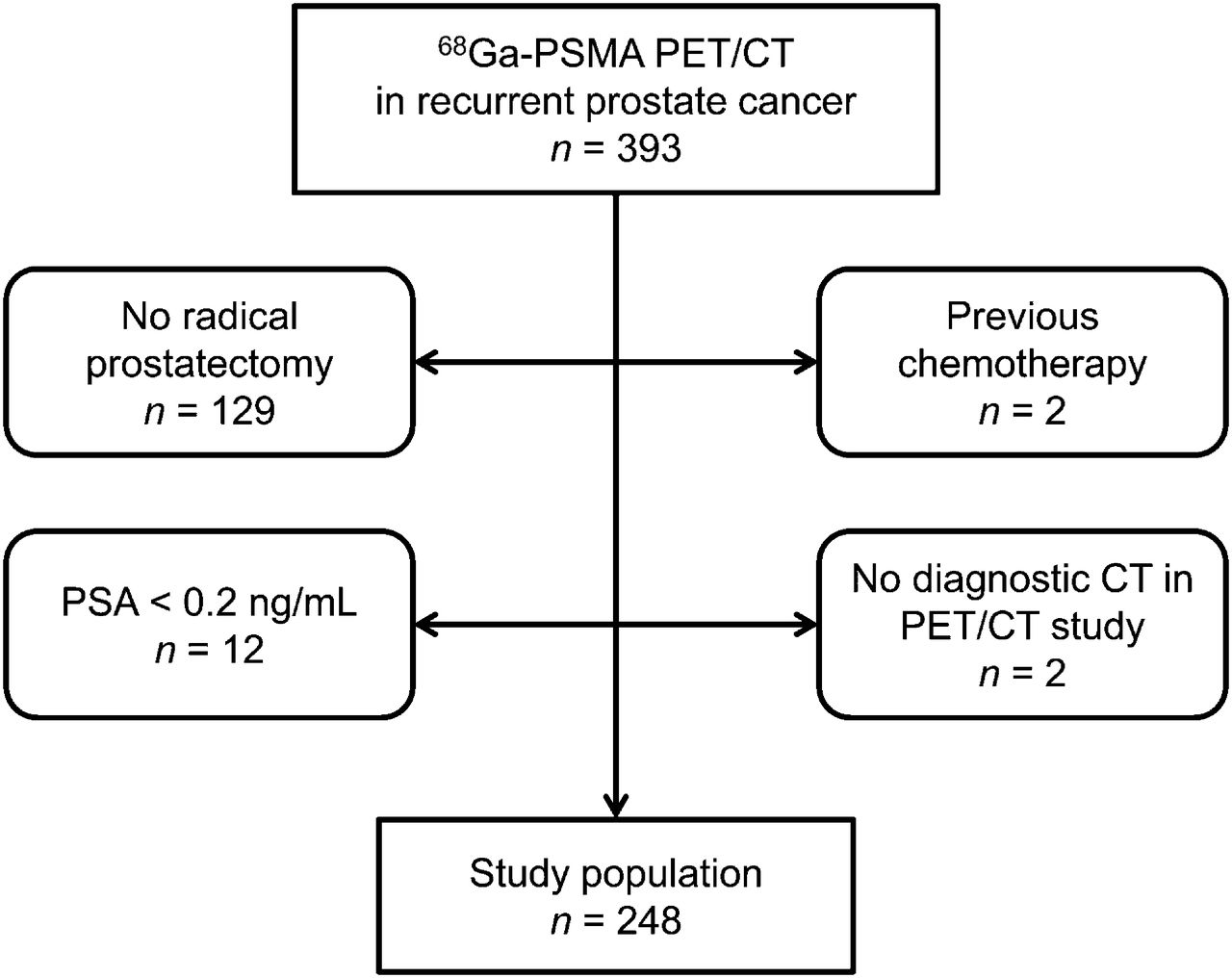
Three hundred ninety-three consecutive patients who underwent 68Ga-PSMA ligand PET/CT imaging for recurrent PC were extracted from the institutions’ database (November 2012 to April 2014). Only patients who had undergone RP, whose PSA level was ≥0.2 ng/mL and had not received chemotherapy, were included (Fig. 1). In total, 248 patients were included in this retrospective study. Patient characteristics are summarized in Table 1. Seventy patients had received androgen-deprivation therapy within the last 6 mo before the examination.
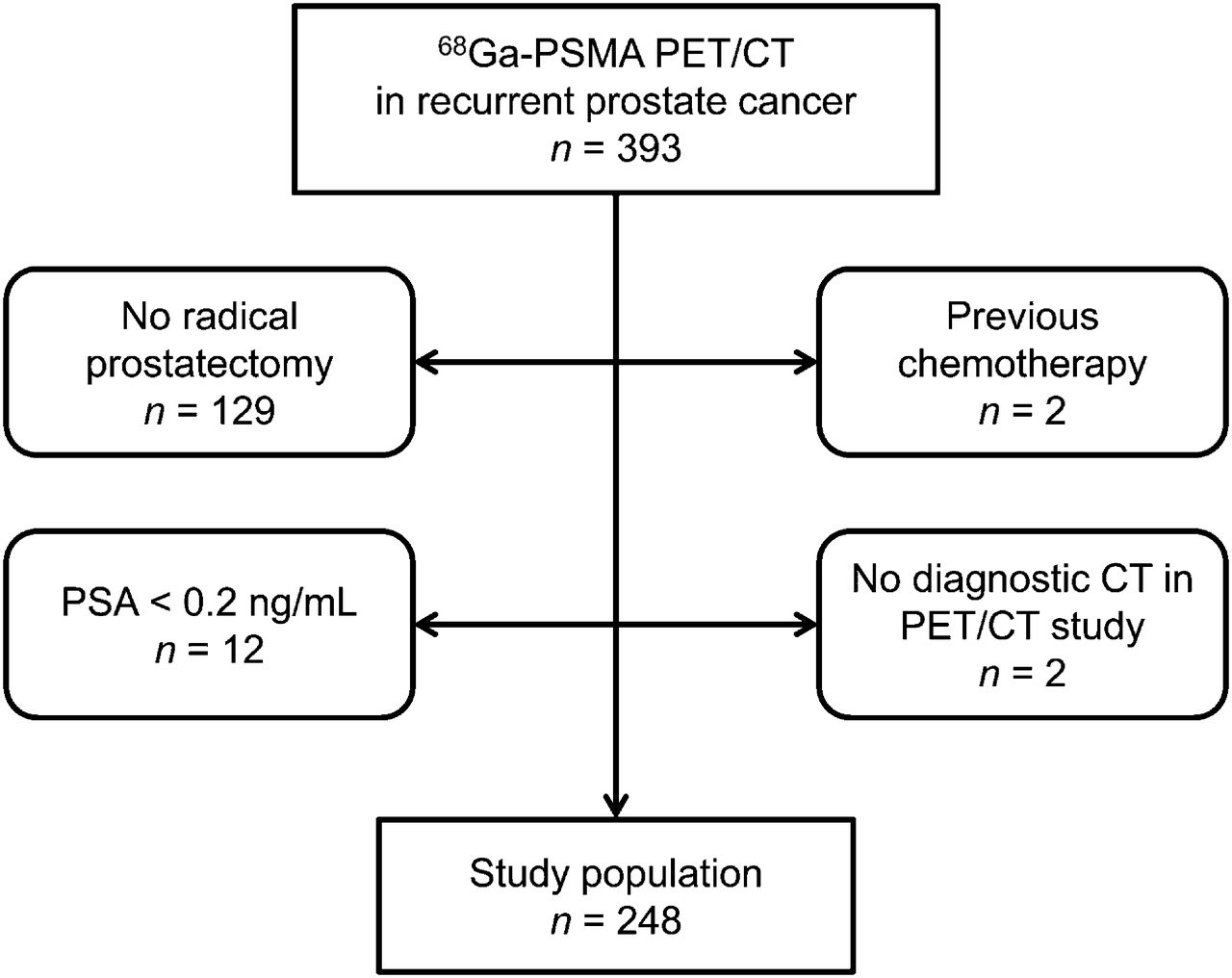
Flow chart of patient selection.
Patient Characteristics
All patients gave written informed consent for the purpose of anonymized evaluation and publication of their data. All reported investigations were conducted in accordance with the Helsinki Declaration and with national regulations. The study was approved by the Ethics Committee of the Technical University Munich (permit 5665/13).
The serum PSA level at the time of the PET/CT scan was available in all patients. In addition, in 144 patients PSA kinetics (PSAvel and PSAdt) were calculated as described previously (20). Only patients who were able to provide at least 2 PSA measurements after PSA progression (i.e., at least 3 PSA values) and in whom therapy had not been changed within the last 6 mo before imaging were included in this subgroup analysis.
Synthesis and Application of 68Ga-PSMA Ligand
Images were obtained with the 68Ga-labeled HBED-CC (16) that was synthesized as described previously (21). The ligand was labeled with 68Ga3+ (half-life, 67.6 min) from a 68Ge/68Ga radionuclide generator (iThemba Labs) by means of a fully automated module (Scintomics) and good manufacturing practice–grade disposable cassettes and reagent kit (ABX) (16,22). The final product was dissolved in isotonic phosphate-buffered saline with subsequent sterile filtration.
The 68Ga-PSMA ligand complex solution was applied to patients via an intravenous bolus (mean ± SD, 155.5 ± 27.4 MBq; range, 88–240 MBq). Variation of injected radiotracer activity was caused by the short half-life of 68Ga and variable elution efficiencies obtained during the lifetime of the 68Ge/68Ga radionuclide generator.
Imaging Protocol
PET acquisition was started at a mean time of 54.2 ± 7.1 min after tracer injection (range, 41–74 min). All patients underwent 68Ga-PSMA ligand PET/CT on a Biograph mCT scanner (Siemens Medical Solutions). First, a diagnostic CT scan was obtained in the portal venous phase 80 s after intravenous injection of contrast agent (Imeron 300), followed by the PET scan. All patients received diluted oral contrast (300 mg of Telebrix) and a rectal filling with a negative contrast agent (100–150 mL). All PET scans were acquired in 3-dimensional mode with an acquisition time of 3–4 min per bed position. Emission data were corrected for randoms, dead time, scatter, and attenuation and were reconstructed iteratively by an ordered-subsets expectation maximization algorithm (4 iterations, 8 subsets) followed by a postreconstruction smoothing gaussian filter (5 mm in full width at one-half maximum).
Image Analysis
All images were interpreted by 1 board-certified nuclear medicine physician and 1 board-certified radiologist. Primarily, 68Ga-PSMA ligand PET images and CT images were interpreted separately followed by a final consensus interpretation. All lesions suggestive for recurrent PC were noted and grouped into local recurrence, lymph node metastases (discrimination into pelvic, retroperitoneal, and supradiaphragmatic location), bone metastases, and other metastases (e.g., lung, liver).
To demonstrate the individual contribution of PET and CT for the final diagnosis, for every lesion the contribution of both PET and CT for defining malignancy was noted. In PET, any focal uptake of 68Ga-PSMA ligand higher than the surrounding background and not associated with physiologic uptake was considered suggestive for malignancy. For CT, for example, any pelvic/retroperitoneal lymph node station containing lymph nodes measuring at least 8 mm or any distinct sclerotic lesion not being associated with degenerative changes were judged as positive (4).
Statistical Analysis
The detection rate (number of patients with at least 1 positive finding) was plotted against the absolute PSA value and PSA kinetics. Two-sample t tests to evaluate differences between single groups (Gleason score, antihormonal treatment) and Mann–Whitney U tests to evaluate differences concerning PSA values between groups with and without pathologic uptakes were used. All tests were performed 2-sided, and a level of significance of α = 5% was used. Statistical analyses were conducted with software (MedCalc, version 13.2.0, 2014; MedCalc).
RESULTS
Detection Efficacy
PSA Level
Of the 248 patients, 222 (89.5%) showed 1 or more localized areas suggestive for recurrent PC. The detection efficacy of 68Ga-PSMA ligand PET/CT was 96.8% (120/124) for a PSA value of ≥2 ng/mL, 93.0% (67/72) for a PSA value of 1 to <2 ng/mL, 72.7% (24/33) for a PSA value of 0.5 to <1 ng/mL, and 57.9% (11/19) for a PSA value of 0.2 to <0.5 ng/mL (Fig. 2A). The different regions involved by recurrent disease are listed in Table 2. Mean PSA was significantly lower in patients with negative 68Ga-PSMA ligand PET/CT results than in patients with positive results (P = 0.0080; Table 3).

Detection rate of 68Ga-PSMA ligand PET/CT in relation PSA level (A), PSAvel (B), and PSAdt (C).
Different Regions Involved by Recurrent PC in 68Ga-PSMA Ligand PET/CT
PSA Level and PSA Kinetics in Patients with Positive and Negative Findings in 68Ga-PSMA Ligand PET/CT
PSA Kinetics
PSAvel ranged from 0.1 to 42.5 ng/mL per year. The detection rates of 68Ga-PSMA ligand PET/CT were 81.8% (54/66), 82.4% (14/17), 92.1% (35/38), and 100% (23/23) in patients with PSAvel values of, respectively, <1 ng/mL/y, 1–2 ng/mL/y, 2–5 ng/mL/y, and >5 ng/mL/y (Fig. 2B). Despite a strong tendency to a higher PSAvel in patients with positive 68Ga-PSMA ligand PET/CT results than in those with negative results, no statistical significance was reached (P = 0.0532; Table 3).
PSAdt values ranged between 0.37 and 158 mo. The detection rates of 68Ga-PSMA ligand PET/CT were 82.7% (62/75), 96.2% (25/26), and 90.7% (39/43) in patients with PSAdt values of >6 mo, 4–6 mo, and ≤4 mo, respectively (Fig. 1C). Mean PSAdt was not significantly different in patients with 68Ga-PSMA ligand PET/CT negative findings, compared with positive patients (P = 0.2971; Table 3).
Contribution of PET and Morphologic Imaging for Lesion Detection
The number and percentage of patients in whom PET and CT were concordantly detecting lesions or in whom PET or CT exclusively defined recurrent disease or showed additional involved regions (outside of primarily detected regions) are given in Figure 3. Notably, whereas 68Ga-PSMA ligand PET (as compared with CT) exclusively provided relevant diagnostic information in 81 (32.7%) patients, CT (as compared with PET) was only able to exclusively provide the diagnostic information in 3 (1.2%) of the cases. Moreover, in 61 (24.6%) patients PET was able to identify additional involved regions, compared with 17 (6.9%) patients in whom CT showed additional regions (Table 4). In most of the cases in which PET provided additional information, lymph node metastases, local recurrence, or bone metastases could not be identified by CT (representative examples are given in Figs. 4 and 5 and Supplemental Fig. 1 [supplemental materials are available at http://jnm.snmjournals.org]). Most of the lesions in which CT provided exclusive information were (sclerotic) bone or lung metastases.
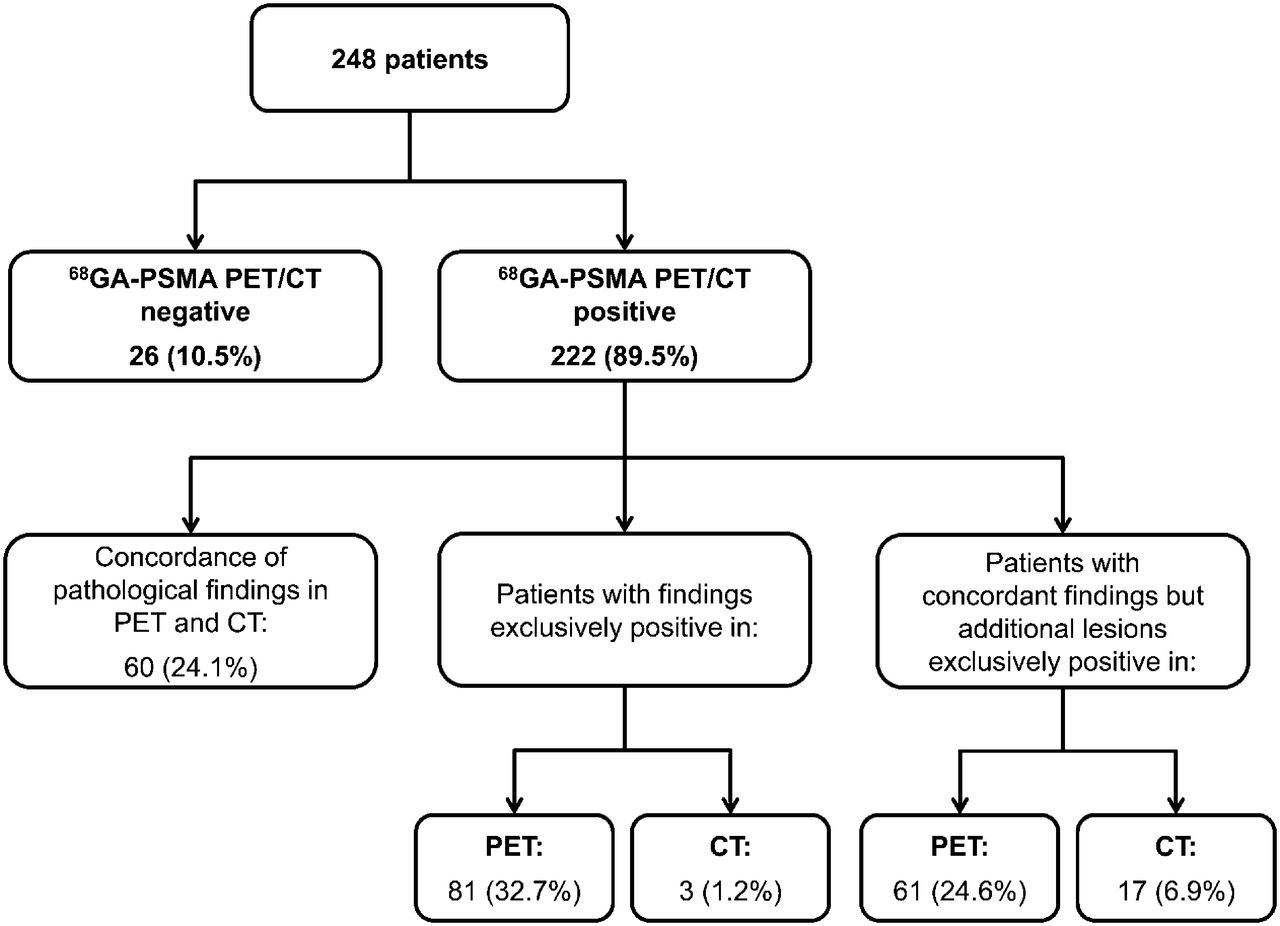
Contribution of PET and morphologic imaging for lesion detection.
Malignant Lesions Exclusively Identified in 68Ga-PSMA PET or CT
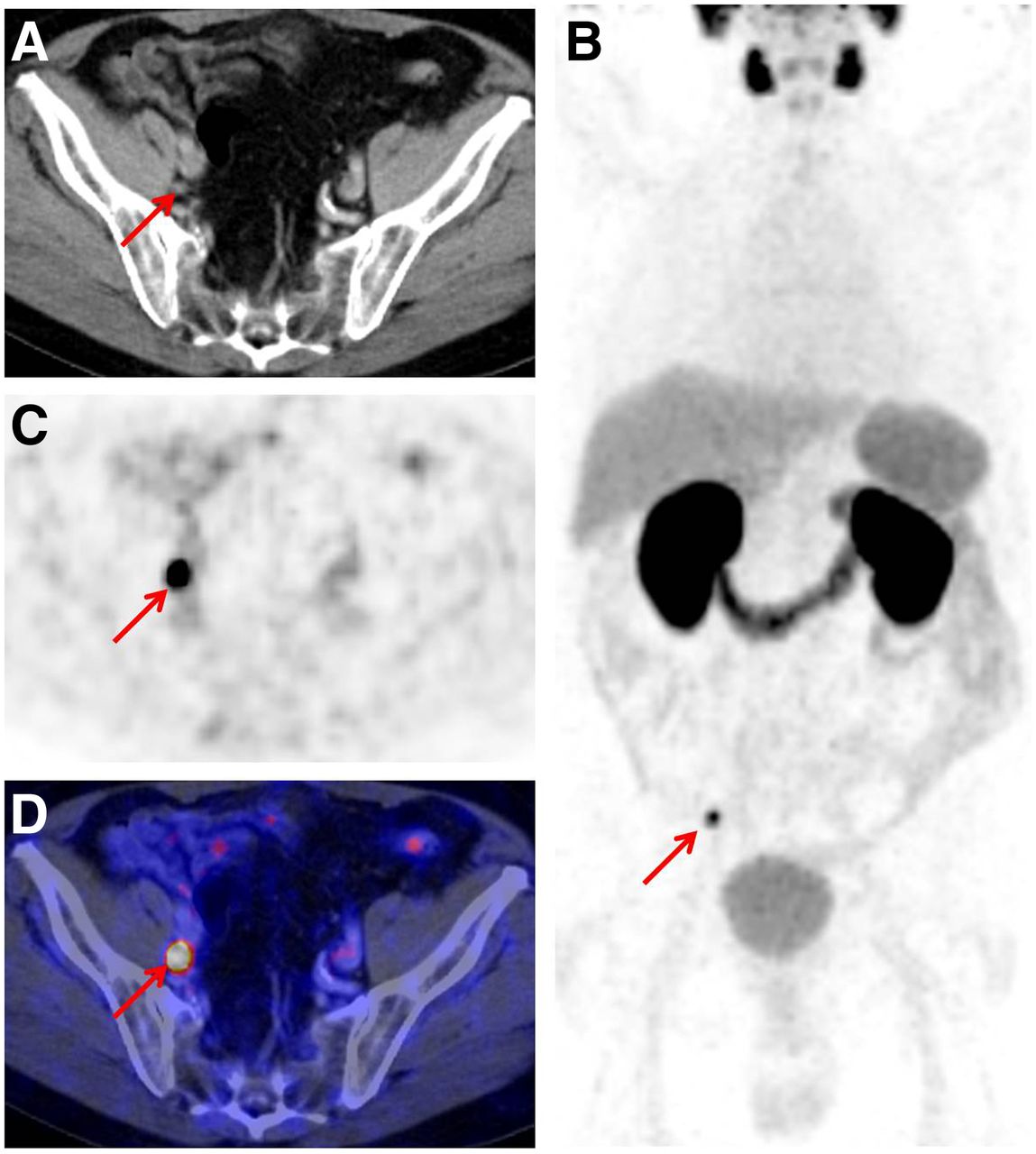
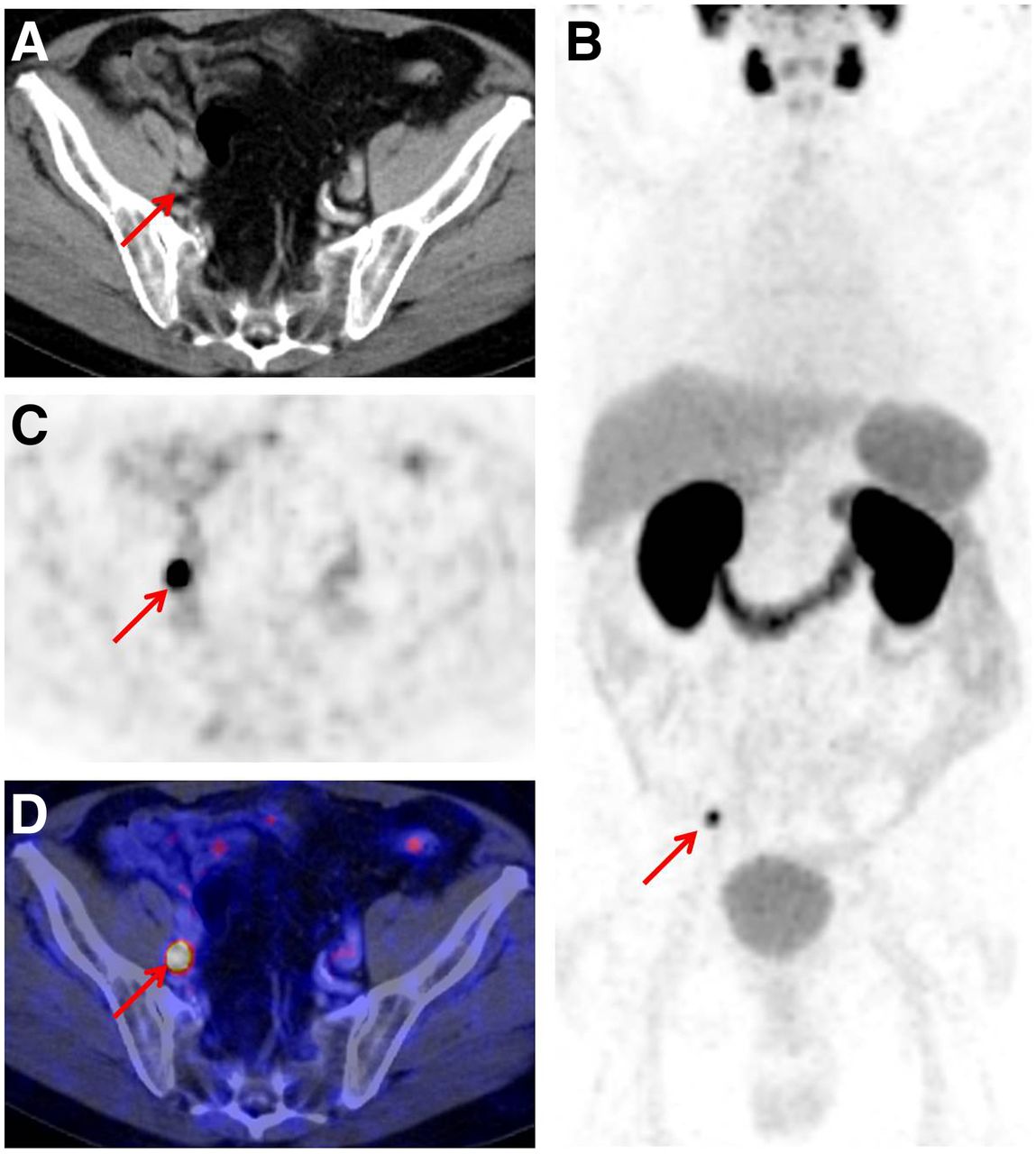
Set of images of a 75-y-old patient with status after RP (2000; Gleason score, 5; pT3b, pN1), radiation therapy (September 2011), and rising PSA value of 1.09 ng/mL (October 2013). CT images (A) reveal no suggestive finding, with 5-mm lymph node behind right external iliac vein. Corresponding PET (C) and fused PET/CT images (D) show intense uptake, with high lesion-to-background ratio in this small lymph node indicating lymph node metastasis. Whole-body maximum-intensity projection (B) displays this lymph node and demonstrates no other suggestive lesion. Selective lymph node picking was performed in December 2013, confirming single lymph node metastasis. Subsequently, PSA value dropped below detection limit (<0.07 ng/mL) without antihormonal treatment (last measurement April 2014).

Set of images of a 73-y-old patient with status after RP (September 2013; Gleason score, 9; pT3b, pN0, PSA nadir below detection limit). Increase of PSA value to 2.0 ng/mL (December 2013) and start of antihormonal treatment. Fused PET/CT image (A) demonstrates high intense uptake in lumbar spine, with no suggestive osteoblastic lesion in corresponding CT image (B). Four months after radiation diffuse sclerosis can be found in CT image (C), indicating posttherapeutic changes/progression.
Influence of Anti–Androgen Therapy and Primary Histologic Differentiation
In our patient collective, no significant difference in detection efficacy could be observed with regard to antiandrogen therapy (P = 0.0783). Lesions were detected in 95.7% (67/70) of patients with antiandrogen therapy and 87.1% (155/178) of patients without antiandrogen therapy. Notably, PSA values were significantly higher in patients with than without antihormonal treatment (8.11 ± 10.83 vs. 2.93 ± 3.11 ng/mL).
With respect to histologic differentiation of the primary PC, 68Ga-PSMA ligand PET/CT was positive in 86.7% (111/128) of patients with a Gleason score ≤ 7 and in 96.8% (90/93) of patients with a Gleason score ≥ 8 (P = 0.0190). No difference in PSA values was present between these 2 groups (PSA mean and median, 4.23 and 1.90 vs. 4.89 and 2.2 ng/mL, respectively).
DISCUSSION
PSA relapse after RP is a common clinical scenario. In this context, biochemical failure defined by a confirmed PSA value of >0.2 ng/mL after RP occurs long before recurrent disease can be localized clinically or by imaging. The goal in these patients is to distinguish whether disease relapse is localized to the prostate bed or whether metastatic disease is present because this affects further treatment. To date, the detection of lesions in biochemical recurrence (especially at PSA values < 1 ng/mL) of PC is a major challenge for all imaging modalities including PET with a variety of tracers (4,5,9).
In this study, we describe the detection rate of hybrid PET/CT imaging using a novel 68Ga-PSMA ligand as a PET tracer in a large number of patients with biochemical recurrence after RP. Despite being retrospective in nature, the strength of our study consists in a homogeneous patient selection. Our results show a considerably higher detection of hybrid PET/CT imaging using the 68Ga-PSMA ligand than reported for other PET tracers. Even in 67% of the patients with PSA levels < 1.0 ng/mL, the potential site of recurrence has been detected. Our data are in line with data by Afshar-Oromieh et al. published online only most recently (19). However, in our study only patients with biochemical recurrence after RP were included, creating the homogeneous patient collective in our study. In addition to the previously mentioned most recent work, we could show that compared with morphologic imaging the information provided by 68Ga-PSMA ligand PET was essential in 58% of the patients: in 33% the site of recurrence could only be detected by PET whereas in an additional 25% of the patients PET showed additional lesions not detectable by CT imaging.
Our results suggest that 68Ga-PSMA ligand PET/CT is highly effective in PC restaging because in our study 89.5% of patients showed at least 1 lesion regarded as characteristic for PC. Our data, based on a large and highly selected patient cohort, are in line with preliminary reports by Afshar-Oromieh (17,23). Compared with reports in the literature stating detection rates between 34% and 88% for 11C-choline, 43%–79% for 18F-choline, and 59%–80% for 11C-acetate (7,24–31), 68Ga-PSMA ligand PET/CT offers a substantially higher detection efficacy. As known from other PET tracers, the detection rate of 68Ga-PSMA ligand PET/CT also increases in parallel with rising PSA value (4). As an important finding, our study shows positive 68Ga-PSMA ligand PET/CT findings for PSA values < 1 ng/mL in 67% of the patients, which is substantially higher than reported for choline-based PET tracers showing detection rates between 19% and 36% at PSA levels below 1–1.5 ng/mL (3,7,32,33). Thus, 68Ga-PSMA ligand PET/CT improves lesion detectability in the group of patients at an early state, potentially allowing more tailored salvage therapies. The detection rate of 58% in patients with a PSA level < 0.5 ng/mL has, in particular, a clinical impact because urological guidelines (e.g., European Association of Urology (34)) define a PSA value of 0.5 ng/mL as the upper limit for salvage radiation therapy. However, it has to be admitted that the overall detection rate of 89.5% implies a false-negative rate of 10.5% for 68Ga-PSMA ligand PET/CT imaging because in the case of biochemical recurrence, by definition a viable recurring tumor must be present. In addition, it has to be mentioned that in this study the use of 68Ga-PSMA ligand PET/CT was not limited to patients with prior negative conventional scans (e.g., bone scanning, CT, MR imaging). Thus, if 68Ga-PSMA ligand PET/CT were used in that preselected setting, the detection rate would potentially be different.
Similarly to choline derivates, our results state a higher detection rate in patients with a higher PSAvel, albeit the P value of 0.0532 could be designed as borderline from a purist statistical point of view (3,32,35). Nevertheless, 68Ga-PSMA ligand PET/CT offers a high rate of positive findings also in patients with low changes in PSA kinetics, with a detection rate of 81.8% compared with 12% for 11C-choline at a PSAvel of 1 ng/mL/Y (35). Notably, our data show no clear trend toward higher detection rates with a decreasing PSAdt, compared with reports for 11C- and 18F-choline (32,35). However, especially at a low PSA value PSAdt is more susceptible to slight changes and thus not optimally suited in this patient collective. In addition, it has to be considered that data for PSAvel and PSAdt were only present in about 60% of the patients (as stated in the “Patients” section). Consequently, our data indicate that for 68Ga-PSMA ligand PET/CT PSA kinetics are not as crucial as for choline derviates because the detection rate is more than 75%, which is also true for patients with a low PSAvel or high PSAdt.
The substantial contribution of 68Ga-PSMA ligand PET in the setting of hybrid PET/CT is reflected by the fact that in 33% of cases the sites of recurrent disease were identified only by PET (Fig. 3; Table 4). In an additional 25% of cases, PET was able to identify further clinically relevant lesions that were not detected by CT. However, the high number of patients in whom the diagnosis of recurrent disease was solely based on PET is not surprising because the limited role of CT imaging, especially for local recurrence and lymph node metastases, is well documented (2,36). Besides the potential results derived from a bone scan in this patient cohort, which with respect to the PSA value would be low, the finding of additional clinically relevant lesions documents the high value of 68Ga-PSMA ligand PET in a setting in which prior conventional imaging would have been negative. Indeed, in our patient collective negative prior conventional imaging was not an inclusion criterion; however, this comparison indicates the potential high number of findings in a negatively preselected group.
Our data show a statistically significant higher detection rate in patients with a Gleason score ≥ 8 versus ≤ 7, which could be potentially attributed to the fact that immunohistochemically PSMA expression is usually higher in lesions with a higher Gleason score than in lesions with a lower Gleason score (37). Our data show a trend toward a higher detection rate in patients with antiandrogen therapy within 6 mo before 68Ga-PSMA ligand PET/CT imaging. However, these data do not reach statistical significance, and it has to be noted that mean PSA values were significantly higher in patients with antihormonal treatment, which could constitute a confounding factor. Nevertheless, there are reports stating a higher PSMA expression of PC tumor cells in the setting of antihormonal treatment (38,39), which could potentially be reflected in higher detection rates. This hypothesis has to be proven in further studies.
A major limitation of our study is the fact that histopathology as a gold standard was only available in a few cases. In 12 patients, 68Ga-PSMA ligand PET/CT–positive lymph node metastases were histologically confirmed. However, a histopathologic confirmation in all patients is not feasible because practical and ethical issues in the setting of recurrent PC. Nevertheless, in 35 patients 68Ga-PSMA ligand PET/CT–guided selective radiation therapy followed by a substantial decrease of PSA proved the nature of PSMA-positive lesions. In another 45 patients, follow-up/other imaging modalities unanimously proved that the positive lesions were metastases of PC. So in total, in 37.1% (92/248) of patients a comprehensive standard of reference (histopathology, decrease of PSA level after targeted radiation therapy, or undisputable follow-up/other imaging methods) was available. In all of these cases, concordant results in correlation with the findings derived from 68Ga-PSMA ligand PET/CT were present.
CONCLUSION
In this study, 68Ga-PSMA ligand PET/CT proved in a large number of patients with biochemical recurrence after RP a substantially higher detection efficacy than reported for other tracers. With a detection rate of >90% at PSA levels more than 1 ng/mL, this method currently surpasses all other imaging modalities for the restaging of PC. In patients in whom salvage therapy decisions are pending, 68Ga-PSMA ligand PET/CT imaging can also be performed at a lower PSA level, with the expectation of a detection rate of approximately 50% and offering the potential of guiding those treatments. In more than 50% of the cases, the information yielded by 68Ga-PSMA PET was crucial for the final diagnosis showing findings that have not been visualized by CT. In addition, the high tumor uptake of PSMA inhibitors makes these compounds in a subset of metastasized patients particularly attractive for endoradiotherapy. Hereby, imaging and therapeutic small-molecule inhibitors of PSMA could potentially be used as a theranostic strategy for patients with metastasized PC.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study received funding from the European Union Seventh Framework Program (FP7) under grant agreement no. 294582 ERC grant MUMI. The development of 68Ga-PSMA synthesis was supported by SFB 824 (DFG Sonderforschungsbereich 824, Project Z1) from the Deutsche Forschungsgemeinschaft, Bonn, Germany. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the whole team from radiochemistry (e.g., Jens Bertram, Petra Watzlowik, Fabian Kügler) for reliable tracer supply and Brigitte Dzewas, Coletta Kruschke, and Sylvia Schachoff as well as Anna Winter for their excellent technical assistance. We also thank Veronika Beck and Lisa Pähr for excellent data management.
Footnotes
↵* Contributed equally to this work.
Published online Mar. 19, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 9, 2015.
- Accepted for publication March 5, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preclinical Evaluation of Gastrin-Releasing Peptide Receptor Antagonists Labeled with 161Tb and 177Lu: A Comparative Study
- Preclinical Comparison of the 64Cu- and 68Ga-Labeled GRPR-Targeted Compounds RM2 and AMTG, as Well as First-in-Humans [68Ga]Ga-AMTG PET/CT
- Validation of 18F-rhPSMA-7 and 18F-rhPSMA-7.3 PET Imaging Results with Histopathology from Salvage Surgery in Patients with Biochemical Recurrence of Prostate Cancer
- 18F-rhPSMA-7 PET for the Detection of Biochemical Recurrence of Prostate Cancer After Curative-Intent Radiation Therapy: A Bicentric Retrospective Study
- Diagnostic Performance and Clinical Impact of 68Ga-PSMA-11 PET/CT Imaging in Early Relapsed Prostate Cancer After Radical Therapy: A Prospective Multicenter Study (IAEA-PSMA Study)
- Early Injection of Furosemide Increases Detection Rate of Local Recurrence in Prostate Cancer Patients with Biochemical Recurrence Referred for 68Ga-PSMA-11 PET/CT
- Head-to-Head Comparison of 68Ga-NOTA (68Ga-NGUL) and 68Ga-PSMA-11 in Patients with Metastatic Prostate Cancer: A Prospective Study
- Matched-Pair Comparison of 68Ga-PSMA-11 and 18F-rhPSMA-7 PET/CT in Patients with Primary and Biochemical Recurrence of Prostate Cancer: Frequency of Non-Tumor-Related Uptake and Tumor Positivity
- Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study
- Positive Predictive Value and Correct Detection Rate of 18F-rhPSMA-7 PET in Biochemically Recurrent Prostate Cancer Validated by Composite Reference Standard
- Impact of 68Ga-PSMA-11 PET on the Management of Recurrent Prostate Cancer in a Prospective Single-Arm Clinical Trial
- Prostate-Specific Membrane Antigen: The Target of the Decade, from Biochemical Recurrence to Widespread Adoption (perspective on "Evaluation of hybrid 68Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence After Radical Prostatectomy" J Nucl Med. 2015;56:668-674)
- Multiphasic 68Ga-PSMA PET/CT in the Detection of Early Recurrence in Prostate Cancer Patients with a PSA Level of Less Than 1 ng/mL: A Prospective Study of 135 Patients
- Mapping Prostate Cancer Lesions Before and After Unsuccessful Salvage Lymph Node Dissection Using Repeat PSMA PET
- 3-Year Freedom from Progression After 68Ga-PSMA PET/CT-Triaged Management in Men with Biochemical Recurrence After Radical Prostatectomy: Results of a Prospective Multicenter Trial
- 18F-DCFPyL PET/CT Imaging in Patients with Biochemically Recurrent Prostate Cancer After Primary Local Therapy
- 18F-rhPSMA-7 PET for the Detection of Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy
- Evaluation of an Automated Module Synthesis and a Sterile Cold Kit-Based Preparation of 68Ga-PSMA-11 in Patients with Prostate Cancer
- Histologically Confirmed Diagnostic Efficacy of 18F-rhPSMA-7 PET for N-Staging of Patients with Primary High-Risk Prostate Cancer
- Head-to-Head Comparison of 68Ga-PSMA-11 with 18F-PSMA-1007 PET/CT in Staging Prostate Cancer Using Histopathology and Immunohistochemical Analysis as a Reference Standard
- Appropriate Use Criteria for Imaging Evaluation of Biochemical Recurrence of Prostate Cancer After Definitive Primary Treatment
- Detection Rate and Localization of Prostate Cancer Recurrence Using 68Ga-PSMA-11 PET/MRI in Patients with Low PSA Values <= 0.5 ng/mL
- An 18F-Labeled PSMA Ligand for PET/CT of Prostate Cancer: First-in-Humans Observational Study and Clinical Experience with 18F-JK-PSMA-7 During the First Year of Application
- Prospective Evaluation of PSMA-Targeted 18F-DCFPyL PET/CT in Men with Biochemical Failure After Radical Prostatectomy for Prostate Cancer
- Matched-Pair Comparison of 68Ga-PSMA-11 PET/CT and 18F-PSMA-1007 PET/CT: Frequency of Pitfalls and Detection Efficacy in Biochemical Recurrence After Radical Prostatectomy
- Prostate-Specific Membrane Antigen-Guided Surgery
- Radiation Dosimetry and Biodistribution of 18F-PSMA-11 for PET Imaging of Prostate Cancer
- Blood-derived dendritic cell vaccinations induce immune responses that correlate with clinical outcome in patients with chemo-naive castration-resistant prostate cancer
- A Prospective Study on 18F-DCFPyL PSMA PET/CT Imaging in Biochemical Recurrence of Prostate Cancer
- 18F-Fluciclovine Parameters on Targeted Prostate Biopsy Associated with True Positivity in Recurrent Prostate Cancer
- Improving 68Ga-PSMA PET/MRI of the Prostate with Unrenormalized Absolute Scatter Correction
- Clinical Impact of Lower-Limb Imaging in 68Ga-PSMA PET/CT for Patients with Prostate Cancer
- qPSMA: Semiautomatic Software for Whole-Body Tumor Burden Assessment in Prostate Cancer Using 68Ga-PSMA11 PET/CT
- Detection Rate of 18F-Choline PET/CT and 68Ga-PSMA-HBED-CC PET/CT for Prostate Cancer Lymph Node Metastases with Direct Link from PET to Histopathology: Dependence on the Size of Tumor Deposits in Lymph Nodes
- Combination of 68Ga-PSMA PET/CT and Multiparametric MRI Improves the Detection of Clinically Significant Prostate Cancer: A Lesion-by-Lesion Analysis
- In Vitro and In Vivo Characterization of an 18F-AlF-Labeled PSMA Ligand for Imaging of PSMA-Expressing Xenografts
- Metaanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology
- Proceedings: Pathways for Successful Translation of New Imaging Agents and Modalities--Phase III Studies
- Follow-up of Lesions with Equivocal Radiotracer Uptake on PSMA-Targeted PET in Patients with Prostate Cancer: Predictive Values of the PSMA-RADS-3A and PSMA-RADS-3B Categories
- Detection Efficacy of 18F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy
- 68Ga-PSMA-11 PET/CT in Primary and Recurrent Prostate Carcinoma: Implications for Radiotherapeutic Management in 121 Patients
- 68Gallium-labelled PSMA-PET/CT as a diagnostic and clinical decision-making tool in Asian prostate cancer patients following prostatectomy
- Outcome After PSMA PET/CT-Based Salvage Radiotherapy in Patients with Biochemical Recurrence After Radical Prostatectomy: A 2-Institution Retrospective Analysis
- Modeling and Predicting Tumor Response in Radioligand Therapy
- The Effect of Including Bone in Dixon-Based Attenuation Correction for 18F-Fluciclovine PET/MRI of Prostate Cancer
- One-Stop-Shop Whole-Body 68Ga-PSMA-11 PET/MRI Compared with Clinical Nomograms for Preoperative T and N Staging of High-Risk Prostate Cancer
- A Prospective Comparison of 18F-Sodium Fluoride PET/CT and PSMA-Targeted 18F-DCFBC PET/CT in Metastatic Prostate Cancer
- Detection Threshold and Reproducibility of 68Ga-PSMA11 PET/CT in a Mouse Model of Prostate Cancer
- 68Ga-PSMA-HBED-CC Uptake in Cervical, Celiac, and Sacral Ganglia as an Important Pitfall in Prostate Cancer PET Imaging
- Molecular Imaging of Prostate Cancer: Choosing the Right Agent
- Prospective Evaluation of 68Ga-RM2 PET/MRI in Patients with Biochemical Recurrence of Prostate Cancer and Negative Findings on Conventional Imaging
- Comparison of 68Ga-PSMA-11 and 18F-Fluciclovine PET/CT in a Case Series of 10 Patients with Prostate Cancer Recurrence
- The Utility of PET/CT in the Planning of External Radiation Therapy for Prostate Cancer
- Biochemical Recurrence of Prostate Cancer: Initial Results with [18F]PSMA-1007 PET/CT
- 64CuCl2 PET/CT in Prostate Cancer Relapse
- Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed miTNM Classification for the Interpretation of PSMA-Ligand PET/CT
- Impact of 68Ga-PSMA-11 PET/CT on the Management of Prostate Cancer Patients with Biochemical Recurrence
- Proposal for a Structured Reporting System for Prostate-Specific Membrane Antigen-Targeted PET Imaging: PSMA-RADS Version 1.0
- Low-Level Endogenous PSMA Expression in Nonprostatic Tumor Xenografts Is Sufficient for In Vivo Tumor Targeting and Imaging
- Anatomic and Molecular Imaging in Prostate Cancer
- Immunohistochemical Validation of PSMA Expression Measured by 68Ga-PSMA PET/CT in Primary Prostate Cancer
- 68Ga-PSMA-11 PET/CT Mapping of Prostate Cancer Biochemical Recurrence After Radical Prostatectomy in 270 Patients with a PSA Level of Less Than 1.0 ng/mL: Impact on Salvage Radiotherapy Planning
- Impact of 68Ga-Prostate-Specific Membrane Antigen PET/CT on Prostate Cancer Management
- The Impact of 68Ga-PSMA PET/CT on Management Intent in Prostate Cancer: Results of an Australian Prospective Multicenter Study
- Treatment Outcomes from 68Ga-PSMA PET/CT-Informed Salvage Radiation Treatment in Men with Rising PSA After Radical Prostatectomy: Prognostic Value of a Negative PSMA PET
- Detection of Synchronous Primary Malignancies with 68Ga-Labeled Prostate-Specific Membrane Antigen PET/CT in Patients with Prostate Cancer: Frequency in 764 Patients
- Impact of 68Ga-PSMA-11 PET on Management in Patients with Biochemically Recurrent Prostate Cancer
- Seduction by Sensitivity: Reality, Illusion, or Delusion? The Challenge of Assessing Outcomes after PSMA Imaging Selection of Patients for Treatment
- Will GRPR Compete with PSMA as a Target in Prostate Cancer?
- 68Ga-PSMA PET/CT and Volumetric Morphology of PET-Positive Lymph Nodes Stratified by Tumor Differentiation of Prostate Cancer
- Initial Experience with Volumetric 68Ga-PSMA I&T PET/CT for Assessment of Whole-Body Tumor Burden as a Quantitative Imaging Biomarker in Patients with Prostate Cancer
- A Prospective Study Comparing 99mTc-Hydroxyethylene-Diphosphonate Planar Bone Scintigraphy and Whole-Body SPECT/CT with 18F-Fluoride PET/CT and 18F-Fluoride PET/MRI for Diagnosing Bone Metastases
- 68Ga-PSMA-11 PET/CT Interobserver Agreement for Prostate Cancer Assessments: An International Multicenter Prospective Study
- PSMA Ligands for PET Imaging of Prostate Cancer
- Exploring New Multimodal Quantitative Imaging Indices for the Assessment of Osseous Tumor Burden in Prostate Cancer Using 68Ga-PSMA PET/CT
- Phase 2 Study of 99mTc-Trofolastat SPECT/CT to Identify and Localize Prostate Cancer in Intermediate- and High-Risk Patients Undergoing Radical Prostatectomy and Extended Pelvic LN Dissection
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- Acceleration of PSMA-Targeted Theranostics to the Clinic: Can Common Sense Prevail?
- 68Ga-THP-PSMA: A PET Imaging Agent for Prostate Cancer Offering Rapid, Room-Temperature, 1-Step Kit-Based Radiolabeling
- Detection Efficacy of Hybrid 68Ga-PSMA Ligand PET/CT in Prostate Cancer Patients with Biochemical Recurrence After Primary Radiation Therapy Defined by Phoenix Criteria
- 68Ga-PSMA-PET/CT Has a Role in Detecting Prostate Cancer Lesions in Patients with Recurrent Disease
- PSA-Stratified Performance of 18F- and 68Ga-PSMA PET in Patients with Biochemical Recurrence of Prostate Cancer
- Semiquantitative Parameters in PSMA-Targeted PET Imaging with 18F-DCFPyL: Variability in Normal-Organ Uptake
- Isolated prostate cancer soft tissue recurrence 10 years after radical prostatectomy
- 68Ga or 18F for Prostate Cancer Imaging?
- The Clinical Impact of Additional Late PET/CT Imaging with 68Ga-PSMA-11 (HBED-CC) in the Diagnosis of Prostate Cancer
- 68Ga-PSMA-11 PET as a Gatekeeper for the Treatment of Metastatic Prostate Cancer with 223Ra: Proof of Concept
- Impact of 18F-Fluciclovine PET on Target Volume Definition for Postprostatectomy Salvage Radiotherapy: Initial Findings from a Randomized Trial
- Radiation Dosimetry for 177Lu-PSMA I&T in Metastatic Castration-Resistant Prostate Cancer: Absorbed Dose in Normal Organs and Tumor Lesions
- Preclinical Evaluation and First Patient Application of 99mTc-PSMA-I&S for SPECT Imaging and Radioguided Surgery in Prostate Cancer
- German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients
- 68Ga-PSMA-11 PET Imaging of Response to Androgen Receptor Inhibition: First Human Experience
- Molecular Imaging and Therapy with a Purpose: A Renaissance of Nuclear Medicine
- Value of 68Ga-PSMA HBED-CC PET for the Assessment of Lymph Node Metastases in Prostate Cancer Patients with Biochemical Recurrence: Comparison with Histopathology After Salvage Lymphadenectomy
- The Rise of PSMA Ligands for Diagnosis and Therapy of Prostate Cancer
- PSMA-Based Radioligand Therapy for Metastatic Castration-Resistant Prostate Cancer: The Bad Berka Experience Since 2013
- (2S)-2-(3-(1-Carboxy-5-(4-211At-Astatobenzamido)Pentyl)Ureido)-Pentanedioic Acid for PSMA-Targeted {alpha}-Particle Radiopharmaceutical Therapy
- Bombesin-Targeted PET of Prostate Cancer