


Abstract
We evaluated the incidence of synchronous primary malignancies in patients undergoing 68Ga-labeled prostate-specific membrane antigen PET/CT for prostate cancer (PC). Methods: Reports for 764 PC patients were reviewed. Incidental lesions atypical for PC metastases and suggestive of a synchronous primary malignancy were identified. Follow-up was obtained to confirm etiology. Results: Lesions atypical for PC metastases were found in 49 (6.4%) of 764 patients, and a synchronous primary malignancy was confirmed in 5 patients (0.7%; 2 lung, 1 lymphoma, 1 thyroid, and 1 base of tongue). In 8 patients (1.0%), lesions were proven to be atypical metastases from PC. In 24 patients (3.1%), lesions had a benign etiology. Follow-up was not available in 12 patients (1.6%). Conclusion: Synchronous 68Ga-labeled prostate-specific membrane antigen–avid malignancies were rare (0.7%) in PC patients; atypical lesions were more commonly unusual PC metastases (1.0%) or benign (3.1%).
In the United States, prostate cancer (PC) is the most common cancer and the second most frequent cause of cancer-related death in men (1). Early diagnosis, accurate staging, and tumor characterization are critical for appropriate selection of patient-tailored therapy. CT, MRI, and bone scanning, although widely used in the diagnosis, staging, and restaging of PC, have suboptimal accuracy. This limitation was recently addressed by the introduction of 68Ga-labeled prostate-specific membrane antigen (PSMA) PET/CT. Several studies revealed higher diagnostic accuracy of 68Ga-PSMA PET/CT than of conventional imaging, including PET with other tracers (2–4). However, clinical experience with reading 68Ga-PSMA PET/CT scans is limited, pending U.S. Food and Drug Administration approval and Centers for Medicare and Medicaid Services payment. Despite the promise of 68Ga-PSMA, its uptake and avidity have been reported to be not completely specific to PC, with recent case reports of uptake in benign lesions as well as non-PC malignancies (5–13). The objective of the present study was to determine the incidence of synchronous 68Ga-PSMA–avid malignancies in a large group of patients undergoing evaluation for known PC.
MATERIALS AND METHODS
Patient Population
A total of 764 patients (mean age, 68 y; range, 48–85) who had undergone 68Ga-PSMA PET/CT from 2013 to 2016 for known PC (73 for staging and 691 for restaging) were included. This single-center retrospective study was approved by the Institutional Human Research Ethics Committee, with a waiver of informed consent of patients who had been scanned for clinical indications.
68Ga-PSMA PET/CT Image Acquisition and Protocol
68Ga was eluted from a 68Ga/68Ge generator (Isotope Technology Group) and compounded with hydroxybenzylethylenediamine diacetic acid (HBED)-PSMA11 (Advanced Biochemical Compounds). PET images were acquired approximately 60 min (range, 40–85) after injection of 68Ga-HBED-PSMA11 at 2 MBq/kg (166 MBq; range, 91–246). Acquisition was performed on a GE Discovery PET/CT 690 or 710 scanner (GE Healthcare) or a Siemens Biograph 64 PET/CT scanner (Siemens Healthcare). CT was performed either with a low-dose noncontrast technique (old protocol) or 10 min (range, 8–15) after intravenous injection of 50 mL of iohexol (Omnipaque [GE Healthcare]; 300 g/mL) contrast medium for optimal ureteral enhancement (new protocol as of mid-2015).
Data Analysis
All reports from clinical 68Ga-PSMA PET/CT were reviewed. We selected for further evaluation lesions with or without 68Ga-PSMA uptake, lesions that were not previously detected by other modalities, and lesions that were considered atypical in location for PC metastases on PET/CT and that were interpreted by the reporting PET specialist as being suggestive of a synchronous primary malignancy. Histopathologic, imaging, and clinical follow-up was obtained to confirm the etiology of these findings.
RESULTS
Possible synchronous malignant tumors were reported in 49 (6.4%) of 764 PC patients (Table 1). In 42 (85.7%) of these 49 patients, the lesions were 68Ga-PSMA–avid, whereas in the remaining 7 patients (14.3%), the lesions were detected only on the contemporaneous CT component of the study.
Summary of Results for 764 Patients
In 8 (1.0%) of 764 patients, 68Ga-PSMA–avid lesions were histologically proven to be metastases from PC (Fig. 1) in the lungs (4 cases) and lymph nodes (4 cases). However, in 5 (0.7%) of 764 patients, 68Ga-PSMA–avid lesions were pathologically proven to be synchronous primary malignancies (Figs. 2 and 3). Proven sites were the lungs (2 cases), thyroid (1 case), base of the tongue (1 case), and lymphoma (1 case).

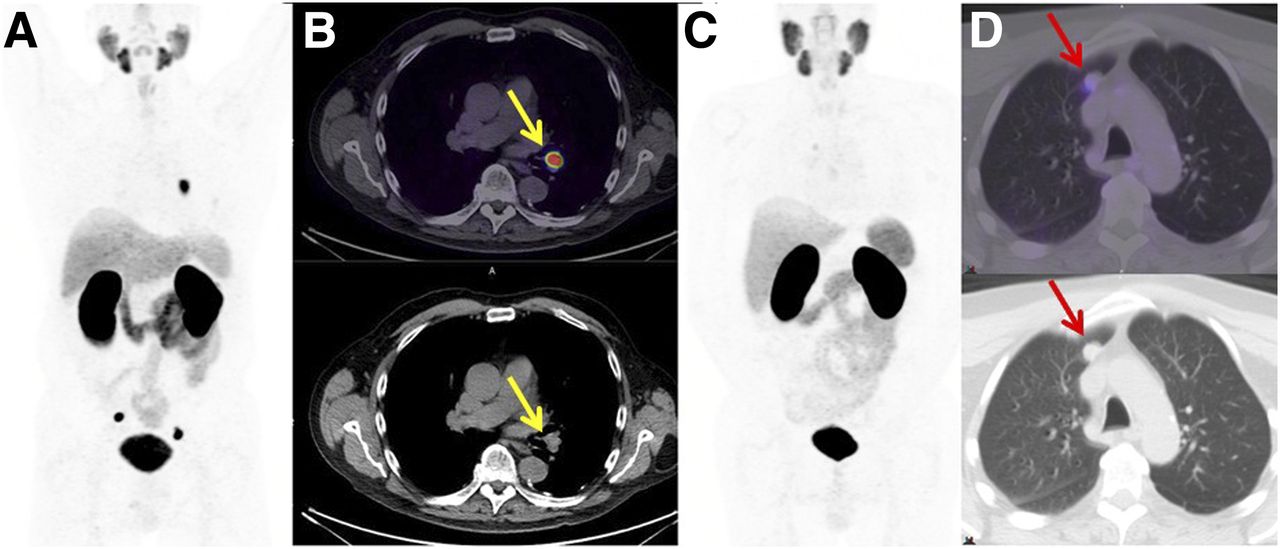
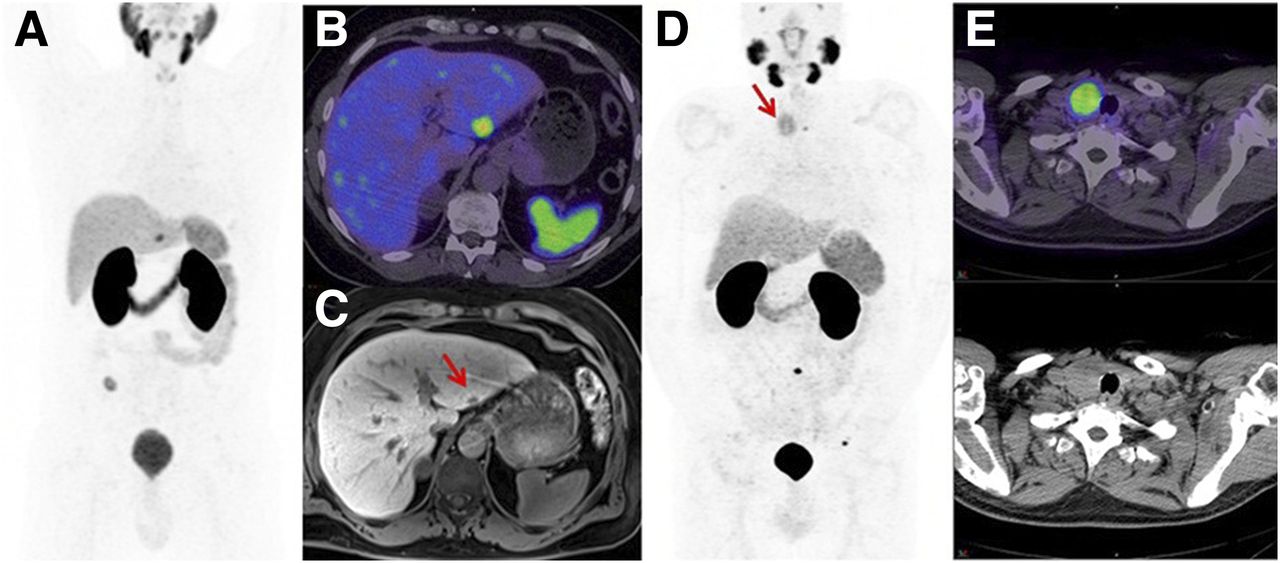
Biopsy-confirmed PC. (A and B) Left hilar node (arrows) (SUVmax, 30). (C and D) Right upper-lobe nodule (arrows) (SUVmax, 3).

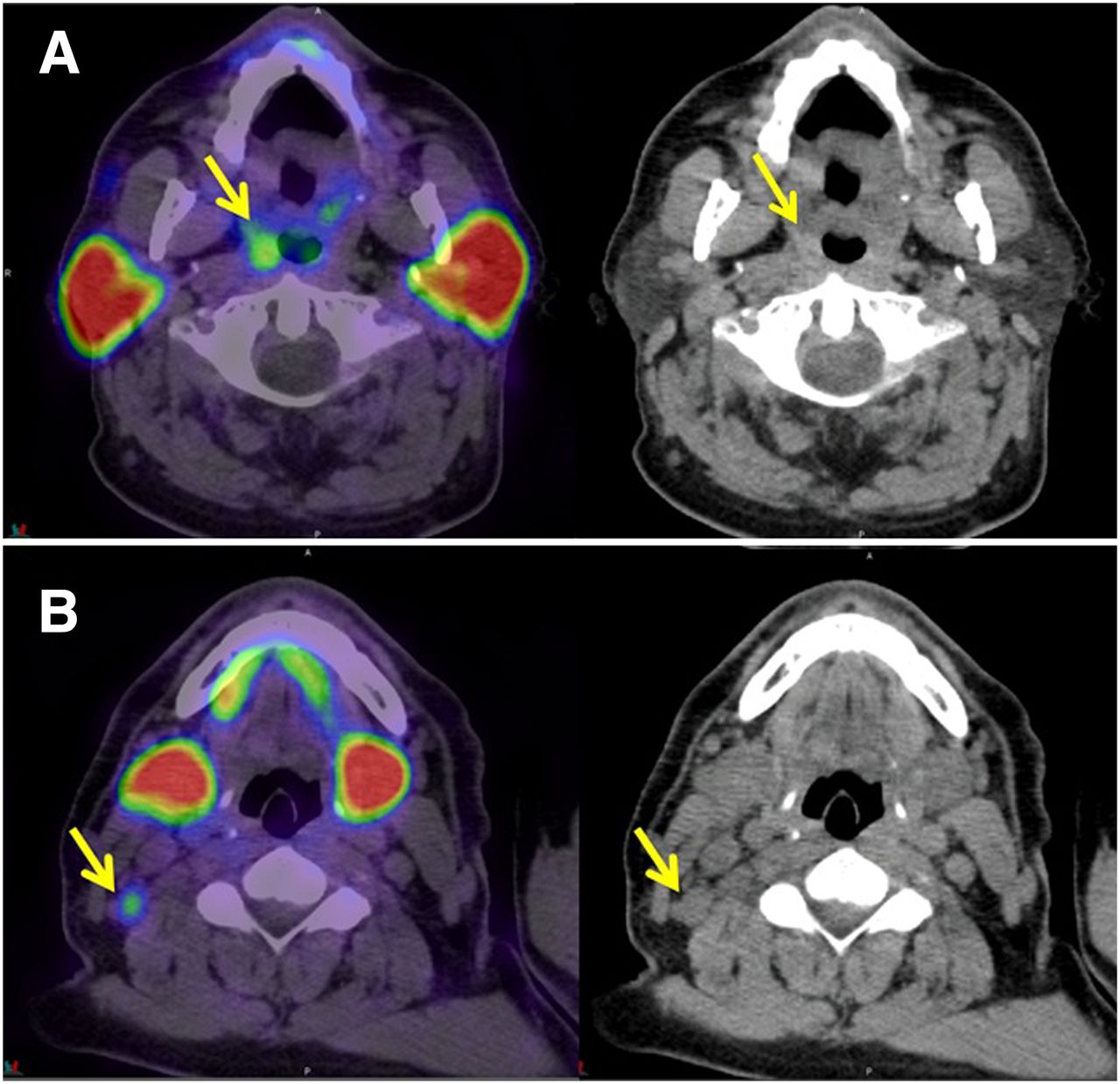
Incidental findings on 68Ga-PSMA PET/CT of focal uptake (arrows) (SUVmax, 5.3) in right oropharynx (A) and ipsilateral mildly enlarged level II lymph nodes (arrows) (SUVmax, 3.6) (B). Biopsy demonstrated squamous cell carcinoma.

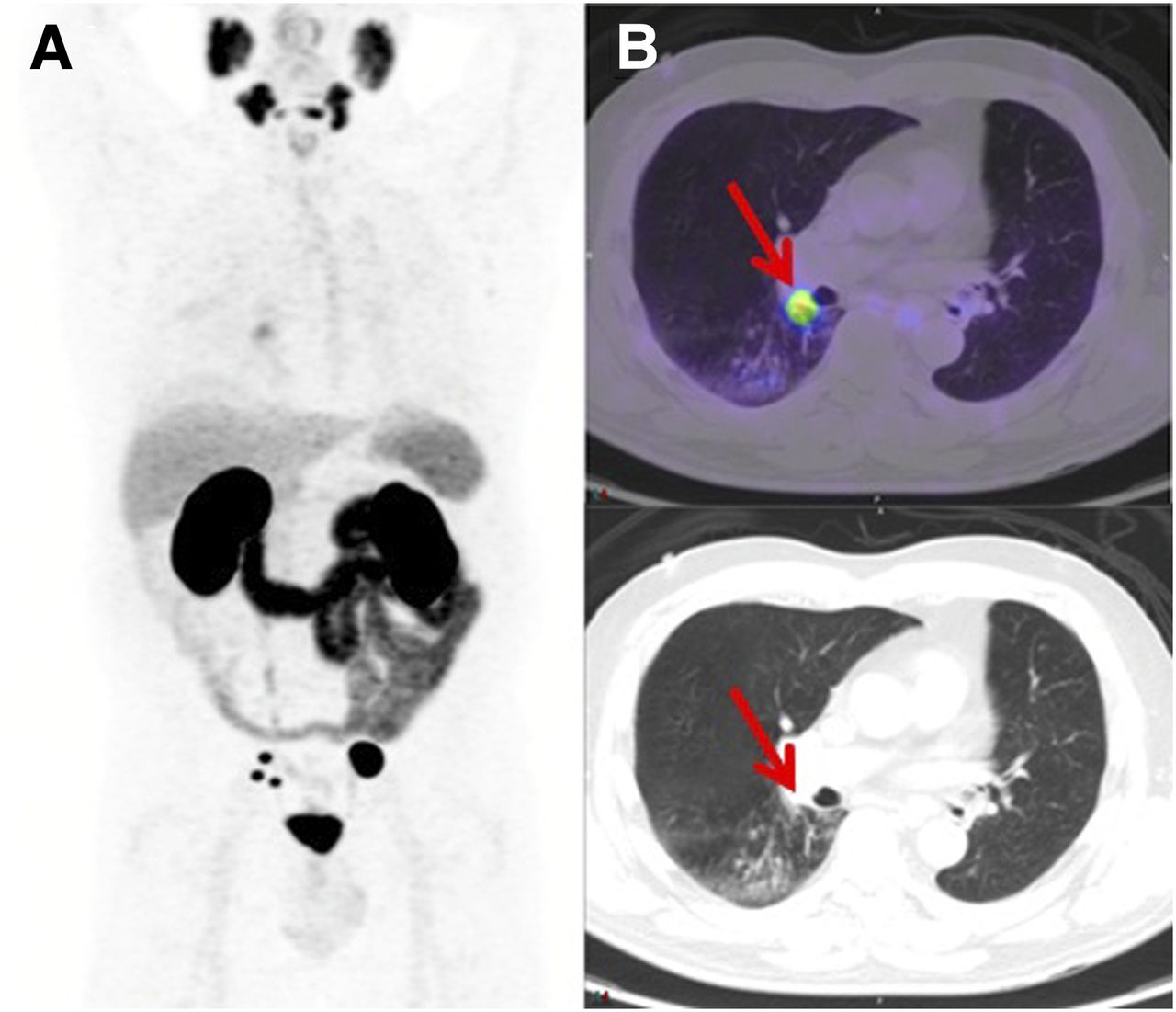
Maximum-intensity projection (A) and fused axial PET/CT and CT (B) showing focal uptake (arrows) (SUVmax, 7) in small right hilar mass on background of more intense uptake in several pelvic nodes (SUVmax, 79). Biopsy demonstrated lung adenocarcinoma.
In 22 patients (with lesions in the following locations: 5 lung, 4 thyroid, 3 liver, 3 lymph node, 2 spleen, 1 brain, 1 pancreas, 1 bone, 1 soft tissue, and 1 skin), there was no progression on follow-up imaging (Figs. 4A, 4B, and 4C) or clinical examination, suggesting benign diagnoses. One patient had a normal endoscopic evaluation for a suspected laryngeal lesion, which likely represented physiologic salivary pooling. One thyroid lesion was a biopsy-proven benign hyperplastic nodule (Figs. 4D and 4E). All biopsy-proven cases are shown in Table 2. In 12 (1.6%) of 764 patients, the follow-up record was not yet available or the final diagnosis of the detected lesion had not yet been clarified.
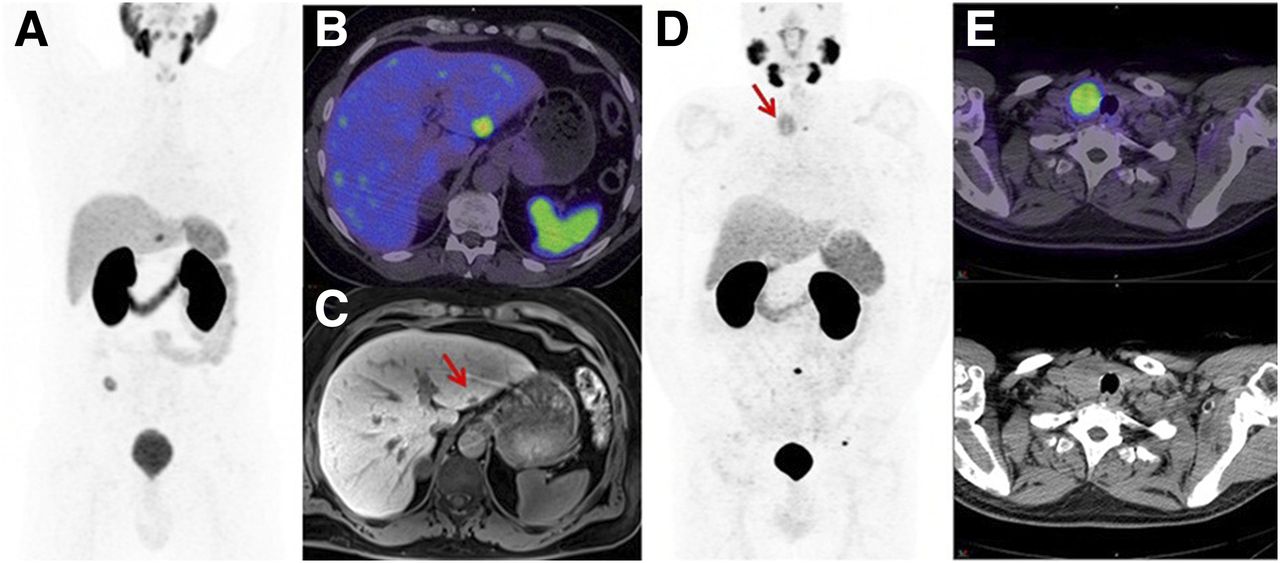
Maximum-intensity projection (A), PET/CT (B), and delayed contrast MRI (C) showing small liver lesion (arrow) (SUVmax, 15), with no abnormality seen on low-dose CT. MRI demonstrated arterial-phase enhancement matching blood pool, consistent with hemangioma. Maximum-intensity projection (D) and fused axial PET/CT and CT (E) showing 40-mm thyroid nodule (arrow) (SUVmax, 6.3). Ultrasound demonstrated predominantly solid, mainly hyperechoic lesion with low-echo rim and increased vascularity. Biopsy demonstrated benign hyperplastic nodule (Bethesda category 2).
Pathology-Proven Cases
For the 7 patients with 68Ga-PSMA–negative lesions identified on contemporaneous CT, 5 lesions were in the lung and 2 were in the thyroid. PC metastases or additional non-PC malignancies were not confirmed for any of these lesions.
DISCUSSION
PSMA is a transmembrane glycoprotein expressed in normal prostate epithelium but overexpressed in virtually all PCs (14). 68Ga-PSMA PET/CT produces images with high tumor-to-background contrast, resulting in high sensitivity and specificity for the detection of PC (4). The accuracy of 68Ga-PSMA PET/CT for the detection of PC was recently evaluated in a systematic review and metaanalysis of 16 articles involving studies of 1,309 patients (15). As determined by a per-patient analysis, the summary sensitivity and specificity were both 86%.
PSMA is also expressed on the neovasculature of many solid tumors (16). Because of the relatively limited clinical experience with 68Ga-PSMA PET/CT, examples of incidental detection of synchronous 68Ga-PSMA–avid malignancies are limited to recent case reports (7–13). In the present study, atypical 68Ga-PSMA–avid lesions were confirmed to be second primary malignancies in only 5 (0.7%) of 764 patients. In our experience, it was more uncommon to encounter 68Ga-PSMA–avid lymph nodes at unexpected locations, either as atypical PC metastases (Fig. 1) or due to additional primary malignancies (Fig. 2). In most cases, the intensity of metabolic activity in nodal or distant metastases parallels that in the primary site of malignancy (17). Therefore, encountering discordant low-grade 68Ga-PSMA activity in multiple enlarged lymph nodes should raise the level of suspicion for a second primary malignancy, such as lymphoma (patient 8 in Table 2). In our experience, a 68Ga-PSMA–avid thyroid lesion could be an exception to the rule for 68Ga-PSMA, in that a benign nodule might present with higher 68Ga-PSMA avidity than the primary PC (Fig. 4; patient 9 in Table 2).
In the present study, lesions atypical for PC metastases (with or without 68Ga-PSMA avidity) were found in 49 (6.4%) of 764 patients. In 8 (1.0%) of 764 patients, atypical 68Ga-PSMA–avid lesions were proven to be metastases from PC. Because of the high sensitivity and specificity of 68Ga-PSMA PET/CT for PC evaluation, differentiation between typical metastases and atypical metastases is evolving as the modality redefines patterns of PC spread. Given the age of patients with PC, encountering lung lesions with or without 68Ga-PSMA avidity is not uncommon, and the degree of uptake may not be reliable for differentiating PC metastases from lung cancer (Fig. 1D vs. Fig. 3). In fact, quantitative analysis of 68Ga-PSMA PET/CT results does not reliably discriminate between pulmonary metastases and primary lung cancer in PC patients (9). Therefore, isolated atypical 68Ga-PSMA–avid lung lesions may need pathologic confirmation. Also, non–68Ga-PSMA–avid lung lesions may need further CT surveillance, 18F-FDG PET/CT, or biopsy.
In 24 (3.1%) of 764 patients, atypical lesions (with or without 68Ga-PSMA avidity) had a benign etiology, as determined by additional follow-up imaging or investigations. To confirm benign causes, stability over time should be confirmed. Also, in the absence of nodal disease, an isolated 68Ga-PSMA–avid lesion at an atypical location is unlikely to be a PC-related distant metastasis. For example, liver metastases from PC are typically multiple, so an isolated 68Ga-PSMA–avid liver lesion as the only metastatic site is less likely. In such cases, multiphase CT or MRI should be performed for further characterization (Fig. 4).
Correct and careful interpretation of the CT scan as part of a 68Ga-PSMA PET/CT examination is of special importance, not only for differentiating physiologic uptake in ganglia or ureters from that in lymph nodes but also for the detection of non–68Ga-PSMA–avid lesions. Seven (14.3%) of 49 patients with lesions atypical for PC metastases had non–68Ga-PSMA–avid lesions detected only on the CT component of the PET/CT examination (5 lung and 2 thyroid). However, none of these was a second primary malignancy or metastasis from PC, suggesting that indeterminate CT findings are frequently benign. Because intravenous contrast material was not routinely used for the contemporaneous CT for all patients, non–68Ga-PSMA–avid but morphologically suggestive lesions could have been underestimated in our analysis.
The present study was limited by retrospective analysis. The reporting styles of readers vary, and our results might not be generalizable to other centers. We aimed to report with high specificity, acknowledging the consequent trade-off in sensitivity, to minimize the likelihood of adverse patient outcomes from false-positive results (17). In addition, the advanced stage of PC patients undergoing 68Ga-PSMA PET/CT, coupled with the relatively short follow-up period and high percentage of cases from remote facilities, led to a relatively high number of patients without a follow-up record or a final diagnosis for the detected lesion.
CONCLUSION
Synchronous 68Ga-PSMA–avid malignancies were rare (0.7%) in PC patients with atypical lesions, which were more commonly unusual PC metastases (1.0%) or benign (3.1%). These findings support the high specificity of 68Ga-PSMA PET/CT for PC, with further investigations for atypical 68Ga-PSMA–avid lesions or CT findings being required in a minority of cases.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 1, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 20, 2017.
- Accepted for publication May 4, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}