


Abstract
Our objective was to evaluate the biodistribution, kinetics, and radiation dosimetry of 64CuCl2 in humans and to assess the ability of 64CuCl2 PET/CT to detect prostate cancer (PCa) recurrence in patients with biochemical relapse. Methods: We prospectively evaluated 50 PCa patients with biochemical relapse after surgery or external-beam radiation therapy. All patients underwent 64CuCl2 PET/CT, 18F-choline PET/CT, and multiparametric MRI within 15 d of each other. Experienced readers interpreted the images, and the detection rate (DR) of each imaging modality was calculated. Histopathology, when available; clinical or laboratory response; and multidisciplinary follow-up were used to confirm the site of disease. In parallel, biodistribution, kinetics of the lesions, and radiation dosimetry of 64CuCl2 were evaluated. Results: From a dosimetric point of view, an administered dose of 200 MBq for 64CuCl2 translated into a 5.7-mSv effective dose. Unlike 18F-choline, 64CuCl2 was not excreted or accumulated in the urinary tract, thus allowing thorough pelvic exploration. The maximum 64CuCl2 uptake at the sites of PCa relapse was observed 1 h after tracer injection. In our cohort, 64CuCl2 PET/CT proved positive in 41 of 50 patients, with an overall DR of 82%. The DRs of 18F-choline PET/CT and multiparametric MRI were 56% and 74%, respectively. The difference between the DRs of 64CuCl2 PET/CT and 18F-choline PET/CT was statistically significant (P < 0.001). Interestingly, on considering prostate-specific antigen (PSA) value, 64CuCl2 PET/CT had a higher DR than 18F-choline PET/CT in patients with a PSA of less than 1 ng/mL. Conclusion: The biodistribution of 64CuCl2 is more suitable than that of 18F-choline for exploring the pelvis and prostatic bed. The 64CuCl2 effective dose is like those of other established PET tracers. In patients with biochemical relapse and a low PSA level, 64CuCl2 PET/CT shows a significantly higher DR than 18F-choline PET/CT.
See an invited perspective on this article on page 442.
Copper is a chemical element required for the normal functioning of many molecules involved in the signal transduction pathway regulating cell proliferation. It plays an important role in tumor angiogenesis (1–3) and can stimulate endothelial cell proliferation (4). So far, we know that copper metabolism and its cellular deposition are altered in neoplastic disease (5). Several authors have reported an increased copper content in tumors (6,7), giving rise to the possibility of using elevated copper concentration in cancer cells as an imaging biomarker for metabolic PET imaging (8,9). Human copper transporter 1 is a high-affinity copper transporter that mediates cellular uptake of copper in humans (10). This transporter is well represented in human cancer, including prostate tumor cells. Preclinical studies have shown that human prostate cancer (PCa) xenograft models in mice display an increased uptake of copper administered as 64CuCl2 (10,11). So far, only one paper, involving few patients, has confirmed the ability of 64CuCl2 PET/CT to detect PCa sites of disease in humans (12). To the best of our knowledge, no studies have assessed the ability of 64CuCl2 PET/CT to detect PCa relapse after surgery or external-beam radiation therapy (EBRT).
Whereas 18F-choline and 11C-choline remain the most validated tracers for the detection of recurrent PCa (13,14), they have significant limitations in terms of sensitivity in the case of low prostate-specific antigen (PSA) level and long PSA doubling time (15). In this field, the recent introduction of new PET radiopharmaceuticals (e.g., 68Ga-PSMA and 18F-FACBC) (16–19), and the possibility of obtaining PET/MRI using dedicated software (20,21) or dedicated tomographs (22), have increased sensitivity in the early detection of PCa relapse, especially in the case of low PSA levels.
In the current trial we aimed to evaluate, for the first time, the ability of 64CuCl2 PET/CT to detect PCa recurrence in patients presenting with biochemical relapse. We compared all the above-mentioned results with those of 18F-choline PET/CT and multiparametric MRI (mpMRI). We also aimed to assess the clinical safety, biodistribution, and radiation dosimetry of 64CuCl2 in humans. Moreover, we studied the 64CuCl2 kinetics of sites of PCa relapse.
MATERIALS AND METHODS
The local ethics committee and the “Agenzia Italiana del Farmaco,” a public agency of the Italian Ministry of Health, approved this study. All subjects signed a written informed consent form. The trial was registered in the European Clinical Trial Database (EudraCT number 2014-005140-18).
Patient Population
From February to October 2016, we prospectively evaluated 50 PCa patients presenting with biochemical relapse (23) after first-line surgery or EBRT. We also included patients with rising PSA levels after salvage EBRT or hormone therapy. All patients underwent 64CuCl2 PET/CT, 18F-choline PET/CT, and mpMRI within 15 d of one another. Table 1 shows the main characteristics of patients and tumors.
Patient Characteristics
64CuCl2 PET/CT
The production of the experimental 64CuCl2 (Sparkle s.r.l.) was approved by Agenzia Italiana del Farmaco. The radiopharmaceutical was prepared in accordance with good manufacturing practices and administered intravenously to fasting patients (≥6 h). Whole-body 64CuCl2 PET/CT was performed 60 min (12) after injection of 200–250 MBq of 64CuCl2. PET scans were acquired in 3-dimensional mode by a PET/CT system (Discovery ST; GE Healthcare). Considering the relatively low positron production and 511-keV photon emission (yield) of 64Cu when compared with those of 18F, PET/CT scans were acquired via 6-min emissions per bed position from the upper neck to the upper thighs, by means of sequential fields of view, each covering 12 cm (matrix of 256 × 256). Images were visualized on a Xeleris Workstation, version 2.1753 (GE Healthcare).
Low-dose CT was performed for both attenuation correction and topographic localization. The CT parameters used for acquisition were 140 kV, 80 mA, and 0.5 s per rotation, with a pitch of 6:1 and a slice thickness of 3.25 mm.
To evaluate the biodistribution and dosimetry of this radiopharmaceutical, all 50 patients underwent another 2 PET/CT acquisitions 4 h and 24 h after tracer injection. The second acquisition time (4 h) was selected in order to have a late acquisition on the same day as the tracer injection to facilitate patient compliance. The third acquisition time (24 h) was selected in order to have a late PET/CT acquisition (after 2 half-lives of the tracer) to improve the quality of the kinetics study.
To evaluate the potential hepatic radiotoxicity of 64CuCl2 administration, according to Agenzia Italiana del Farmaco suggestions, blood tests were performed on all patients and used to determine the following parameters: hematocrit, hemoglobin, C-reactive protein, aspartate transaminase, alanine transaminase, alkaline phosphatase, albumin, total bilirubin, γ-glutamyl transferase, lactate dehydrogenase, total proteins, serum creatinine, and azotemia. The tests were performed immediately before radiopharmaceutical administration and 10 d after the first 64CuCl2 whole-body scan.
18F-Choline PET/CT
18F-choline PET/CT was performed in the fasting state (≥6 h). An 18F-choline activity of 200 MBq (IASOcholine; IASON Labormedizin GesmbH und Co. KG) was administered intravenously; data were acquired 20 min after the injection by means of the above-mentioned PET/CT system. PET was performed over an acquisition time of 3 min in the same manner as for 64CuCl2 PET/CT and visualized on the same workstation. The same CT parameters were also used.
mpMRI
All patients underwent mpMRI performed with a 1.5-T MRI scanner (Signa HDxt; GE Healthcare) equipped with an 8-channel pelvic phased-array surface coil. The procedure was performed according to a standardized protocol (20). A large–field-of-view fast spin echo T2-weighted sequence was set in order to visualize the pelvis and infrarenal paracaval and paraaortic lymph node stations. High-resolution oblique axial and coronal scans were further oriented perpendicular and parallel to the rectoprostatic plane. Diffusion-weighted imaging was acquired in the axial plane, using the same slice locations as for the first fast spin echo T2-weighted sequence. Dynamic contrast-enhanced MRI was acquired during intravenous injection of the paramagnetic contrast medium with a flow rate of 3 mL/s. A 3-dimensional spoiled gradient echo fat-saturated T1-weighted pulse sequence was repeated in the axial plane 27 times with a temporal resolution of 12 s, during the injection of a single dose of contrast agent. An axial short T1 inversion recovery sequence was performed to detect focal bone lesions.
Image Interpretation
All PET images were reviewed by 2 experienced nuclear medicine physicians (at least 5 y of experience in PET/CT examinations) masked to other PET/CT and mpMRI results. On 18F-choline PET/CT and 64CuCl2 PET/CT, any focal, nonphysiologic uptake higher than that of the surrounding background level was considered pathologic. The reference tissues were the prostate parenchyma, prostatic fossa, residual seminal vesicles, vesicourethral anastomoses, abdominal and pelvic lymph nodes, and bone.
18F-choline PET/CT and 64CuCl2 PET/CT studies were interpreted visually and semiquantitatively using the SUVmax, on a patient-by-patient and lesion-by-lesion basis. In patient-based analysis, detection rate (DR) was defined as the ability to detect at least one pathologic finding in each subject. In lesion-based analysis, the DR was defined as the ability to detect suspected lesions in relation to the total number of lesions detected by both tracers and mpMRI (17).
Tumor-to-background ratios (TBRs) were determined for each lesion on both the 64CuCl2 and the 18F-choline images. TBR was established by placing a 2-dimensional region of interest in the pelvis and measuring the SUVmax of the background fat within the area (16). This value was then used as the denominator for the TBR. No SUVmax or TBR cutoffs were introduced to assess tumor lesions, although these parameters were calculated as a support to visual interpretation.
All mpMRI studies were reviewed on a dedicated workstation (Advantage Workstation, version 4.6; GE Healthcare) by an abdominal radiologist (with at least 5 y of experience in prostate mpMRI) masked to the results of the PET studies.
PCa recurrence was diagnosed when a focal morphologic alteration was accompanied by at least one corresponding functional abnormality (on apparent-diffusion-coefficient or perfusion maps) or when 2 functional mpMRI criteria were present without a definite morphologic lesion. Morphologic criteria were also adopted to distinguish between benign and malignant lymph nodes (i.e., short-axis diameter > 10 mm) (20,21). The axial short T1 inversion recovery sequence was used to detect bone metastases.
Standard of Reference
Although only DRs were calculated for each diagnostic modality, we applied a standard of reference, which could provide some confirmation of the site of disease. Histopathology was performed on transrectal ultrasound–guided biopsy in 7 of 25 patients (28%) showing only local recurrence; this confirmed the presence of disease. Moreover, undetectable PSA values were found after salvage EBRT in another 4 of the 11 patients with only local recurrence and not previously treated with EBRT. For lymph node and distant metastases, we used a multidisciplinary follow-up based on mpMRI, 18F-choline PET/CT, and reduction of PSA values after salvage therapy. A median follow-up time of 7 mo (range, 5–15 mo) was available for each patient.
Radiation Dosimetry
For dosimetric calculation, volumes of interest were drawn, for all PET and CT datasets, using automatic rigid coregistration (PMOD). Time–activity curves for all organs and for the total body were fitted as a biexponential function. We calculated accumulated activity for each organ (the sum of all nuclear transitions inside the organ) as the area under the time–activity curve, and the residence time was obtained by dividing accumulated activity by administered activity. The accumulated activity of the remainder of the body was calculated by subtracting all source organs from the total-body activity. The absorbed dose for each organ was calculated using the MIRD system (24,25). S factors specific for a reference adult male for 64Cu are tabulated in OLINDA/EXM software (26). The effective dose was also calculated using the coefficients of radiosensitivity of the organs present in publications 60 and 103 of ICRP (27,28).
Lesion Kinetics
To evaluate lesion kinetics, volumes of interest were drawn for all PET and CT datasets using automatic rigid coregistration (PMOD). Time–activity curves for various lesions (all local-relapse lymph-node metastases with short axis diameter > 15 mm and all bones metastases) were fitted as a biexponential function to calculate maximum specific uptake and clearance.
Statistical Methods
Since no literature data were available on the experimental diagnostic method used, no formal test hypothesis or sample size calculation was made; therefore, the study was intended as a pilot, and sample size (n = 50) was determined on the basis of feasibility. The primary objective was to calculate and compare the DRs of the experimental tests (64CuCl2 PET/CT) with those of the standard tests (18F-choline PET/CT and mpMRI).
The main descriptive statistics used were median, minimum, and maximum for continuous data and absolute and relative frequency for categoric data. DRs were calculated as the ratio between the number of positive patients (or lesions in the case of lesion-based analysis) and the total number of patients enrolled (or lesions). The exact binomial 95% confidence intervals of the DRs were calculated. The χ2 and Fisher exact tests were adopted to compare categoric data; the exact McNemar test was used to compare DRs between diagnostic procedures on the same subjects, also stratified by total PSA levels (<1, 1.1–2, 2.1–4, and >4 ng/mL). A 2-tailed, paired test was used to analyze and compare TBR ratios between scans. Because the study was exploratory, no corrections for multiple tests were applied. Statistical significance was assigned to values of α-error (2-tailed) lower than 0.05. All statistical analyses used Stata software (release 14; StataCorp LP).
RESULTS
Adverse Events
No drug-related pharmacologic effects or physiologic responses occurred. No adverse reactions were observed after the injection of 64CuCl2. All observed parameters (i.e., blood pressure, heart rate, body temperature) remained normal and unchanged during and after the examination. No patient reported subjective symptoms. In addition, no modification of the above-mentioned blood tests was reported 10 d after 64CuCl2 injection.
Tracer Distribution and Dosimetry
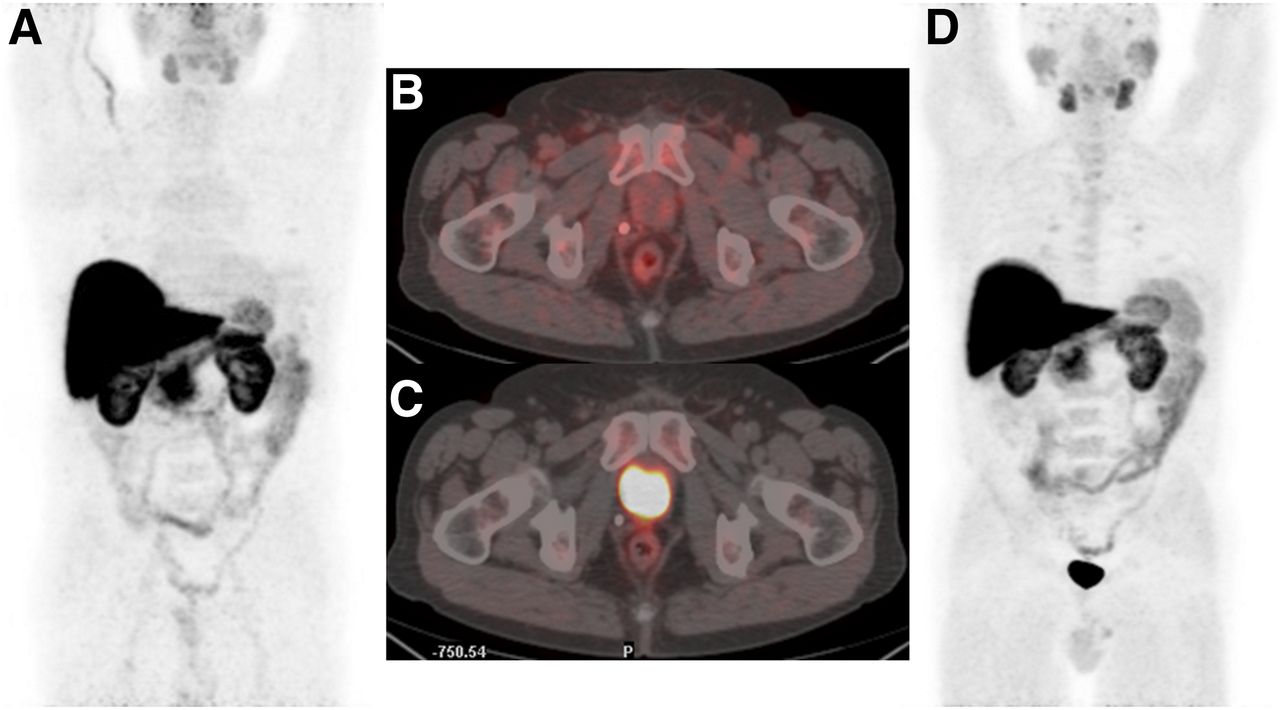
Physiologic uptake of 64CuCl2 differed from that of 18F-choline. 64CuCl showed high uptake in the liver and less intense uptake in the salivary glands, biliary tract, pancreas, spleen, and kidney. No significant 64CuCl uptake was found in the bone marrow. 64CuCl was not excreted via the urinary tract, and no accumulation in the bladder was found (Fig. 1).
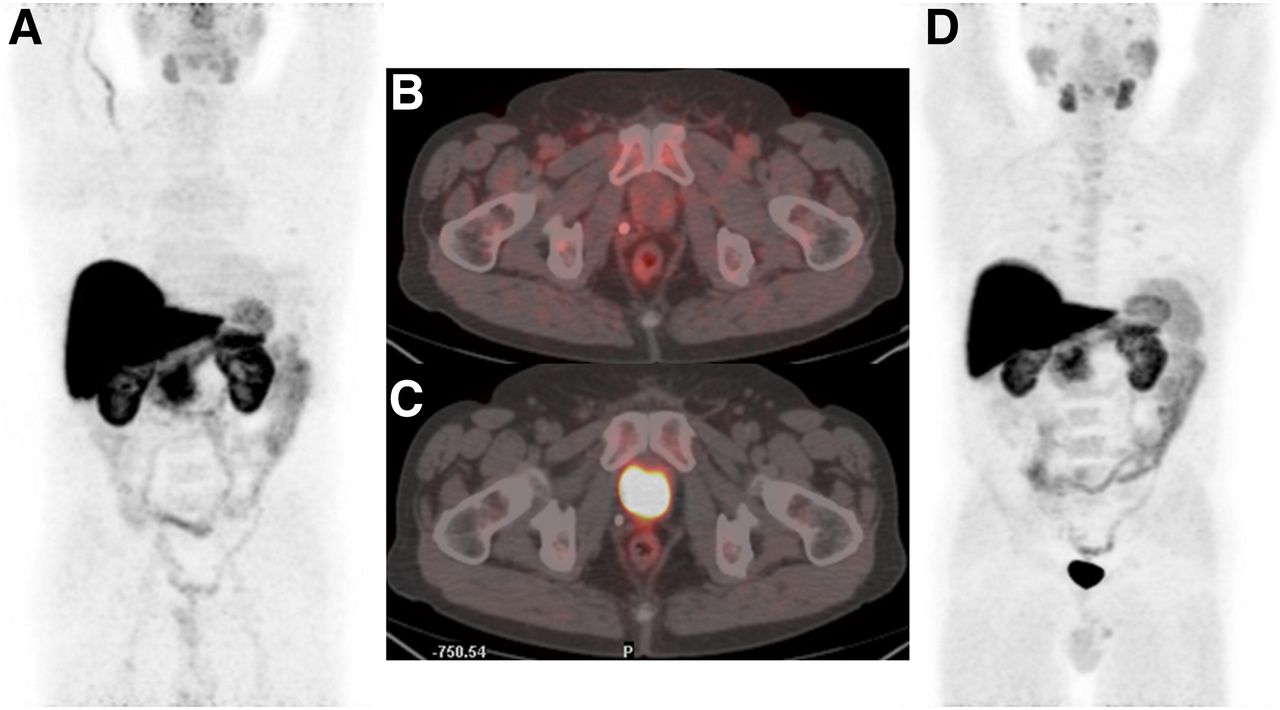
Maximum-intensity-projection images and PET/CT images of pelvis when 64CuCl2 (A and B) and 18F-choline (C and D) were used. Images were acquired 1 h and 20 min after 64CuCl2 and 18F-choline injection, respectively.
The critical organ for 64CuCl is the liver, as was already reported in ICRP 53 (29) and in a study by Capasso et al. (12). The liver accumulates about 30% of the administered activity, and the absorbed dose is 2.71E−1 mGy/MBq. Table 2 shows the absorbed dose per administered activity and comparison with 18F-choline and 68Ga-PSMA. Uptake in the liver, pancreas, and gallbladder maximizes about 1.5–2 h after administration, whereas the kidneys, spleen, and salivary glands have rapid uptake, maximizing in less than 1 h. Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org) shows typical time–activity curves (as percentages of the injected activity) for the various source organs. Radiation dosimetry revealed an effective dose of 2.83E−2 mSv/MBq.
Absorbed Organ Dose per Administered Activity: Comparison with 18F-Choline and 68Ga-PSMA (39)
Lesion Kinetics
As in the case of organs at risk, time–activity curves for lesions showed rapid uptake, maximizing about 1 h after administration (Supplemental Fig. 2). The study of the lesion time–activity curves revealed a slow clearance dictated by the radionuclide physical half-life (mean effective half-life, 9.5 h).
Patient-Based Analysis
PCa relapse was found in 44 patients. Local relapse was detected in 34 patients (68%). We identified lymph node metastases in 17 patients (34%) and bone metastases in 5 patients (10%).
Table 3 summarizes the differences in DR between 64CuCl2 PET/CT and each of the other 4 diagnostic modalities and shows the DRs recorded when different sites of PCa recurrence were considered separately. The difference between the DR of 64CuCl2 PET/CT and that of 18F-choline PET/CT was statistically significant (P = 0.002).
Patient-Based Analysis
When the level of PSA was considered (Fig. 2), 64CuCl2 PET/CT identified a higher number of positive patients than did 18F-choline PET/CT in every PSA level cohort, except for a PSA level of more than 4 ng/mL.

Patient-based analysis. Comparison of 64CuCl2 PET/CT vs.18F-choline PET/CT. DR was calculated for each PSA cohort.
When we considered the differences between the prostatectomy and nonprostatectomy populations, we found that 64CuCl2 PET/CT identified a higher number of positive patients than did 18F-choline PET/CT among those treated with surgery (P = 0.001). In particular, 64CuCl2 PET/CT identified a significantly higher number (P < 0.001) of local relapses (Supplemental Table 1).
A detailed description of the multidisciplinary standard of reference considered for each patient is provided in Supplemental Figure 3.
Lesion-Based Analysis
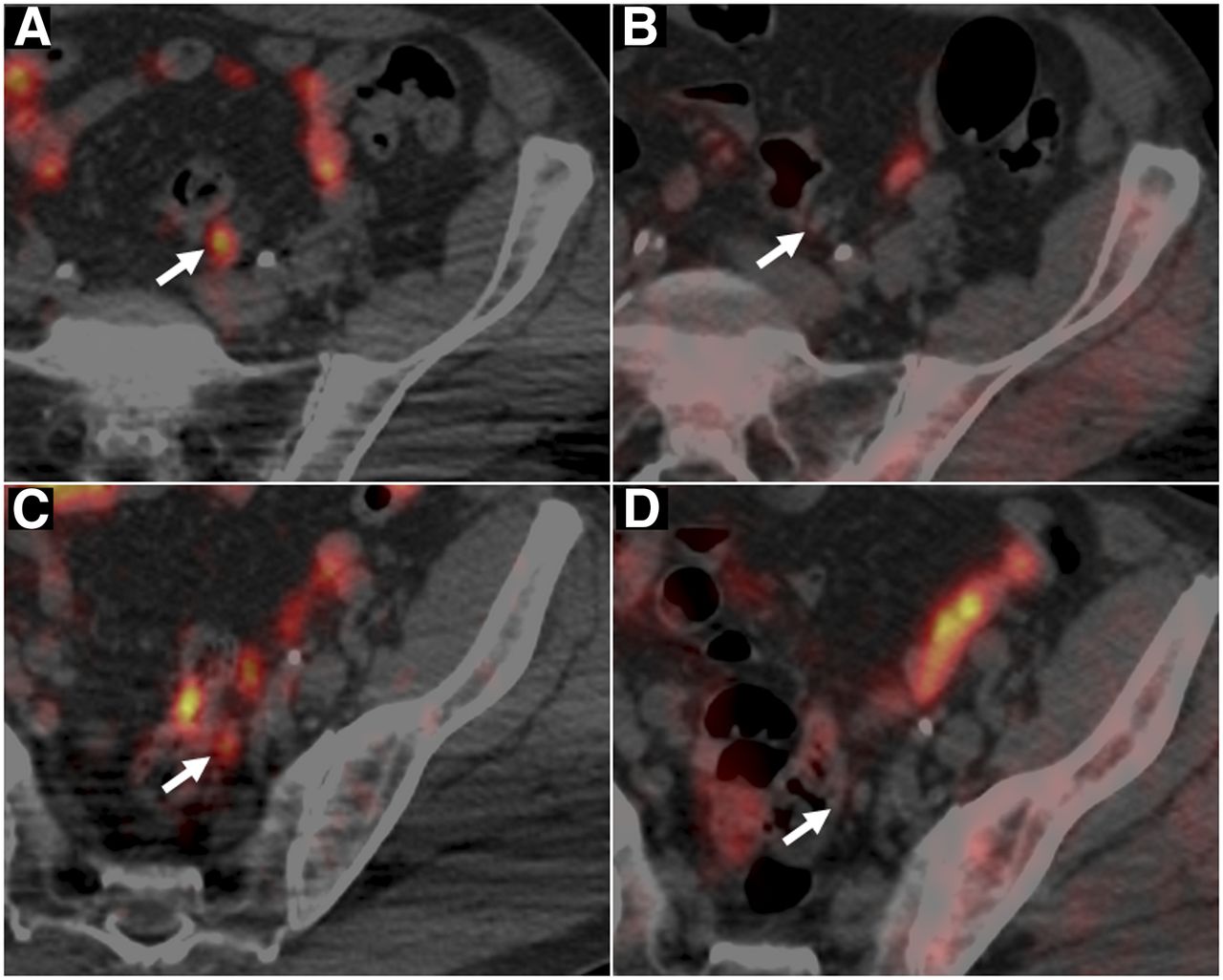
To determine the DR of each modality in detecting recurrent lesions in different anatomic locations, we also performed a lesion-based analysis; the results are summarized in Table 4. Overall, 118 lesions were detected in our analysis, 44 of which were local relapses, 60 abdominal lymph-node metastases, and 14 bone metastases (pelvis, proximal femurs, and lumbar spine). Indeed, 64CuCl2 PET/CT showed significantly higher DRs than did 18F-choline PET/CT and mpMRI (Table 4). The DR of 64CuCl2 PET/CT was particularly high in the case of local relapse. Two cases of local recurrence are illustrated in Figures 3 and 4. In addition, 64CuCl2 PET/CT identified a significantly higher number of lymph node metastases than did 18F-choline PET/CT and mpMRI. In particular, all lymph nodes with positive 64CuCl2 and negative 18F-choline findings had a short-axis diameter of less than 7 mm. Two cases are illustrated in Figures 5 and 6. In the event of bone metastases, mpMRI showed the highest DR. No difference in bone DR was observed between 18F-choline PET/CT and 64CuCl2 PET/CT (Fig. 7).
Lesion-Based Analysis
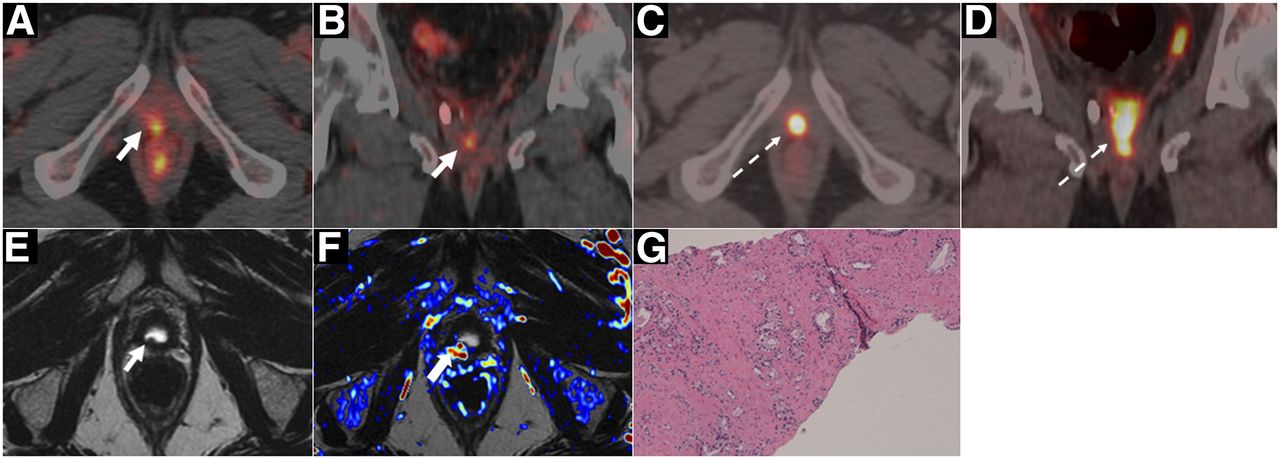
A 72-y-old man with Gleason 4 + 3 PCa treated with radical prostatectomy, with rising PSA level (1.0) and PSA doubling time of 11 mo. (A and B) 64CuCl2 PET/CT images (axial and coronal) reveals focal tracer uptake (arrow) in vesicourethral anastomosis. (C and D) In 18F-choline PET/CT images (axial and coronal), urinary tracer accumulation (dotted arrows) obscures walls of anastomosis. (E) T2-weighted mpMR image shows small hypointense nodular thickening (arrow) in anastomosis. (F) Wash-in perfusion map (derived from dynamic contrast-enhanced sequences) shows focal area of hypervascularization in correspondence to hypointense nodular thickening of anastomosis. (G) Local PCa relapse was histopathologically confirmed by transrectal ultrasound–guided biopsy (hematoxylin–eosin, ×10).
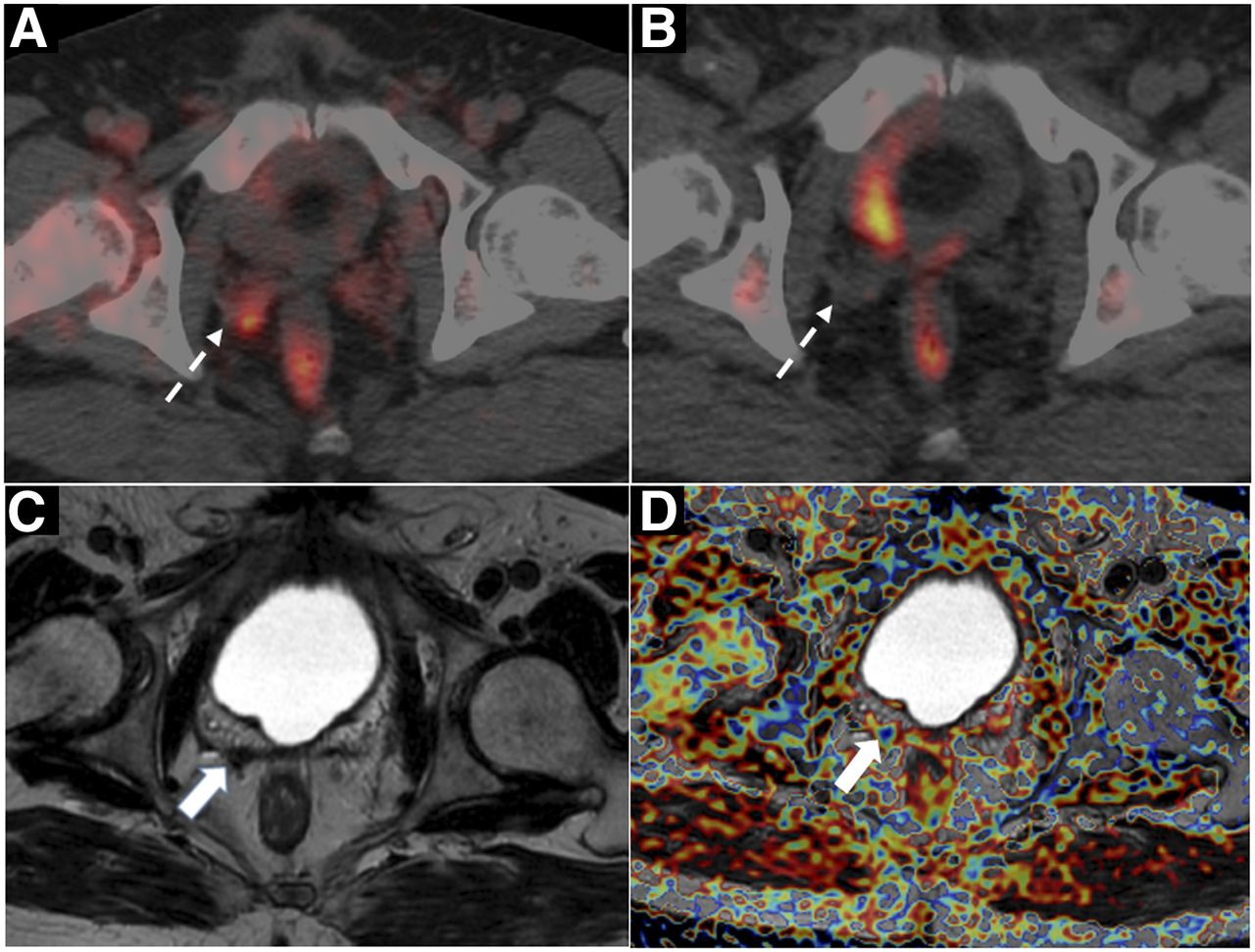
A 70-y-old man with Gleason 4 + 3 PCa treated with radical prostatectomy, with rising PSA level (1.34) and PSA doubling time of 5.3 mo. (A) 64CuCl2 PET/CT images reveals focal uptake (dotted arrow) in residual right seminal vesicle. (B) 18F-choline PET/CT is negative. (C) T2-weighted axial image mpMRI shows hypointense area in right seminal vesicle remnants. (D) Apparent-diffusion-coefficient map derived from diffusion-weighted imaging sequence shows focal area of signal restriction in correspondence to remnants of right seminal vesicle.

An 81-y-old man with Gleason 5 + 4 PCa treated with EBRT, with rising PSA level (1.09) and PSA doubling time of 4.9 mo. (A) 64CuCl2 PET/CT images reveal 2 positive small iliac lymph nodes. (B) 18F-choline PET/CT is negative (arrows). (C) Four months later (PSA value, 3.1), 18F-choline PET/CT reveals correspondence between positive uptake and 2 iliac lymph-nodes (arrows).

A 62-y-old man with Gleason 4 + 3 PCa treated with radical prostatectomy, with rising PSA level (1.32) and PSA doubling time of 3.7 mo. (A and C) 64CuCl2 PET/CT images reveal 2 positive small left iliac lymph nodes. (B and D) 18F-choline PET/CT is negative (arrows).
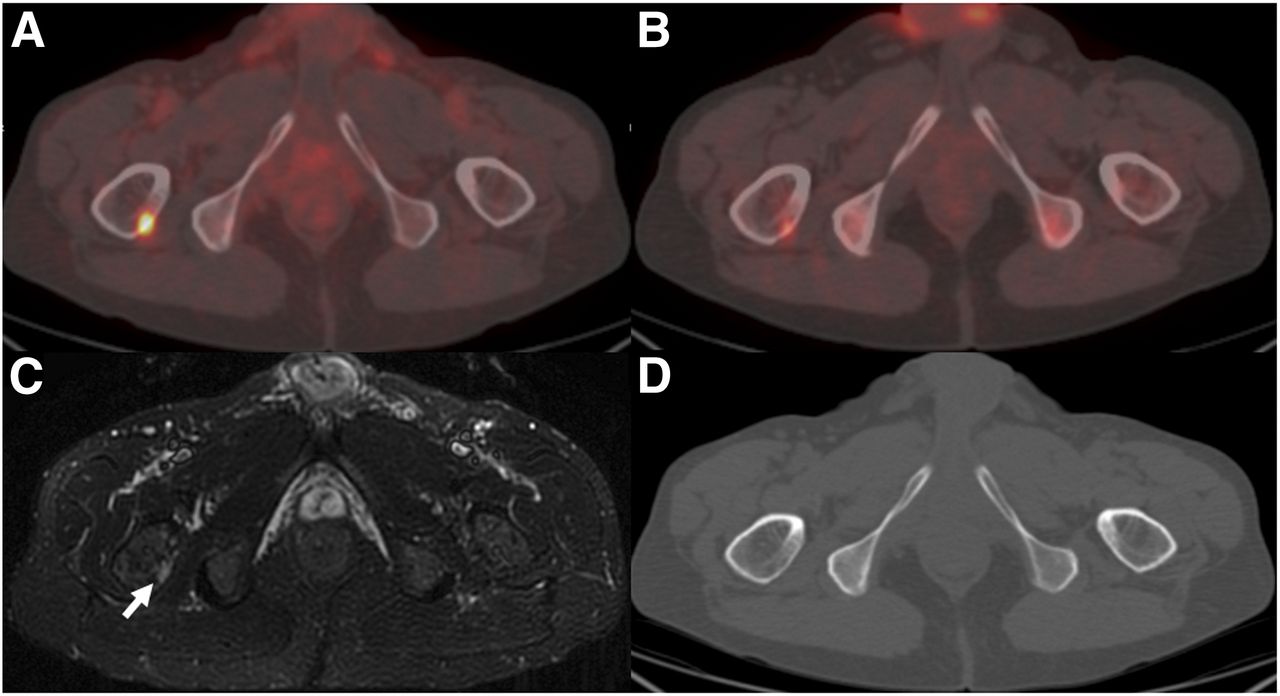
A 79-y-old man with Gleason 4 + 5 PCa treated with radical prostatectomy, with rising PSA level (1.89) and PSA doubling time of 2.1 mo. Both 64CuCl2 PET/CT and 18F-choline PET/CT images reveal intense, focal tracer uptake in proximal epiphysis of right femur. However, TBR was higher for 64CuCl2 PET/CT than for 18F-choline PET/CT (24.2 vs. 7.8). (C and C) Bone lesion (arrow) is evident on short T1 inversion recovery image (C) but is not appreciable in corresponding axial CT image (D).
All 18F-choline-positive PCa lesions (local, lymph nodes, and bone) showed 64CuCl2 uptake.
More generally, the 64CuCl2 TBR evaluated 1 h after tracer injection was higher than that of 18F-choline. The mean TBR was 13.4 for 18F-choline and 16.4 for 64CuCl2 (P = 0.02). The typical time–activity curves of 64CuCl2 for fat, marrow, and muscles compared with that of one site of disease is illustrated in Supplemental Figure 4.
DISCUSSION
Our study was the first to prospectively evaluate the biodistribution, dosimetry, and lesion kinetics of 64CuCl2 in a considerable number of PCa patients with biochemical relapse.
We found that the biodistribution of 64CuCl2 was more suitable than that of 18F-choline in evaluating PCa relapse, as 64CuCl2 is neither excreted nor accumulated in the urinary tract. This enables better assessment of the pelvis and prostatic fossa, thus increasing the possibility of identifying small lesions close to the bladder or vesicourethral anastomosis.
We found that the critical organ for 64CuCl2 was the liver, and we showed that the effective dose and liver exposure were lower than those calculated previously in only 7 patients (11% less and 8% less, respectively) (12). Our findings imply that potential hepatic radiotoxicity might be induced only by means of a high injected activity. We also found that the effective dose of 64CuCl2 was about 40% greater than that of 18F-choline (30). Thus, for an administered activity of 200 MBq, the effective dose of 64CuCl is 5.7 mSv, whereas that of 18F-choline is 4 mSv (30). However, this difference in radiation exposure can be considered negligible, especially in elderly patients with PCa biochemical relapse.
The time–activity curves of the PCa site of disease showed that 64CuCl2 has a rapid uptake that maximizes about 1 h after administration. This result supports the choice to perform PET imaging early after the injection. In addition, this analysis showed that the 64CuCl2 clearance in PCa relapse is slow and dictated by the radionuclide physical decay.
These data on dosimetry, biodistribution, and kinetics are potentially useful. Indeed, given its decay scheme (half-life, 12.7 h; β+, 17.86%; β−, 39.0%) (31), 64Cu could play a dual role in the development of molecular agents for PET imaging and in oncologic therapy (32). The additional emission of Auger electrons associated with the electron capture decay canal (electron capture, 43.075%) might considerably contribute to the possible therapeutic effectiveness of this radionuclide. Auger electrons have low kinetic energies and short-range penetration but concomitantly high linear-energy transfer (33), like heavier particles (34,35). The present study might provide the basis for evaluating the radiation safety of 64CuCl2 and estimating the dose absorbed by organs at risk in the case of theranostic application.
Our study demonstrated that 64CuCl2 PET/CT could detect local recurrence and lymph node and bone metastases in PCa patients with biochemical relapse and was the first to prospectively compare the diagnostic performance of 64CuCl2 PET/CT with those of 18F-choline PET/CT and mpMRI.
In our patient-based analysis, the DR of 64CuCl2 PET/CT was significantly higher than that of 18F-choline PET/CT. This difference stems from the high DR of 64CuCl2 PET/CT in identifying local recurrence, which is often undetected by 18F-choline PET/CT. In this analysis, no difference emerged between 64CuCl2 PET/CT and mpMRI. This is in line with the well-known high sensitivity of mpMRI in detecting local recurrence (36).
Indeed, 64CuCl2 PET/CT detected more patients with PCa relapse than did 18F-choline PET/CT in each PSA cohort, except for a PSA level of more than 4 ng/mL. These data demonstrate the high DR of 64CuCl2 PET/CT even in patients with a PSA level of less than 1 ng/mL. In this subgroup, more than 70% of patients presented a positive 64CuCl2 PET/CT, which was often consistent with local relapse. In other words, these patients may still benefit from salvage, PET-guided RT (37).
In the lesion-based analysis, 64CuCl2 PET/CT had a significantly higher DR than did 18F-choline PET/CT and mpMRI. We found that the significant difference in DR was due to the greater ability of 64CuCl2 PET/CT to detect both local recurrence and lymph node metastases (especially in small lymph nodes; i.e., those with a short axis diameter of <7 mm).
These findings open a door to the possibility of using 64CuCl2 PET/CT in cases of suspected local PCa relapse when mpMRI remains inconclusive.
Despite our encouraging results, some important limitations should be noted. First, we assessed only the DRs of the diagnostic techniques mentioned, assuming a priori that all patients were true-positives, in that they presented with biochemical relapse. Indeed, we introduced a descriptive standard of reference, which was used only to confirm the sites of disease without providing information on the diagnostic accuracy of 64CuCl2 PET/CT. Second, only a few cases of local findings were confirmed histopathologically. Histopathology was performed on transrectal ultrasound–guided biopsy in 7 of 25 patients (28%) showing only local recurrence; this confirmed the presence of disease. In addition, undetectable PSA values were found after salvage EBRT in another 4 of the 11 patients with only local recurrence and not previously treated with EBRT. Generally, we found a high concordance between positive findings on 64CuCl2 PET/CT, 18F-choline PET/CT, and mpMRI.
However, the lack of proper histopathologic confirmation is common in most articles (16–19,38) comparing different PET tracers in the detection of PCa recurrence. Indeed, the aim of these studies, as in our case, was not to determine the diagnostic accuracy but to assess and compare the DRs of the tracers.
CONCLUSION
The biodistribution of 64CuCl2 is more suitable than that of 18F-choline for exploring the pelvis and prostatic bed. The 64CuCl2 effective dose is similar to those of other established PET tracers. In patients with biochemical relapse and a low PSA level, 64CuCl2 PET/CT shows a significantly higher DR than does 18F-choline PET/CT. Larger trials with this PET tracer are expected to further define its capabilities and role in the management of PCa.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Sep. 8, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 11, 2017.
- Accepted for publication July 25, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Role of 64CuCl2 PET/CT in Detecting and Staging Muscle-Invasive Bladder Cancer: Comparison with Contrast-Enhanced CT and 18F-FDG PET/CT
- Development of Novel PSMA Ligands for Imaging and Therapy with Copper Isotopes
- The War Is Opened: PSMA vs. 64CUCL2 vs. Choline PET/CT
- Insights into Trace Metal Metabolism in Health and Disease from PET: "PET Metallomics"
- A New Type of Prostate Cancer Imaging: Will 64CuCl2 PET/CT Flourish or Vanish?