


Abstract
The main objective of this prospective study was to determine the impact of multiphasic acquisition of 68Ga-PSMA PET/CT in the detection of recurrent prostate cancer in the early stage of biochemical recurrence with a prostate-specific antigen (PSA) level of less than 1 ng/mL. Also, 68Ga-PSMA PET/CT positivity was correlated with clinical parameters for the assessment of predictive markers. Methods: A prospective monocentric study was conducted on 135 prostate cancer patients with biochemical recurrence and a PSA level of less than 1 ng/mL. All patients had undergone initial prostatectomy, with additional radiation therapy in 19.3% of patients and androgen-deprivation therapy in 7.4%. The patients underwent dynamic acquisitions from the prostate bed (1–8 min after injection), standard whole-body acquisitions (60 min after injection), and limited-bed-position delayed acquisitions (120–150 min after injection). The studies were reviewed by 2 board-certified nuclear medicine specialists, independently. A combination of visual and semiquantitative analyses and correlation with morphologic (e.g., MRI) or clinical follow-up findings was used for the final interpretation of lesions as benign or malignant. 68Ga-prostate-specific membrane antigen (PSMA) PET/CT positivity was also correlated with primary clinical findings. Results: Incorporating the information from all phases, we were able to detect 116 lesions in 49.6% of patients (22 local recurrences, 63 lymph nodes, and 31 distant metastases). The detection rates were 31.8%, 44.9%, and 71.4% for PSA < 0.2 ng/mL, 0.2 ≤ PSA < 0.5, and 0.5 ≤ PSA < 1, respectively. Additional dynamic or delayed phases resulted in better determination of equivocal lesions and a higher diagnostic performance in 25.9% of patients. Stand-alone dynamic and delayed images led to better interpretation of equivocal findings in the prostate bed (31.4%) and in other lesions (lymph node or bone) (20%), respectively. Conclusion: 68Ga-PSMA PET/CT showed promise for early detection of recurrent disease in patients with a PSA level of 0.5–1.0 ng/mL. However, it showed limited value in patients with a PSA level of less than 0.5 ng/mL. Multiphasic 68Ga-PSMA PET/CT led to a better determination of equivocal findings. Although dynamic images may provide helpful information for assessment of the prostate bed, delayed acquisitions seem to have a greater impact in clarifying equivocal findings.
Prostate cancer (PCa) is the second most common cancer worldwide, responsible for 6.7% of cancer-related mortality among men (1). Biochemical recurrence (BR) after initial treatment is a common phenomenon (2), reported in 20%–30% of patients after radical prostatectomy and in up to 60% after external-radiation therapy (3). Therefore, early detection of recurrent disease may provide a chance for salvage therapy and improve prognosis (3,4). The 5-y survival drops to 30% in patients with distant metastases, indicating the importance of discriminating among locoregional, oligometastatic, and distant spread of the disease (5).
Several clinical parameters and imaging techniques are used to diagnose recurrent disease, among these, prostate-specific antigen (PSA) is of particular relevance (6). The impact of molecular imaging using PET/CT in the detection of recurrent PCa disease seems stronger with the advent of specific PET tracers. However, detection of early recurrence in patients with a low PSA level (e.g., <1.0 ng/mL) remains challenging (4,7,8).
Prostate-specific membrane antigen (PSMA) is particularly expressed in prostatic cells and is one of the main targets for depicting cancerous tissues (9,10). Various PSMA radioligands are used in PET imaging, such as 68Ga-PSMA-11, 68Ga-PSMA I&T, and 18F-PSMA-1007 (11,12). These agents demonstrate different characteristics. Longer half-life, better physical spatial resolution, and lower urinary excretion are the prominent advantages of, for example, 18F-PSMA-1007 over 68Ga-labeled PSMA. In the assessment of pelvic lesions, the low urinary activity of 18F-labeled PSMA may overcome the limitation of 68Ga-ligand PSMA due to high tracer accumulation in the urinary bladder (12,13).
Despite the advantages of 68Ga-PSMA PET/CT as one of the most commonly used radiotracers in the assessment of BR, it showed limited value in patients with a PSA level of less than 1.0 ng/mL (8,14–16). This limitation may be related to urinary excretion and the intense activity in the bladder, which may obscure small locoregional lesions. Multiple studies using early images have tried to overcome the impact of intense physiologic activity in the bladder (17,18). Early or delayed imaging has revealed an additive value in improving the detection rate (11,18,19).
In this prospective study, we evaluated the impact of early dynamic and delayed images on the diagnostic performance of 68Ga-PSMA PET/CT in early assessment of BR in PCa patients with a PSA level of less than 1.0 ng/mL. Also, we correlated relevant predictive clinical factors with scan results to study when 68Ga-PSMA PET/CT would be of maximal benefit.
MATERIALS AND METHODS
Patients
This prospective single-center study was performed in accordance with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable standards and was approved by the institutional review board (trial EKS 10/19/EC-2017-005078-20) to be performed in the course of the clinical diagnostic workup of PCa patients. Written informed consent was obtained from all participants.
We included 135 consecutive PCa patients (mean age ± SD, 66.8 ± 8.0 y) with evidence of early BR and a PSA level of less than 1.0 ng/mL (Table 1). All were referred to the PET/CT Center of St. Vincent’s Hospital, Linz, Austria, from July 2017 to February 2019. In 19.3% (26/135) and 7.4% (10/135) of the patients, radiation therapy and androgen-deprivation therapy (ADT), respectively, had been performed after recurrence. The interval between primary treatment and the 68Ga-PSMA PET/CT studies was 2–266 mo (median, 42 mo).
Patient Data
Radiotracer Preparation
68Ga-PSMA-11 was prepared using a lyophilized sterile cold kit (ANMI SA) and a commercial 68Ge/68Ga generator made using good manufacturing practices. The feasibility of this preparation method in clinical practice was demonstrated in our previous study (15).
PET/CT Acquisition and Image Reconstruction
The study was performed using a dedicated PET/CT scanner (Discovery 710; GE Healthcare) with an extended–field-of-view (FOV), full-ring, high-resolution lutetium oxyorthosilicate PET component and a 128-slice spiral CT component. Images were acquired at 2 time points (in all patients) or 3 time points (in 97 patients) after a bolus injection of 68Ga-PSMA-11 (2 MBq/kg of body weight). Early dynamic images started at the first minute after injection. The acquisition field was targeted on the prostatic bed (15.6-cm axial FOV). The early dynamic phase was continued for 8 min, at 60 s/frame, with low-dose CT. Standard whole-body images were acquired for 2.5 min/bed position, starting 60 min after injection, from the skull base to the proximal thigh, alongside diagnostic contrast-enhanced CT. Finally, the delayed images were obtained—at a minimum of 2 bed positions—covering the pelvic and lower abdominal regions, as well as the upper abdominal or thoracic regions in some patients, at 120–150 min after injection, accompanied by low-dose CT.
In 38 (28%) patients, the delayed examination was not performed because of clear PET findings in the pelvis or lack of patient compliance with continuing the examination. Moreover, those studies that were not obtained during the scheduled time frame were excluded from the study.
In cases of equivocal or unclear findings in the other parts of the body, additional images were obtained for further clarification. Images were reconstructed identically using ordered-subsets expectation maximization (4 iterations, 18 subsets) followed by a postreconstruction smoothing gaussian filter (4.0 mm in full width at half maximum). In all patients, a contrast-enhanced CT scan with a high-beam tube-current modulation was obtained (120–330 mA, 0.6 s/rotation, 5.0-mm reconstructed section thickness, 0.5-mm overlap, 512 × 512 matrix, pitch index of 1.5).
Image Interpretation
An independent, consecutive masked reading of each examination phase was performed by 2 experienced board-certified nuclear medicine specialists who were aware only of the clinical information (e.g., the PSA value). In cases of equivocal findings or discrepancies between the 2 readers, the final interpretation was decided in a consensus meeting. Finally, a combination of visual and semiquantitative analyses and correlation with morphologic (e.g., MRI) or clinical follow-up findings was used for ultimate classification of the abnormalities as benign or malignant.
Every frame of the dynamic-phase images was examined separately. Advanced PET/CT software (AW-4.6; GE Healthcare) was used for reading. Respecting the substantially high specificity of 68Ga-PSMA (2), we speculated that every clearly abnormal focus of tracer uptake that could not be explained by physiologic 68Ga-PSMA activity was positive for tumoral involvement. The final interpretation was based on the findings for all 3 acquisition phases. A finding was considered equivocal when the presence of urinary activity was suspected in a typical anatomic location or when a lesion with an abnormal tracer accumulation showed mild intensity but had no definite morphologic findings, especially in the prostate bed or iliac region. The findings on dynamic or delayed acquisition were used to better classify such lesions as benign or malignant. With consideration of the anatomic location, lesions were categorized into 4 groups: local recurrence in the prostate bed, pelvic lymph nodes (internal, external, common iliac, or presacral regions), bone metastases, and visceral metastases.
SUVmax was calculated by drawing a volume of interest over suggestive areas in each phase. The SUVmax of the lesions in the dynamic phase was evaluated at the fourth minute of the study. This timing was chosen because of our previous experience and because lesions were visualized on dynamic images at a mean of 2.9 ± 1.9 min (median, 3.0 min) and urinary activity appeared at a mean of 6.1 ± 1.2 min (median, 6.0 min). To maintain unity, those lesions not visualized up to the fourth minute were excluded from the semiquantitative analysis.
Furthermore, background tracer uptake in soft tissue was evaluated by drawing a standard reference volume of interest on the right gluteus muscle, sparing intramuscular vessels, in each phase.
Statistical Analysis
Numeric data are presented as median or mean ± SD. Statistical analysis was conducted with dedicated software (SPSS 23.0; IBM). The relationship between PET/CT positivity and clinical parameters was evaluated. Data that showed a normal distribution on Kolmogorov–Smirnov testing were analyzed using the independent t test with 95% confidence intervals. Data that did not show a normal distribution, such as initial PSA and current PSA, were compared using a nonparametric Mann–Whitney test. The history of radiation therapy and ADT was compared using the χ2 test. Numbers of lesions and their SUV were compared using the Wilcoxon test. A P value of less than 0.05 was considered significant.
RESULTS
Patient-Based Analysis
The patients were categorized into 3 groups based on PSA level on the day of examination (trigger PSA): PSA < 0.2 ng/mL (16.3%; 22/135), 0.2 ≤ PSA < 0.5 (57.8%; 78/135), and 0.5 ≤ PSA < 1 (25.9%; 35/135). Considering the results of all 3 phases, at least 1 pathologic lesion was detected in 49.6% (67/135) of patients.
The dynamic, standard whole-body, and delayed images were positive in 27.4% (37/135), 48.1% (65/135), and 43.3% (42/97) of the patients, respectively.
68Ga-PSMA PET/CT showed a detection rate of 31.8%, 44.9%, and 71.4% in patients with PSA < 0.2 ng/mL, 0.2 ≤ PSA < 0.5, and 0.5 ≤ PSA < 1, respectively (Table 2).
Detection Rates by PSA Category
There was a significant correlation between 68Ga-PSMA PET/CT positivity and trigger-PSA level (P < 0.001), even after evaluation of each phase separately (P < 0.003). Moreover, considering the final interpretation, the history of ADT was found to be a predictive factor for positive scans (P = 0.008). However, no significant correlation was observed between 68Ga-PSMA PET/CT positivity and primary clinical parameters such as initial PSA, Gleason score, disease grade, T stage, surgical margin, the history of radiation therapy, and the interval from initial treatment.
Given the fact that the FOV of standard whole-body scans provides a general overview of the examined structures compared with the limited views of dynamic and delayed images, only the similar FOV of the pelvic region was considered in correlation analyses between different phases. Therefore, only 81 studies were relevant for the comparative analysis. The overall detection rates in the same FOV were 28.4%, 39.8%, and 35.5% for dynamic, standard whole-body, and delayed-phase imaging, respectively. Standard whole-body images showed significant superiority to only the dynamic-phase images (P = 0.012).
Lesion-Based Analysis
In total, 25, 42, and 39 tumoral lesions were detected in the identical FOV in the pelvic area on the dynamic, standard whole-body, and delayed images, respectively (Table 3). There was a significantly higher detection rate for lymph nodes on standard whole-body images than on dynamic-phase images (P = 0.004). However, no superiority was seen in the depiction of local recurrences (P = 0.37). Additionally, standard whole-body and delayed images performed similarly in revealing suggestive lesions in the same FOV, regarding both local recurrences and lymph node metastases (P = 0.37). There were only a few bone and visceral metastases in the pelvic area from which to draw a clinical statement (Table 3).
Numbers of Detected Lesions on Each Phase and in Same FOV
Semiquantitative analysis by means of SUVmax showed a significant increasing pattern from dynamic to standard whole-body acquisition in lymph nodes (P = 0.006), whereas there was no significant change in SUVmax in local recurrent lesions or between standard whole-body and delayed images (P = 0.50) (Table 4).
SUVmax of Detected Lesions in Same FOV Regarding All 3 Phases
The SUVmax of detected lymph nodes was lower in subcentimetric lesions on standard whole-body (P = 0.023) and delayed (P = 0.005) images. However, there was no significant difference in the SUVmax of local recurrent lesions between subcentimetric and larger lesions (Table 4).
Impact of Multiphasic Scanning
In 25.9% (35/135) of patients, equivocal findings or discrepancies were observed in at least 1 lesion between the different phases of scanning. To confidently differentiate positive from negative results, we defined a general interpretation, according to the study protocol, that considered all phases and looked for the possibility that more information was provided by dynamic and delayed images. We encountered 2 patients (1.5%) with negative standard whole-body studies in whom obvious positive lesions were present, one on dynamic images and the other on delayed images (Figs. 1 and 2). Nevertheless, in the remainder of the patients, the impact of the additional studies stemmed mainly from clarification of equivocal findings.

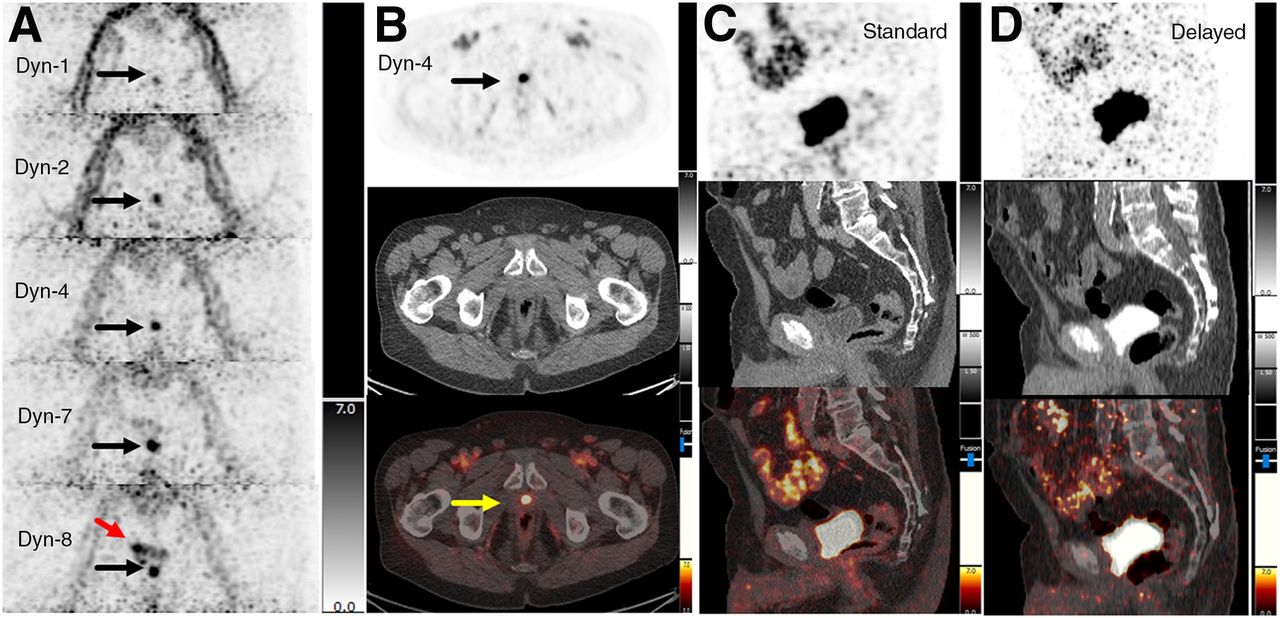
Impact of dynamic 68Ga-PSMA PET/CT on PCa patient with BR (PSA, 0.50 ng/mL). (A) Dynamic phase: focal tracer uptake (black arrows) is perceived in prostate bed from first minute. Urinary activity in bladder (red arrow) is visible from seventh minute. (B) Dynamic phase, axial view (PET at top, CT in middle, and PET/CT at bottom), from fourth minute shows focal uptake in prostate bed (arrows) suggestive of local recurrence. (C and D) Standard and delayed acquisitions: suggestive focal uptake in prostate bed is completely masked by physiologic urinary activity in bladder.

Impact of delayed 68Ga-PSMA PET/CT on PCa patient with BR (PSA, 0.34 ng/mL). Standard whole-body maximum-intensity projection (MIP) (A); dynamic acquisition, axial view, at fourth minute (PET at top, CT in middle, and PET/CT at bottom) (B); and standard acquisition, axial view (C), show no abnormal tracer uptake in pelvic lymph nodes (A–C, arrows). (D) Delayed phase: focal tracer uptake is seen on small external iliac lymph node (black and yellow arrows). Urinary uptake is seen in both ureters (red arrows).
Additional images (i.e., dynamic, delayed, or both) provided more data for better delineation of the equivocal findings, resulting in a final interpretation of positive in 13.3% (18/135) of the patients and negative in 12.6% (17/135) (Table 5; Fig. 3). In these patients, stand-alone dynamic images were informative in 31.4%, stand-alone delayed images were informative in 20.0%, either dynamic or delayed images were informative in 37.1%, and both dynamic and delayed images were informative in 11.5%. Overall, additional delayed scans were more helpful than the other types of scans in determining the status of equivocal lesions.
Additional Data Provided by Dynamic or Delayed Images

Impact of dynamic and delayed 68Ga-PSMA PET/CT on PCa patient with BR (PSA, 0.28 ng/mL). Standard whole-body maximum-intensity projection (MIP) (A) and dynamic acquisition, axial view, at fourth minute (PET at top, CT in middle, and PET/CT at bottom) (C) show abnormal tracer accumulation in prostate bed, suggestive of local recurrence (arrows). (B) Dynamic phase: no abnormal activity is seen in prostate bed (arrow). (D) Delayed phase: contrast medium (white arrow) is present in suggestive region visualized on standard image concomitant with urinary activity in bladder.
DISCUSSION
The current prospective study had 3 main goals: determining the impact of 68Ga-PSMA PET/CT in recurrent PCa, determining the value of early dynamic and delayed studies on the diagnostic performance of 68Ga-PSMA PET/CT compared with standard whole-body imaging, and determining the correlation between clinical parameters (e.g., initial PSA and Gleason score) and 68Ga-PSMA PET positivity in BR.
68Ga-PSMA PET/CT has shown promising results in the assessment of PCa recurrence (14,15,20). Although previous studies reported a close correlation between PSA values and 68Ga-PSMA PET/CT positivity, the diagnostic accuracy of 68Ga-PSMA PET/CT in patients with low PSA levels has been controversial (2,19,21). In an early study, Eiber et al. retrospectively examined the value of 68Ga-PSMA PET/CT in 248 PCa patients with BR and found sensitivities of 57.9% and 72.7% for PSA levels of 0.2 to less than 0.5 ng/mL and PSA levels of 0.5 to less than 1 ng/mL, respectively (21). In a study with a large patient population, Afshar-Oromieh et al. reported an overall detection rate of 79.5% in 1,007 PCa patients with BR and a median PSA level of 2.2 ng/mL, along with sensitivities of 46%, 46%, and 73% for PSA levels of 0.2 ng/mL or less, 0.21–0.5 ng/mL, and 0.51–1.0 ng/mL, respectively (2). The findings of our study were consistent with previous retrospective reports showing detection rates of 31.8%, 44.9%, and 71.4% for PSA < 0.2 ng/mL, 0.2 ≤ PSA < 0.5, and 0.5 ≤ PSA < 1, respectively. Furthermore, distant metastases were detected in 3% of patients even with very low PSA levels (≤0.5 ng/mL)—a finding that was of great clinical relevance for therapeutic decision making.
The impact of early dynamic and multiple–time-point 68Ga-PSMA PET/CT acquisitions has been investigated in previous studies (15,19,22). Uprimny et al. reported a detection rate of 62.1% for 68Ga-PSMA PET/CT in 203 recurrent-PCa patients with a median PSA level of 1.44 ng/mL (19). However, only 20.2% of patients had a PSA level of less than 0.5 ng/mL. Additionally, the dynamic imaging was started about 5 min after tracer injection. Low number of patients with a PSA level of less than 1.0 ng/mL and performing the dynamic imaging 5 min after injection may cause a bias in the results of this study. On the basis of our experience, renal excretion of 68Ga-PSMA is usually seen 4–6 min after tracer injection; thus, performing the dynamic acquisition after 5 min may affect the interpretation of the pelvic lesions. Furthermore, it has been reported that tumoral lesions are commonly visualized in the first 3 min of the study, when no urinary activity is present in the bladder (18,19). However, in our study, some lesions (6 small recurrent lesions and 7 lymph nodes) were detected after the third minute. This result was due mainly to the considerable presence of the tracer in iliac vessels in initial frames, obscuring the adjacent lymph nodes.
In the current study, dynamic imaging performed better in detecting local recurrence, as was consistent with the findings of other reports (18). Additional dynamic and delayed images led to better classification of lesions in 26% of patients with indeterminate or negative findings on standard whole-body scans. These additional acquisitions changed equivocal findings into final interpretations that were positive for PCa in 13.3% of patients and negative in 12.6% (Table 5). In a considerable number of patients with low PSA levels, the standard whole-body phase alone seems unsatisfactory for making an accurate interpretation.
Furthermore, 3 local recurrent lesions and 1 lymph node observed on dynamic or standard whole-body images were not visible on delayed images, when considering the same FOV. The considerably small size of lesions and lower tumor-to-background ratio may explain this observation. The rapid-washout phenomenon can be another reason for falsely negative findings on delayed images in certain patients. Slow internalization in some tumor cells and a moderate affinity to PSMA may lead to a rapid washout of activity from tumors (23).
The correlation between clinical parameters (e.g., trigger PSA and ADT) and 68Ga-PSMA PET/CT positivity in recurrent-PCa patients has been a controversial topic, with most investigators finding a correlation with a shorter PSA doubling time (2,9,21). Our results were compatible with previous reports showing higher detection rates corresponding to trigger PSA, which seems to be an invariable factor (2,24). However, our data additionally showed a correlation between 68Ga-PSMA PET/CT positivity and a history of receiving ADT (at any time point). This finding may be related to the primary stage of disease, as administrating ADT after prostatectomy may imply more advanced disease that may cause higher rates of recurrence. Nevertheless, we found no correlation between Gleason score and positive PET/CT results.
The main limitation of our study was the lack of histopathologic verification. This limitation was due mainly to the small size of the lesions and the challenge of accessing them. Moreover, when a consensus existed among the scan results, the anatomic imaging results (e.g., MRI), and the clinical results, obtaining a biopsy was not ethical. Furthermore, the small size of the common FOV in the various phases of PET/CT acquisition limited the number of analyzed lesions available for an accurate comparative assessment. The various FOVs in the different phases (e.g., 1 bed position in dynamic acquisitions vs. 2 or more on delayed or whole-body acquisitions) may cause a bias in the results of this study. In addition, the cost effectiveness of 68Ga-PSMA PET/CT in patients with a low PSA value (i.e., < 1 ng/mL) and the impact of 68Ga-PSMA PET/CT on patient management is an important issue, which should be evaluated in future studies. In our opinion, there is also an unmet need to optimize the imaging protocols for 68Ga-PSMA PET/CT in order to improve its diagnostic performance in individual patients (e.g., those with early recurrence and a low PSA value) who are being considered for salvage treatment.
Finally, the small number of patients who had a history of receiving ADT limits the statistical power of our results for this group. Studies with larger numbers of patients are needed to further evaluate the correlations between 68Ga-PSMA PET/CT positivity and a history of receiving ADT.
CONCLUSION
Multiphasic imaging, by clarifying equivocal findings, seems to improve the diagnostic performance of 68Ga-PSMA PET/CT in PCa patients with early BR and a low PSA level (i.e., <1.0 ng/mL), for whom early detection of recurrent disease provides a better chance for salvage therapy and a better prognosis. Furthermore, trigger PSA and a history of ADT seem to be predictive of 68Ga-PSMA PET/CT positivity.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does multiphasic acquisition improve the diagnostic performance of 68Ga-PSMA PET/CT in PCa patients with a PSA level of less than 1 ng/mL?
PERTINENT FINDINGS: In this prospective study assessing the impact of multiphasic acquisition on the diagnostic performance of 68Ga-PSMA PET/CT in 135 PCa patients with BR and a PSA level of less than 1 ng/mL, the detection rates were 31.8%, 44.9%, and 71.4% for PSA < 0.2 ng/mL, 0.2 ≤ PSA < 0.5, and 0.5 ≤ PSA < 1, respectively. Reviewing the findings in all phases resulted in a better determination for equivocal lesions, leading to higher diagnostic performance in 25.9% of patients.
IMPLICATIONS FOR PATIENT CARE: Multiphasic imaging seems to improve the diagnostic performance of 68Ga-PSMA PET/CT in patients with early BR and low levels of PSA (i.e., <1.0 ng/mL), for whom early detection of recurrent disease provides a better chance for salvage therapy and a better prognosis.
Footnotes
Published online Feb. 14, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 11, 2019.
- Accepted for publication February 6, 2020.





{kind=link}
{kind=link}
{kind=link}