


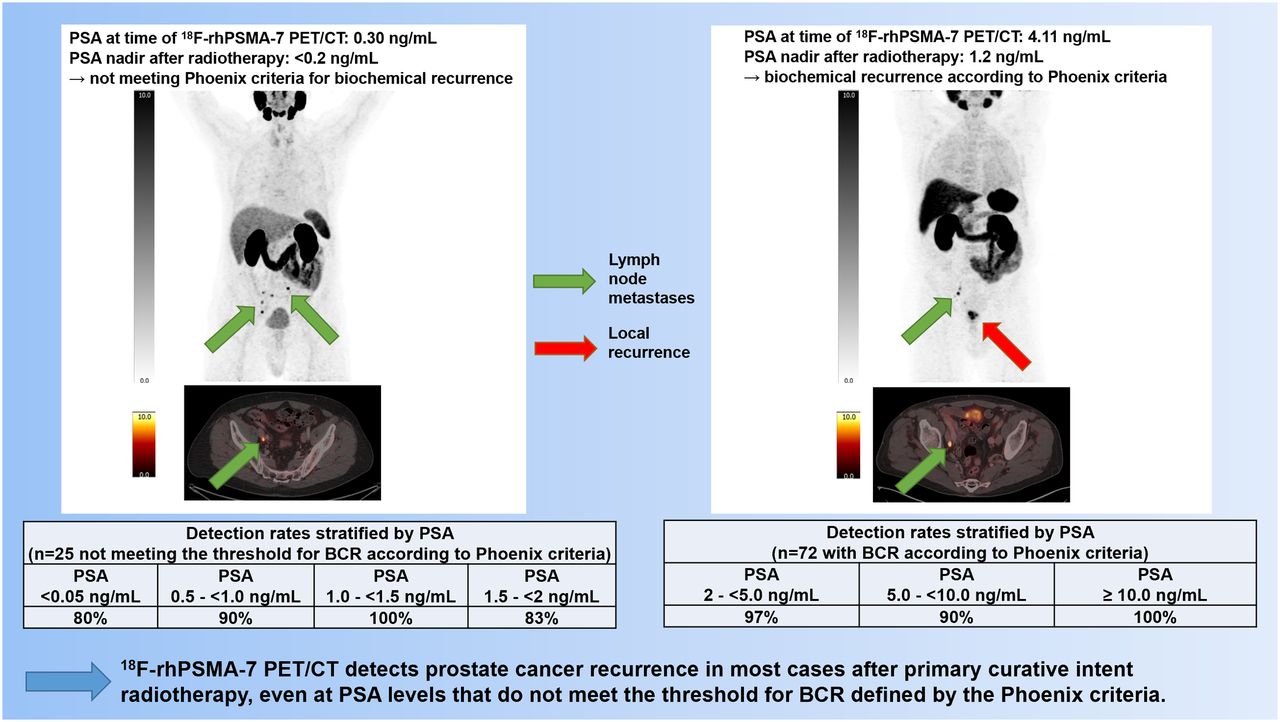
Visual Abstract

Abstract
This bicentric, retrospective analysis investigated the efficacy of PET/CT with a novel theranostic prostate-specific membrane antigen (PSMA)--targeting ligand, 18F-rhPSMA-7, in patients with biochemical recurrence (BCR) of prostate cancer after curative-intent primary radiotherapy. Methods: Datasets from patients with BCR of prostate cancer after external-beam radiation therapy or brachytherapy who underwent 18F-rhPSMA-7 PET/CT at either Technical University Munich or Ludwig-Maximilians-University Munich were retrospectively reviewed by experienced nuclear medicine physicians and radiologists at both centers. The median injected activity was 299 MBq (range, 204–420 MBq), and the median uptake time was 77 min (range, 46–120 min). All lesions suggestive of recurrent prostate cancer were noted. Detection rates were correlated with patients’ prostate-specific antigen (PSA) level, primary Gleason score, and prior use of androgen-deprivation therapy (ADT). Results: Ninety-seven patients were included (65 at Technical University Munich and 32 at Ludwig-Maximilians-University Munich). The median prescan PSA was 4.19 ng/mL (range, 0.1–159 ng/mL). The primary Gleason score was ≤6 in 19 patients, 7 in 25, ≥8 in 33, and unknown in 20. Thirty patients received ADT in the 6 mo preceding PET/CT. 18F-rhPSMA-7 identified lesions in 91 of 97 (94%) patients. Detection rates stratified by PSA were 88% (22/25), 97% (30/31), 90% (19/21), and 100% (20/20) for a PSA of <2, 2–<5, 5–<10, and ≥10 ng/mL, respectively. Detection rates in the subgroup of patients not meeting the Phoenix criteria for BCR were 80% (4/5), 90% (9/10), 100% (4/4), and 83% (5/6) for a PSA of <0.5, 0.5–<1, 1–<1.5, and 1.5–2 ng/mL, respectively. There were no significant differences in detection rates between patients with and without prior ADT (100% vs. 91%, P = 0.173) or patients with a Gleason score of ≤7 and a Gleason score of ≥8 (98% vs. 91%, P = 0.316).18F-rhPSMA-7 revealed local recurrence in 80% (78/97); pelvic lymph node metastases in 38% (37/97); retroperitoneal and supradiaphragmatic lymph node metastases in 9% (9/97) and 4% (4/97), respectively; bone metastases in 27% (26/97); and visceral metastases in 3% (3/97). In the subgroup of patients with a PSA of <2 ng/mL above nadir, local recurrence occurred in 76% (19/25) and pelvic lymph node metastases in 36% (9/25). Conclusion: 18F-rhPSMA-7 PET/CT demonstrates high detection rates in prostate cancer patients with BCR after primary radiation therapy, even at low PSA values. Its diagnostic efficacy is comparable to published data for other PSMA ligands.
Biochemical recurrence (BCR) of prostate cancer with rising prostate-specific antigen (PSA) levels is observed in up to half of patients after radical prostatectomy (RP) or primary radiotherapy with curative intent and represents the first sign of treatment failure (1). The definition of BCR, however, depends on the applied primary therapy option. BCR after RP is defined by 2 consecutive PSA rises of >0.2 ng/mL (2), whereas BCR after radiotherapy is defined by a PSA rise of ≥2 ng/mL above the nadir (3). This PSA threshold defined by the Phoenix criteria was presented in 2006, when detection of prostate cancer recurrence was based on conventional imaging. Highly sensitive molecular imaging methods, such as PET with prostate-specific membrane antigen (PSMA)–targeting ligands, were not yet available.
68Ga-labeled PSMA ligands provide high sensitivity for the detection of BCR, with increasing pooled detection rates of 42%, 58%, 76%, and 95% at rising PSA categories of 0–0.2, >0.2–1, >1–2, and >2 ng/mL (4). Thus PSMA PET might also be of high value in patients after primary curative-intent radiotherapy, even those at earlier stages of BCR with low PSA values. Although 68Ga-labeled compounds are currently the most used tracers for PSMA-targeted PET imaging, 18F-labeled PSMA ligands offer advantages regarding half-life and image resolution.
Several 18F-labeled PSMA ligands (e.g., DCFPyL and PSMA-1007) have been introduced and are being evaluated in phase III clinical studies, with DCFPyL being recently approved. The first data indicate similar diagnostic performance, with pooled BCR detection rates of 49%, 73%, 88%, and 92% for PSA categories of 0–0.5, >0.5–1, >1–2, and >2 ng/mL, respectively (5). Furthermore, hepatobiliary excretion of 18F-PSMA-1007 reduces tracer accumulation in the urinary bladder, as might be of particular value in cases of BCR after primary radiotherapy, with local recurrence and pelvic lymph node metastases representing common localizations of prostate cancer recurrence (6,7). Detection rates for BCR are reported mainly in patients after primary RP, and data on the diagnostic efficacy of 18F-labeled PSMA ligands have been presented only within mixed cohorts of RP and radiotherapy patients; therefore, specific information on diagnostic performance in patients with BCR after curative-intent radiotherapy is rare (5).
Recently, radiohybrid PSMA (rhPSMA) ligands have been introduced as novel theranostic PSMA agents enabling radiolabeling with radiometals (e.g., 68Ga and 177Lu) and 18F (8). Initial data for its lead compound, 18F-rhPSMA-7, state that its diagnostic performance for primary N-staging and localization of BCR after RP is similar to that of other PSMA ligands (9,10). Its urinary excretion is lower than that of 68Ga-PSMA-11 even after an uptake time of up to 2.5 h (11). Here, we present the results of a bicentric, retrospective analysis evaluating the diagnostic efficacy of 18F-rhPSMA-7 PET/CT in patients with BCR after primary curative-intent radiotherapy.
MATERIALS AND METHODS
Patients
Data from prostate cancer patients with BCR after primary radiotherapy with curative intent who underwent PET/CT with 18F-rhPSMA-7 between October 2017 and March 2019 at the Technical University Munich (TUM) or the Ludwig-Maximilians-University Munich (LMU) were retrospectively reviewed. Patients with prior salvage prostatectomy after primary radiotherapy or documented castration-resistant disease were excluded. Finally, 97 patients were included, and their PSA values and clinical information on prior therapies, including prior androgen deprivation therapy (ADT), were noted. The retrospective analysis was approved by the local Ethics Committee at both centers (TUM permit 290/18S; LMU permit 20-178). The requirement to obtain written informed consent was waived.
Synthesis, Administration, and Imaging of 18F-rhPSMA-7
18F-rhPSMA-7 was radiolabeled as described previously (8). 18F-rhPSMA-7 was administered in compliance with the German Medicinal Products Act, AMG § 13 2b and the responsible regulatory body (government of Upper Bavaria). All patients gave written informed consent. The median injected activity was 299 MBq (mean, 306 MBq; range, 204–420 MBq), and the median uptake time was 77 min (mean, 76 min; range, 46–120 min). Patients received a diluted oral contrast medium (300 mg of Telebrix) and 20 mg of furosemide.
18F-rhPSMA-7 PET/CT was performed on a Biograph mCT Flow scanner (Siemens Medical Solutions) (73 patients: 65 at TUM and 8 at LMU) and on a Discovery 690 scanner (GE Healthcare) (24 patients at LMU). PET/CT scans were acquired in 3-dimensional mode with an acquisition time of 1.1 mm/s on the Biograph mCT Flow and 2.5 min per bed position on the Discovery 690. PET images were reconstructed using ordered-subset expectation maximization (Biograph mCT Flow: TrueX, 4 iterations, 8 subsets; Discovery 690: VUE point FX, 2 iterations, 26 subsets) followed by a postreconstruction smoothing gaussian filter (5 mm in full width at half maximum). Phantom studies based on the National Electrical Manufacturers Association NU2-2001 standard were conducted at LMU to allow valid pooling of results between Siemens and GE Healthcare scanners. A diagnostic CT scan was performed before the PET scan during the portal venous phase 80 s after intravenous injection of contrast agent.
Image Analysis
All images were interpreted during clinical rounds by a consensus reading by an experienced, board-certified nuclear medicine physician and a board-certified radiologist and centrally reevaluated by an experienced nuclear medicine physician at each site. Any focal tracer accumulation higher than the surrounding background and not associated with physiologic uptake or unspecific tracer uptake due to typical pitfalls (12) was considered suggestive of malignancy. All lesions suspected of representing prostate cancer recurrence were noted. Lesions were categorized as local recurrence (prostate bed), lymph node metastases (further stratified as pelvic, retroperitoneal, or supradiaphragmatic), bone metastases, or other distant metastases (e.g., visceral metastases).
Statistical Analysis
Detection rates of lesions representing prostate cancer recurrence were plotted against baseline PSA values on a per-patient basis and on a localization basis (local recurrence, lymph node metastases, bone metastases, and other metastases). Descriptive analysis was performed by calculating the median, mean, range, and interquartile range. Unpaired 2-sample t tests and Mann–Whitney U tests were used to evaluate differences between single groups. The Fisher exact test was used to evaluate detection rates in patients with and without ADT and in patients with Gleason scores of ≤7 and ≥8. A P value of less than 0.05 was considered significant. Statistical analyses were performed using SPSS statistics (version 26; IBM).
RESULTS
In total, 97 patients were included in this bicentric retrospective analysis. The median age was 74 y (range, 57–87 y). The PSA value within the 4 wk preceding 18F-rhPSMA-7 PET/CT was documented for every patient; median PSA before PET was 4.19 ng/mL (range, 0.0–159 ng/mL; interquartile range, 1.96–8.6 ng/mL). Twenty-five patients (26%) had a PSA of ≤2 ng/mL and did not reach the PSA threshold for BCR defined by the Phoenix criteria; the median PSA in this subgroup was 0.88 ng/mL (range, 0.0–1.96 ng/mL; interquartile range, 0.7–1.46 ng/mL). Thirty patients (31%) had received ADT within 6 mo before PET/CT. Detailed patient characteristics, including primary Gleason score and initial PSA, are provided in Table 1.
Patient Characteristics
Detection Rate of 18F-rhPSMA-7 PET/CT on a Patient Basis
Detection Efficacy
18F-rhPSMA-7 PET/CT showed pathologic findings suggestive of prostate cancer recurrence in 91 of 97 patients (94%). The mean PSA in patients with at least one localized area suggestive of recurrent prostate cancer was 9.6 ng/mL, compared with 3.1 ng/mL in PET-negative patients (P = 0.183). The overall detection efficacy stratified by PSA was 88% (22/25) for a PSA of <2 ng/mL, 97% (30/31) for 2–<5 ng/mL, 90% (19/21) for 5–<10 ng/mL, and 100% (20/20) for ≥10 ng/mL (Fig. 1). After further subclassification of patients outside the Phoenix criteria for BCR (n = 25), detection rates were 80% (4/5) for a PSA of <0.5 ng/mL, 90% (9/10) for 0.5–<1 ng/mL, 100% (4/4) for 1–<1.5 ng/mL, and 83% (5/6) for 1.5–<2 ng/mL (Fig. 2).

Overall detection rate for all patients (n = 97) stratified by PSA value.

Detection rate stratified by PSA value in patients with PSA of <2 ng/mL not meeting Phoenix criteria for BCR after radiotherapy (n = 25).
Effect of ADT and Gleason Score
There were no significant differences in detection rates among patients with prior ADT in the 6 mo preceding 18F-rhPSMA-7 PET/CT (100% [30/30]) and those without prior ADT (91% [61/67], P = 0.173; Fig. 3A) or patients with a Gleason score of ≤7 (98% [42/43]) and those with a Gleason score of ≥8 (91% [31/34], P = 0.316; Fig. 3B).

Detection rates stratified by prior ADT use within 6 mo preceding 18F-rhPSMA-7 PET/CT (A) and primary Gleason score (B). GS = Gleason score.
Localization of 18F-rhPSMA-7 PET–Positive Lesions
Detailed localization of 18F-rhPSMA-7–avid lesions suggestive of recurrence of prostate cancer is shown in Table 2. A clear trend toward a higher proportion of patients with distant metastases (nonregional lymph node metastases and bone metastases) was noted with rising PSA (Fig. 4). Overall local recurrence was observed in 80% (78/97), pelvic lymph node metastases in 38% (37/97), nonregional lymph nodes in 13% (13/97), bone metastases in 27% (26/97), and visceral metastases in 3% (3/97; 2 patients with penile metastases and 1 patient with lung metastasis).
Localization of 18F-rhPSMA-7 PET–Positive Tumor Lesions Stratified by PSA Value
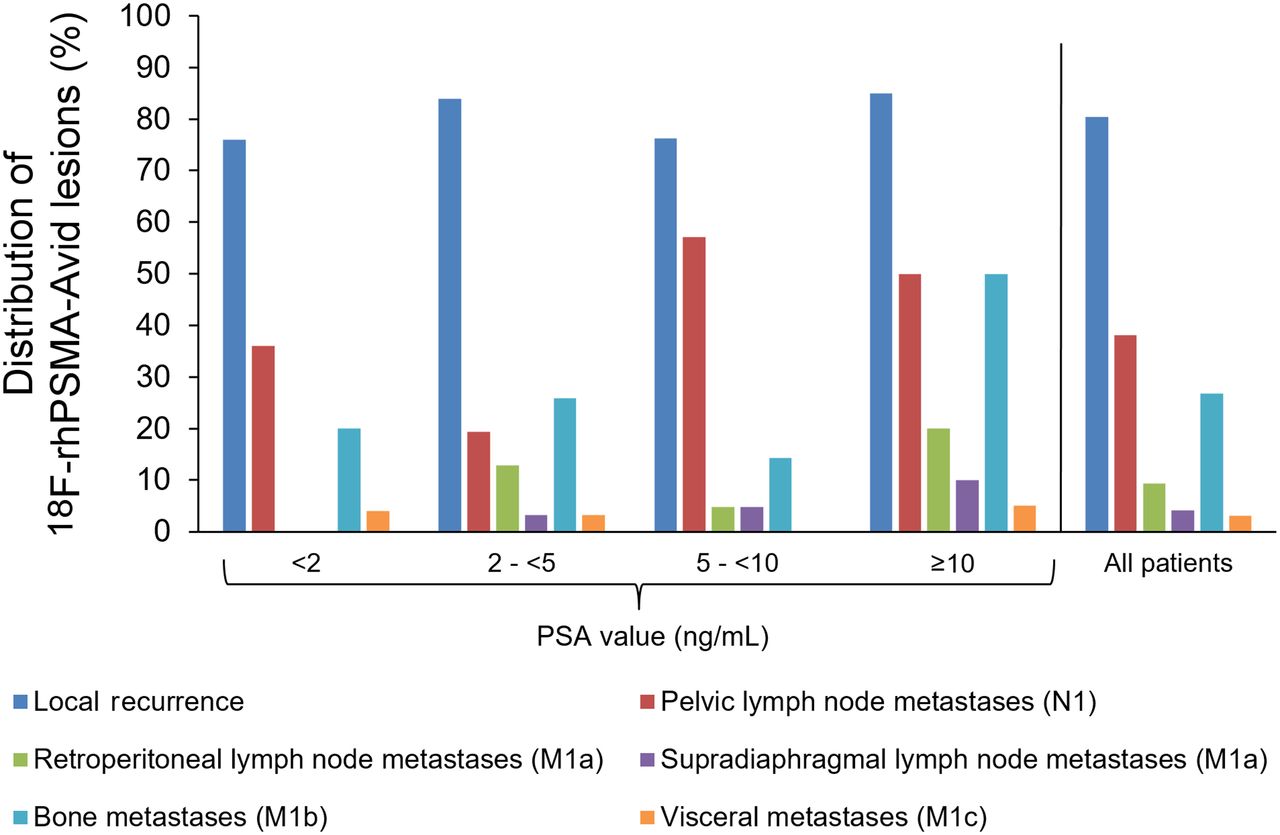
Localization of 18F-rhPSMA-7–positive tumor lesions for all patients and stratified by PSA value.
In the subgroup of patients with PSA values of <2 ng/mL, local recurrence occurred in 76% of patients (19/25) and pelvic lymph node metastases in 36% (9/25). Furthermore, a low number of distant metastases, including bone metastases in 20% (5/25) and visceral metastasis in 4% (1/25), were present; no nonregional retroperitoneal or supradiaphragmatic lymph nodes were detected on 18F-rhPSMA-7 PET/CT.
DISCUSSION
This bicentric, retrospective analysis evaluated the diagnostic efficacy of the novel 18F-labeled PSMA ligand, 18F-rhPSMA-7, for the detection of prostate cancer recurrence in patients after primary radiotherapy with curative intent. Recently, it has been shown that 18F-rhPSMA-7 provides high detection rates for BCR after RP (9). Of 261 patients with a median PSA of 0.91 ng/mL, 211 (81%) showed at least 1 lesion suggestive of prostate cancer recurrence. In analogy to previously described data for other 18F- and 68Ga-labeled PSMA ligands, increasing detection rates were observed at increasing PSA values (9,13–15).
The current analysis focused on patients with BCR after primary curative-intent radiotherapy. A rising PSA after RP and curative-intent radiotherapy is the first sign of primary-therapy failure, and salvage therapies include pelvic lymph node dissection or radiotherapy in cases of pelvic lymph node metastases or systemic therapies, including ADT, and chemotherapy in cases of distant metastases (1). However, detection and localization of prostate cancer recurrence in patients with BCR after curative-intent radiotherapy can be challenging. Considering the availability of different salvage therapy options and the impact of PSMA PET imaging on patient management, early detection of recurrence remains crucial for optimal treatment planning (2,16,17).
BCR rates after primary curative-intent radiotherapy range from 10% to 60% with external-beam radiation therapy or from 7% to 35% with brachytherapy, and up to 44% despite external-beam radiation therapy dose escalation of 78 Gy (18–20). Although the overall pooled diagnostic efficacy of 18F-labeled PSMA ligands for the detection of BCR is 81% (95% CI, 71%–88%), it increases from 49% to 92% at PSA levels of <0.5 and ≥2 ng/mL, respectively (5). However, data are reported mainly after RP, and detailed information on BCR detection rates in patients after primary radiotherapy are available mainly for small subgroups of mixed cohorts (5). Dietlein et al. reported overall BCR detection rates of 79% (19/24) and 92% (56/61) for 18F-DCFPyL PET and 68Ga-PSMA-11 PET, respectively, after primary radiotherapy and 71% (27/38) and 68% (46/68) for 18F-DCFPyL PET and 68Ga-PSMA-11 PET, respectively. after RP (21). Surprisingly, detection rates were PSA-independent in the radiotherapy group, whereas rising PSA levels have been reported to be clearly associated with higher detection rates in patients after RP (13–15). This finding might at least partially be explained by the Phoenix criteria definition of a PSA rise of 2 ng/mL above the nadir. However, with the nadir varying substantially between patients, the absolute PSA value at the time of imaging might be less relevant than in patients with BCR after RP.
Similarly, detection rates also did not correlate positively with PSA in the present study. This finding might be related partly to the high detection efficacy in all subgroups: 88%, 97%, 90%, and 100% for a PSA of <2, 2–<5, 5–<10, and ≥10 ng/mL, respectively. PSA independence was also observed in the subgroup of patients, who did not reach the threshold for BCR defined by the Phoenix criteria (PSA of ≥2 ng/mL above the nadir), with detection rates of 80%, 90%, 100%, and 83% for a PSA of <0.5, 0.5–<1, 1–<1.5, and 1.5–<2 ng/mL, respectively. Similar detection efficacies (including both 68Ga-PSMA-11 and 18F-DCFPyL PET scans) in a subgroup of 63 patients not meeting the Phoenix criteria were most recently reported (22). The authors found no influence of PSA value on PET outcome, and detection rates of 75.0% (12/16), 89.3% (25/28), and 84.2% (16/19) at PSA levels of <1.0, 1.0–1.49, and 1.5–1.99 ng/mL, respectively, above the nadir, were present. However, PSA independence might be a consequence of the relatively small number of patients in each PSA group reported in these cohorts, including the present work (21,22).
Notably, Meredith et al. described increasing detection rates for 68Ga-PSMA-11 in 107 patients after primary radiotherapy; however, lower detection rates in patients with very low PSA values might also be attributed to the small sample sizes in these groups, with detection rates of 33% at a PSA of 0.01–<0.5 ng/mL in 1 of 3 patients and 71% at a PSA of 0.5–<1 ng/mL in 5 of 7 patients, respectively (23). Recently, Raveenthiran et al. presented data on the diagnostic efficacy of 68Ga-PSMA-11 in 276 patients after primary radiotherapy, representing the largest cohort so far (24). Although 203 patients were above the threshold for BCR defined by the Phoenix criteria, PSA in the remaining 73 patients was <2 ng/mL. They observed a slight trend toward increasing detection rates at rising PSA levels, at 66.7% (8/12) for a PSA of <0.5 ng/mL, 77.8% (14/18) for 0.5–<1 ng/mL, 76.7% (33/43) for 1–<2.0 ng/mL, and 90.6% (184/203) for >2 ng/mL. Likewise, Einspieler et al. presented higher detection rates with rising PSA levels in a cohort of 118 patients with BCR according to the Phoenix criteria, at 81.8% (36/44), 95.3% (41/43), and 96.8% (30/31) for PSA levels of 2–<5, 5–<10, and ≥10 ng/mL, respectively (7).
In summary, the detection efficacy of PSMA ligand PET in patients meeting the Phoenix criteria ranges from 91% to 100% (Table 3) (3,7,23,24). With an overall detection rate of 96%, our data for 18F-rhPSMA-7 PET/CT fit well into this range. Moreover, our data add to the increasing evidence in the literature indicating that PSMA ligand PET imaging might also detect lesions indicative of recurrent disease in patients with PSA levels below the threshold set by the Phoenix criteria for BCR. In the present work, the overall detection rate for 18F-rhPSMA-7 in patients with BCR at PSA levels of <2 ng/mL was 88% (22/25) and highly comparable to the cohorts of Jansen et al. (84% [53/63]) (22), Raveenthiran et al. (75% [55/73]) (24), and Meredith et al. (80% [20/25]) (Table 3) (23). These results strongly indicate that the classic definition of BCR after radiotherapy should be redefined in an era of sensitive PSMA ligand PET imaging. Sonni et al. presented data from a prospective single-center study evaluating the impact of PSMA PET imaging on patient management in different clinical situations (17). According to this trial, patients with BCR after primary radiotherapy who do not meet the Phoenix criteria seem to be those profiting most from the high sensitivity of PSMA PET imaging. In the era of PSMA PET, the definition of BCR according to the Phoenix criteria should be revisited or PSMA PET should be integrated into the definition of recurrence. However, larger patient groups and, preferably, prospective data are required to confirm this hypothesis.
Detection Rates in Patients with BCR after Primary Curative-Intent Radiotherapy Stratified by PSA Level
Comparable to previously described data, PSMA PET detection rates for BCR after primary radiotherapy were not clearly influenced by prior ADT therapy or primary Gleason score (7). We found no significant differences in detection rates between patients who received ADT in the 6 mo preceding 18F-rhPSMA-7 PET and patients without prior ADT (100% vs. 91%, P = 0.173). Similar results have been demonstrated using 18F-rhPSMA-7 PET in patients with BCR after RP (detection rate of 81% for both prior ADT and no ADT, P = 0.54) (9). However, the impact of ADT on PSMA PET is still a matter of debate. Despite data indicating reduced PSMA ligand uptake after long-term ADT (25), the need for withdrawal of ADT before PSMA-targeted PET remains controversial, particularly when considering the therapeutic effects of ongoing ADT (26). However, concomitant use of ADT at the time of primary radiotherapy will have an impact on patterns of failure, which might have an impact on lesion detection. Unfortunately, because of the retrospective design of this study, detailed information on concomitant use of ADT during primary radiotherapy was not available for all patients.
Localization of prostate cancer recurrence at early stages of BCR and the impact on treatment planning represent one of the main strengths of PSMA ligand PET. In a recent review, the impact of PSMA ligand PET on therapy planning ranged from 30% to 76% (17,27,28). Up to 40% of patients can be guided away from systemic treatment, and up to 60% of patients can be guided toward application of PSMA-directed local therapy (28). PSA before salvage therapy represents the strongest predictor of survival after salvage RP and salvage radiotherapy (29–31). Most patients in our cohort showed localized disease, with local recurrence in 80% (78/97) and pelvic lymph node metastases in 38% (37/97); however, distant metastases were observed in up to 27% of patients, with bone metastases representing the main site. This analysis lacks details on potential unspecific bone uptake. This potential pitfall has been reported for different PSMA ligands in a large number of case reports, specific analyses, and reviews (12,32–34). Specifically, using 18F-rhPSMA-7, Kroenke et al. (34) reported that 120 areas of focal increased uptake were interpreted as not related to prostate cancer, with the majority (n = 45) being in the ribs.
Likewise, in the study by Raveenthiran et al., local sites of tumor recurrence were most common, but they were seen in only 57% (157/276) of patients, compared with 80% in our cohort (24). This difference might be attributed to the high accumulation of 68Ga-PSMA-11 in the urinary bladder, potentially impairing detection of small local recurrences near the bladder (35). Nonetheless, false-positive findings in the prostate represent a further possible pitfall of PSMA PET imaging, particularly in the postradiotherapy setting, as described in a recently published prospective multicenter trial (36). We acknowledge that given the lack of histopathologic validation in the present study, this possibility cannot be completely excluded. However, all scans were reevaluated by experienced readers.
Although the small sample size limits meaningful conclusions, the tumor distribution was not influenced by patients’ PSA in the present study. However, whereas no nonregional lymph node metastases were observed in patients with PSA levels of <2 ng/mL, bone metastases and even visceral metastases were identified in 20% (5/25) and 4% (1/25), respectively. In the overall cohort, visceral metastases were identified in the lung and in the penile shaft in 2 cases, both representing rare sites of tumor recurrence after BCR (37,38). In one patient with a PSA of 0.72 ng/mL, a penile metastasis represented the only finding on 18F-rhPSMA-7 PET. Almost-consistent rates of localized disease and distant metastases indicate that early identification of localized salvage therapy or systemic therapy might be delayed when strictly following Phoenix criteria thresholds in BCR patients after primary radiotherapy. Our findings warrant further investigations using PSMA ligand PET in patients with low PSA not meeting the Phoenix criteria.
This study had several limitations. First, 18F-rhPSMA-7 PET findings were not validated by histology, which represents the reference standard for definition of prostate cancer recurrence. However, biopsy was not feasible for many lesions because of difficulty in localization and their small size. Second, the data were retrospective, and the sample size was relatively small; particularly, only 25 patients were below the threshold of 2 ng/mL defined by the Phoenix criteria. Currently, there are 2 clinical trials investigating the safety and diagnostic efficacy of an 18F-labeled rhPSMA ligand: one on patients with prostate cancer recurrence (SPOTLIGHT trial; NCT04186845) and another on patients with newly diagnosed prostate cancer (LIGHTHOUSE trial; NCT04186819). Furthermore, detailed information on primary radiotherapy was missing because of the retrospective design of this study (e.g., radiation field and dose, concomitant ADT); lack of this information is likely to have an impact on patterns of failure.
CONCLUSION
18F-rhPSMA-7 PET/CT demonstrates high detection rates in patients with BCR of prostate cancer after primary radiotherapy. The detection rate was not influenced by Gleason score, prior use of ADT, or PSA levels. Consistent with published data for other PSMA ligands, high detection rates were observed even in patients with PSA levels of <2 ng/mL, indicating that 18F-rhPSMA-7 has the potential to guide salvage therapy even at early stages of BCR after primary radiotherapy.
DISCLOSURE
Hans-Jürgen Wester, Alexander Wurzer, and Matthias Eiber are named as inventors on a patent application for rhPSMA. Hans-Jürgen Wester and Matthias Eiber received funding from the SFB 824 (DFG Sonderforschungsbereich 824, project B11) from the Deutsche Forschungsgemeinschaft, Bonn, Germany, and from Blue Earth Diagnostics (licensee for rhPSMA) as part of an academic collaboration. Hans-Jürgen Wester is a founder, shareholder, and advisory board member of Scintomics GmbH, Fuerstenfeldbruck, Germany. Matthias Eiber is a consultant for Blue Earth Diagnostics. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the detection efficacy of 18F-rhPSMA-7 PET/CT in patients with BCR of prostate cancer after primary curative-intent radiotherapy?
PERTINENT FINDINGS: 18F-rhPSMA-7 PET/CT offers high detection efficacy in patients with BCR of prostate cancer above and below the PSA threshold of 2 ng/mL defined by the Phoenix criteria. Efficacy is highly comparable to data published for 68Ga-PSMA-11.
IMPLICATIONS FOR PATIENT CARE: 18F-rhPSMA-7 has the potential to guide therapy for BCR after failure of primary radiotherapy.
ACKNOWLEDGMENT
Writing support was provided by Dr. Catriona Turnbull (Blue Earth Diagnostics, Oxford, U.K.).
Footnotes
Published online Mar. 10, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 7, 2021.
- Accepted for publication December 2, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.