


Abstract
68Ga-labeled prostate-specific membrane antigen (PSMA) PET/CT is increasingly used in men with biochemical recurrence (BCR) after radical prostatectomy (RP), but its longer-term prognostic or predictive potential in these men is unknown. The aim of this study was to evaluate the predictive value of PSMA PET for a 3-y freedom from progression (FFP) in men with BCR after RP undergoing salvage radiotherapy (sRT). Methods: This prospective multicenter study enrolled 260 men between 2015 and 2017. Eligible patients were referred for PSMA PET with a rising level of prostate-specific antigen (PSA) after RP. Management after PSMA PET was recorded but not mandated. PSMA PET protocols were standardized across sites and reported prospectively. Clinical, pathologic, and surgical information; sRT; timing and duration of androgen deprivation; 3-y PSA results; and clinical events were documented. FFP was defined as a PSA rise of no more than 0.2 ng/mL above nadir after sRT, with no additional treatment. Results: The median PSA was 0.26 ng/mL (interquartile range, 0.15–0.59 ng/mL), and follow-up was 38 mo (interquartile range, 31–43 mo). PSMA PET had negative results in 34.6% (90/260), showed disease confined to the prostatic fossa in 21.5% (56/260), showed disease in the pelvic nodes in 26.2% (68/260), and showed distant disease in 17.7% (46/260). Of the patients, 71.5% (186/260) received sRT: 38.2% (71/186) to the fossa only, 49.4% (92/186) to the fossa plus the pelvic nodes, and 12.4% (23/186) to the nodes alone or stereotactic body radiation therapy. PSMA PET was highly predictive of FFP at 3 y after sRT. Overall, FFP was achieved in 64.5% (120/186) of those who received sRT, 81% (81/100) with negative results or fossa-confined findings versus 45% (39/86) with extrafossa disease (P < 0.0001). On logistic regression, PSMA PET was more independently predictive of FFP than established clinical predictors, including PSA, T stage, surgical margin status, or Gleason score (P < 0.002). Thirty-two percent of men with a negative PSMA PET result did not receive treatment. Of these, 66% (19/29) progressed, with a mean rise in PSA of 1.59 ng/mL over the 3 y. Conclusion: PSMA PET results are highly predictive of FFP at 3 y in men undergoing sRT for BCR after RP. In particular, men with negative PSMA PET results or disease identified as still confined to the prostatic fossa demonstrate high FFP, despite receiving less extensive radiotherapy and lower rates of additional androgen deprivation therapy than those with extrafossa disease.
- prostate-specific membrane antigen
- PSMA
- PET/CT
- treatment outcome
- biochemical failure
- radical prostatectomy
Radical prostatectomy (RP) is the most widely used treatment for men with localized prostate cancer. However, up to 20%–50% of the prostate cancer patients managed with RP will experience biochemical recurrence (BCR), especially those with poorly differentiated disease and positive surgical margins (1,2). Currently in these men, salvage radiotherapy (sRT) with or without androgen deprivation therapy (ADT) is the only remaining potentially curative treatment option. Overall, the 5-y progression-free survival rate in patients undergoing sRT is strongly related to serum prostate-specific antigen (PSA) level at the start of sRT and varies from 71% in men with a pre-sRT PSA of less than 0.2 ng/mL to only 18% in men with a pre-sRT PSA of more than 1.5 ng/mL (1,3–5). The addition of more extensive radiotherapy fields and short-term ADT has further improved freedom from progression (FFP) (4,6). Prostate-specific membrane antigen (PSMA) is a glycoprotein highly expressed on the cell surface of prostate cancers that has recently been effectively targeted using small-molecule peptides labeled with PET radioisotopes (7–10). Prospective evaluation of PSMA PET in men with a rising PSA after RP has demonstrated a very high sensitivity for disease detection even in men with very low PSA values (10,11). Further, PSMA PET identifies disease outside the prostatic fossa in up to 43% of men with a rising PSA after RP (11,12) and consequently has shown a high impact on management and early treatment responses in these men (13,14). However, what is not yet known is whether PSMA PET findings impact longer-term outcomes and whether the PSMA PET results should indeed dictate subsequent treatment. The aim of this study was to prospectively observe how the results of PSMA PET impact management and subsequent treatment outcomes.
MATERIALS AND METHODS
Study Design
This prospective study was conducted at 4 Australian hospitals (St Vincent’s and Royal North Shore, Sydney, and Sir Charles Gairdner and Fiona Stanley, Perth). Eligible patients had a histologic diagnosis of prostate cancer and were referred for PSMA PET/CT imaging for BCR with a rising PSA level (PSA ≥ 0.05 and < 5.0 ng/mL) after RP without any contraindications for sRT. All PSMA PET/CT was undertaken between January 2015 and March 2017. Informed written consent was obtained from all patients, and Institutional Human Research Committee ethics approval was obtained for each site.
68Ga-PMSA PET/CT
68Ga-PSMA PET/CT scans were performed using a standardized protocol across institutions. Patients were injected with a 1.8–2.2 MBq/kg dose of 68Ga-PSMA 11 and imaged a minimum of 60 min later, with no delayed imaging undertaken. Vertex to mid-thigh PET/CT imaging was performed on time-of-flight PET/CT scanners at all institutions (Biograph PET/64-slice CT [Siemens] or Ingenuity/64-slice CT [Phillips]). For the PSMA PET/CT, unenhanced CT was performed using a slice thickness of 2 mm, a soft-tissue reconstruction kernel, 120 keV, and 50 mAs. Immediately after CT scanning, a whole-body PET scan was acquired for 2 min per bed position. All PET images were interpreted prospectively by credentialed nuclear medicine physicians with experience in reporting prostate PET images. Data for all PSMA PET scans were analyzed both visually and quantitatively. Visual analysis included a 4-point certainty scoring scale (definitely negative; equivocal: probably negative; equivocal: probably positive; definitely positive), as well as anatomic site and size of lesions. Semiquantitative analysis was undertaken using SUVmax. For database purposes, each positive finding was coded according to anatomic site, SUVmax, number of lesions, and reporter certainty. The coded PSMA PET results were those available to treating investigators as a decision-making tool before undertaking sRT.
Data Collection
Data collected at enrollment included age, time since RP, initial pathology including pathologic T stage, Gleason score, surgical margin status, lymph node staging, and PSA at the time of PSMA PET. As a part of the trial, investigators completed management-impact questionnaires both before and after PSMA PET imaging, the results of which have been published previously (13). After PSMA PET, the questionnaire results were documented, as were subsequent treatments. Importantly, PSMA PET results were made available to the treating clinician; however, treatments were monitored rather than mandated by the trial. Management plans after the PSMA PET were documented for each patient, including date and type of treatment initiated (observation, systemic therapy, or local therapy). The posttreatment PSA level was the most recent one recorded for each patient before analysis.
sRT
All sRT undertaken was based on the management decisions of the treating clinician after learning the PSMA PET result, using local institutional sRT protocols. For the purposes of the trial, any site of targeted radiation treatment was documented. In the case of the sRT fields delivered, the patient’s treatments were categorized as prostatic fossa only, prostatic fossa with pelvic lymph nodes, pelvic lymph nodes only, or stereotactic body radiotherapy to metastases within or external to the pelvis. The use, timing, and duration of ADT were also documented.
Outcome Measures
The primary outcome measure was FFP, defined as serum PSA remaining no more than 0.2 ng/mL above the post-sRT nadir, without either the initiation of ADT or additional radiation therapy after completion of sRT (5).
Statistical Analysis
The time of follow-up was measured from the date of sRT to the last PSA undertaken before analysis or to the date of either disease progression (PSA rise > 0.2 ng/mL) or the addition of systemic treatment or radiation. The rates of FFP were estimated by Kaplan–Meier analysis. Multivariate Cox regression analyses were used to identify determinants for differences in FFP between the PSMA PET result, pathologic T and N stage, RP surgical margins, Gleason score (sum), PSA level at the time of PSMA PET, and time (mo) to BCR after RP. Pearson correlation was used to identify associations between FFP, PSMA PET result, pT stage, pN stage, Gleason score, PSA level at the time of PSMA PET, PSA before surgery, and time (mo) to BCR after RP. For the purposes of analysis, all scans scored as either definitely positive or probably positive on the PSMA PET were considered positive. P values of less than 0.05 were considered statistically significant. Statistical analysis was performed with SPSS Statistics (version 25.0; IBM).
RESULTS
Demographics
Baseline characteristics are summarized in Table 1. The inclusion criteria for this study were met by 260 people, who were prospectively enrolled. Only 2.3% (6/260) were lost to long-term follow-up. Median age at the time of PSMA PET scanning was 68 y (interquartile range [IQR], 63–72 y). The median time between RP and PSMA PET was 37.8 mo (IQR, 8.6–87.0 mo). The median PSA value at PSMA PET was 0.26 ng/mL (IQR, 0.15–0.59 ng/mL), and the median follow-up after PSMA PET was 38 mo (IQR, 31–43 mo).
Patient Characteristics
PSMA PET
PSMA PET results were positive in 65.4% (170/260) of enrolled patients. Sites of disease included the prostatic fossa only, in 21.5% (56/260); pelvic nodal involvement, in 26.2% (68/260); distant lymph nodes, in 6.2% (16/260); bone, in 9.6% (25/260); and the viscera, in 1.9% (5/260) (Table 2). In total, 46% of men had positive PSMA PET findings beyond the prostatic fossa and 18% had extrapelvic metastatic disease. PSMA PET positivity increased with higher PSA values, with 50.6% (42/84) positive at a PSA of less than 0.2 ng/mL, compared with 90.2% positive (37/41) at a PSA of more than 1.0 ng/mL (P < 0.001) (Table 3). In total, 34.6% (90/260) of patients had negative PSMA PET results. Negative results were strongly associated with PSA level (P < 0.001), pT stage (P = 0.03), and surgical margins (P = 0.03) but not with GS, pN stage, or extracapsular extension.
Sites of Disease Recurrence on PSMA PET
PSMA PET Result Stratified by Increasing PSA Level
sRT
Of the 186 men who underwent sRT, 38% (71/186) received treatment to the prostatic fossa alone, 50% (92/186) to the prostatic fossa and pelvic lymph nodes, and 5% (9/186) to pelvic lymph nodes only, whereas 7% (14/186) received stereotactic body radiotherapy to either pelvic lymph nodes or distant sites. Finally, 25% (46/186) received adjuvant ADT with sRT (median, 10.25 mo; IQR, 6.33–9.18 mo). Overall, PSMA PET positivity conferred a higher likelihood of treatment with sRT (Table 4). The use of more extensive sRT fields was significantly more likely in those with PSMA PET–positive disease than in those with negative PSMA PET findings (42% [71/170] vs. 23% [21/90], respectively; P < 0.03). The use of ADT was also significantly higher in men with positive PSMA PET findings (31% [40/129]) than in those with negative findings (11% [6/56]) (P < 0.001). Of the 75 men who did not receive sRT, 45% (34/75) had negative PSMA PET findings; 32% (26/75) of these men received either ADT or other forms of systemic treatment, 4% (3/75) were managed with surgical lymph node dissection, and 65% (49/75) were observed, with no documented treatment in the follow-up period.
Treatment Administered on the Basis of PSMA PET Results
3-Year FFP
Overall, 64.5% of men who underwent sRT enjoyed FFP at 3 y. PSMA PET findings before sRT were highly predictive of FFP in those men who underwent sRT. Three-year FFP dropped from 81% (81/100) in those with negative or fossa-confined findings to 45% (39/86) when PSMA PET–positive disease was identified outside the prostatic fossa (P < 0.0001) (Fig. 1). A negative PSMA PET result in men receiving sRT was the most predictive of 3-y FFP, at 82.5% (47/57), followed closely by PSMA PET–avid disease confined to the prostatic fossa, at 79% (34/43); in the pelvic nodes, at 55% (33/59); in the distant lymph nodes, at 25% (2/8), and in the viscera or bones, at 21% (4/19; P < 0.0001) (Table 5). On univariate Cox regression analysis, PSMA PET findings, PSA at the time of sRT, and surgical margin status were all predictive of FFP. After multivariate Cox regression analysis, PSMA PET positivity was the only independently predictive factor for FFP in men who underwent sRT (Table 6). Despite a strong association between PSA level and PSMA PET findings, Kaplan–Meier curves demonstrated the stronger predictive value of PSMA PET for FFP (Fig. 2).

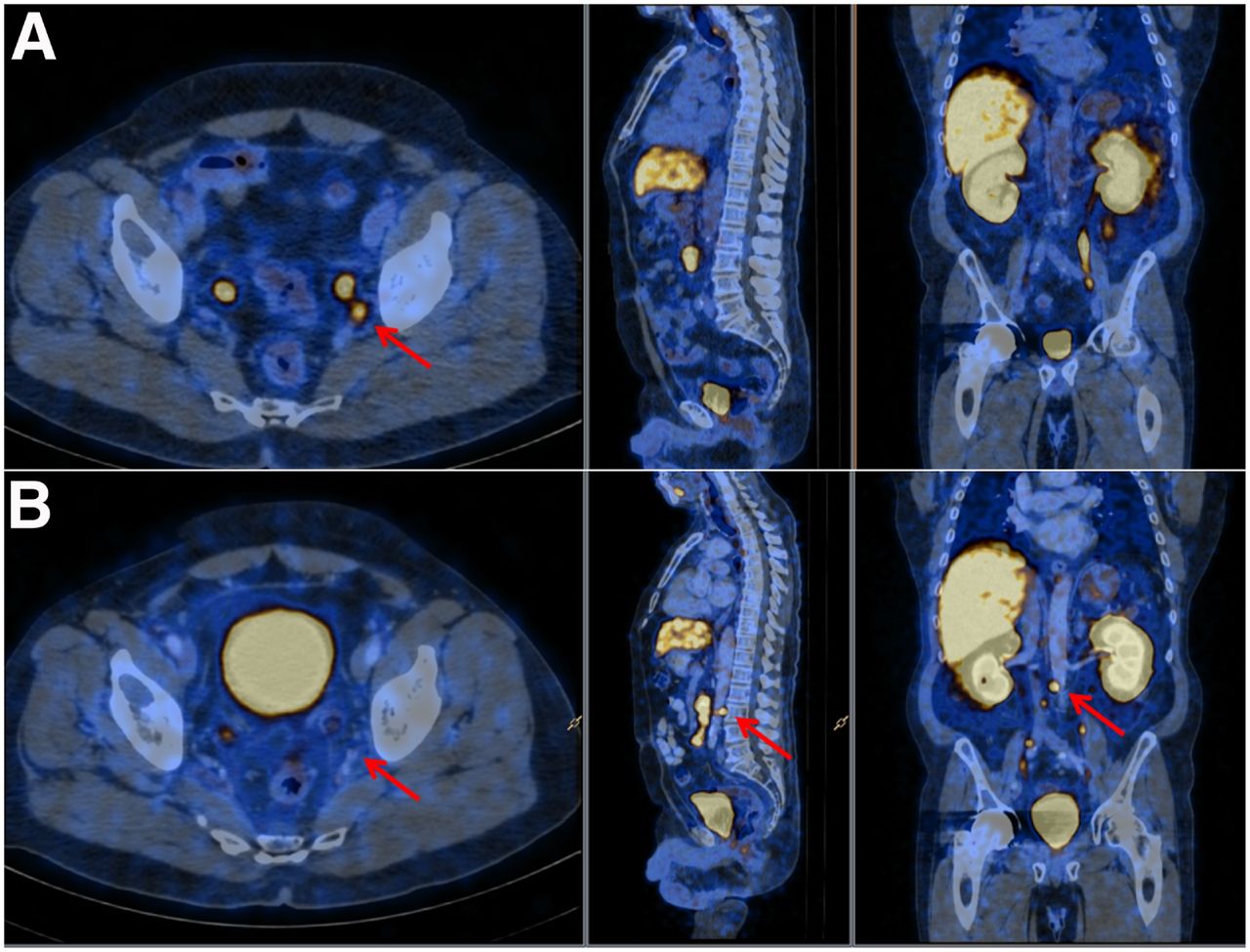
(A) PSMA PET images of man with Gleason score 9 prostate cancer and PSA of 0.23 ng/mL, treated with initial RP 12 mo beforehand, demonstrate PSMA PET–positive left obturator node (arrows). Patient subsequently underwent sRT to prostatic fossa and pelvic nodes. However, PSA did not respond. (B) Repeat PSMA PET images 10 mo later demonstrate treatment response in left obturator lymph node, but multiple new PSMA-avid lymph nodes (arrows) are seen immediately above sRT treatment field, extending superiorly to paraaortic region.
Incidence of FFP or Progressive Disease Based on PSMA PET Findings in Men Treated with sRT
Cox Logistic Regression Analysis of Clinical and Imaging Variables for Prediction of FFP in Men Who Underwent sRT

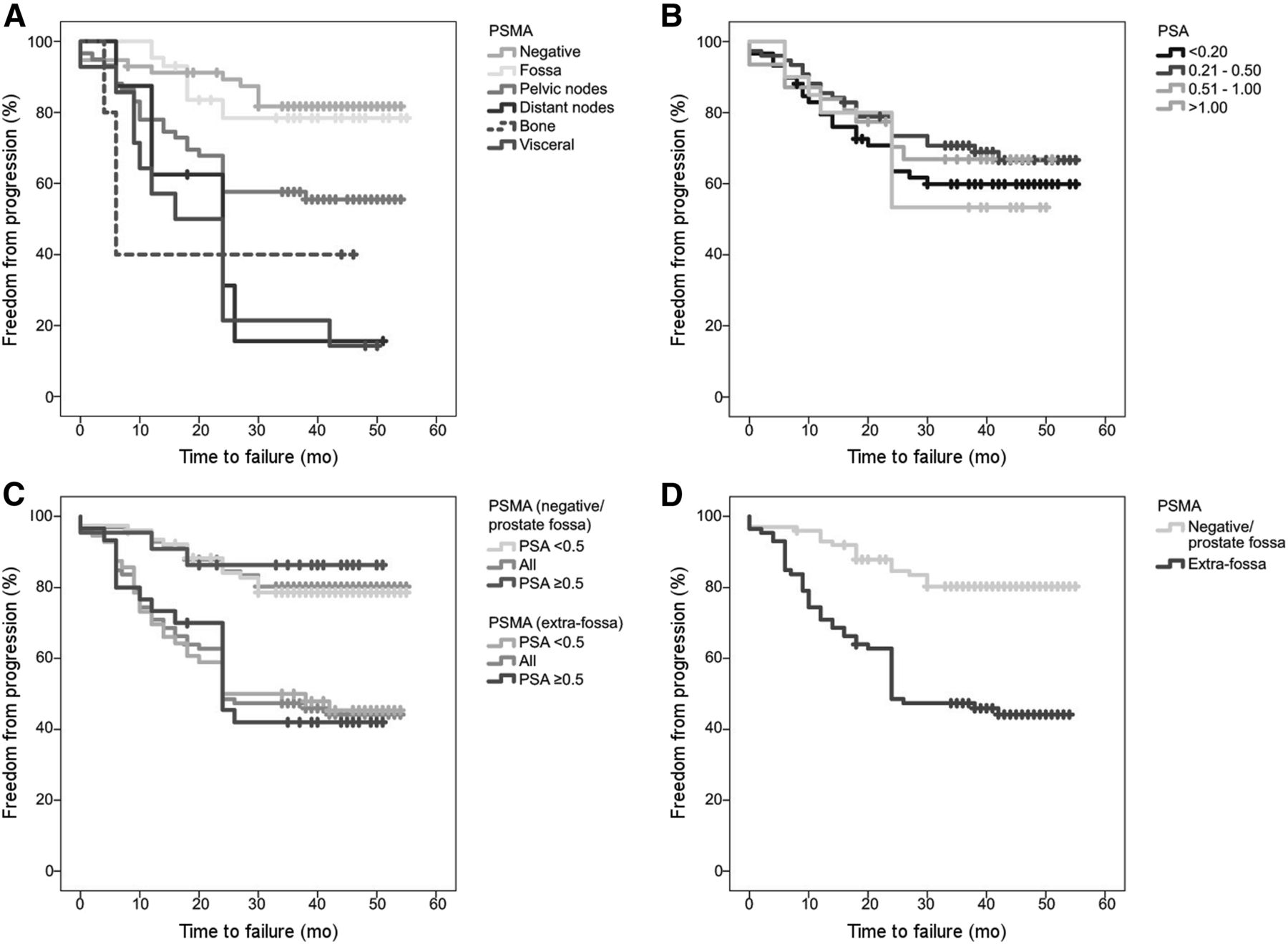
Kaplan–Meier curves for FFP based on PSMA PET (A), PSA (ng/mL) at PSMA PET (B), PSMA PET (negative/fossa-confined vs. outside fossa) stratified for both PSA and PSMA PET (C), and PSMA PET (negative/fossa-confined vs. outside fossa) (D).
Negative PSMA PET Results
Men with negative PSMA PET findings (34.6% [90/260]) were the most likely group to achieve 3-y FFP if they received sRT (82.5%), despite receiving less extensive radiotherapy fields or ADT (Table 3). Paradoxically, this group was also the least likely to receive sRT, with a higher chance of observation only in men with a negative compared with a positive PSMA PET result: 32% (29/90) versus 12.3% (21/170) (P < 0.001). In those men with negative results who were observed, without treatment, 66% (19/29) had an ongoing rise (>0.2 ng/mL) in PSA over the 3 y of follow-up (mean increase from baseline PSA, 1.59 ng/mL) (Fig. 3). Subgroup analysis of those men with negative results who were observed demonstrated that the PSA at the time of PSMA PET was lower when there was no significant rise in PSA during follow-up (0.15 vs. 0.56 ng/mL). There was no significant difference in risk grouping (surgical margin, Gleason score, or surgical T stage) between men with negative results who were treated with sRT and those who were observed.

FFP in men with negative scan results who underwent sRT vs. men who were observed over 3 y (P < 0.0001).
DISCUSSION
Prostatic fossa sRT for men with BCR after RP is the last potentially curative treatment, with up to 56% of these men enjoying long-term treatment control or “cure” (5). However, sRT is not without toxicity, and treatment will fail in a significant proportion of these men, with the added burden of treatment-induced toxicity. More recently reported studies have improved disease control rates by escalating treatment regimens; expanding radiotherapy fields, which modern sRT techniques such as intensity-modulated radiotherapy safely permit; or adding adjuvant ADT (4). However, although beneficial in improving FFP rates, treatment intensification increases the possibility of toxicity from both larger sRT fields and the metabolic effects of ADT. Identifying those men who would most benefit from escalated treatment regimens, versus those likely to be cured with fossa sRT alone (or safely observed), is a current need. PSMA PET has been thrown into the mix as a powerful diagnostic tool that is capable of identifying biochemically recurrent prostate cancer at low PSA levels that is still potentially curable (10,11,15,16). This study reports the first longer-term FFP results from PSMA PET–triaged treatments in a prospective study of men with BCR after RP.
This multisite prospective study has previously demonstrated a high management impact (62%) for pretreatment PSMA PET/CT in men with biochemical failure after RP (13). Ongoing follow-up at 3 y in this cohort has now highlighted the valuable predictive potential of PSMA PET in men with BCR managed with sRT. Men with either a negative PSMA PET result or a scan positive for disease confined to the fossa who underwent sRT had significantly higher 3-y FFP rates than men with either pelvic nodal or distant metastatic disease on PSMA PET. Furthermore, PSMA PET was found to be a significantly more powerful predictive indicator of 3-y FFP than established clinical predictors such as Gleason score, pathologic stage, surgical margin status, extracapsular extension, or PSA level at the time of sRT.
PSMA PET/CT is a sensitive technique for identifying sites of recurrence in the post-RP biochemical failure setting at low PSA levels (11,12,17,18). Most men with a PSA level of less than 1.0 ng/mL will have a positive PSMA PET result, with the detection rate of the scan dependent on PSA level at the time of imaging (12,17,19–22). Around half the men with a positive result will have disease beyond the fossa, a finding confirmed in this report. However, a significant proportion of men with PSA in the curative range for sRT will have a negative result (35% of our cohort). This study suggests that these men are excellent candidates for sRT, with the negative finding on PSMA PET being a more important predictor of long-term sRT control than risk factors such as PSA level, high Gleason score, high T stage, and positive surgical margin status. Further, this excellent treatment control in men with negative PSMA PET results is achieved despite the fact that treatment intensification via the use of more extensive sRT fields or adjuvant ADT was lower in this group than in men with positive PSMA PET findings.
Negative scan results in men who respond to fossa sRT are likely to represent a combination of low PSMA expression and low volume of disease at the time of imaging. That men with low PSMA expression do well with targeted therapy fits with our knowledge of the pathophysiology of the PSMA receptor in prostate cancer (23). The receptor plays a key role in glutamate cleavage and activation of growth pathways (phosphoinositide-3-kinase and protein Kinase B) in the cancer cell. High PSMA expression is known to equate to poor outcomes (24). It is likely that men with PSMA PET–positive disease occupy a biologically poorer prognostic category than those with negative scan results, with higher growth rates and metastatic potential in those demonstrating significant PSMA expression. It has previously been shown that men with a negative PSMA PET result do well with sRT, even in the presence of other high-risk indicators on the Stephenson nomogram (25) Although most men in this study with negative results who did not undergo sRT had a significant rise in PSA, 34% of these men had PSA levels that rose by less than 0.2 ng/mL over the 3 y, suggesting it may be possible to safely monitor a subgroup men with negative results. The predictive potential of PSMA PET in personalizing treatment regimens in BCR warrants further evaluation.
Two randomized trials have examined the role of treatment intensification in men with rising PSA after RP (4). Both studies predate PSMA PET imaging. The first randomized 743 men to either sRT alone or fossa sRT combined with 6 mo of ADT. That trial reported a 20% benefit in FFP (from 62% to 80%) at 5 y with the addition of ADT (GETUG16) (4). In the second study, a 3-arm multicenter randomized trial of 1,736 eligible men with rising PSA after RP, the 5-y FFP increased from 71% to 89% for fossa-alone sRT compared with fossa sRT plus pelvic node sRT plus 6 mo of ADT. That trial defined PSA progression as nadir plus 2 ng/mL, likely explaining the higher FFP rates than those in the current trial (26). Clearly, further prospective work is required to determine whether PSMA PET can help identify those men who will benefit from treatment intensification and those for whom it can safely be avoided.
The overall treatment response rate to sRT was lower in this study than in some reported studies. There are 2 likely reasons for this finding. First, the definition of FFP with a rise in PSA of more than 0.2 ng/mL is lower than in the recently reported studies, which used a PSA rise of more than 2 ng/mL. Pisansky et al. used a PSA of more than 0.2 ng/mL and found FFP rates (63.5% at 5 y) similar to those documented in the current study in over 1,000 men (5,27). Second, several patients with negative results or fossa-confined disease did not receive sRT over the 3 y of the study, with a significant rise in PSA in most of these men (mean PSA rise, 1.59 ng/mL). If these men had received sRT, we estimate the overall response rate to sRT would have been more than 70%.
At the time this prospective trial was commenced, the value of PSMA PET in the setting of biochemical failure after RP was poorly understood. Hence, it was appropriate in this trial that treatment decisions be documented but not dictated on the basis of the PSMA PET findings. Although treatment was not mandated and was left to the discretion of the treating radiation oncologist, men with positive pelvic nodes more frequently received pelvic nodal sRT and ADT than did men with negative scan results. This clearly reinforces our findings, as the predictive power of negative or fossa-confined PSMA PET results for FFP was not impacted by treatment intensification. Men with negative or fossa-confined PSMA PET results were more likely to received standard radiotherapy fields, without including the pelvic nodes, and were less likely to receive ADT.
This study prospectively recorded PSMA PET results using a standardized method across sites, with experienced prostate imagers. However, the study did not implement a double-read assessment to derive κ-scores or assess biopsies undertaken. These results have been documented for PSMA PET in other trials (11,28,29). We have previously undertaken a prospective trial in which histopathology was directly compared with PSMA PET results in men undergoing extended pelvic lymph node dissection. This study demonstrated a 62% sensitivity and 95% specificity for lymph nodal involvement on PSMA PET (29). Similarly, Fendler et al. recently reported an excellent PPV (84%) for PSMA PET based on a histopathology gold standard, giving good evidence for the diagnostic accuracy of the modality (11). The focus of this trial was to evaluate the outcomes of PSMA PET–triaged management based on the PET results conveyed to the treating clinician before treatment, which we believe is a more generalizable (and clinically relevant) scenario.
CONCLUSION
PSMA PET results are highly predictive of FFP at 3 y in men undergoing sRT for BCR after RP. In particular, men with negative PSMA PET results or disease identified as still confined to the prostatic fossa demonstrate high FFP despite receiving less extensive radiotherapy and lower rates of additional ADT than those with extrafossa disease.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: PSMA PET frequently changes management in men with BCR after RP, but does it improve longer-term outcomes and should its results dictate subsequent treatment choices?
PERTINENT FINDINGS: This prospective observational multicenter study found that PSMA PET results in 260 men with BCR after RP were highly predictive of freedom from failure at 3 y after sRT treatment.
IMPLICATIONS FOR PATIENT CARE: The study demonstrates the predictive value of PSMA PET in dictating which patients will most benefit from targeted radiation therapy and which patients will need further treatment intensification to control their disease.
Footnotes
Published online Nov. 1, 2019.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication August 11, 2019.
- Accepted for publication October 14, 2020.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Factors That Influence Repeat 68Ga-PSMA-11 PET/CT Scan Positivity in Patients with Recurrent Prostate Cancer Under Observation After a Negative 68Ga-PSMA-11 PET/CT Scan: A Single-Center Retrospective Study
- Utility of 64Cu-Sarcophagine-Bombesin PET/CT in Men with Biochemically Recurrent Prostate Cancer and Negative or Equivocal Findings on 68Ga-PSMA-11 PET/CT
- Differences in Failure-Free Survival After Salvage Radiotherapy Guided by Conventional Imaging Versus 18F-Fluciclovine PET/CT in Postprostatectomy Patients: A Post Hoc Substratification Analysis of the EMPIRE-1 Trial
- Feasibility of 99mTc-MIP-1404 for SPECT/CT Imaging and Subsequent PSMA-Radioguided Surgery in Early Biochemically Recurrent Prostate Cancer: A Case Series of 9 Patients
- The PRIMARY Score: Using Intraprostatic 68Ga-PSMA PET/CT Patterns to Optimize Prostate Cancer Diagnosis
- Role of Prostate-Specific Membrane Antigen PET in Metastatic Prostate Cancer: We Have the Answers
- Changes in Management After 18F-DCFPyL PSMA PET in Patients Undergoing Postprostatectomy Radiotherapy, with Early Biochemical Response Outcomes
- PSMA PET Validates Higher Rates of Metastatic Disease for European Association of Urology Biochemical Recurrence Risk Groups: An International Multicenter Study
- Appropriate Use Criteria for Prostate-Specific Membrane Antigen PET Imaging
- Salvage Radiotherapy Management Decisions in Postprostatectomy Patients with Recurrent Prostate Cancer Based on 18F-Fluciclovine PET/CT Guidance
- Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer
- Identification of PCWG3 Target Populations Is More Accurate and Reproducible with PSMA PET Than with Conventional Imaging: A Multicenter Retrospective Study
- PSMA-Ligand PET for Early Castration-Resistant Prostate Cancer: A Retrospective Single-Center Study