


Visual Abstract

Abstract
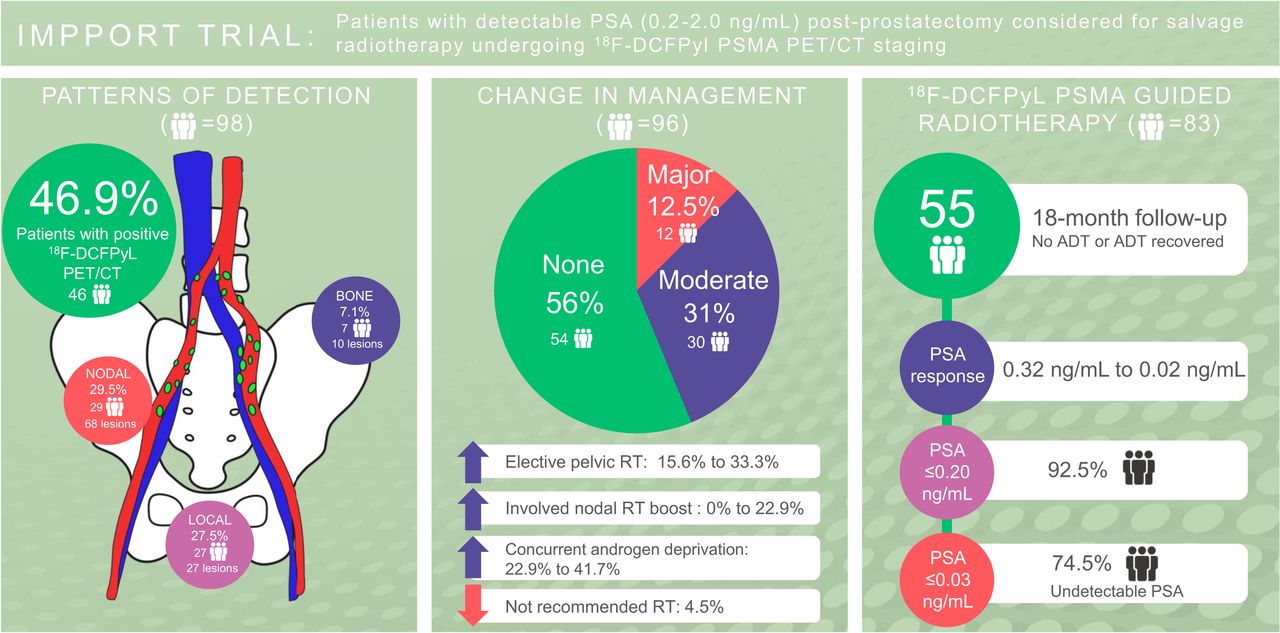
Prostate-specific membrane antigen (PSMA) tracers have increased sensitivity in the detection of prostate cancer, compared with conventional imaging. We assessed the management impact of 18F-DCFPyL PSMA PET/CT in patients with prostate-specific antigen (PSA) recurrence after radical prostatectomy (RP) and report early biochemical response in patients who underwent radiation treatment. Methods: One hundred patients were enrolled into a prospective study, with a prior RP for prostate cancer, a PSA of 0.2–2.0 ng/mL, and no prior treatment. All patients underwent diagnostic CT and PSMA PET/CT, and management intent was completed at 3 time points (original, post-CT, and post-PSMA) and compared. Patients who underwent radiotherapy with 6-mo PSA response data are presented. Results: Ninety-eight patients are reported, with a median PSA of 0.32 ng/mL (95% CI, 0.28–0.36), pT3a/b disease in 71.4%, and an International Society of Urological Pathology grade group of at least 3 in 59.2%. PSMA PET/CT detected disease in 46.9% of patients, compared with 15.5% using diagnostic CT (PSMA PET, 29.2% local recurrence and 29.6% pelvic nodal disease). A major change in management intent was higher after PSMA than after CT (12.5% vs. 3.2%, P = 0.010), as was a moderate change in intent (31.3% vs. 13.7%, P = 0.001). The most common change was an increase in the recommendation for elective pelvic radiation (from 15.6% to 33.3%), nodal boost (from 0% to 22.9%), and use of concurrent androgen deprivation therapy (ADT) (from 22.9% to 41.7%) from original to post-PSMA intent because of detection of nodal disease. Eighty-six patients underwent 18F-DCFPyL–guided radiotherapy. Fifty-five of 86 patients either did not receive ADT or recovered after ADT, with an 18-mo PSA response from 0.32 to 0.02 ng/mL; 94.5% of patients had a PSA of no more than 0.20 ng/mL, and 74.5% had a PSA of no more than 0.03 ng/mL. Conclusion: 18F-DCFPyL PET/CT has a significant impact on management intent in patients being considered for salvage radiotherapy after RP with PSA recurrence. Increased detection of disease, particularly in the pelvic lymph nodes, resulted in increased pelvic irradiation and concurrent ADT use. Early results in patients who are staged with 18F-DCFPyL PET/CT show a favorable PSA response.
Prostate-specific antigen (PSA) recurrence after radical prostatectomy (RP) for prostate cancer occurs in up to 20%–50% (1,2) and is defined by a PSA level of more than 0.2 ng/mL. Salvage radiotherapy, most commonly to the prostate bed, results in 5-y biochemical control of 56% (3). Failure after salvage radiotherapy is most likely due to disease outside the prostate bed, which can include the pelvic lymph nodes, paraaortic lymph nodes, and distant metastases.
PET using prostate-specific membrane antigen (PSMA) tracers have increased detection of disease compared with more conventional imaging with CT and bone scintigraphy. PSMA is a type II cell-surface glycoprotein overexpressed in more than 90% of prostate cancer epithelial cells (4). Various PSMA tracers are available, including 68Ga-PSMA-11, which has the most evidence for superior sensitivity in detecting disease. Newer PSMA tracers include 18F-labeled agents such as 18F-DCFPyL and have the advantages of increased manufacturing capacity, improved spatial resolution, and higher tumor-to-background ratio (5). PSMA PET/CT is now recommended in international guidelines as a staging method for biochemical failure when PSA is more than 0.2 ng/mL (6).
We aimed to evaluate the role of 18F-DCFPyL PET/CT in patients being considered for salvage radiotherapy, primarily assessing the change in management, and also reporting the early 6-mo biochemical response rate in patients who then undergo radiation therapy.
MATERIALS AND METHODS
We performed a prospective nonrandomized trial at 9 GenesisCare sites within Victoria, Australia. Between August 2018 and July 2020, we recruited 100 patients who had evidence of a rising PSA level of between 0.2 and 2.0 ng/mL after RP and were referred to a radiation oncologist for consideration of salvage radiotherapy. Exclusion criteria included previous pelvic radiotherapy and previous androgen deprivation therapy (ADT). The protocol was approved by the St. Vincent’s Hospital Melbourne Human Research Ethics Committee and was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12618001530213). All patients gave written informed consent.
All patients underwent diagnostic CT of the chest, abdomen, and pelvis and PSMA PET/CT on the same day at the Department of Nuclear Medicine of St. Vincent’s Hospital. Scans were performed on a Discovery 710 PET/CT device (GE Healthcare) combining a 64-slice multidetector CT scanner with a dedicated, full-ring PET scanner. For the diagnostic CT of the chest, abdomen, and pelvis, 100 mL of intravenous contrast medium were administered, and patients were scanned from the apex of the lungs to the lesser trochanters 70 s afterward. An additional 10-min delayed pelvic CT scan was also obtained to assist in distinguishing between the ureters and lymph nodes. For the PSMA PET/CT scan, 250 MBq of good-manufacturing-practice–quality 18F-DCFPyL manufactured by Cyclotek Australia was injected, followed by an uptake time of 120 min.
Imaging Acquisition and Interpretation
CT images of the chest, abdomen, and pelvis were interpreted by an experienced genitourinary radiologist, and PSMA PET/CT images were interpreted by 2 experienced nuclear medicine physicians. The reporting physicians did not have access to the images or reports of the other modality, except for the delayed pelvic CT scan to allow the nuclear medicine physician to localize the ureters and anastomosis on the PET images.
Both scans were reported using a standardized template that encompassed local, nodal, and distant disease, with each section being designated as positive, equivocal, or negative. Positive or equivocal disease was defined as focal uptake on PSMA PET/CT that was not physiologic and was higher than the surrounding background. Local recurrence was subclassified into prostate bed (including the anastomosis) or seminal vesicle bed (the bilateral rectovesical lateral areas on CT where soft-tissue densities are seen and where the seminal vesicles are usually located, with or without surgical clips). Lymph node involvement on CT of the chest, abdomen, and pelvis was defined on the basis of size and morphology and designated as positive, equivocal, or negative.
Changes in Management
After patient registration and before imaging, the radiation oncologist was required to outline the treatment plan on a questionnaire (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org), specifying whether radiotherapy or the proposed alternative management would be offered. If radiotherapy were to be offered, target-site dose and fractions needed to be specified, as well as whether pelvic nodal boost, stereotactic radiotherapy, and addition of ADT would be used. This treatment plan was referred to as the original intent, and after its completion, patients underwent diagnostic CT of the chest, abdomen, and pelvis and PSMA PET/CT. The diagnostic CT results were released first, and the clinician was required to complete a second questionnaire (post-CT intent). Then, the results of the PSMA PET/CT scan were released and the clinician completed a final questionnaire (post-PSMA intent). Change in management was graded on the basis of the impact on management and was defined as major, minor, or no change, as demonstrated in Table 1. This grading system was based on a publication by van Leeuwen et al. and further modified (7).
Impact of Changes in Management Intent
Radiotherapy and Disease Outcome
For this analysis, we assessed early biochemical response at 6 mo after the last day of radiotherapy and performed a subgroup analysis for patients who did not receive concurrent ADT. The radiotherapy protocol did not mandate the target volumes and dose prescription. However, clinical target volume guidelines for the prostate bed (8) and elective pelvic nodal irradiation (9) were provided; the recommendation was a dose of 70.2 Gy to the prostate bed, elective nodal irradiation of 56 Gy, and a nodal boost of 68 Gy in 39 fractions. Stereotactic radiotherapy to nodes or bone was recommended in 3–5 fractions with a dose range of 30–40 Gy. Concurrent ADT, if prescribed, was recommended using a luteinizing hormone–releasing agonist for 6 mo.
Statistical Methods
The McNemar exact test was used to compare changes in management between original intent and post-CT intent versus original intent and post-PSMA intent. The Kendall τ-b correlation was used to assess associations of change in intent with positive versus negative scan results (both CT and PSMA PET/CT), International Society of Urological Pathology (ISUP) grade, and pretreatment PSA. Statistical summaries were performed for patients undergoing radiotherapy with 6-mo PSA response data available. Particularly, for patients who did not receive ADT, we used t tests, ANOVA with multiple comparisons, and regression to compare differences and percentage changes between PSA at the 6-mo follow-up and prescan PSA across levels of several factors (PET scan positivity, pTN staging, ISUP grade, margin status, biochemical recurrence vs. persistence).
RESULTS
Between August 2018 and July 2020, 100 participants were enrolled across 9 sites by 6 radiation oncologists. Two patients were excluded on review because their prescan PSA level was outside the eligibility criteria (PSA ≥ 2.0), leaving 98 patients suitable for final analysis (Supplemental Fig. 1). A further 2 patients were excluded because of incomplete management intent forms, leaving 96 patients eligible for this analysis. Baseline characteristics (Supplemental Table 2) included a median age of 68.0 y, a median prescan PSA of 0.32 ng/mL (95% CI, 0.28–0.36 ng/mL); 58.9% had an ISUP grade group of at least 3 at RP. Biochemical recurrence occurred in 60.2% of patients, versus biochemical persistence in 39.8%. Pelvic nodal sampling or dissection was performed in only 32.7% of patients, with a median nodal count of 5.0 (95% CI, 4.1–7.9); 5.1% overall had pN1 disease. Histopathologic characteristics from RP revealed extraprostatic extension in 68.4%, seminal vesicle invasion in 24.5%, and a positive surgical margin in 37%.
Patterns of Disease Detection on PSMA PET/CT and Diagnostic CT of the Chest, Abdomen, and Pelvis
Overall, 46.9% (n = 46) of our cohort had positive PSMA PET/CT results, and a further 5.1% (n = 5) had equivocal results. The location of PSMA-avid disease is shown in Supplemental Table 3. Local disease recurrence was identified in 28 patients (29.2%), nodal disease in 29 patients (29.6%), and distant bony metastases in 7 patients (7.1%). One patient was unable to undergo the CT of the chest, abdomen, and pelvis, resulting in 97 available for analysis. Local recurrence was diagnosed in 9 patients (5 positive, 4 equivocal), nodal disease in 11 patients (9 positive, 2 equivocal), and an equivocal distant bone metastasis in 1 patient.
Changes in Management
Changes in treatment from original intent to postscan intent (post-CT and post-PSMA) are shown in Table 2. Overall, 43.8% (42/96) of patients demonstrated a change in management (major or moderate) after PSMA, versus 16.7% (16/95) after diagnostic CT of the chest, abdomen, and pelvis. There was a 12.5% versus 3.2% major change for post-PSMA versus post-CT, the difference being significant (P = 0.010). There were more patients with moderate changes after PSMA than after CT, 31.3% versus 13.7% (P = 0.001). Either a positive or an equivocal finding on CT or PSMA was strongly associated with a major or moderate treatment intent change (P < 0.001). Particularly for positive or equivocal PSMA findings, there were major or moderate changes in 42 of 50 patients (84%), compared with no changes in 46 patients with negative findings. Both higher PSA (P = 0.009) and higher ISUP grade (P < 0.001) were associated with higher likelihood of major or moderate changes in management after PSMA (Supplemental Fig. 2). Positive nodal disease findings on PSMA (nodal only or in combination) always resulted in a change in management (moderate or major) (Supplemental Table 4).
Change in Management Intent from Original to Post-CT Versus Post-PSMA
Changes in Management: Original Versus Post-CT Versus Post-PSMA
Changes in management after CT and PSMA are shown in Figure 1 and Supplemental Table 5. The original treatment intent was curative for most patients (94/96), with a minimal change after CT (92/95) and PSMA (92/95). The number of patients for whom radiotherapy was recommended was similar originally (n = 88), after CT (n = 87), and after PSMA (n = 88). Of these, prostate bed radiotherapy was recommended for almost all (original, n = 88; post-CT, n = 87; post-PSMA, n = 88). The largest effect from both CT and PSMA PET was an increased recommendation for elective pelvic radiotherapy, nodal boost, or concurrent ADT. Elective nodal irradiation increased to 20% (19/95) after CT and 33.3% (32/96) after PSMA, compared with 15 of 96 (15.6%) originally. Nodal boost was offered in more patients after PSMA, at 22.9% (22/96), versus 7.4% (7/95) after CT. Concurrent ADT use increased from 22.9% (22/96) originally to 24.2% (23/95) after CT and 41.7% (40/96) after PSMA. No stereotactic radiotherapy was recommended at original intent, with only small numbers of patients receiving a recommendation for stereotactic nodal irradiation (post-CT, n = 1; post-PSMA, n = 1) or stereotactic irradiation to bony metastases (post-CT, n = 1; post-PSMA, n = 4). There was only 1 patient with a change in dose (not fractions), with dose escalation of prostate bed PSMA-avid local recurrence (from 70.2 to 75.6 Gy).

Overall management intent at original (O) vs. post-CT (CT) vs. post-PSMA (PSMA). RT = radiotherapy.
Individual Changes in Management from Original Intent to Post-PSMA Intent
Figure 2 depicts the change in management flow for each patient between original intent and the post-PSMA scan. For most patients (61/96), prostate bed radiotherapy alone and after PSMA was originally recommended; 41 remained with the same recommendation (no change). In 19 patients, a change in radiotherapy treatment volume was recommended (moderate change); in 1 patient, a change to no radiotherapy was recommended (major change); and in 1 patient, additional stereotactic radiotherapy was recommended (major change). In the remaining 27 of 96 patients, the original intent was a recommendation for prostate bed radiotherapy, with ADT in 22 patients and elective pelvic radiotherapy in 15 patients. After PSMA, there were some changes in these 27 patients, with no consistent dominant change.

Sankey diagram demonstrating specific change in management per patient from original intent to post-PSMA scan, particularly for radiation target volumes. B = boost to node; PB = prostate bed; Pel = elective pelvic radiation; RT = radiotherapy; S = stereotactic radiotherapy.
Twelve patients had a major change in management after PSMA. Four of 8 changed from active surveillance originally to radiotherapy after PSMA. Four of 88 (4.5%) changed from radiotherapy originally to no radiotherapy after PSMA (ADT alone, n = 1; ADT plus chemotherapy, n = 2; surveillance, n = 1). Four of 88 patients received a recommendation that stereotactic radiotherapy be added to nodal or bone metastases.
Biochemical Response in Patients Undergoing Salvage Radiotherapy
In total, 86 patients received radiotherapy. Most received prostate bed radiotherapy only (50/86), and ADT was prescribed in 33 patients (6-mo duration) (Table 3). The median pretreatment PSA was 0.32 ng/mL (range, 0.20–1.84 ng/mL), and 59 patients had 18-mo posttreatment PSA response data with a median PSA of 0.02 ng/mL (range, 0.01–0.29 ng/mL).
Radiotherapy Treatment Volumes and Dose and Fractionations Delivered
Of the 59 patients with 18-mo follow-up data, 55 either had not received concurrent ADT or had ADT recovery. At the 18-mo follow-up, 52 of 54 (92.5%) had a PSA of no more than 0.20 ng/mL and 41 of 54 (74.5%) had an undetectable PSA (≤0.03), with no difference between a positive and negative PSMA scan.
DISCUSSION
Our prospective study showed that just under 50% of patients for whom salvage radiotherapy is planned because of PSA recurrence after RP have a change in management when undergoing 18F-DCFPyL PET/CT. The change in management was more than double that with diagnostic CT. There have been various studies demonstrating significant changes in management using 68Ga-PSMA-11 (10–12) and 18F-DCFPyL (13–15) in PET imaging for prostate cancer. Many of these studies were limited in that they enrolled heterogenous groups of patients, such as patients for whom PET was used for staging or for PSA failure; patients for whom prior treatment included surgery, radiotherapy, and ADT; and patients with a high prescan PSA. We postulate that the slightly lower management changes in our study are due to lower detection rates and a homogeneous post-RP cohort without prior treatment, with a lower pretreatment PSA (mean, 0.32 ng/mL), and with lower proportion of higher-grade disease (ISUP ≥ 4 was <20%).
We previously reported patterns of disease detection and the safety of 18F-DCFPyL PET/CT in our cohort (16) and provided a nomogram to predict a positive scan result. The improved detection of pelvic nodal disease was responsible for the moderate management change (31.3%) in our study, doubling the recommendation for pelvic nodal irradiation, nodal boost, and concurrent ADT with prostate bed radiotherapy. Many studies have shown that PSMA scans have improved the detection of disease after RP outside the prostate bed (10,11,17–19) which is not encompassed by standard salvage prostate bed radiotherapy volumes.
Major changes were small and occurred in only 12.5% (12/96) of patients after 18F-DCFPyL PET/CT. These were patients for whom radiotherapy was not recommended because of detection of metastatic disease, patients for whom surveillance was changed to treatment, and patients for whom stereotactic radiotherapy was added (node or bone). Improved detection of distant metastasis in the PSA recurrence setting can avoid radiotherapy toxicity and costs by omitting futile prostate bed radiotherapy, and the use of targeted radiotherapy to oligometastatic disease can improve progression-free survival (20) or delay the use of ADT (21). It important to recognize that there was no change in management in 56.3% of patients using 18F-DCFPyL PET/CT—a choice that was driven by a negative scan. The rate of positive versus negative scans in our study is similar to that of other studies in the post-RP PSA recurrence setting using 68Ga-PSMA-11 (22–24) and 18F-DCFPyL (15,25–29). The high negative scan rate raises questions regarding the additional role of elective nodal radiotherapy to prostate bed radiation, with trials supporting improved biochemical control (30,31).
With the impact on management change by 18F-DCFPyL staging, we have shown an early favorable PSA response in patients who then underwent radiotherapy. Of patients who had 18-mo response data available, who did not receive ADT, or who had ADT recovery, 92.5% had a PSA of less than 0.20 ng/mL and 74.5% had an undetectable PSA, with no difference in patients with a positive or negative scan. Previous studies have shown that using 68Ga-PSMA-11–guided salvage radiotherapy has favorable disease outcomes with similar follow-up (32,33). These studies, including ours, have shown that a negative PSMA scan is not associated with inferior response or outcomes, and we recommend salvage radiotherapy in patients with a negative PSMA scan. A recent randomized trial by Jani et al. showed that 18F-fluciclovine PET/CT–staged patients undergoing salvage radiotherapy have improved 3-y event survival compared with patients who were conventionally staged (34), and we await the results of a similar trial using 18F-DCFPyL (35).
Strengths of our study include the prospective design, with controlled high-compliance stepwise assessment of management intent change. Our eligibility criteria reflect a common scenario facing patients and clinicians with a rising PSA after RP: having had no prior therapy, with a PSA entry criterion of 0.2–2.0 ng/mL. Our study is relevant given that recent guidelines and trials support early referral for radiotherapy when PSA is more than 0.1–0.2 ng/mL (36–38). The limitations of our study include the lack of histopathologic or radiologic confirmation of disease, the fact that management change could vary at different institutions, and the limited follow-up. We will follow up patients until 3 y after radiotherapy to validate 18F-DCFPyL–staged radiotherapy. Another limitation is that our analysis of 18F-DCFPyL PET/CT scans did not use newer guidelines (PROMISE, PSMA-RADS, E-PSMA), which were not available at the time of protocol development; we will incorporate these in future trials.
CONCLUSION
18F-DCFPyL PET/CT has a significant impact on patients being considered for salvage radiotherapy. With improved detection of local recurrence and nodal disease, 18F-DCFPyL PET/CT improves confidence when irradiating the prostate bed and results in increased use of pelvic nodal irradiation. We recommend that PSMA PET/CT be considered for all patients for whom salvage radiotherapy is being considered after RP and for whom PSA is more than 0.2 ng/mL. Early results for 18F-DCFPyL–staged patients receiving radiotherapy show a favorable PSA response rate, but longer-term follow-up is needed.
DISCLOSURE
The sponsor, GenesisCare, along with Cyclotek (Aust.) Pty. Ltd., provided financial support and access to their good-manufacturing-practice–approved product, 18F-DCFPyL-PSMA radiopharmaceutical. Cyclotek provided support through a project grant from the Department of Industry, Science, Energy, and Resources Cooperative Research Centre Program. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How does improved detection of disease by 18F-DCFPyL PSMA PET change management in prostate cancer patients being considered for salvage radiotherapy because of PSA recurrence after prostatectomy?
PERTINENT FINDINGS: 18F-DCFPyL PSMA PET detected disease in 46.9% of patients, resulting in a major change in management in 12.5% and a moderate change in 31.3%; the greatest change was the increase in pelvic nodal irradiation.
IMPLICATIONS FOR PATIENT CARE: Increased detection of disease by PSMA PET allows better selection of patients for salvage radiotherapy, as well as selection of appropriate radiation fields for a favorable treatment response in patients who received PSMA-guided radiotherapy.
Footnotes
Published online Jan. 20, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 16, 2021.
- Revision received January 12, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.