


Abstract
The prostate-specific membrane antigen (PSMA) is highly expressed on most prostate cancer (PC) cells. Therefore, the targeting of PSMA has become increasingly important over the last decade. Glu-urea–based PSMA ligands used for both imaging and radioligand therapy are the mainstays of the current success. For PET imaging, both 68Ga- and 18F-labeled agents have been successfully translated to clinical applications. Mainly retrospective cohort studies have shown a high value in the setting of biochemical recurrence, with high detection rates even in the presence of low prostate-specific antigen levels. Preliminary data indicated that radioguided surgery with PSMA ligands may help to further improve patient outcomes because it facilitates the removal of small tumor deposits that are otherwise difficult to detect. For primary PC, PSMA ligand PET imaging has been shown to be superior to cross-sectional imaging for the detection of metastatic lymph nodes. In addition, it promises to also provide intraprostatic tumor localization, especially when used in combination with multiparametric MRI. Increasing numbers of studies have reported considerable changes in management resulting from PSMA ligand PET imaging for both biochemical recurrence and primary disease. The use of 177Lu-PSMA–based radioligand therapy has demonstrated a reasonable response, mainly as defined by a prostate-specific antigen response of more than 50%, comparable to other recently introduced agents. Especially given the high level of safety of 177Lu-PSMA radioligand therapy, with only minimal grade 3 and 4 toxicities reported so far, it has the potential to expand options for metastatic castration-resistant PC. This review is intended to provide a comprehensive overview of the current literature on low-molecular-weight PSMA ligands for both PET imaging and therapeutic approaches, with a focus on agents that have been clinically adopted.
Prostate cancer (PC) is the most common malignancy worldwide in men, with persistently high numbers dying from this disease (1,2). Imaging has increasingly been used over the last 2 decades to improve initial staging and help localize tumor deposits in recurrent disease. For instance, multiparametric MRI (mpMRI) has been shown to be effective in detecting or ruling out clinically significant disease, with a high negative predictive value of greater than 90% in various studies, and it can guide targeted biopsy (3,4). Primary staging by bone scanning and cross-sectional imaging, as recommended for high-risk disease, is hampered by a high percentage of lymph node (LN) metastases in nonenlarged LNs (pooled sensitivity, 39%–42%) (5,6).
Approximately 30%–40% of patients will fail primary treatment, and a rising prostate-specific antigen (PSA) level will herald the onset of biochemical recurrence (BCR) (7). After potential salvage procedures (radiation and surgery), patients usually undergo androgen deprivation therapy. This treatment is typically followed by an increase in the PSA level after 2–8 y; this increase indicates the onset of metastatic castration-resistant PC (mCRPC)—the lethal form of the disease (8). Reactivation of androgen receptor signaling occurs in early mCRPC; therefore, second-line agents targeting the androgen receptor signaling axis have extended survival in clinical trials (9,10). Treatment with other systemic agents, including taxane-based chemotherapy (e.g., docetaxel), sipuleucel-T, and the bone-seeking α-emitter 223Ra, has been shown to improve overall survival and quality of life (9,11–16). Nevertheless, patients with mCRPC have a poor prognosis and a median survival of 19 mo (17).
Molecular imaging has not played a major role until recently, as most PCs have only a low glycolytic rate, which limits the potential for 18F-FDG PET imaging (18,19). Further advances have been achieved with choline derivatives. At BCR, a pooled detection rate of 62% was reported for 11C-choline PET/CT, but the rates were significantly lower when the PSA levels were low (<1–2 ng/mL) (20). At primary staging, the pooled sensitivity of choline PET/CT for the detection of LN metastases was low (49.2%) in a recent metaanalysis (21). The results were similar when different choline-based agents were compared (22). The intraprostatic localization of primary disease is hampered by nonspecific uptake in benign changes (e.g., benign prostatic hyperplasia) (23). Notably, choline derivatives and 18F-FDG have shown potential in assessing the therapy response in mCRPC (24,25). Most recently, 1-amino-3-18F-fluorocyclobutane-1-carboxylic acid, an amino acid transport imaging agent, was approved by the U.S. Food and Drug Administration; however, its detection rate in recurrent PC is similar to those of choline derivatives (26,27).
UNMET CLINICAL NEEDS IN PC
Accurate staging in primary PC and localization of early BCR for tailoring initial and subsequent treatment strategies are unmet clinical needs. Once mCRPC is diagnosed, effective therapy for improving overall survival and quality of life is desperately needed. Prostate-specific membrane antigen (PSMA) ligands are currently being investigated intensively, as they hold promise for extending the frontier in PC imaging and radioligand therapy (RLT). This review is intended to deliver a comprehensive overview of current and past investigations of low-molecular-weight PSMA radioligands for PC imaging and therapy. Providing insights into past and promising current developments regarding PSMA antibody imaging, especially targeting J591, is beyond the scope of this review.
PSMA AS TARGET FOR PC IMAGING AND THERAPY
PSMA is a type II transmembrane glycoprotein. PSMA expression and localization in the normal human prostate are associated with the cytoplasm and apical side of the epithelium surrounding the prostatic ducts (28). PSMA is enzymatically active only in its dimeric form, but its function for prostate cells is still unknown (29). Dysplastic and neoplastic transformation of prostate tissue results in the transfer of PSMA from the apical membrane to the luminal surface of the ducts (30,31). For several reasons, PSMA is an ideal target in PC.
First, it is significantly overexpressed (100–1,000 fold) on nearly all PC cells (32–35), although 5%–10% of primary PC or PC lesions had negative PSMA results on PET (36,37). However, the underlying etiology of PC with negative PSMA results on PET is still unclear, given the lack of prospective studies and correlation with immunohistochemistry.
Second, its expression is further increased in advanced stages and in mCRPC (32,34,38).
Third, after binding to the active center of the extracellular domain, PSMA ligands are internalized. Subsequent endosomal recycling increases the deposition, leading to enhanced tumor uptake, retention, and subsequent high image quality for diagnostic procedures and a high local dose for therapeutic applications (29,39,40).
Preclinical data showed that PSMA expression is independent of the use of taxane-based chemotherapy. This property may allow direct PC imaging—an advantage over bone scintigraphy and CT imaging—without the “flare phenomenon” (41). However, gene transcription analysis demonstrated that androgen can suppress the promoter of the PSMA gene (42,43). Therefore, the initiation of androgen deprivation therapy induces early but temporary upregulation of PSMA expression, downregulation under prolonged androgen deprivation therapy and, finally, overexpression of PSMA in androgen-resistant tumors (44–47). A preliminary work outlined this effect, which could be leveraged for improved diagnosis and therapy (48).
Interestingly, PSMA expression in the tumor neovasculature of some solid tumors (colon, breast, kidney, and subtypes of bladder cancer) poses potential pitfalls in imaging (32,49–54) but also offers potential opportunities for theranostic applications in cancers other than PC.
COMPREHENSIVE OVERVIEW OF DIFFERENT CLASSES OF PSMA LIGANDS IN CLINICAL USE
To date, no PSMA small molecule has been approved by the U.S. Food and Drug Administration or European Medicines Agency. The only approved agent targets the intracellular domain (7E11) of PSMA: the radiolabeled anti-PSMA antibody capromab pendetide (ProstaScint; EUSA Pharma) (35). Binding of the relatively large antibody to the intracellular domain of PSMA leads to false-positive findings after successful radiotherapy and very low rates of detection of viable tumor lesions (55).
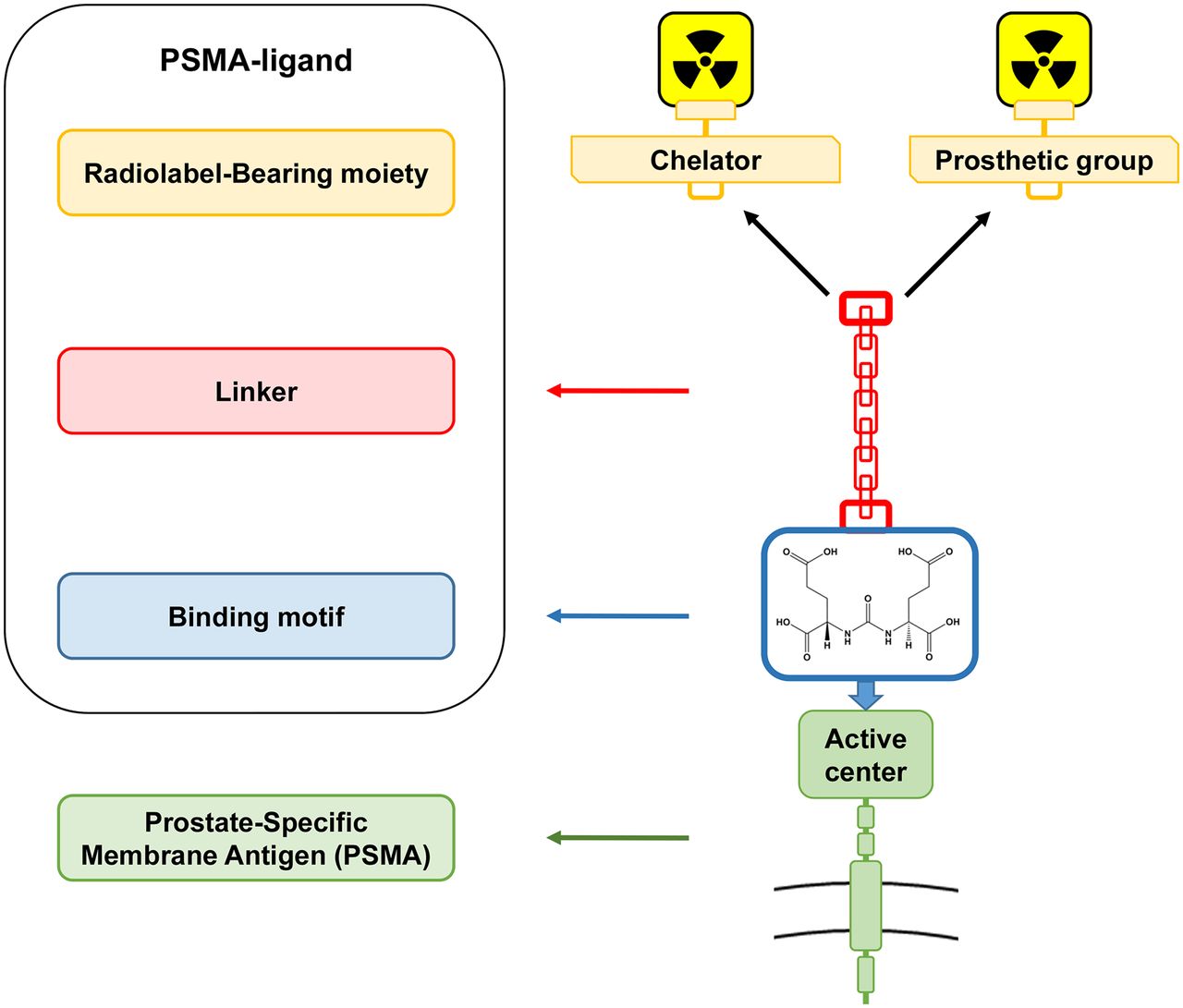
In contrast, small-molecule PSMA ligands are relatively small peptide mimetic agents that are usually cleared rapidly from the circulation, leading to low background activities early after injection. The recognition of the structural and functional homology between N-acetyl-L-aspartyl-L-glutamate peptidase I and PSMA supported the development of these small molecules (56). The first class of PSMA-targeting radiopharmaceuticals based on phosphorous esters failed in early clinical translation (57). Other promising lead structures, such as carbamates, are still in preclinical evaluation (58). The focus of this review is the clinically most advanced category, the urea-based PSMA ligands, which usually consist of 3 components: the binding motif (glutamate-urea-lysine [Glu-urea-Lys] is the most widely used scaffold), a linker, and a radiolabel-bearing moiety (chelator molecule for radiolabeling or a prosthetic group for fluorinated agents) (Fig. 1).
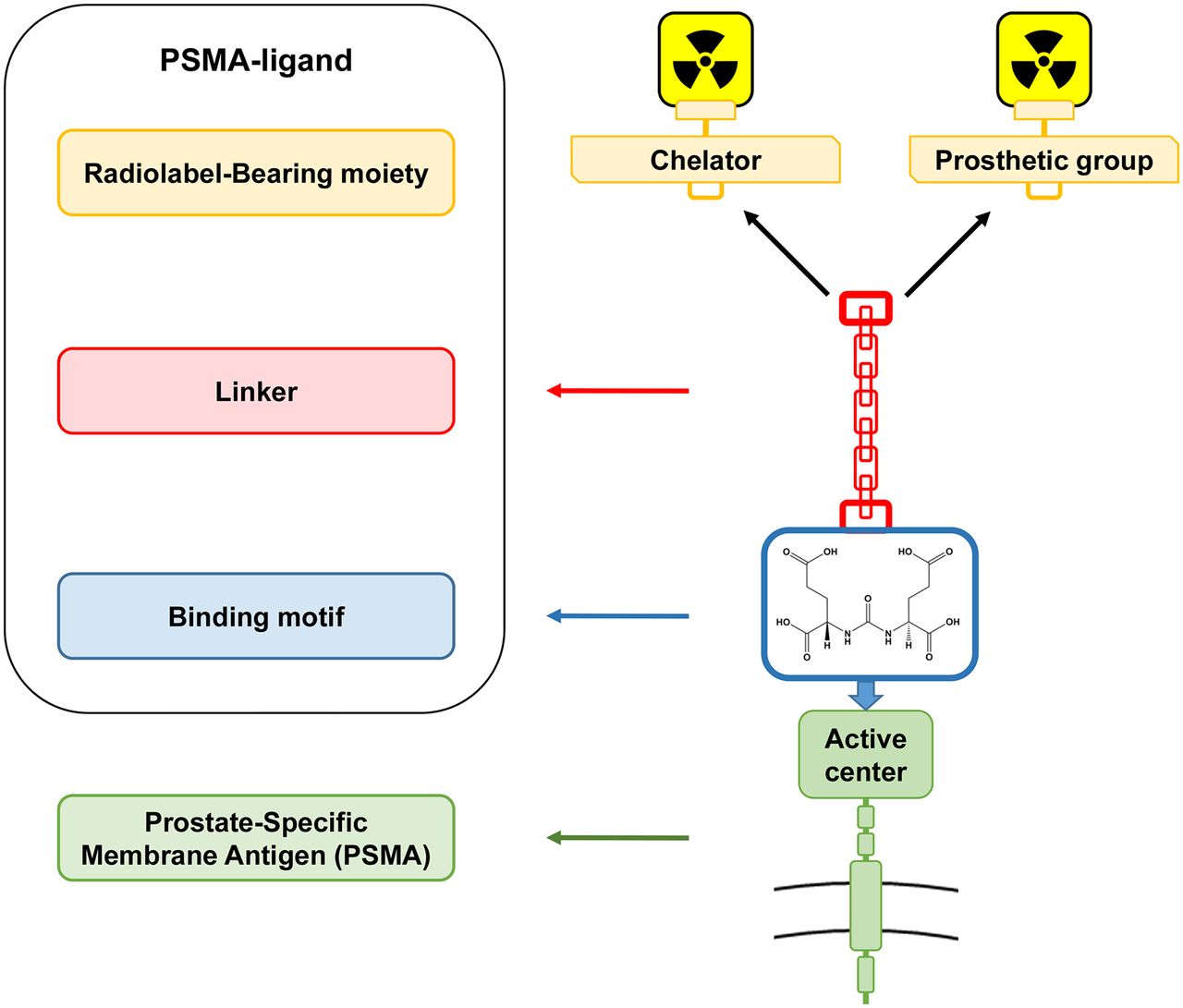
Structural components of urea-based PSMA ligands.
Several of these agents have already been translated to clinical applications. Recent reviews described in detail the history and different characteristics of a broad spectrum of PSMA ligands, which is beyond the scope of this review (59–61). Table 1 provides an overview of the most commonly used low-molecular-weight PSMA ligands.
Overview of Most Commonly Used Glu-Urea–Based PSMA Ligands
123I-MIP-1072 and 123I-MIP-1095 (62), the first agents, were followed by 99mTc-MIP-1404 and 99mTc-MIP-1405 (41) for SPECT imaging in clinical trials. N-[N-[(S)-1,3-dicarboxypropyl]carbamoyl]-4-18F-fluorobenzyl-l-cysteine (18F-DCFBC) (63) and 68Ga-PSMA-11 (68Ga-PSMA–N,N′-bis-[2-hydroxy-5-(carboxyethyl)benzyl]ethylenediamine-N,N′-diacetic acid) (64) were the first agents for PET imaging. Initial therapeutic studies conducted with 131I-MIP-1095 (65) were soon followed by the introduction of chelator-based PSMA-617 (66) and another PSMA inhibitor for imaging and therapy, PSMA-I&T (67), which are theranostic agents capable of being labeled with PET, SPECT, or therapeutic radionuclides. 18F-labeled agents exploit an average lower positron energy leading to a higher intrinsic spatial resolution. Although 18F-DCFBC had persistently high blood-pool activity and relatively low tumor-to-background ratios, a second-generation, 18F-labeled, small-molecule urea derivative known as 2-(3-{1-carboxy-5-[(6-18F-fluoro-pyridine-3-carbonyl)-amino]-pentyl}-ureido)-pentanedioic acid (18F-DCFPyL) overcame these limitations (68). Most recently, 18F-PSMA-1007 (69) was introduced as another 18F-labeled agent exploiting very low urine clearance and potentially facilitating improved evaluation of the prostatic bed. 18F-labeled agents also offer a longer half-life and potentially easier centralized production and distribution than 68Ga-labeled compounds (70). With a 99mTc-labeled PSMA for imaging and surgery, an alternative to the use of 111In for PSMA ligand–guided surgery is now available and may allow fast, convenient, kitlike labeling (71).
PSMA LIGAND IMAGING
Biochemical Recurrence
68Ga-Labeled PSMA Ligands
Since the initial report from 2012 (72), the most extensive experience with PSMA ligand PET imaging has been obtained for BCR. A recent metaanalysis based mainly on retrospective series summarized data for 68Ga-PSMA-11 (73). Ten single, yet partially substantial, studies resulted in pooled detection rates of 58% and 76% for PSA levels of 0.2–1 and 1–2 ng/mL, respectively (Figs. 2 and 3). The largest retrospective series of 319 patients (24 without prior definitive treatment) reported a detection rate of 88.1% on a per-patient basis (74). For lesions with histologic proof, a sensitivity of 76.6% and a specificity of 100% were demonstrated. In another study (75), a pooled detection rate of 89.5% was demonstrated for a homogeneous cohort of 248 patients after radical prostatectomy. Detection rates for early BCR at PSA levels of 0.2–0.5 and 0.5–1 ng/mL were 57.9% and 72.7%, respectively. In both studies, tumor detection was positively associated with PSA level but not with PSA doubling time.
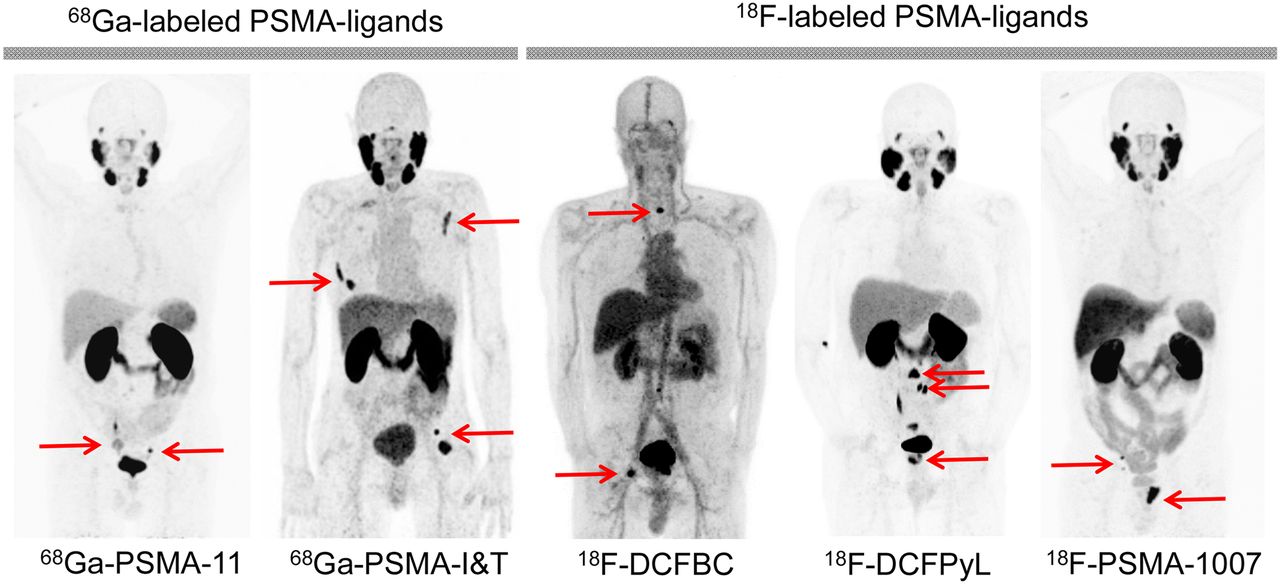
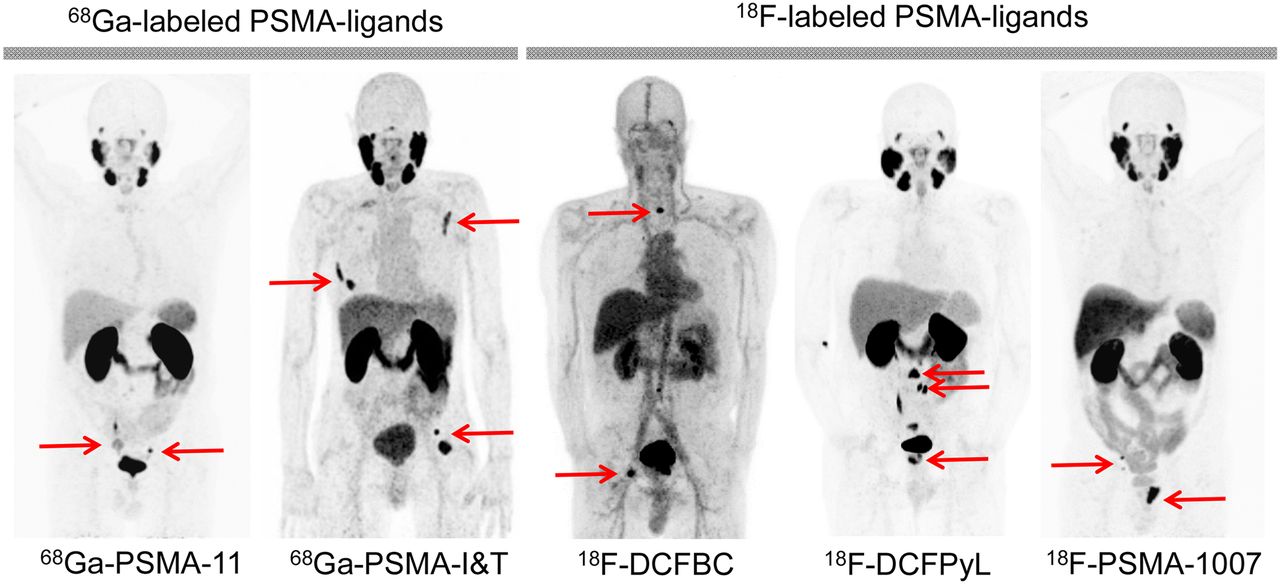
Maximum-intensity-projection images of PSMA ligands most commonly used for PET imaging (68Ga- and 18F-labeled agents). Images were acquired at different centers and show typical biodistribution as well as different numbers of positive lesions, depending on extent of disease in respective patients. Specific tumor uptake is indicated by red arrows.
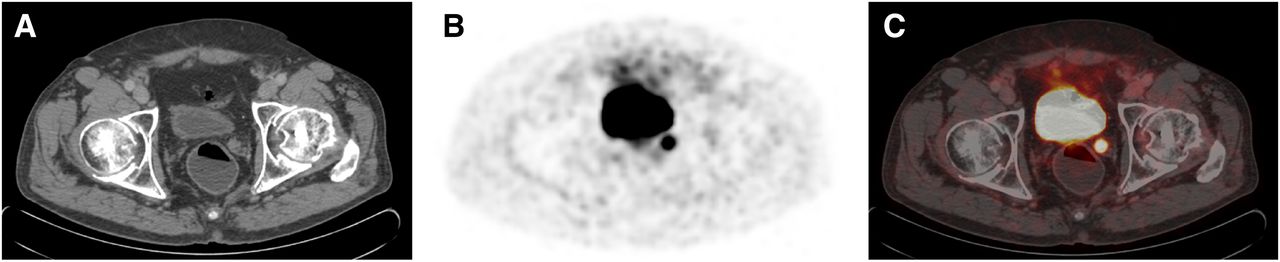
76-y-old patient with BCR (PSA of 0.4 ng/mL) after radical prostatectomy (initial stage, pT2c pN0 G2; Gleason score of 7b). Patient was referred for 68Ga-PSMA-11 PET/CT for restaging. 68Ga-PSMA-11 PET/CT showed local recurrence in left seminal vesicle bed. (A) Transaxial CT. (B) Transaxial PET. (C) Transaxial fused PET/CT.
In contrast, however, Ceci et al. (76) analyzed 39 patients with a PSA level of less than 2 ng/mL and reported a strong relationship with PSA doubling time: The detection rates were 85% for a PSA doubling time of less than 6.5 mo but only 19% for a PSA doubling time of greater than 6.5 mo. For 68Ga-PSMA-I&T, an initial study (77) reported detection rates of 52% for a PSA level of less than 0.5 ng/mL, 55% for 0.5–1.0 ng/mL, 70% for 1.0–2.0 ng/mL, and 93% for 2.0–5.0 ng/mL; these results were relatively comparable to those for 68Ga-PSMA-11, although they were limited by the small number of patients (n = 83).
Several studies demonstrated the superiority of 68Ga-PSMA-11 over choline derivatives for PET/CT in a head-to-head comparison of patients with BCR (78–80). Afshar-Oromieh et al. detected PC in 32 of 37 BCR patients (86.5%) with 68Ga-PSMA-11 but in only 26 of 37 patients (70.3%) with 18F-fluorocholine (80). Both the SUVmax and tumor-to-background ratios were superior for 68Ga-PSMA-11 in most lesions (79% and 95%, respectively). In a study by Morigi et al., 14 of 26 patients (53.8%) had positive results only in 68Ga-PSMA-11 PET/CT, 1 patient (4%) had positive results only in 18F-fluoromethylcholine PET/CT, and the remaining patients were diagnosed by consensus in both investigations (78).
There is increasing evidence that a patient’s prognosis is improved by the initiation of salvage therapy before the PSA level exceeds 0.5 ng/mL (17). For such patients, the rate of detection by 68Ga-PSMA-11 PET/CT in various studies was reported to be between 50.0% and 57.9% (74,75,78,81)—higher than for any other imaging modality. Thus, 68Ga-PSMA-11 PET/CT potentially allows for more effective salvage treatment, including radiotherapy with focal boost and salvage node dissection. Further evidence is needed to ascertain whether this treatment improves patient outcomes, but modifying management rather than administering blind radiotherapy to the prostate bed in patients with occult extraprostatic disease identified by PSMA PET/CT is a logical approach.
18F-Labeled PSMA Ligands
A first-in-man study of 18F-DCFBC in 5 patients with metastatic disease revealed favorable dosimetry and biodistribution for the detection of PC (63). In addition, putative sites of occult disease on conventional imaging were detected. A small prospective study of 17 patients with known progressive metastatic PC (both patients with hormone-naive disease and those with castration-resistant disease) demonstrated the superiority of 18F-DCFBC PET/CT over conventional imaging with CT and bone scanning for lesion detection (82).
A first-in-man analysis of 18F-DCFPyL in 9 patients with known metastatic PC determined favorable dosimetry, biodistribution, and safety (83). Subsequent analyses demonstrated markedly increased lesion detection efficiency relative to that of conventional imaging (84). In a head-to-head comparison of 14 selected patients who underwent 18F-DCFPyL PET/CT after 68Ga-PSMA-11 PET/CT because of negative or inconclusive findings, 18F-DCFPyL PET/CT revealed additional lesions in 3 of 14 patients (21.4%) (85). In addition, the mean SUVmax in concordant 18F-DCFPyL PSMA–positive lesions was significantly higher than that obtained with 68Ga-PSMA-11 (14.5 vs. 12.2; P = 0.028; n = 15). In a follow-up study by this group, PSA-stratified detection rates in different patients (n = 62 with 18F-DCFPyL and n = 129 with 68Ga-PSMA-11) were compared (86). These initial data in a limited number of patients suggested that 18F-DCFPyL was not inferior to 68Ga-PSMA-11 and indicated that imaging with 18F-DCFPyL might even exhibit improved sensitivity in localizing relapsed tumors after prostatectomy for moderately increased PSA levels. However, further conclusions are difficult to draw because of the different patient populations, administered activities, and PET acquisition techniques.
The potential of 18F-PSMA-1007 to detected morphologically occult disease was demonstrated in a recent case report (87). Lesions had an SUVmedian and an SUVmax of 7.7 and 18.8, respectively.
PSMA Ligands for SPECT Imaging
Only a few studies have investigated the use of SPECT agents in recurrent PC. An initial study of 99mTc-MIP-1404 in 6 healthy men and 6 patients with radiographic evidence of metastatic PC showed favorable biodistribution, identified most bone metastases (compared with bone scintigraphy), and detected soft-tissue PC lesions, including subcentimeter LNs (88). Subsequently, in an evaluation of 99mTc-MIP-1404 in 60 patients, the detection rates at PSA levels of greater than 2 ng/mL and less than or equal to 2 ng/mL were 91.4% and 40.0%, respectively (89). A direct comparison of 111In-PSMA-I&T and 68Ga-PSMA-11 in patients with early recurrence clearly showed a lower detection rate for 111In-PSMA-I&T (90). Only 14 of 29 lesions with PET-positive results (48.3%) were visualized by 111In-PSMA I&T.
Impact on Clinical Decisions
Evidence that PSMA ligand PET imaging significantly affects management in patients with early BCR is increasing. In a homogeneous cohort of 70 patients who had a PSA level of less than 1 ng/mL and were potential candidates for salvage radiation treatment, 68Ga-PSMA-11 PET/CT led to a major change in management (disease in LN or bone not covered by the conventional radiation therapy field) for 28.6% of patients (81). In an additional 26% of patients, the disease was confined to the prostate bed, possibly defining these patients as optimal candidates for salvage radiation therapy. Morigi et al. prospectively evaluated the impact on management of 68Ga-PSMA-11 in patients with BCR and prior 18F-fluorocholine treatment; they demonstrated a major impact in approximately one-third of patients, especially those with a low PSA level (78). Two other studies reported similar results (91,92). Data are limited in patients with metastatic disease. The potential of PSMA PET/CT to stratify and monitor advanced disease is unclear (Fig. 4). A preliminary report indicated that 68Ga-PSMA-11 might be a useful gatekeeper before 223Ra-dichloride therapy (93).
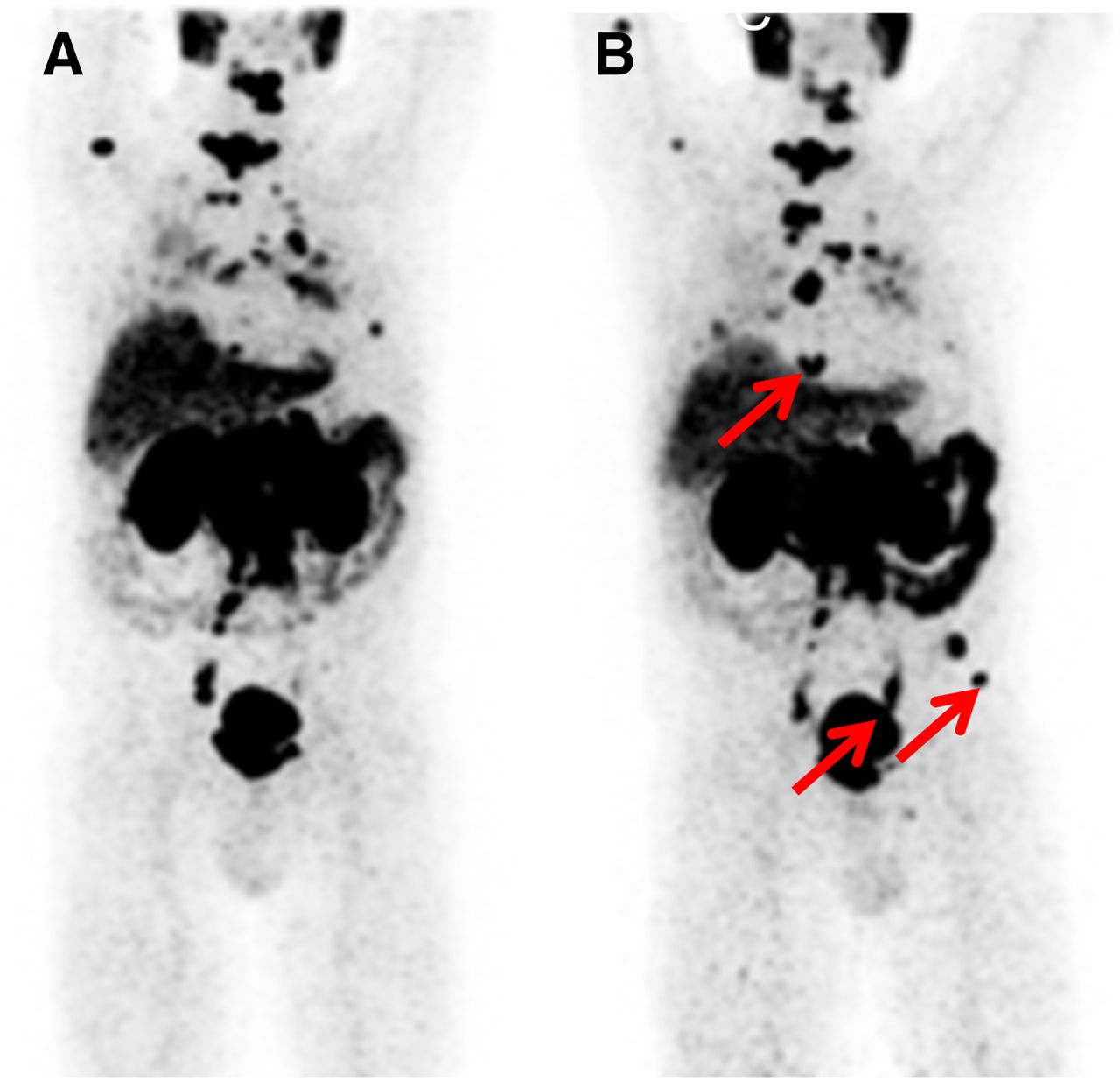
73-y-old patient with mCRPC (Gleason score of 9). Patient received systemic treatment and was referred for 68Ga PSMA-11 PET/CT before and after docetaxel chemotherapy for therapy response assessment. (A) Baseline PET/CT revealed PSMA-positive disseminated bone, nodal, and lung metastases (maximum-intensity projection [MIP]). (B) Follow-up PET/CT showed mixed response, with evidence of new metastases (red arrows) (MIP). Accordingly, PSA level increased from 343 ng/mL at baseline to 455 ng/mL at follow-up.
Primary Staging
68Ga-Labeled PSMA Ligands
Several studies have focused on the accuracy of 68Ga-PSMA-11 PET/CT for primary LN staging (Fig. 5). In a retrospective analysis of 130 consecutive patients with primary intermediate- to high-risk PC and subsequent template-based pelvic LN dissection, 68Ga-PSMA-11 PET outperformed cross-sectional imaging at the patient and template levels (P = 0.002 and P < 0.001, respectively). Reported values for the sensitivity of 68Ga-PSMA-11 PET/CT versus conventional imaging were 65.9% versus 43.9%, respectively, at the patient level and 68.3% versus 27.3%, respectively, at the template level. Moreover, 68Ga-PSMA-11 PET had a high specificity—greater than 95%. Nine patients with LNs found positive by histopathology but negative by 68Ga-PSMA-11 PET harbored only micrometastases in single LNs (mean size of negative LNs, 3 mm). Impaired detection of LN metastases smaller than 5 mm was anticipated and was also reported by other groups with similar results for the overall performance of 68Ga-PSMA-11 PET for node staging (81,94,95).
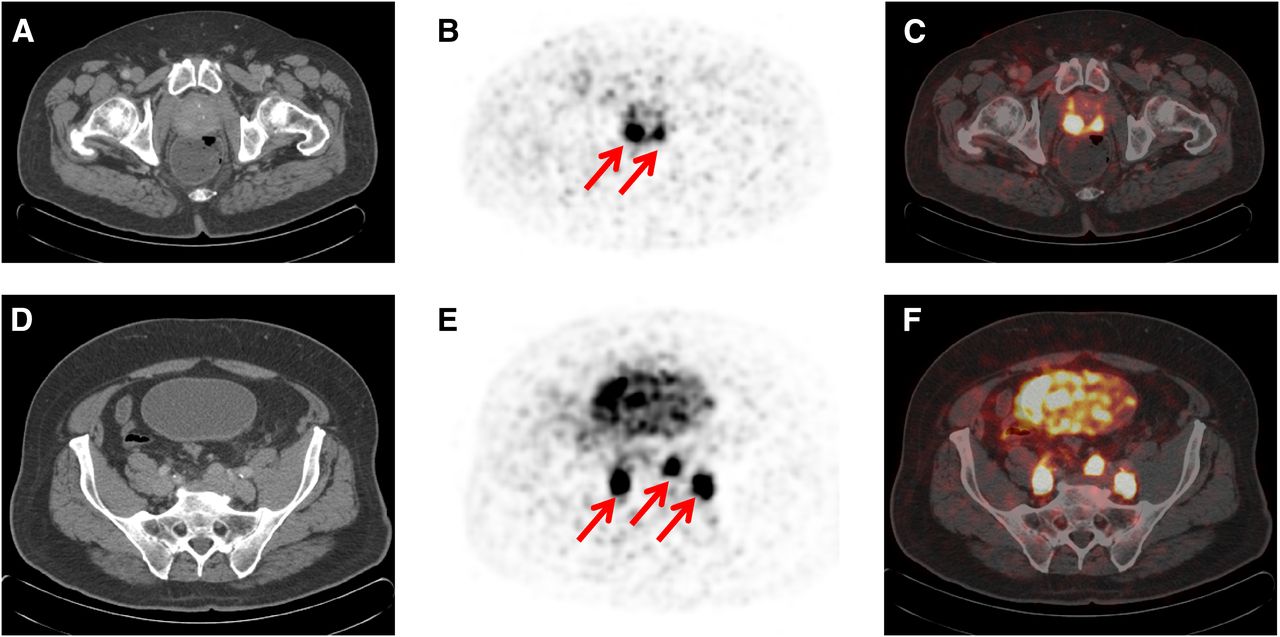
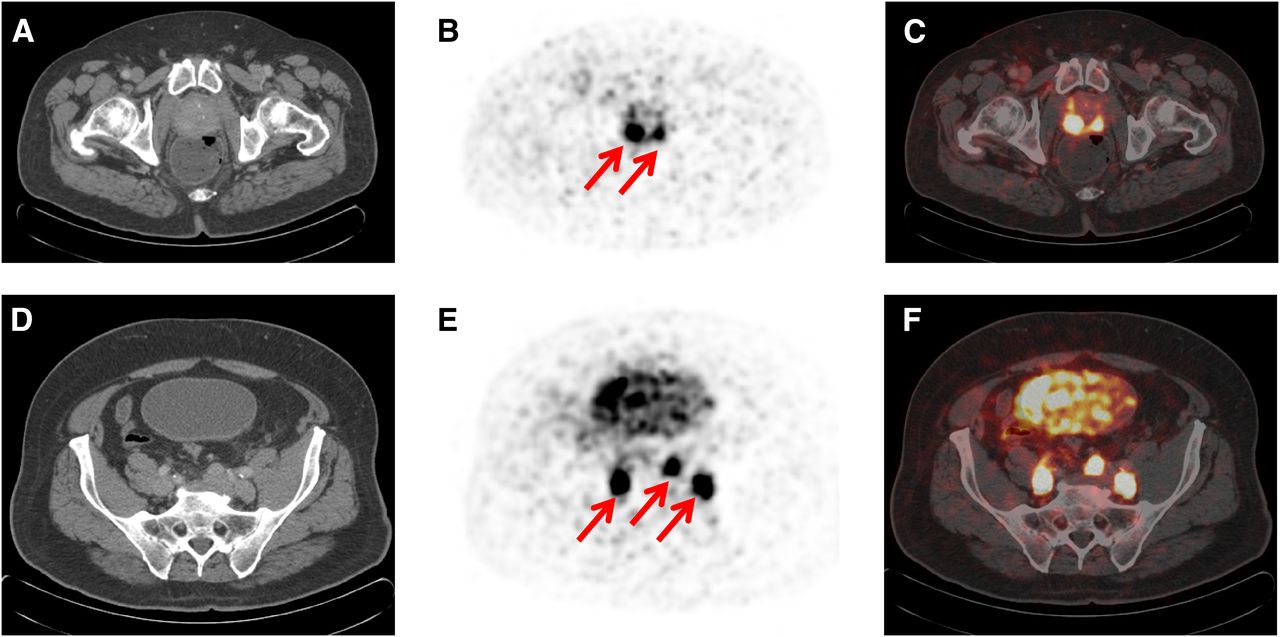
70-y-old patient with biopsy-proven high-risk PC (Gleason score of 9; PSA of 94 ng/mL). Patient was referred for 68Ga-PSMA-11 PET/CT for primary staging. 68Ga-PSMA-11 PET/CT showed PSMA-positive primary tumor (red arrows) (transaxial CT [A], PET [B], and fused PET/CT [C]) and pelvic LN involvement on both sides (red arrows) (transaxial CT [D], PET [E], and fused PET/CT [F]).
For the identification of bone metastases, 68Ga-PSMA-11 PET was clearly superior to bone scanning in a preliminary comparison that also explored primary PC on both per-patient and per-region bases (P = 0.006 and P < 0.0001, respectively) (96). A prospective phase 3 multicenter trial comparing 68Ga-PSMA-11 PET with conventional imaging (CT and bone scanning) in men with newly diagnosed Gleason grade group 3 to 5 PC is currently under way (ANZCTR 12617000005358).
Increasing numbers of studies have investigated the potential of 68Ga-PSMA-11 for intraprostatic tumor localization (97–102). For example, on the basis of a 6-segment model per slice, histopathologically positive segments (n = 100 in 21 patients) had significantly higher 68Ga-PSMA-11 uptake than negative segments (SUVmax, 11.8 vs. 4.9), suggesting an SUVmax of 6.5 as an optimal discriminator (sensitivity of 67% and specificity of 92% for the detection of tumor-involved segments) (97). Other retrospective studies investigating 6 and 9 patients and using segment and voxelwise approaches reported similar results (98,101).
68Ga-PSMA-11 PET was compared head-to-head with mpMRI, the current standard method for intraprostatic tumor localization, in several studies. Giesel et al. analyzed the concordance between the methods (102). The nearly total agreements between positive findings on one modality and a positive correlate on the other were 89.4% for mpMRI and 96.8% for 68Ga-PSMA-11 PET; these results indicated a potential benefit of a combination of the methods for tumor detection. The use of combined 68Ga-PSMA-11 PET/MRI was analyzed in 53 patients with intermediate- and high-risk PC (99). In a sextant-based analysis of the whole prostate gland, a higher accuracy was found for combined mpMRI and 68Ga-PSMA-11 PET. Sensitivities and specificities were 76% and 97%, respectively, for hybrid 68Ga-PSMA-11 PET/MRI; 58% and 82%, respectively, for mpMRI (P = 0.003); and 64% and 94%, respectively, for 68Ga-PSMA-11 PET. Potential implications include improvement of biopsy guidance or radiation treatment planning.
Zamboglou et al. investigated the gross tumor volume based on mpMRI, 68Ga-PSMA-11 PET, and the combination in 7 patients (101). The gross tumor volume based on PET plus mpMRI had a significantly higher overlap (57% ± 22% [mean ± SD]) than did the gross tumor volume based on mpMRI alone (42% ± 18%) or 68Ga-PSMA PET alone (45% ± 24%) when the data were validated by histopathology. Interestingly, each lesion with the highest uptake in PET corresponded to the lesion with the highest diffusion restriction (lowest apparent diffusion coefficient) in mpMRI.
18F-Labeled PSMA Ligands
In a study of 13 patients who underwent 18F-DCFBC PET/CT before prostatectomy, 12 had contemporaneous pelvic MRI for comparison (103). Although the sensitivity of MRI was superior to that of 18F-DCFBC PET/CT imaging in this cohort, 18F-DCFBC PET/CT had a high specificity for the most clinically significant high–Gleason score and high-volume tumors. Furthermore, a correlation between the degree of radiotracer uptake and the Gleason score of the dominant tumor was noted, although the small number of patients contributed to wide confidence intervals (103)—in contrast to a larger patient cohort imaged with 68Ga-PSMA-11 (99). Unlike the results obtained with many non-PSMA-targeted radiotracers, foci of benign prostatic hyperplasia were photopenic when imaged with 18F-DCFBC PET/CT (103). Preliminary data for 18F-PSMA-1007 indicated a high accuracy for the detection of nodal involvement in primary disease (69). Most affected LNs (18/19 LN metastases in a total of 309 resected LNs), including nodes as small as 1 mm in diameter, were identified correctly.
PSMA Ligands for SPECT Imaging
In a phase 2 clinical trial, 99mTc-MIP-1404 had a sensitivity of 94% and a specificity of 100% for the detection of primary PC in a preselected high-risk population. Its clinical impact is currently being evaluated in a prospective phase 3 clinical trial (ClinicalTrials.gov identifier: NCT02615067).
Impact on Clinical Decisions
The decision to use primary radiotherapy or radical prostatectomy either with or without extended pelvic lymphadenectomy or radiation of lymphatic drainage is challenging and depends mainly on patient as well as pretherapeutic tumor characteristics. Current approaches use epidemiological data to pretherapeutically estimate the baseline risk for disease-positive nodes (104,105). In a recent publication, 68Ga-PSMA-11 PET/CT and standard-of-care imaging (including bone scanning, CT, and MRI) were performed in 57 patients for primary radiotherapy. Imaging led to modifications in 50.8% of patients (91). The specific impact of 68Ga-PSMA-11 PET on planning for local radiation was also indicated in a study involving mpMRI comparison. Besides a 47% concordance of PET and mpMRI for identifying the dominant intraprostatic lesion at the patient level, the PET-based gross tumor volume was significantly larger (106).
PSMA LIGAND–BASED THERAPEUTIC APPLICATIONS
Radionuclide Therapy
The radiolabeled anti-PSMA antibody 177Lu-J591, which targets the extracellular domain of PSMA, resulted in any PSA decline in 60% of 47 patients included in the study; however, only 11% experienced a decline in the PSA level of greater than 50%, and treatment was limited by hematologic toxicity, with grade 4 thrombocytopenia occurring in 47% (107). The slow diffusion of antibodies into solid lesions, with an uptake maximum at 6 or 7 d after injection, and hematotoxicity caused by a long circulation time in blood are significant limitations of radiolabeled antibody therapy (108). Small-molecule PSMA ligands for endoradiotherapy were first used by Zechmann et al., who treated 28 mCRPC patients with a single therapeutic dose of 131I-MIP-1095 (mean activity, 4.8 GBq; range, 2–7.2 GBq) (65). The retention of 131I-MIP-1095 in lesions was visualized up to 17 d after a single dose, and considerable symptom relief and a decline in the serum PSA level of greater than 50% were noted in more than half of the patients.
Safety and Efficacy of 177Lu-Labeled PSMA Ligands
177Lu offers several advantages over 131I, such as easier distribution to therapy centers (less heavy shielding needed because of the lower β-particle energy: 133 vs. 182 keV), easier radiolabeling, and a lower proportion of γ-radiation—potentially resulting in reduced hospital admission times and lower toxicity (109). The German Society of Nuclear Medicine recently published a consensus recommendation on the use of 177Lu-PSMA-617 in mCRPC patients (110). Most retrospective case series for PSMA-targeted RLT involved 177Lu-PSMA-617 (111–115). Most studies showed a decrease in the PSA level of greater than or equal to 50% in 30%–60% of mCRPC patients (Fig. 6). Side effects seemed to be relatively mild, with only a few cases of grade 3 and no grade 4 nonhematologic toxicity being reported. However, long-term results regarding potential toxicities to the salivary glands and kidneys, given the high levels of physiologic accumulation, are still pending.

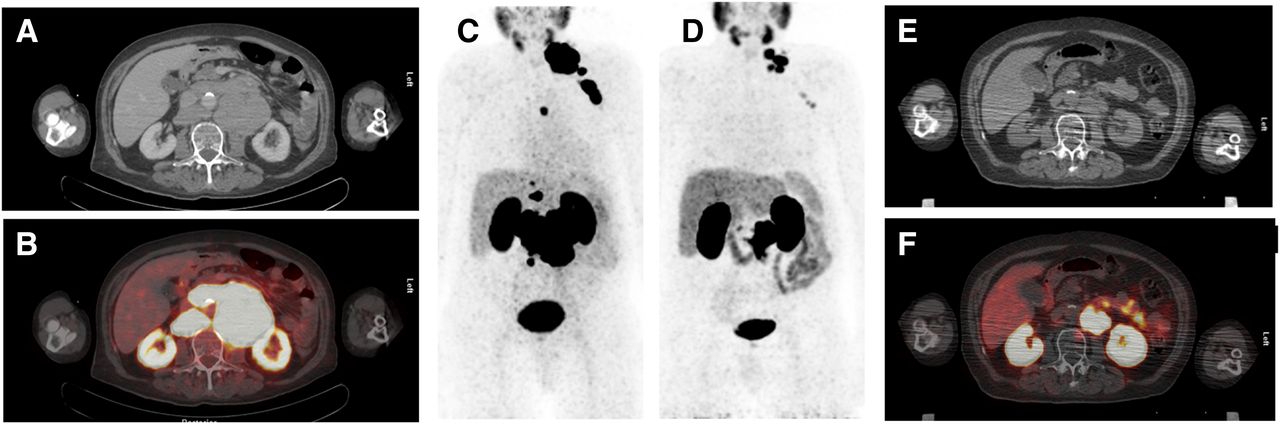
77-y-old patient with mCRPC (initial stage, cT3a cN1 cM0 G2b; Gleason score of 7a) before (A–C) and after (D–F) 177Lu-PSMA-617 RLT. Patient received androgen deprivation therapy, local irradiation, and several lines of systemic therapy. Because of progression, patient was referred for 3 cycles of 177Lu PSMA-617 therapy. 68Ga-PSMA-11 PET/CT demonstrated extensive PSMA-positive nodal metastases at baseline (transaxial CT [A], fused PET/CT [B], and maximum-intensity projection [MIP] [C]) and reduced tumor load after 3 cycles of 177Lu-PSMA-617 therapy (MIP [D], transaxial CT [E], and fused PET/CT [F]). PSA level dropped from 291 ng/mL before 177Lu-PSMA-617 therapy to 38 ng/mL after 177Lu-PSMA-617 therapy.
The largest multicenter retrospective case series for toxicity and PSA response in patients after 177Lu-PSMA-617 treatment was published as part of an initiative by the German Society of Nuclear Medicine (110). Data were collected for 145 patients who had mCRPC and had undergone a median of 2 cycles (range, 1–4) of 177Lu-PSMA-617 RLT at 12 centers. Most patients received 5.5–6.5 GBq (median, 6.0 GBq) or greater than 6.5 GBq (median, 7.4 GBq) per cycle. The rate of nonhematologic grade 3 or 4 events was low (0–3 patients; 0%–2%). Grade 3 or 4 anemia occurred in 15 patients (10%), and grade 3 or 4 thrombocytopenia occurred in 5 patients (4%).
A decline in the PSA level of greater than or equal to 50% was seen in 45 of 99 patients (45%) over the entire follow-up period. Any decline in the PSA level occurred in 59 of 99 patients (60%). After the first therapy cycle, a decline in the PSA level of greater than or equal to 50% was observed in 40 of 99 patients (40%), and any decline in the PSA level was observed in 65 of 99 patients (66%). After the second therapy cycle, a decline in the PSA level of greater than or equal to 50% was seen in 35 of 61 patients (57%), and any decline in the PSA level was seen in 44 of 61 patients (72%). Most patients who received a third or fourth cycle showed a decline in the PSA level of greater than or equal to 50% (65% or 100%, respectively). A potential limitation of that study (110) was the strict date for data inclusion, which omitted an analysis of follow-up data as well as inclusion of further cycles in patients still under treatment.
Baum et al. published a study of the largest series of patients with 177Lu-PSMA-I&T RLT (112). A total of 125 cycles (up to 5 cycles per patient; median administered activity, 5.8 GBq) were administered in 56 patients. A decrease in the serum PSA level was reported in 80.3% of patients. The median progression-free survival was 13.7 mo, and the median overall survival was not reached at the follow-up of 28 mo. Heck et al. reported the safety and efficacy of 177Lu-PSMA-I&T in mCRPC patients (116). No grade 3 or 4 toxicity was reported. Grade 1 or 2 xerostomia occurred in 7 patients (37%), anemia occurred in 6 patients (32%), and thrombocytopenia occurred in 5 patients (25%). A maximum decline in the PSA level of greater than or equal to 50% was achieved in 33% of patients. The Eastern Cooperative Oncology Group performance status improved or was stable in 74% of patients. Complete resolution or reduced pain after treatment was achieved in 58% of patients with bone pain.
Dosimetry
Several dosimetric analyses for both 177Lu-PSMA-617 and 177Lu-PSMA-I&T have been published (112,117–120). They documented favorable dosimetry with a low red marrow dose—approximately 0.03 Gy/GBq. Organs at risk are the kidneys (0.5–0.7 Gy/GBq) and the salivary or lacrimal glands (1.2–2.8 Gy/GBq). However, universal limits for a cumulative dose by endoradiotherapy have not been established, and radiation-induced nephropathy or severe xerostomia has been observed only in individual cases thus far. Tumor doses were estimated to be between 1.2 and 47.5 Gy/GBq (mean, 13.1 Gy/GBq). Despite high tumor doses, all authors reported that some patients (20%–40%) were refractory to treatment with 177Lu-PSMA ligands even though there was sufficient PSMA expression on pretherapeutic PET. Patients with diffuse red marrow infiltration, which was considered a risk factor for the development of a higher level of hematotoxicity (118), presented another challenge. A promising option for overcoming this limitation could be the application of PSMA ligands labeled with the short-range α-particle emitter 225Ac. Kratochwil et al. reported a promising response with 225Ac-PSMA-617 in 2 patients who showed progression after 177Lu-PSMA-617 treatment (121). However, in that initial experience, substantial xerostomia was a side effect.
Radioguided Surgery (RGS)
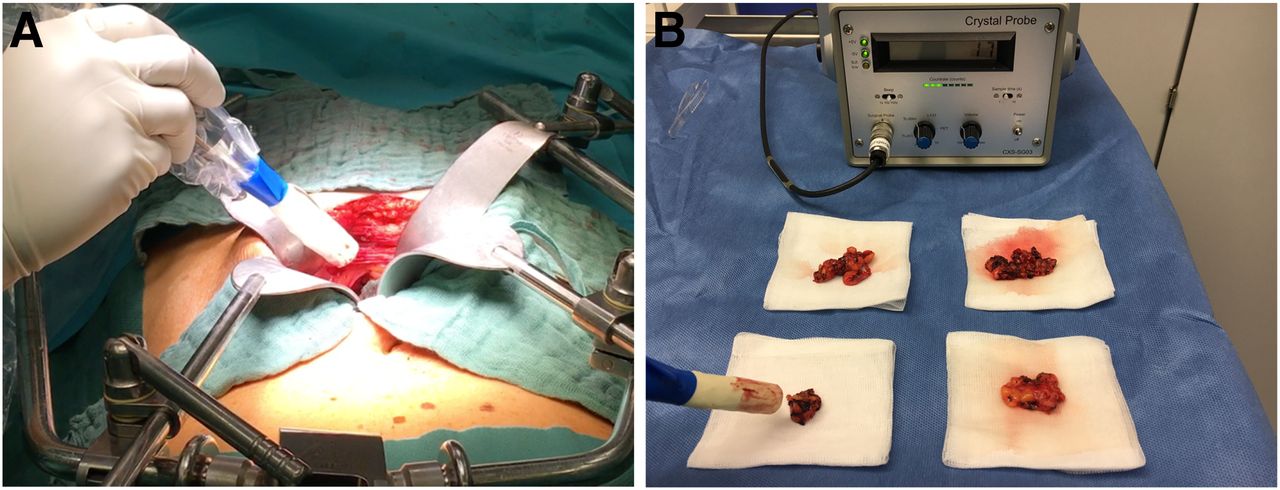
Improved tumor localization with PSMA ligands now allows the detection in early BCR of tiny and often atypically located lesions that often cannot be visualized reliably during surgery (Fig. 7). Maurer et al. attempted to expand the spectrum of radiolabeled PSMA ligands toward RGS using 111In-labeled PSMA-I&T (122). One patient with primary disease and 4 patients with BCR and evidence of solely regional LN metastases only on 68Ga-PSMA-11 PET underwent RGS. Patients received a mean of 146 MBq (range, 110–169 MBq) of 111In-PSMA-I&T 24 h before surgery. In that feasibility study, all tissue specimens that showed positive radiosignals in vivo were confirmed to bear PSMA-expressing metastatic disease by ex vivo histopathology (Fig. 7). The detection of subcentimeter lesions was enabled by RGS. In 2 patients, tumor deposits that were not visualized on preoperative 68Ga-PSMA-11 PET imaging were detected by RGS.
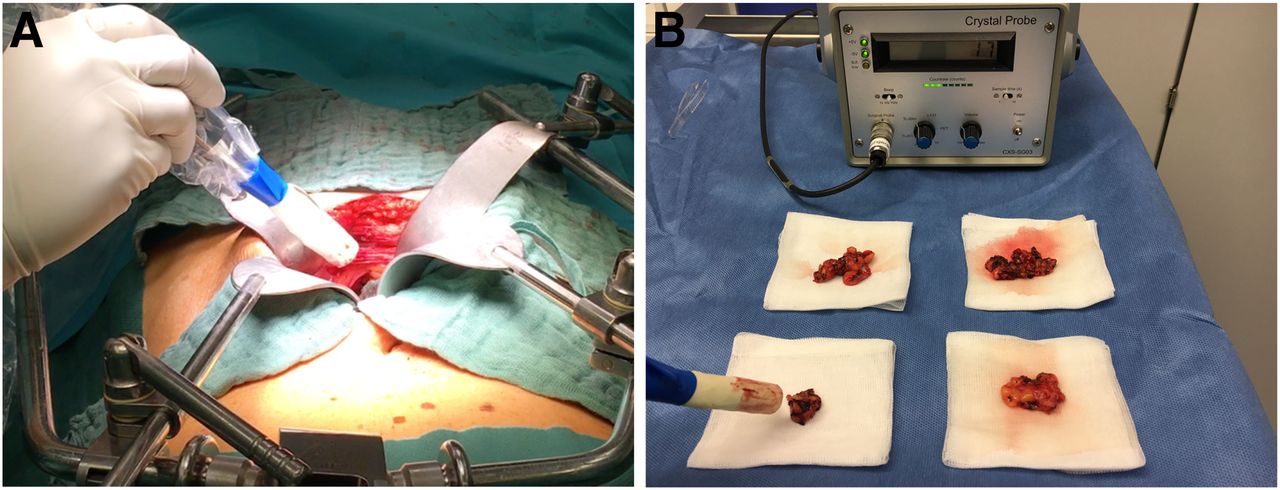
PSMA RGS. In vivo (A) and ex vivo (B) intraoperative γ-probe measurements facilitated complete resection of PSMA ligand–positive LN prior to detection on 68Ga-PSMA-11 PET/CT.
A follow-up study summarized the data for 31 patients after salvage PSMA RGS (123). Declines in the PSA level of greater than 50% and greater than 90% were observed in 23 of 30 patients (76.7%) and 16 of 30 patients (53.3%), respectively. In 18 of 30 patients (60.0%), a decline in the PSA level to less than 0.2 ng/mL was achieved. In 10 of 30 patients (33.3%), further PC-specific treatment was given after a median of 125 d (range, 48–454 d) following 111In-PSMA-I&T RGS. The remaining 20 patients were treatment-free at a median follow-up of 337 d (range, 81–591 d). These data indicate that 111In-PSMA I&T RGS might have a beneficial influence on further disease progression; however, the identification of suitable patients on the basis of PSMA PET as well as clinical variables is essential for satisfactory results. A potential limitation of RGS is the missing direct visualization of tumor tissue in real time. At present, researchers are working on PSMA ligands suitable for real-time near-infrared fluorescence imaging of surgical margins and fluorescence-guided resection of tumor residues (124).
CONCLUSION
PSMA ligands for both imaging and therapy have been adopted clinically at an unprecedented rate, resulting in dramatic increases in the number of research publications. Current evidence from the literature strongly indicates that PSMA ligand PET imaging may have considerable influence on the management of early recurrent disease as well as primary (intermediate- and high-risk) PC. In addition, therapeutic approaches, mainly with 177Lu-PSMA RLT, have been shown to be valuable for the treatment of advanced disease; further advances are to be expected from the use of α-emitters. However, current data rely predominantly on retrospective analyses. Well-defined patient cohorts and dedicated endpoints are needed for the implementation of these technologies into guidelines. Fortunately, several academic as well as industry-driven studies are already under way or planned and may provide the needed evidence. However, because of the multitude of PSMA ligands as well as the different approaches chosen, predicting which agents may finally reach regulatory approval and clinical reimbursement is difficult. For the well-being of their patients, both nuclear medicine physicians and their clinical counterparts must jointly create algorithms for the wise use of these new tools.
DISCLOSURE
Clemens Kratochwil and Frederik L. Giesel disclose a patent application (EP 15 002 800.9, DKFZ) for PSMA-1007. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Thorsten Derlin for contributing a case of 68Ga-PSMA-I&T PET/CT imaging as well as Christine Mona for assisting in designing figures.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.
- 13.
- 14.
- 15.
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.
- 47.↵
- 48.↵
- 49.↵
- 50.
- 51.
- 52.
- 53.
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.
- 114.
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- Received for publication February 2, 2017.
- Accepted for publication March 20, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dansylated Amino Acid-Modified Long-Acting PSMA Derivatives 68Ga/177Lu-LNC1011 as Prostate Cancer Theranostics
- Matched-Pair Comparison of 18F-DCFPyL PET/CT and 18F-PSMA-1007 PET/CT in 240 Prostate Cancer Patients: Interreader Agreement and Lesion Detection Rate of Suspected Lesions
- The Impact of Monosodium Glutamate on 68Ga-PSMA-11 Biodistribution in Men with Prostate Cancer: A Prospective Randomized, Controlled Imaging Study
- PSA-Targeted Alpha-, Beta-, and Positron-Emitting Immunotheranostics in Murine Prostate Cancer Models and Nonhuman Primates
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy
- The Effects of Monosodium Glutamate on PSMA Radiotracer Uptake in Men with Recurrent Prostate Cancer: A Prospective, Randomized, Double-Blind, Placebo-Controlled Intraindividual Imaging Study
- Comparison of 3 Interpretation Criteria for 68Ga-PSMA11 PET Based on Inter- and Intrareader Agreement
- Total-Body 68Ga-PSMA-11 PET/CT for Bone Metastasis Detection in Prostate Cancer Patients: Potential Impact on Bone Scan Guidelines
- Lymph Node Involvement in Treatment-Naive Prostate Cancer Patients: Correlation of PSMA PET/CT Imaging and Roach Formula in 280 Men in Radiotherapeutic Management
- Prostate-Specific Membrane Antigen-Guided Surgery
- 177Lu-PSMA-617 Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer Patients with a Single Functioning Kidney
- The Future of Nuclear Medicine as an Independent Specialty
- qPSMA: Semiautomatic Software for Whole-Body Tumor Burden Assessment in Prostate Cancer Using 68Ga-PSMA11 PET/CT
- Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine
- Preserving Preclinical PET Quality During Intratherapeutic Imaging in Radionuclide Therapy with Rose Metal Shielding Reducing Photon Flux
- Early Experience of Rechallenge 177Lu-PSMA Radioligand Therapy After an Initial Good Response in Patients with Advanced Prostate Cancer
- Entering the Era of Molecularly Targeted Precision Surgery in Recurrent Prostate Cancer
- Synthesis and Preclinical Characterization of the PSMA-Targeted Hybrid Tracer PSMA-I&F for Nuclear and Fluorescence Imaging of Prostate Cancer
- One-Stop-Shop Whole-Body 68Ga-PSMA-11 PET/MRI Compared with Clinical Nomograms for Preoperative T and N Staging of High-Risk Prostate Cancer
- A Prospective Comparison of 18F-Sodium Fluoride PET/CT and PSMA-Targeted 18F-DCFBC PET/CT in Metastatic Prostate Cancer
- A Perspective on the Evolving Story of PSMA Biology, PSMA-Based Imaging, and Endoradiotherapeutic Strategies
- Intraindividual Comparison of 18F-PSMA-1007 and 18F-DCFPyL PET/CT in the Prospective Evaluation of Patients with Newly Diagnosed Prostate Carcinoma: A Pilot Study
- Proposed Criteria Positions PSMA PET for the Future
- Theranostic Concepts: More Than Just a Fashion Trend--Introduction and Overview