


Abstract
Our aim was to retrospectively evaluate the feasibility of rechallenge 177Lu-prostate-specific membrane antigen (177Lu-PSMA) radioligand therapy. Methods: Rechallenge radioligand therapy was defined as subsequent treatment with 177Lu-PSMA after initial exposure with an excellent response followed by progression. Biochemical, radiographic, clinical antitumor response, and adverse events were analyzed. Prostate-specific antigen (PSA) progression-free survival (PFS) and overall survival were calculated. Results: Eight patients underwent a median of 2 (range: 1–4) cycles of rechallenge with 177Lu-PSMA for imaging and therapy. A maximum PSA decrease of 50% was achieved in 3 patients (37.5%). Radiographic response was favorable in 3 patients, whereas 4 exhibited progressive disease. Eastern Cooperative Oncology Group performance status was stable during therapy in all patients. No grade 4 toxicity was noticed, and grade 3 toxicity occurred in 3 patients (37.5%). The median PSA-PFS and overall survival were 3.2 mo (95% confidence interval, 2.6–3.7 mo) and 14.0 mo (95% confidence interval, 6.2–21.8 mo), respectively. Conclusion: In a small patient cohort with an initial excellent response, 177Lu-PSMA rechallenge is still active, with lower efficacy and higher toxicity.
Metastatic castration-resistant prostate cancer (mCRPC) is the lethal phenotype of the disease. Despite several new agents having been approved, more than 250,000 men still die of prostate cancer worldwide each year (1). In recent years, prostate-specific membrane antigen (PSMA) became an attractive target for both diagnosis and treatment of prostate cancer (2). The application of PSMA ligands labeled with the radionuclide 177Lu has demonstrated encouraging efficacy and a good safety profile for 177Lu-PSMA radioligand therapy (RLT) (3,4). Rechallenge of docetaxel in patients with mCRPC who initially responded to a docetaxel chemotherapy regimen was described as a potential treatment option after a docetaxel-free interval. Available data indicate reasonable antitumor response at moderate toxicity (5,6).
So far, data for rechallenge of 177Lu-PSMA RLT in patients after prior effective treatment followed by progressive disease after a 177Lu-PSMA–free interval have not been published. Therefore, we aimed to retrospectively assess the efficacy and safety profile of 177Lu-PSMA rechallenge in this specific patient cohort.
MATERIALS AND METHODS
All patients who underwent RLT with 177Lu-PSMA for imaging and therapy (I&T) in a rechallenge setting at our institution between October 2014 and February 2018 were extracted. The median patient age at rechallenge treatment was 72 y (range: 62–77 y). The median number of 177Lu-PSMA-I&T cycles was 6 (range: 4–6) at initial treatment and 2 (range: 1–4) at rechallenge. Seven patients received at least 2 cycles and 2 patients underwent at least 3 cycles at 177Lu-PSMA-I&T rechallenge. The median time of the 177Lu-PSMA-I&T–free interval was 5.4 mo (range: 3.8–14.7 mo). During this interval, all patients received continuous androgen deprivation therapy. The median prostate-specific antigen (PSA) level at the beginning of rechallenge treatment was 52 ng/mL (range: 5–2,328 ng/mL).
The rationale to consider initial 177Lu-PSMA-I&T accomplished were completion of 4 or 6 cycles, at least a 50% PSA decline, minimum 50% decrease in extent and uptake of metastases on 68Ga-PSMA-11 PET imaging, and/or resolution of clinical symptoms if present. On the basis of dosimetry data and data for radiation dose limits for normal organs (7), we limited the maximum number of cycles to 4 in the initial phase of our experience with 177Lu-PSMA-I&T. The rationale was not to exceed the dose limit for the kidneys, which are the critical organ at risk. As we did not notice any relevant treatment-related kidney function impairment (3), the maximum number was subsequently increased to 6 cycles for the initial treatment.
The inclusion criteria for 177Lu-PSMA rechallenge were completion of initial 177Lu-PSMA RLT, tumor progression (increasing PSA levels) during the 177Lu-PSMA–free interval, and PSMA-avid lesions on 68Ga-PSMA-11 PET/CT before rechallenge treatment (3,7). Rechallenge treatment was applied every 6–8 wk, including 68Ga-PSMA-11 PET/CT every 2 cycles. All patients gave written informed consent to compassionate-use treatment. The institutional review board approved the analysis (reference 115/18S).
Nonhematologic and hematologic adverse events were graded according to the Common Terminology Criteria for Adverse Events, version 5.0. Biochemical response was defined as a PSA decline of at least 30%, 50%, and 90% during initial and rechallenge treatment. For radiographic response, 68Ga-PSMA-11 PET/CT findings were assessed as described recently (8). Clinical response was assessed by Eastern Cooperative Oncology Group performance status and changes in bone pain from the Brief Pain Inventory. Overall survival and PSA progression-free survival (PSA-PFS) were calculated according to the guidelines of the Prostate Cancer Trials Clinical Working Group 3 (9).
PSA-PFS and overall survival were determined using the Kaplan–Meier curve method with corresponding 95% confidence interval (95%CI). Statistical analyses were performed using IBM SPSS Statistics, version 22.0 (IBM Corp.).
RESULTS
Eight patients with 177Lu-PSMA-I&T RLT in a rechallenge setting were analyzed. One patient even underwent a third course of treatment. Details on patient characteristics are given in Table 1.
Patient Characteristics
Safety Profile
Specific nonhematologic and hematologic parameters for all patients at baseline and after 177Lu-PSMA-I&T rechallenge are presented in Supplemental Table 1 and Figure 1 (supplemental materials are available at http://jnm.snmjournals.org). Adverse events graded according to the Common Terminology Criteria for Adverse Events, version 5.0, are shown in Table 2. No grade 4 adverse events were noticed. Grade 3 adverse events occurred in 3 patients (37.5%), 2 of them with thrombocytopenia and 1 with anemia. A grade 1 increase in creatinine serum was observed in 1 patient (12.5%). Grade 1 xerostomia was noticed in 2 patients (25%). Nearly all patients with grade 2 or 3 toxicities had presented with grade 1 toxicity at the start of the 177Lu-PSMA-I&T rechallenge.
Adverse Events at 177Lu-PSMA-I&T Rechallenge Graded According to Common Terminology Criteria for Adverse Events, Version 5.0
Antitumor Response
Biochemical
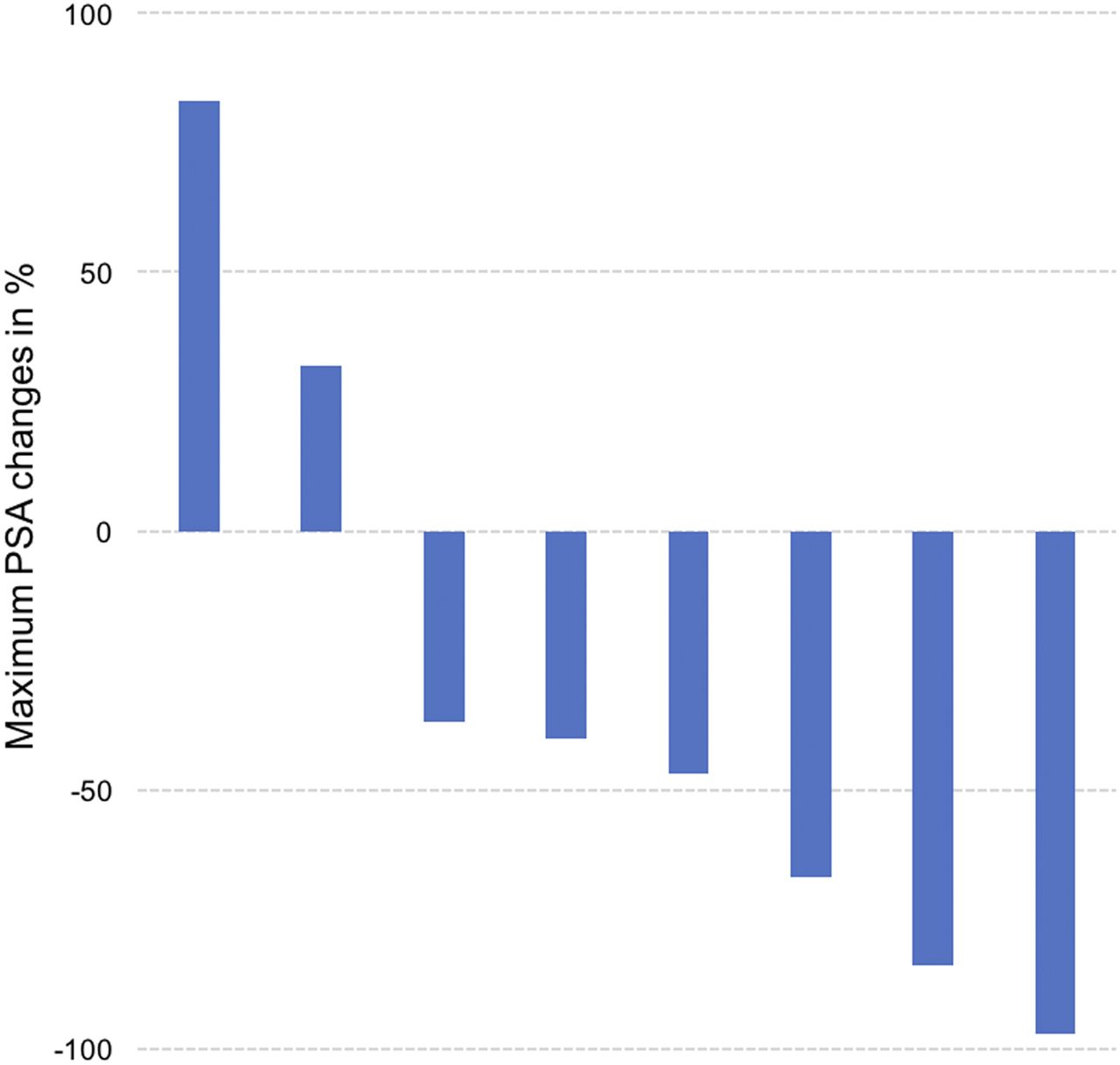
At initial treatment with 177Lu-PSMA-I&T, all patients achieved a maximum PSA decline of at least 50%, and 75% of patients (6/8) had at least a 90% PSA decline. During 177Lu-PSMA-I&T rechallenge, a maximum PSA decline of at least 30%, 50%, and 90% was achieved in 75.0% of patients (6/8), 37.5% (3/8), and 12.5% (1/8), respectively. Table 1 presents intraindividual PSA responses and PSA levels at baseline and after 177Lu-PSMA-I&T, both at initial and at rechallenge treatment. Figure 2 shows the waterfall plot of maximum PSA responses at rechallenge treatment.
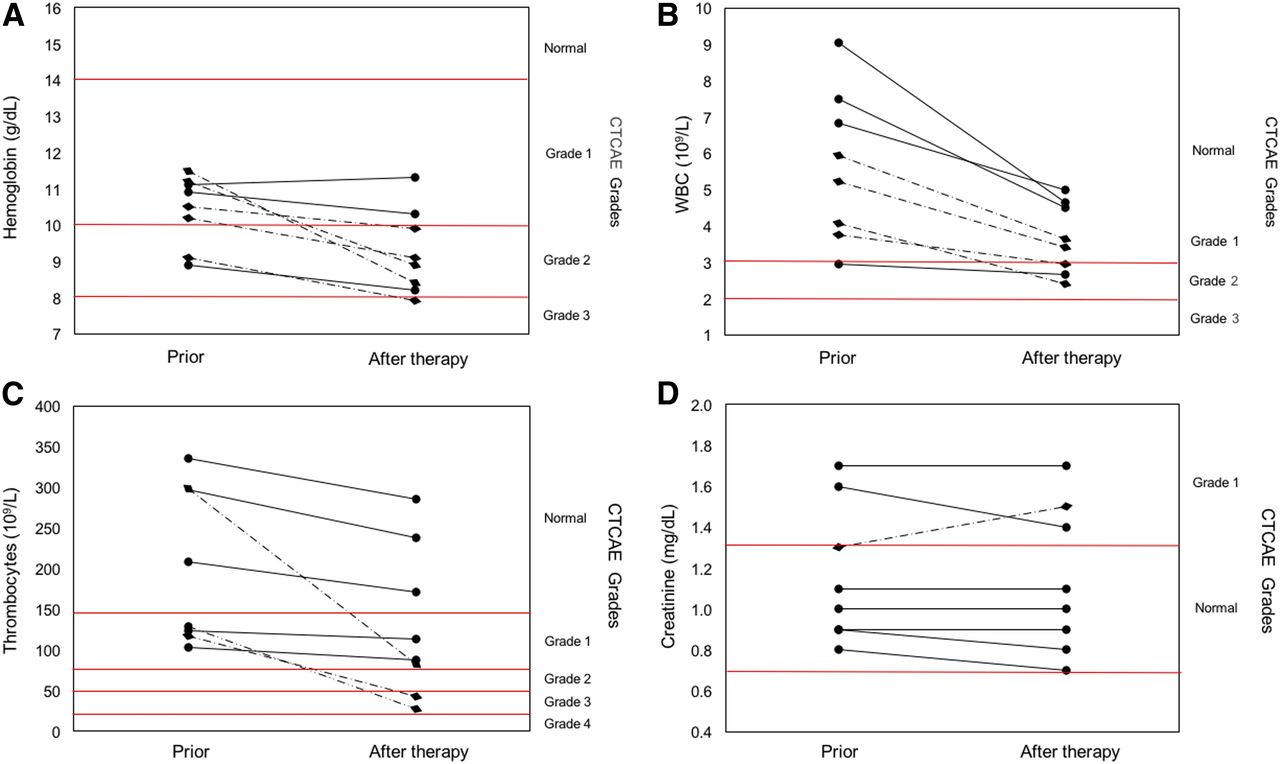
Comparison of hematologic lab results for hemoglobin (A), white blood cells (WBC) (B), thrombocytes (C), and creatinine (D) before and after 177Lu-PSMA-I&T rechallenge. CTCAE = Common Terminology Criteria for Adverse Events.
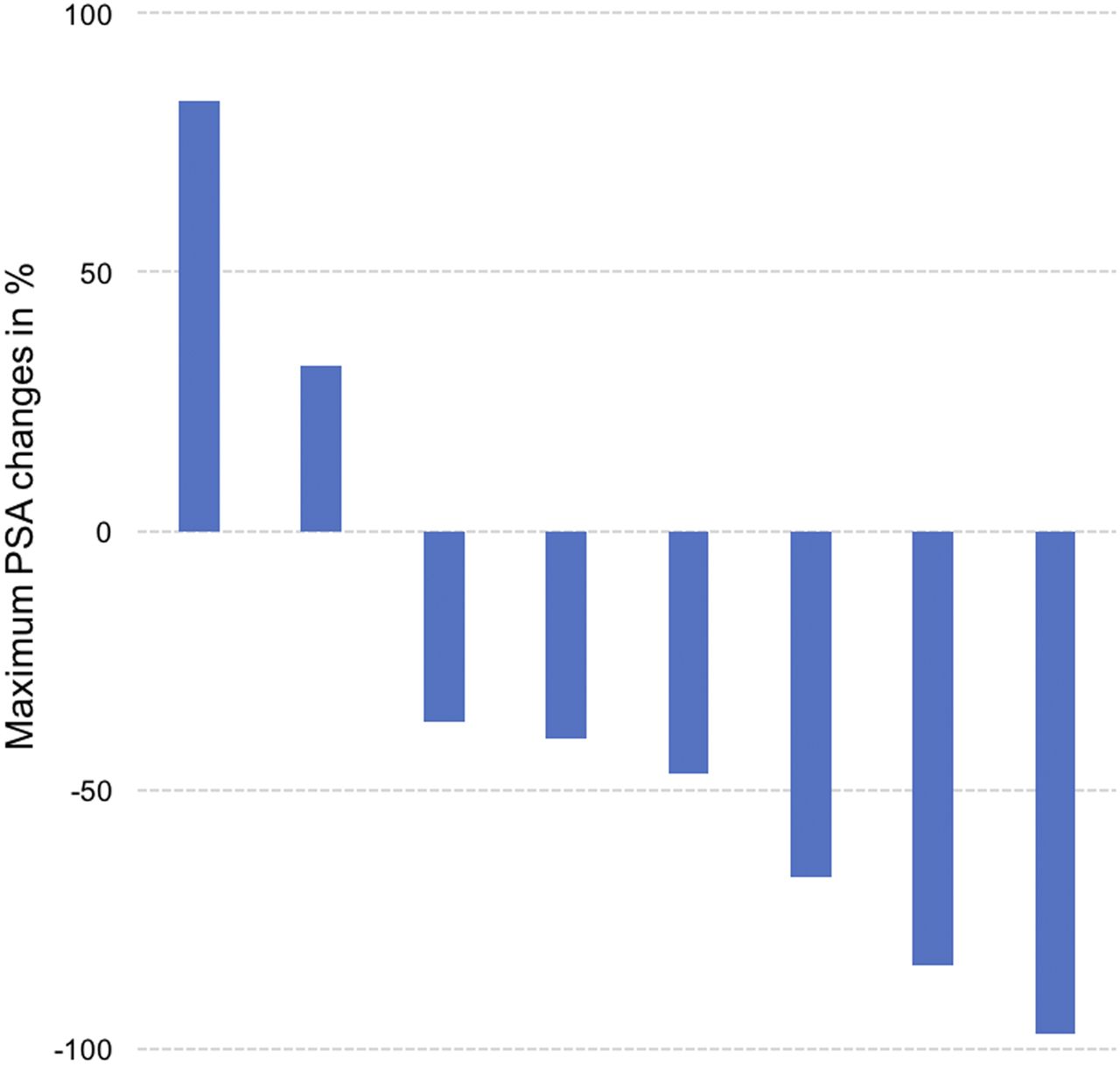
Waterfall plot of maximum PSA responses during 177Lu-PSMA-I&T rechallenge as compared with baseline levels.
Radiographic
Radiographic antitumor response was assessed in 7 patients. One patient did not undergo the follow-up 68Ga-PSMA-11 PET/CT because of progressive disease and general deterioration. According to the adapted PERCIST 1.0 (10), 3 patients had a partial response, and 4 patients exhibited progressive disease due to new lesions.
Clinical
At baseline, an Eastern Cooperative Oncology Group score of 0, 1, and 2 was present in 1 (12.8%), 6 (75%) and 1 (12.8%) patients, respectively. Eastern Cooperative Oncology Group Performance Status remained stable in all patients during the course of rechallenge treatment. At baseline, 6 patients had pain related to bone metastases. Of these, 2 (33%) reported complete resolution of pain, 1 (16%) had partial remission, 2 (32%) reported no changes, and 1 (16%) reported worsening bone pain.
Time on Treatment and Survival Curve Analyses
The swimmer plot (Fig. 3) displays intraindividual mCRPC therapy duration and maximum PSA response at 177Lu-PSMA-I&T rechallenge. Treatment was discontinued in 4 patients because of adverse events (3 with thrombopenia and 1 with renal function impairment) and in 3 patients because of biochemical or radiographic progression. In 1 patient, 177Lu-PSMA rechallenge was halted after 4 cycles because of an exceptional response; this patient was restarted on the third course after an additional 177Lu-PSMA–free interval. One case example is displayed in Supplemental Figure 1.

Swimmer plot demonstrating mCRPC treatment duration and maximum PSA response at 177Lu-PSMA-I&T rechallenge.
Median overall survival was 23.1 mo (95%CI, 19.5–26.7 mo) after the first initiation of 177Lu-PSMA-I&T and 14.0 mo (95%CI, 6.2–21.8 mo) after initiation of rechallenge treatment. Three patients (37.5%) were alive at the last follow-up. The median PSA-PFS was 12.4 mo (95%CI, 10.4–14.3 mo) from the beginning of the initial 177Lu-PSMA-I&T RLT and 3.2 mo (95%CI, 2.6–3.7 mo) from the beginning of rechallenge treatment.
DISCUSSION
To our knowledge, this is the first report assessing the efficacy and safety profile of 177Lu-PSMA rechallenge in patients with mCRPC. Exposing a patient to the same oncologic treatment as that which was effective during the primary application is an increasingly used concept, for example, for docetaxel (5,6).
In our selected group of patients with excellent response to initial 177Lu-PSMA-I&T, the median PSA-PFS at the first therapy course was 12.4 mo (95%CI, 10.4–14.3 mo), versus 3.3 mo (95%CI, 2.6–3.7 mo) at treatment rechallenge, and also was much shorter than that of an unselected cohort of patients at initial 177Lu-PSMA-I&T treatment (median PSA-PFS, 5.8 mo [95%CI, 1.2–10.5 mo] (3)). Only 37.5% of patients achieved a 50% PSA decline during rechallenge. In a similar setting involving patients who had an initial good response to docetaxel, a 50% PSA decline was reported in 28%–40% of patients at rechallenge treatment (5,6). These results outline that rechallenge treatment offers antitumor activity, but to a lower extent than initial treatment.
The benefits of 177Lu-PSMA rechallenge have to be weighed against the risk of cumulative toxicity. All 3 patients with grade 3 adverse events exhibited impaired lab results before 177Lu-PSMA rechallenge (Fig. 1). Furthermore, both patients with grade 3 thrombopenia had substantial tumor progression during rechallenge treatment. Therefore, discriminating the etiology of bone marrow failure (progression vs. treatment-related) is difficult.
There are no guidelines for the optimum number of cycles of 177Lu-PSMA in patients who show a good response. Currently, in our institution, the initial treatment with 177Lu-PSMA is typically discontinued after a maximum of 6 cycles. Usually, patients who undergo RLT are heavily pretreated with other mCRPC therapies, including second-line androgen receptor target treatments or taxane-based regimens. In our study, patients underwent a mean of 4 (range: 2–8) mCRPC pretreatment lines. Chemotherapy with cabazitaxel and the radiopharmaceutical 223Ra-dichloride are 2 common therapeutic choices after initial 177Lu-PSMA RLT discontinuation. When compared, the median overall survivals were 14.5 mo (95%CI, 13.5–15.3 mo), 14.5 mo (95%CI, 13.5–15.3 mo), and 14.0 mo (95%CI, 6.2–21.8 mo) for 3-weekly 25 mg/m2 cabazitaxel, 223Ra, and our small cohort of 177Lu-PSMA-I&T rechallenge, respectively (11,12). However, with only 8 patients in our analysis, caution is warranted regarding comparison with the survival data of other treatments. Notably, in a recent abstract describing 177Lu-PSMA-617 in a rechallenge setting, 75% of patients achieved any PSA decrease at an acceptable toxicity level (13).
Our analysis has limitations. First, we report only a small cohort of 8 patients. Consequently, our results have to be interpreted with caution, and further analyses (e.g., predictor factors) were not possible. However, 177Lu-PSMA RLT has been introduced only recently and the number of patients with an excellent response is limited. Second, because of the lack of an established system to evaluate response on PSMA PET, we adopted PERCIST 1.0, as previously described (8). The validation of PERCIST for non–18F-FDG application is still under discussion.
CONCLUSION
Our results in a small patient cohort with an initial excellent response during 177Lu-PSMA RLT indicate that this treatment is still active in a rechallenge setting, but with lower efficacy and higher toxicity. The present study proposes 177Lu-PSMA rechallenge as a potential therapeutic option in this palliative setting with a lack of alternatives. Its benefits have to be weighed against the risk of cumulative toxicity. Further prospective studies with larger patient cohorts are warranted to investigate the clinical outcome for mCRPC patients undergoing 177Lu-PSMA rechallenge.
DISCLOSURE
Matthias Eiber received funding from the SFB 824 (DFG Sonderforschungsbereich 824, project B11) from the Deutsche Forschungsgemeinschaft, Bonn, Germany. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Nov. 15, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 6, 2018.
- Accepted for publication October 10, 2018.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Evidence-Based Clinical Protocols to Monitor Efficacy of [177Lu]Lu-PSMA Radiopharmaceutical Therapy in Metastatic Castration-Resistant Prostate Cancer Using Real-World Data
- Challenges with 177Lu-PSMA-617 Radiopharmaceutical Therapy in Clinical Practice
- Safety and Efficacy of Extended Therapy with [177Lu]Lu-PSMA: A German Multicenter Study
- Novel Framework for Treatment Response Evaluation Using PSMA PET/CT in Patients with Metastatic Castration-Resistant Prostate Cancer (RECIP 1.0): An International Multicenter Study
- Administration Routes for SSTR-/PSMA- and FAP-Directed Theranostic Radioligands in Mice
- Early Prostate-Specific Antigen Changes and Clinical Outcome After 177Lu-PSMA Radionuclide Treatment in Patients with Metastatic Castration-Resistant Prostate Cancer
- Genetic signature of prostate cancer mouse models resistant to optimized hK2 targeted {alpha}-particle therapy
- Genetic signature of prostate cancer resistant to optimized hK2 targeted alpha-particle therapy