


Abstract
Prostate-specific antigen (PSA) is widely used to monitor treatment response in patients with metastatic castration-resistant prostate cancer. However, PSA measurements are considered only after 12 wk of treatment. We aimed to evaluate the prognostic value of early PSA changes after 177Lu-labeled prostate-specific membrane antigen (177Lu-PSMA) radionuclide treatment in metastatic castration-resistant prostate cancer patients. Methods: Men who were treated with 177Lu-PSMA under a compassionate-access program at our institution and had available PSA values at baseline and at 6 wk after treatment initiation were included in this retrospective analysis. Patients were assigned to 3 groups on the basis of PSA changes: response (≥30% decline), progression (≥25% increase), and stable (<30% decline and <25% increase). The coprimary endpoints were overall survival and imaging-based progression-free survival. The secondary endpoints were PSA changes at 12 wk and PSA flare-up. Results: We identified 124 eligible patients with PSA values at 6 wk. A greater than or equal to 30% decline in PSA at 6 wk was associated with longer overall survival (median, 16.7 mo; 95% CI, 14.4–19.0) than stable PSA (median, 11.8 mo; 95% CI, 8.6–15.1) (P = 0.007) or PSA progression (median, 6.5 mo; 95% CI, 5.2–7.8) (P < 0.001). Patients with a greater than or equal to 30% decline in PSA at 6 wk also had a lower risk of imaging-based progression than patients with stable PSA (hazard ratio, 0.60; 95% CI, 0.38–0.94) (P = 0.02), whereas patients with PSA progression had a higher risk of imaging-based progression than patients with stable PSA (hazard ratio, 3.18; 95% CI, 1.95–5.21) (P < 0.001). The percentage changes in PSA at 6 and 12 wk were highly associated (r = 0.90; P < 0.001). Of 31 patients who experienced early PSA progression at 6 wk, 29 (94%) showed biochemical progression at 12 wk. Overall, only 1 (3%) of 36 patients with PSA progression at 6 wk achieved any PSA decline at 12 wk (1% of the entire cohort). The limitations of the study included its retrospective nature and the single-center experience. Conclusion: PSA changes at 6 wk after 177Lu-PSMA initiation are an early indicator of long-term clinical outcome. Patients with PSA progression after 6 wk of treatment could benefit from a very early decision to switch treatment. PSA flare-up during 177Lu-PSMA treatment is very uncommon. Prospective studies are now warranted to validate our findings and potentially inform clinicians earlier on the effectiveness of 177Lu-PSMA.
- metastatic castration-resistant prostate cancer
- radionuclide therapy
- prostate-specific antigen
- prostate-specific membrane antigen
- 177Lu-PSMA
Despite recent therapeutic advances, only one-third of patients with metastatic castration-resistant prostate cancer (mCRPC) survive more than 5 y, with survival rates depending on known prognostic risk factors (1,2). The results of 177Lu-labeled prostate-specific membrane antigen (177Lu-PSMA) radionuclide therapy of mCRPC have been reported for more than 1,000 patients in compassionate-access programs in Germany and other countries (3). These results as well as encouraging efficacy in phase 2 clinical trials (4,5) have led to an ongoing phase 3 clinical trial (VISION; ClinicalTrials.gov identifier: NCT03511664). Reliable markers and early prognostic factors are urgently needed to support patient management decisions and to select optimized therapy sequencing in mCRPC.
Since the introduction of serum prostate-specific antigen (PSA) screening in the 1980s (6), prostate cancer management has been guided by this biomarker. For mCRPC, 30% and 50% declines in PSA after 12 wk of treatment have been consistently associated with longer survival (7–9). Similarly, a 25% rise in PSA from baseline/nadir has been associated with a poor outcome (10,11). According to Prostate Cancer Working Group 3 (PCWG3) recommendations for mCRPC, PSA progression should not be determined in the first 12 wk of treatment because of possible late declines and flare reactions reported in patients treated with taxanes (12–14). However, previous reports found early PSA changes after 4 wk of treatment with abiraterone acetate and enzalutamide to be associated with overall survival, with flare reactions being uncommon (15,16). Insufficient data have been reported regarding the clinical outcome of early PSA changes in mCRPC patients treated with 177Lu-PSMA. The primary objective of this study was to evaluate the association between PSA changes at 6 wk after treatment initiation and clinical outcome. The secondary objectives were to assess the frequency of PSA flare-up and the associations between PSA changes at 6 wk and those at 12 wk. We hypothesized that patients with an early 25% increase in PSA will also develop PSA progression at 12 wk.
MATERIALS AND METHODS
Patient Population and Treatment Regimen
Patients with progressive mCRPC treated with 177Lu-PSMA imaging and therapy (177Lu-PSMA) at our institution under a compassionate-access program (9) were retrospectively considered for this analysis. All patients provided written informed consent. The retrospective data analysis was approved by the Medical Ethics Committee of the Technical University of Munich (reference number: 115/18S). Eligible patients had available serum PSA levels at baseline and after 6 wk of treatment and survival data. When available, PSA measurements 12 wk after 177Lu-PSMA initiation were also extracted. Our institutional eligibility criteria for 177Lu-PSMA are provided in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
Intravenous treatment with 7.4 GBq of 177Lu-PSMA was applied every 6–8 wk and was continued for up to a maximum of 6 cycles in patients with the absence of progressive disease and a lack of severe toxicity, according to the investigator. Progressive disease was defined as biochemical, imaging-based, or clinical progression according to PCWG3 criteria (12). For biochemical progression earlier than 12 wk, the treatment continuation/discontinuation decision was made on the basis of available imaging, laboratory tests, and the patient’s performance status. Patients who successfully completed the initial treatment (≥50% decline in PSA) were considered for further 177Lu-PSMA treatment in a rechallenge setting, as recently described (17). Patients were evaluated using PSMA-targeted PET/CT at baseline and every 2 cycles.
Endpoints
The coprimary endpoints were overall survival and imaging-based progression-free survival. The secondary endpoints were PSA changes at 12 wk after 177Lu-PSMA initiation and PSA flare-up. Imaging-based progression-free survival was defined as the time between treatment initiation and the occurrence of imaging-based progression or death. Using modified PCWG3 criteria, we defined imaging-based progression as at least 2 new bone metastases on PSMA-targeted PET, any new soft-tissue lesion on morphologic imaging or PSMA-targeted PET, or soft-tissue progression on CT, in accordance with RECIST version 1.1 (12). The percentage changes in PSA from baseline at 6 and 12 wk were categorized as response (≥30% decline), progression (≥25% increase), and stable (<30% decline and <25% increase). A subanalysis defining the PSA response as a decline of greater than or equal to 50 from baseline was performed. The evaluation of PSA changes was consistent with published consensus guidelines (PCWG3) (12). PSA flare-up was defined as an increase of at least 25% at 6 wk followed by any decline below baseline levels at 12 wk.
Statistical Analysis
The results are presented as median and interquartile range (IQR) for continuous variables and as number and percentage for categoric variables. Kaplan–Meier analysis was used to estimate overall survival and imaging-based progression-free survival. The log-rank test was used to compare survival curves between groups of patients according to PSA changes at the 6- and 12-wk time points. Associations among PSA changes, radiologic progression, and survival were evaluated in univariable and multivariable Cox regression analyses. The multivariable Cox models included PSA changes after 6 wk as a categoric variable, clinical history (Gleason score at diagnosis, metastasis status at diagnosis, time since diagnosis of prostate cancer, and chemotherapy status), and baseline characteristics (presence of visceral metastases, Eastern Cooperative Oncology Group performance status, pain status, and PSA, lactate dehydrogenase, and alkaline phosphatase levels). Continuous variables with a nonnormal distribution were log-transformed. The Spearman ρ-correlation coefficient (r) was calculated to evaluate the association between the percentage of PSA decline at 6 wk and that at 12 wk. The association between the PSA response at 6 wk and that at 12 wk as dichotomized variables (progression/nonprogression) was assessed using χ2 and relative risk tests. Statistical analyses were performed using SPSS version 22 (IBM) and STATA version 15 (StataCorp LLC).
RESULTS
From 160 considered patients, we identified 124 consecutive patients who met the eligibility criteria. The first 177Lu-PSMA treatment was administered in December 2014, and the last cycle was administered in September 2018. The cutoff for follow-up was September 1, 2019. All patients had available PSA values at 6 wk, at a mean time of 6.16 (95% CI, 6.03–6.29) wk after treatment initiation. Of the 124 patients, 115 had available PSA values at 12 wk, at a mean time of 12.03 (95% CI, 11.81–12.26) wk after treatment initiation. The study protocol is displayed in Figure 1. Baseline characteristics are summarized in Table 1; 96 patients (77%) had received previous chemotherapy, 20 (16%) had received second-line cabazitaxel, and all patients had previously received abiraterone or enzalutamide.
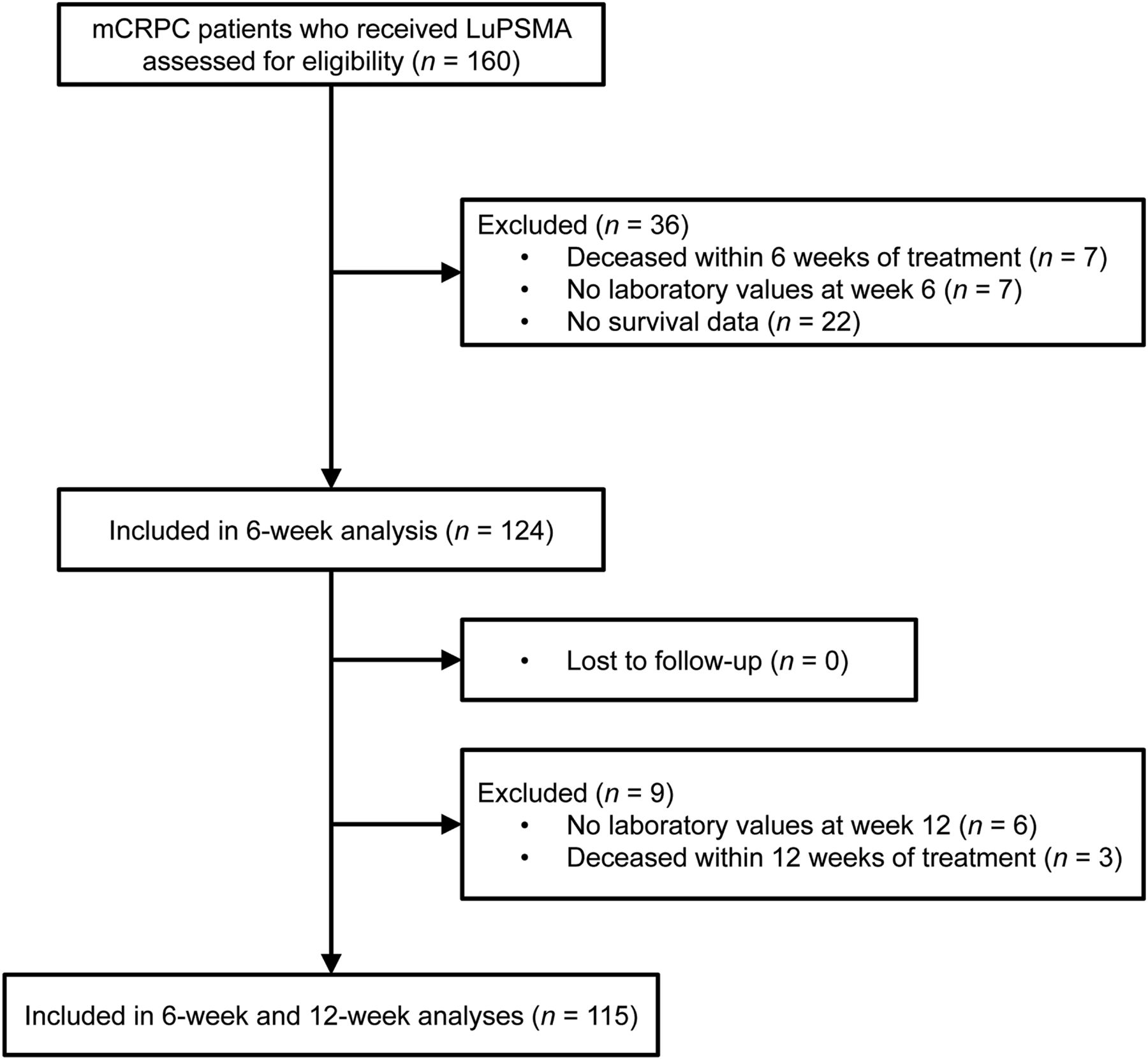
Study protocol. LuPSMA = 177Lu-PSMA imaging and therapy.
Baseline Characteristics for 124 Patients
Overall, 429 cycles of 177Lu-PSMA were administered, at a median of 3 (IQR, 2–5) cycles per patient. All patients received cycle 1 of 177Lu-PSMA, and 118 patients (95%), 61 patients (49%), and 28 patients (23%) received cycles 2, 4, and 6, respectively. The median number of treatment cycles was lower in patients with PSA progression after 6 wk of treatment (2 [IQR, 2–2] cycles) than in those who had stable PSA (4 [IQR, 2–5] cycles) or a PSA response (4 [IQR, 4–6] cycles) (P < 0.001). Twelve patients (10%) received further 177Lu-PSMA treatment in a rechallenge setting. The median follow-up was 23.4 mo (IQR, 20.0–28.7), and 109 patients (88%) were deceased at the last follow-up. The median overall survival was 13.4 mo (95% CI, 11.1–15.6), and the median imaging-based progression-free survival was 3.3 mo (95% CI, 2.0–4.6).
PSA Changes at 6 and 12 wk
The median PSA change at 6 wk was −11.8% (IQR, −49.2% to 38.75%), whereas at 12 wk it was −12.8% (IQR, −62.8% to 62.5%). Fifty patients (40%) experienced a greater than or equal to 30% decline in PSA at 6 wk after 177Lu-PSMA initiation, whereas 30 patients (24%) achieved a greater than or equal to 50% decline in PSA and 36 patients (29%) had PSA progression. At 12 wk, 50 patients (43%) experienced a greater than or equal to 30% decline in PSA, whereas 39 patients (33%) achieved a greater than or equal to 50% decline in PSA. Among the 115 patients with PSA values available at both 6- and 12-wk time points, 25 of 28 patients (89%) with an early PSA decline of greater than or equal to 50% showed a biochemical response at 12 wk, 41 of 48 patients (85%) with an early PSA decline of greater than or equal to 30% achieved a greater than or equal to 30% PSA decline at 12 wk, and 29 of 31 patients (94%) with early PSA progression experienced PSA progression at 12 wk (Tables 2 and 3). The percentage changes in PSA at 6 and 12 wk were highly associated (r = 0.90; P < 0.001).
Relationship Between PSA Changes at 6 Weeks and Those After 12 Weeks When ≥30% PSA Decline Was Included as Early PSA Response
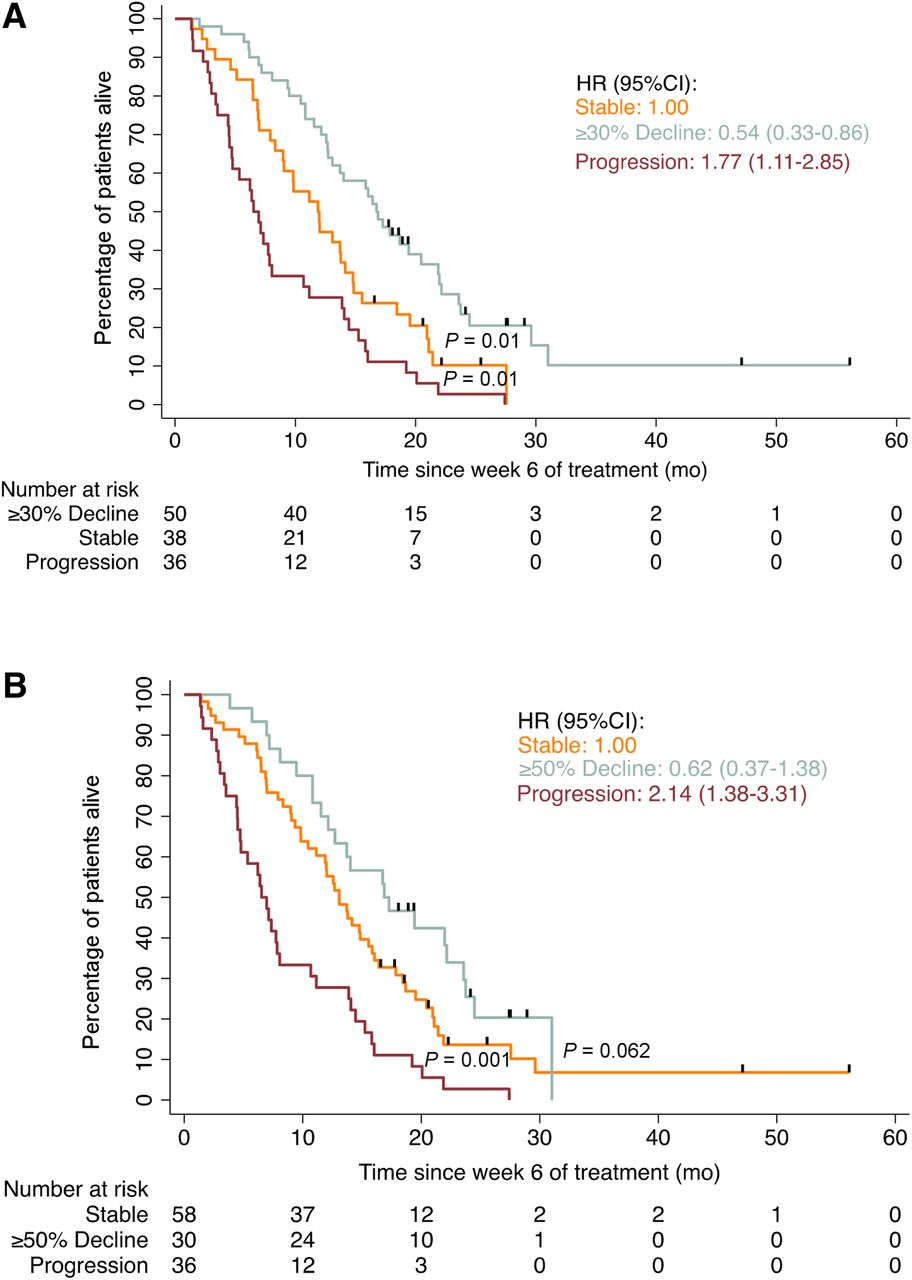
Kaplan–Meier curves of landmark analysis of overall survival based on changes in PSA at 6 wk, considering response to be ≥30% PSA decline (A) or ≥50% PSA decline (B).
Relationship Between PSA Changes at 6 Weeks and Those After 12 Weeks When ≥50% PSA Decline Was Included as Early PSA Response
Of the 36 patients with PSA progression at 6 wk, 5 underwent an additional imaging-based assessment at 6 wk (as previously described (18)) and discontinued the treatment because of progressive disease; however, 29 of the remaining 31 patients (94%) had PSA progression at 12 wk. All 29 of these patients experienced progressive disease at 12 wk; this condition led to 177Lu-PSMA discontinuation. Of the remaining 2 patients, 1 (3%) had stable PSA at 12 wk and 1 (3%) showed a greater than or equal to 30% decline in PSA at 12 wk. Overall, 1 of 36 patients (3%) with PSA progression at 6 wk (representing 0.8% of the overall cohort) achieved a PSA decline below baseline levels at 12 wk. Patients with PSA progression at 6 wk had a higher likelihood of experiencing PSA progression at 12 wk than patients without early PSA progression (relative risk, 8.7; 95% CI, 4.6–16.3) (P < 0.001). PSA progression at 6 wk had a sensitivity of 93.5% and a specificity of 89.3% for predicting biochemical progression at 12 wk.
Early PSA Changes and Overall Survival
In a landmark analysis at 6 wk, a greater than or equal to 30% decline in PSA at 6 wk was associated with longer overall survival (median, 16.7 mo; 95% CI, 14.4–19.0) than stable PSA (median, 11.8 mo; 95% CI, 8.6–15.1) (P = 0.007) or PSA progression (median, 6.5 mo; 95% CI, 5.2–7.8) (P < 0.001) (Fig. 2A). Patients with a greater than or equal to 30% decline in PSA at 6 wk also had a lower risk of death than patients with stable PSA (hazard ratio [HR], 0.54; 95% CI, 0.33–0.86) (P = 0.01), whereas patients with PSA progression had a higher risk of death than patients with stable PSA (HR, 1.77; 95% CI, 1.11–2.85) (P = 0.01). In the multivariable Cox model including greater than or equal to 30% PSA decline, PSA changes at 6 wk (response: HR, 0.45 [95% CI, 0.25–0.78]; progression: HR, 1.98 [95% CI, 1.11–3.52]), presence of visceral metastases (HR, 1.97; 95% CI, 1.17–3.32), Eastern Cooperative Oncology Group performance status (0 vs. 2: HR, 3.54; 95% CI, 1.36–9.20), time since prostate cancer diagnosis (HR, 0.34; 95% CI, 0.14–0.78), and baseline PSA levels (HR, 1.63; 95% CI, 1.14–2.33) were significantly associated with overall survival (Table 4).
Landmark (Week 6) Multivariable Cox Model for Association with Overall Survival
In brief, a greater than or equal to 50% decline in PSA at 6 wk (median, 19.4 mo; 95% CI, 13.9–24.9) was not significantly associated with longer overall survival than stable PSA (median, 12.6 mo; 95% CI, 10.7–14.6) (P = 0.052) but was significantly associated with PSA progression (median, 6.5 mo; 95% CI, 5.2–7.8) (P < 0.001) (Fig. 2B).
Early PSA Changes and Progression-Free Survival
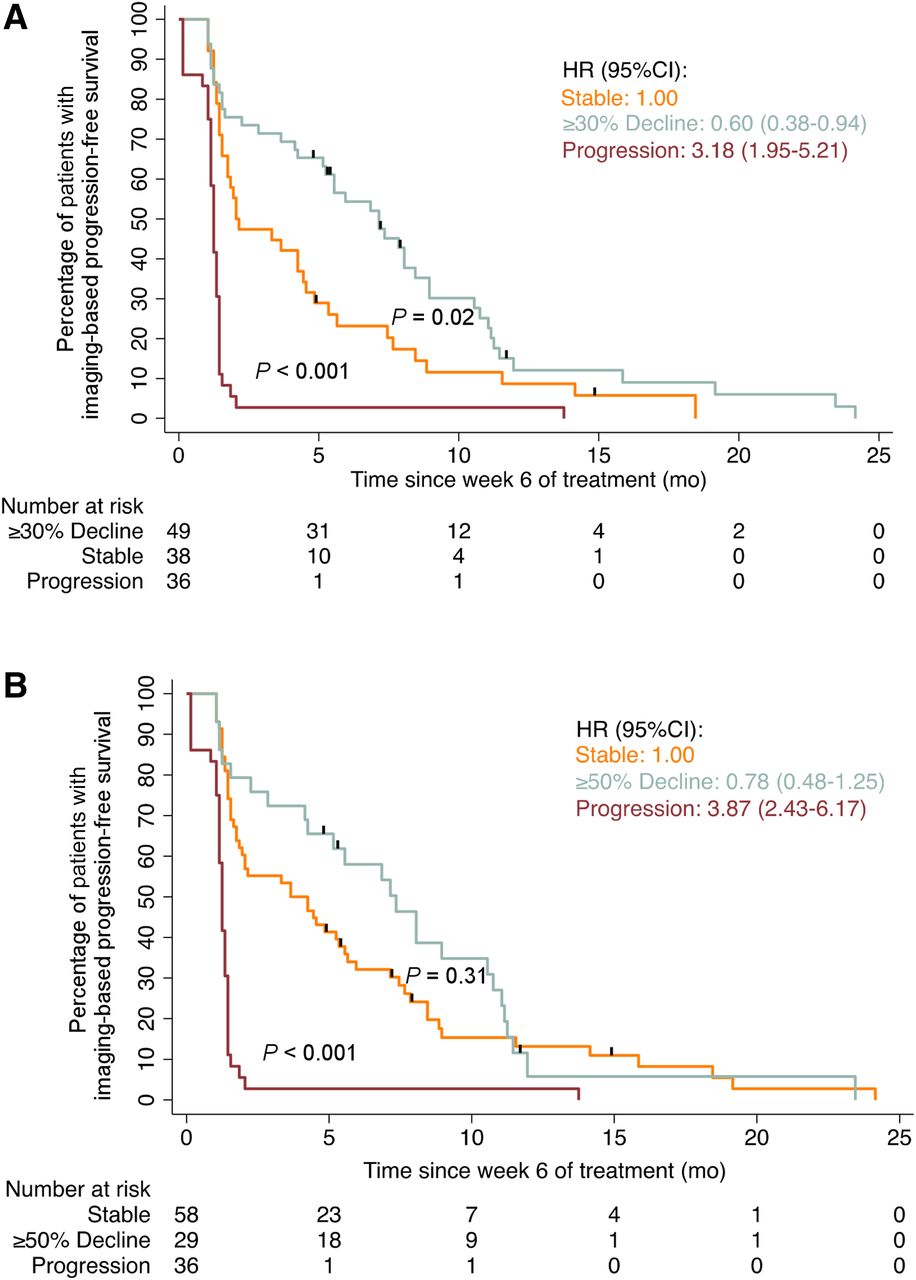
A greater than or equal to 30% decline in PSA at 6 wk was associated with longer imaging-based progression-free survival (median, 7.1 mo; 95% CI, 4.7–9.5) than stable PSA (median, 2.0 mo; 95% CI, 0.1–4.1) (P = 0.01) or PSA progression (median, 1.2 mo; 95% CI, 1.1–1.3) (P < 0.001) (Fig. 3A). Patients with a greater than or equal to 30% decline in PSA at 6 wk also had a lower risk of imaging-based progression than patients with stable PSA (HR, 0.60; 95% CI, 0.38–0.94) (P = 0.02), whereas patients with PSA progression had a higher risk of imaging-based progression than patients with stable PSA (HR, 3.18; 95% CI, 1.95–5.21) (P < 0.001). In the multivariable Cox model including greater than or equal to 30% PSA decline, PSA changes at 6 wk (response: HR, 0.47 [95% CI, 0.28–0.80]; progression: HR, 3.70; 95% CI, 2.09–6.89), chemotherapy status (HR, 1.75; 95% CI, 1.02–3.00), and metastasis status at diagnosis (HR, 1.78; 95% CI, 1.05–3.02) were significantly associated with imaging-based progression-free survival (Table 5).

Kaplan–Meier curves of landmark analysis of imaging-based progression-free survival based on changes in PSA at 6 wk, considering response to be ≥30% PSA decline (A) or ≥50% PSA decline (B).
Landmark (Week 6) Multivariable Cox Model for Association with Imaging-Based Progression-Free Survival
In brief, a greater than or equal to 50% decline in PSA at 6 wk was not significantly associated with longer imaging-based progression-free survival (median: 7.1 mo; 95% CI 4.6–9.6) compared with stable PSA (median: 3.6 mo; 95% CI 1.1–6.1; P = 0.30), but to PSA progression (median: 1.2 mo; 95% CI 1.1–1.3; P < 0.001) (Fig. 3B).
DISCUSSION
In the present retrospective analysis, we found that PSA measurements as early as 6 wk after 177Lu-PSMA initiation were associated with clinical outcome in patients with mCRPC. Most importantly, a 30% PSA decline at 6 wk was associated with longer overall survival than stable PSA or PSA progression. Moreover, PSA flare-up was very uncommon, involving less than 1% of the entire patient population. As the treatment of mCRPC becomes more complex, with evolving definitions of disease progression, improved biomarkers for rapid recognition of resistance are warranted. Rapid treatment discontinuation in patients showing inherent resistance to a drug may have decisive implications for the clinical outcome to the following treatments (19). In a recent study inquiring about specialists′ experience in treating mCRPC outside clinical trials, it was reported that 41.4% of the interviewed physicians disregarded changes in PSA before 12 wk of treatment, making decisions about treatment discontinuation based only on clinical progression (20). Traditionally, an evaluation of PSA changes earlier than 12 wk of treatment has been discouraged (12), since flare reactions have been described in greater than or equal to 20% of patients treated with taxanes (13,21). Unlike data for chemotherapy, our data indicate that an early PSA flare-up, defined as an increase of 25% in the first 6 wk followed by a decline below baseline levels at 12 wk, is very uncommon after 177Lu-PSMA. Only 1 of 36 patients (3%) showing initial PSA progression achieved a PSA decline below baseline levels at 12 wk, involving less than 1% of the entire cohort. Similar results have been reported for new-generation hormonal agents (15,16).
A strategy involving early switching between taxanes on the basis of PSA status at 12 wk has been associated with an improved PSA response rate (TAXYNERGY) versus the results for the historical control (TAX327) (11). In the present study, a 30% or greater decline in PSA at 12 wk was associated with longer overall survival (16.6 mo) than stable PSA (10.7 mo) or PSA progression (5.8 mo) (P < 0.001). Therefore, a switching strategy at 12 wk based on a 30% PSA decrease might identify patients who may or may not further benefit from the therapy and should be further investigated.
Nevertheless, therapies can increase differentiation (and slow progression) of prostate cancer, leading to increasing PSA levels despite reducing tumor volume (22). With this information in mind, current guidelines (12,23) highlight the importance of avoiding sole reliance on PSA measurements during therapeutic assessment and recommend a sufficient window of drug exposure, enabling treatment until there is clear sign of imaging-based or clinical progression. However, we found that 94% of patients showing PSA progression at 6 wk after 177Lu-PSMA initiation developed imaging-based progression within 12 wk, resulting in treatment discontinuation. In addition, patients who had a 25% PSA increase at 6 wk had shorter survival and were 8.7 times more likely to show biochemical progression at 12 wk. These results may be of clinical relevance, especially in a scenario in which 177Lu-PSMA is administered at an earlier stage of mCRPC, with other therapeutic options still being available. In addition to the ongoing phase 3 clinical trial investigating the efficacy of 177Lu-PSMA versus the best standard of care (VISION; ClinicalTrials.gov identifier: NCT03511664), 177Lu-PSMA versus cabazitaxel (second-line chemotherapy) is also being investigated in a phase 2 randomized trial (TheraP; ClinicalTrials.gov identifier: NCT03392428). These clinical trials might enable drug approval and the possibility of 177Lu-PSMA being offered as a third-line or even second-line treatment for mCRPC. Positive results regarding the long-term outcome for patients treated with 177Lu-PSMA in a phase 2 clinical trial were recently reported (24).
One previous study found a PSA decline of at least 20.9% after 1 cycle of 177Lu-PSMA to be independently associated with longer overall survival (25). However, the clinical utility of this definition is limited because this cutoff was derived by fitting a retrospective receiver operating characteristic curve analysis. In other retrospective analyses, the lack of a 30% PSA decline after the first therapy cycle with 177Lu-PSMA was associated with shorter survival (9,26). However, in corresponding multivariate analyses, only the presence of visceral metastases and elevated lactate dehydrogenase levels remained independent predictors for overall survival. In the multivariable Cox model in the present study, PSA changes at 6 wk were independently associated with overall survival along with other variables (presence of visceral metastases, Eastern Cooperative Oncology Group performance status, time since diagnosis of prostate cancer, and baseline PSA levels). For patients with an insufficient response to 177Lu-PSMA, 2 modified treatment regimens have been proposed for an improved therapeutic outcome: accelerated administration at intervals of 4 wk (currently 6–8 wk) and a dose escalation strategy (27). However, these 2 regimens might not improve treatment efficacy in patients showing inherent drug resistance, with possibly high toxicity levels. Thus, patients showing an initial high sensitivity to 177Lu-PSMA (>30% PSA decrease at 6 wk) are most likely to experience a clinical benefit from any of these proposed regimens.
Imaging-based progression-free survival (often termed “radiographic progression-free survival”) has been commonly used as a primary/coprimary endpoint in phase 3 clinical trials for mCRPC, being significantly associated with overall survival (28). In our analysis, the PSA response at 6 wk was significantly associated with longer imaging-based progression-free survival (median, 8.4 mo) than stable PSA (3.3 mo) or PSA progression (2.5 mo). Similar to the results for overall survival, PSA changes at 6 wk were significantly associated with imaging-based progression-free survival along with other variables (chemotherapy status and presence of distant metastases at diagnosis).
We found that a 50% decline in PSA at 6 wk showed a clear trend toward improved survival; however, in contrast to a 30% decline in PSA, it failed to be associated with longer survival. At first glance, this finding appears paradoxical; intuitively, a greater PSA decline should be associated with a stronger antitumor effect. However, the inability to establish the association of early PSA measurements with clinical outcome at higher rates of PSA declines may reflect the fact that fewer patients achieved higher-percentage PSA declines, leading to a reduction in statistical power. In the present study, at 6 wk after 177Lu-PSMA treatment, 24% of patients had PSA declines of greater than 50%, whereas 40% of patients had PSA declines of greater than 30%. However, other studies testing PSA changes at 12 wk for surrogacy found similar results, with a 50% decline in PSA failing to meet the surrogacy criteria, whereas a 30% decline did (7).
The present study has several limitations. First, because of its retrospective nature and single-center experience, the findings of the present study need to be further evaluated in a prospective multicenter setting. Second, current guidelines recommend the use of bone scanning and CT for imaging-based assessment (12), whereas in the present study, patients were evaluated using hybrid PSMA-targeted PET/CT. The fact that PSMA-targeted PET showed a higher sensitivity than conventional imaging techniques might result in a bias toward shorter imaging-based progression-free survival (29).
Compared with taxanes, new-generation hormonal agents as well as 177Lu-PSMA seem to have a different impact on PSA kinetics, with flare reactions being rare. After a prospective validation, these findings should be considered in future guidelines for mCRPC.
CONCLUSION
PSA changes at 6 wk after 177Lu-PSMA initiation are an early indicator of long-term clinical benefit for both overall survival and imaging-based progression-free survival. Patients with PSA progression after 6 wk of treatment could benefit from a very early decision to switch treatment, resulting in a decrease in overtreatment. PSA flare-up during 177Lu-PSMA treatment is very uncommon. Prospective studies are now warranted to validate our findings and potentially inform clinicians earlier on the effectiveness of 177Lu-PSMA.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Are PSA changes after 6 wk of treatment with 177Lu-PSMA associated with clinical outcome in patients with mCRPC?
PERTINENT FINDINGS: In a retrospective study including 124 patients, PSA progression after 6 wk of 177Lu-PSMA treatment was associated with shorter overall survival and progression-free survival than PSA response and stable PSA. Overall, only 3% of patients with PSA progression at 6 wk achieved any PSA decline at 12 wk (1% of the entire cohort).
IMPLICATIONS FOR PATIENT CARE: Patients with PSA progression after 6 wk of 177Lu-PSMA treatment could benefit from a very early decision to switch treatment, resulting in a decrease in overtreatment; PSA flare-up during 177Lu-PSMA treatment is very uncommon.
Footnotes
Published online Feb. 28, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 2, 2019.
- Accepted for publication February 6, 2020.





{kind=link}
{kind=link}
{kind=link}