


Abstract
We retrospectively evaluated the utility of 68Ga-PSMA-11 PET for planning 223RaCl2 therapy of patients with metastatic prostate cancer and its impact on the therapeutic response as determined by prostate-specific antigen (PSA) and alkaline phosphatase (ALP), as well as the correlation of PSA changes with the results of prostate-specific membrane antigen (PSMA) PET follow-up scans. Methods: Sixty-three patients with a median age of 73 y who underwent 307 cycles of therapy with 223RaCl2 were analyzed. In 31 patients, bone scanning and radiologic imaging were performed for pretherapeutic imaging (group 1). In 32 patients, bone scanning and PSMA PET were performed before therapy (group 2). Patients with small lymph node metastases and local recurrence were not excluded from treatment, consistent with current guidelines. PSA and ALP were measured before each treatment cycle and 4 wk after the final cycle. Thirteen patients from group 2, who underwent a second PSMA PET scan as a follow-up, were evaluated to determine the significance of PSA changes as a follow-up marker. Results: In group 1, 4 patients (12.9%) showed a PSA decline, of whom 2 patients and 1 patient showed a PSA decline of more than 30% and more than 50%, respectively. In contrast, in group 2, 14 patients (43.8%) showed a PSA decline, of whom 10 and 8 patients showed a decline of more than 30% and more than 50%, respectively (P = 0.007). Thirty-seven patients had a high ALP level (19 from group 1 and 18 from group 2). Twelve (63.2%) and 16 (88.9%) patients in groups 1 and 2, respectively, showed an ALP decline. This difference was not significant; however, 7 (36%) and 13 (72.2%) patients in groups 1 and 2, respectively, showed an ALP decline of more than 30% (P = 0.04). Considering any ALP decline as a response, no patient with increasing ALP showed a PSA response (P = 0.036). There was a significant correlation between the PSA changes and the therapeutic response according to follow-up PSMA PET. Conclusion: When PSMA PET is used as the gatekeeper in addition to bone scanning, radionuclide therapy with 223Ra may be more effective and have more success regarding changes in the PSA. An increase in PSA during therapy cycles occurs because of disease progression.
Although different β-emitters, such as 153Sm, 188Re, and 82Sr (1), have been used for many years for the treatment of bone metastases of prostate cancer (PC), 223Ra-dichloride (223Ra; Xofigo) is the first α-emitting radiopharmaceutical agent approved for the treatment of patients with symptomatic bone metastases without visceral metastases that has been shown to improve overall survival. It has also been shown to delay skeletal-related events (2–5) and is recommended by international guidelines (6–8). Prostate-specific antigen (PSA) is the most important PC-related biomarker for the evaluation of therapeutic response in many studies (9–11); however, during therapy cycles with 223Ra, several patients show a continuous PSA increase, which may be interpreted as therapy-induced. Thus, regarding therapy for bone metastases using 223Ra, the Prostate Cancer Working Group recommends basing the decision to discontinue treatment on clinical symptomatology and therapeutic tolerability as well as on radiographic progression, not solely on PSA kinetics (12). Therefore, it is recommended that patients receive all 6 cycles of 223Ra, which is the recommended treatment course to achieve an overall survival benefit (13,14). Bone scintigraphy should precede radionuclide therapy with 223Ra for the evaluation of eligible candidates. The existence of any visceral metastasis is a contraindication for 223Ra therapy. Bone marrow involvement should also be a contraindication, which cannot be diagnosed using bone scanning or CT. Presently, at least in central Europe, 68Ga-PSMA-11 PET (PSMA PET; PSMA is prostate-specific membrane antigen) is increasingly performed for PC, with a high diagnostic sensitivity and specificity (15–19). PSMA PET should also precede radioligand therapy with 177Lu-PSMA (20). In our recently published study, we showed a significant correlation between PSA changes and the degree and number of PSMA-expressing lesions in patients treated by 177Lu-PSMA (21), which confirms the value of PSA as a follow-up marker. Compared with PSA, alkaline phosphatase (ALP) may be a better biomarker to evaluate treatment response (3,5,13); however, as a marker, it is only useful in patients with high ALP levels. ALP also has prognostic potential in metastatic PC treated with 223Ra (3). For the planning of therapy with 223Ra, to rule out visceral metastases as well as bone marrow involvement, we recommend PSMA PET in addition to bone scintigraphy; however, this cannot be performed routinely in our department because of reimbursement issues. In this study, we retrospectively evaluated the utility of PSMA PET for therapy planning and its influence on the therapeutic response measured by PSA and ALP. We also evaluated the significance of PSA changes in correlation with the results of PSMA PET, acquired as a follow-up scan.
MATERIALS AND METHODS
Patient Population
Three-hundred fifty-three cycles of 223Ra were performed for 80 castration-resistant PC (CRPC) patients between March 2014 and March 2016 in the Department of Nuclear Medicine (University Hospital Bonn). For this retrospective analysis, patients with at least 2 cycles of 223Ra and with at least 1 follow-up examination 4 wk after the last cycle were included. The local ethics committee approved this retrospective study, and all subjects signed a written informed consent form.
Patient Preparation
All patients underwent bone scintigraphy before the first cycle. The patients were divided into 2 groups. Group 1 included patients with routine staging using abdominal and chest CT in addition to pretherapeutic bone scintigraphy; patients with large or extensive lymph node metastases or visceral metastases had been excluded before referral to our department. These patients were treated with chemotherapy, 177Lu-PSMA, or best supportive care. Group 2 included patients who received PSMA PET/CT for staging as well as bone scintigraphy. Two patients from group 1 with a superscan in bone scintigraphy were excluded from the analysis because of the poor prognosis and response in this group of patients.
According to pretherapeutic PSMA PET, patients with bone marrow involvement, large lymph node metastases (>2 cm), or extensive lymph node metastases and visceral metastases did not receive therapy with 223Ra.
Bone Scintigraphy
Whole-body bone scintigraphy was performed 2 h after an intravenous injection of a mean of 650 MBq of 99mTc-methylene diphosphonate using a double-head γ-camera system (Symbia T2; Siemens Medical Solutions).
68Ga-PSMA-11 PET/CT
68Ga-PSMA-11 was applied via slow intravenous injection (30–60 s) using a weight-adapted dose of 2 MBq/kg of body weight in a total volume of 5–10 mL (diluted with 0.9% sterile sodium chloride solution). The average injected dose was 140 MBq. PET/CT images were obtained on a Biograph 2 PET/CT scanner on average 77 min after injection. First, low-dose CT (16 mAs, 130 kV) was performed from the base of the skull to mid thigh. The PET scan was acquired over the same area. CT data were reconstructed in 512 × 512 matrices with a slice thickness of 5 mm. PET data were reconstructed in 128 × 128 matrices with a slice thickness of 5 mm using an attenuation-weighted ordered-subsets expectation maximization algorithm and performing attenuation and scatter correction as implemented by the manufacturer.
Comparison of PSMA PET with Bone Scintigraphy
In group 2, the comparison of the 2 modalities was performed visually. To simplify the process, we classified the patients into 2 subgroups: PET > bone scan, including patients with lymph node metastases, local recurrence, and focal bone marrow involvement, and PET ≤ bone scan, including patients with a higher number of bone lesions in the bone scan or patients with the same tumor involvement in both scans. Small bone lesions, especially small rib metastases, which could be detected only using PSMA PET, were not considered for the comparison.
Follow-up PSMA PET in Group 2
Of the patients in group 2, 13 underwent a second PSMA PET scan as well as bone scintigraphy for restaging. The results of these scans were correlated with PSA changes.
Radionuclide Therapy with 223Ra
223Ra was administered intravenously. Each patient received 50 kBq per kg of whole-body weight every 4 wk. Patients were counseled before each cycle regarding the possible adverse effects and radiation safety according to the rules of the Federal Office for Radiation Protection in Germany (BfS).
Data Collection and Follow-up
On each treatment day, hematologic and renal status, tumor markers (PSA), and ALP were assessed in all patients. Laboratory examinations were performed in all patients for at least up to 4 wk after the last cycle.
Tumor Response Evaluation
The tumor marker PSA was used as the main marker for the response evaluation. The response was defined as any decline in the PSA level 4 wk after the last cycle compared with the baseline PSA; however, the number of patients with a PSA decline of >30% and >50% were determined as well. Any increase in the PSA level measured 4 wk after the last cycle was considered to indicate disease progression. We also compared the percentage changes in ALP in the patients of both groups who had an ALP > 117 U/L (the reference range in our clinic is 34–117 U/L). Here, any decline in ALP as well as a >30% decline were used. The PSMA PET images were evaluated as follows: partial response, >30% reduction in PSMA expression in the target lesions; progressive disease, >30% increase in PSMA expression in the target lesions or developing new lesions; and stable disease, <30% change in PSMA expression. Up to 5 bone and lymph node metastases in each patient were selected as target lesions.
Statistical Analysis
Variables in both groups were compared using the Student t test for continuous variables and the χ2 or Fisher exact test for categoric variables. Data were analyzed using SPSS software (SPSS 20.0 for Windows; SPSS).
RESULTS
Fifty-one patients underwent PSMA PET for the evaluation of 223Ra therapy, of whom 19 patients (37.3%) were not eligible for this therapy because of the abovementioned reasons (Fig. 1). Of our 80 treated patients, 63 with a median age of 73 y (range, 52–84 y) met the inclusion criteria of this retrospective study; these patients underwent 307 cycles of 223Ra. Thirty-one patients with a median age of 74 y (range, 52–83 y) were in group 1, and 32 patients with a median age of 73 y (range, 62–84 y) were in group 2. There were no significant differences between groups regarding different pretherapeutic parameters or the number of cycles (Table 1). In group 2, 13 patients were classified as PET ≤ bone scan and 19 as PET > bone scan, of whom 10 of 19 showed focal bone marrow involvement; 3 of 19 showed small lymph node metastases as well as focal bone marrow involvement; 3 of 19 showed local recurrence as well as lymph node metastases; and 3 of 19 showed local recurrence, small lymph node metastases, and focal bone marrow involvement.

A 72-y-old patient with hormone- and chemorefractory PC who underwent bone scintigraphy (A, ventral view; B, dorsal view) was referred for 223Ra therapy. PSMA PET/CT (C) showed diffuse bone and bone marrow metastases, most not detectable by bone scan. Apart from bone metastases, there were many lymph node metastases, for example, mediastinal and left clavicular (pink arrows). PSA level at time of PET imaging was 630 ng/mL, ALP in reference range. Patient underwent radioligand therapy with 177Lu-PSMA-617.
Pretherapeutic Parameters in Both Groups
Therapeutic Response According to PSA Changes
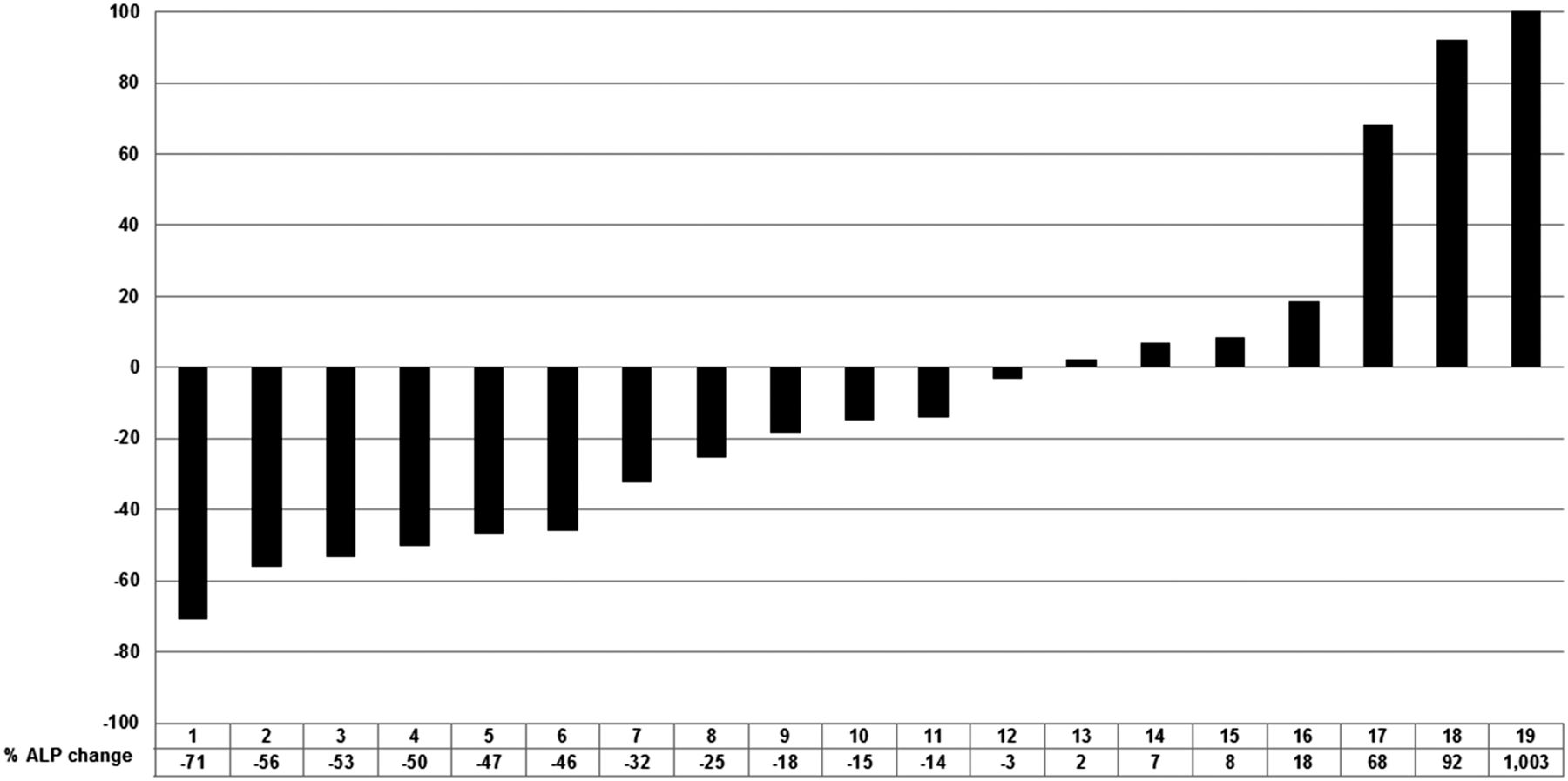
In group 1, 4 patients (12.9%) showed PSA decline, of whom 2 patients (6.4%) and 1 patient (3.2%) showed a PSA decline of >30% and >50%, respectively (Fig. 2). In contrast, in group 2, 14 patients (43.8%) showed a PSA decline, of whom 10 (32.2%) and 8 patients (25%) showed a decline of >30% and >50%, respectively (P = 0.007) (Fig. 3). In group 2, in the PET > bone scan subgroup, 6 patients (31.6%) showed a PSA decline, whereas in the PET ≤ bone scan subgroup, 9 patients (69.2%) showed a PSA decline (P = 0.04) (Fig. 4). Of the patients who showed a PSA response in group 1 and group 2, 3 patients received abiraterone with 223Ra and 3 patients received entzalutamide with 223Ra concurrently, respectively. In these patients, we could not clearly differentiate between the success of hormone therapy or radionuclide therapy or both of them together.
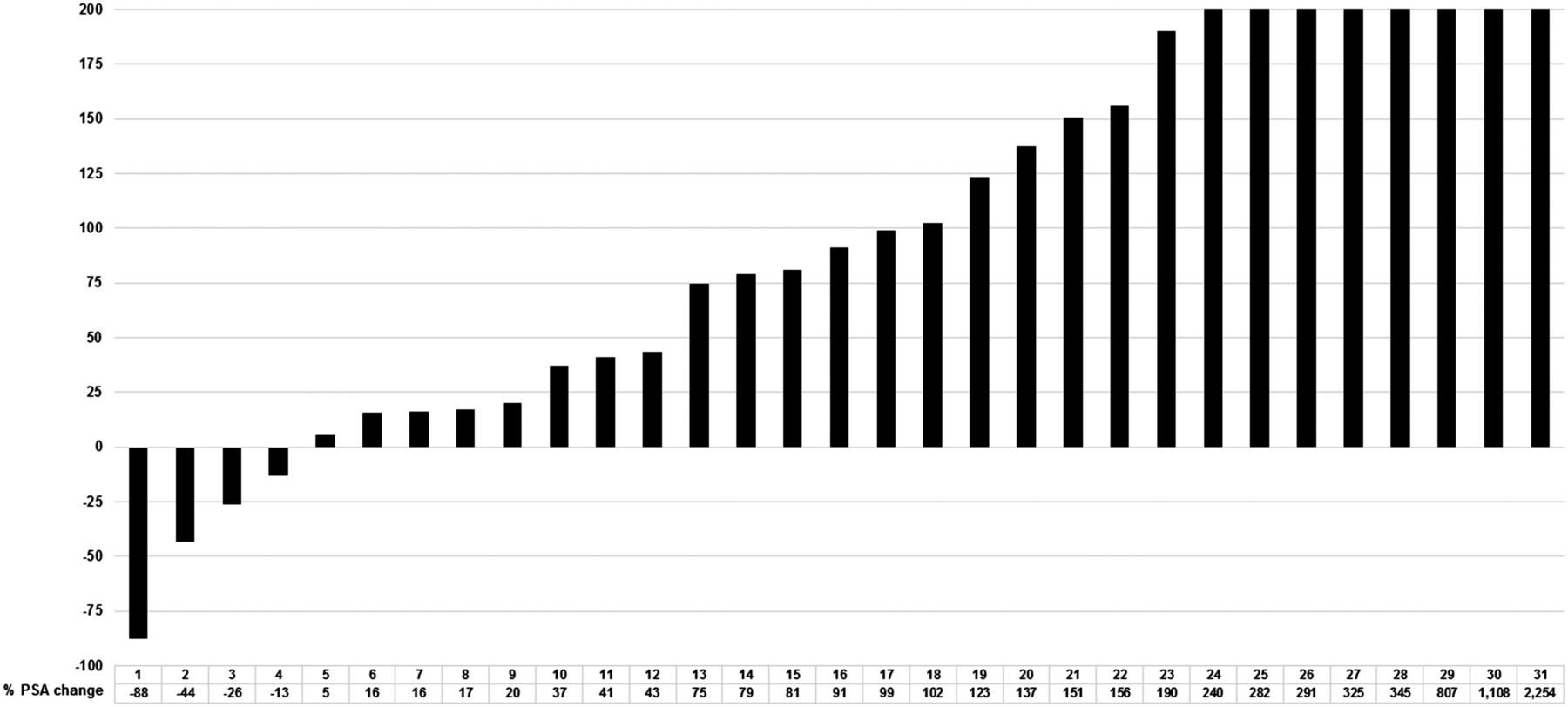
Waterfall plot showing percentage PSA change in group 1 from baseline at 4 wk after last cycle in 31 patients.
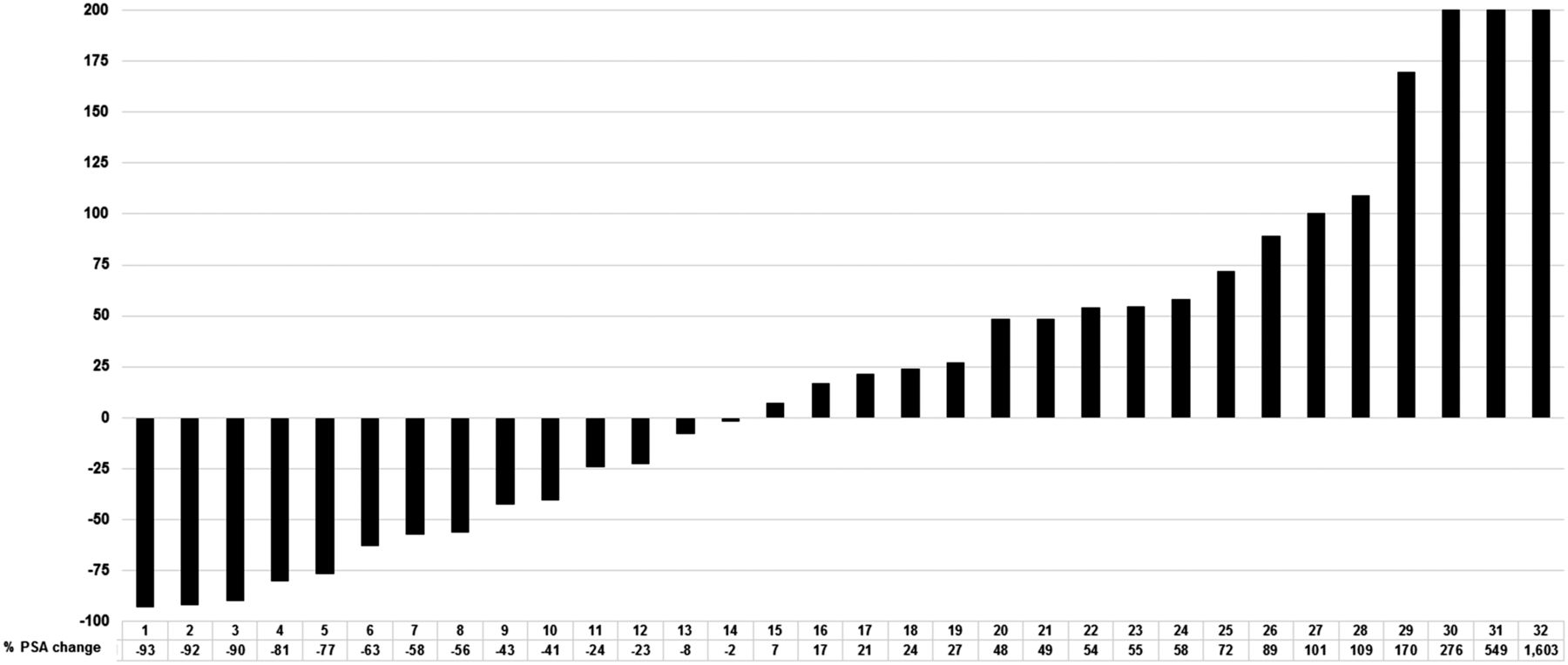
Waterfall plot showing percentage PSA change in group 2 from baseline at 4 wk after last cycle in 32 patients.
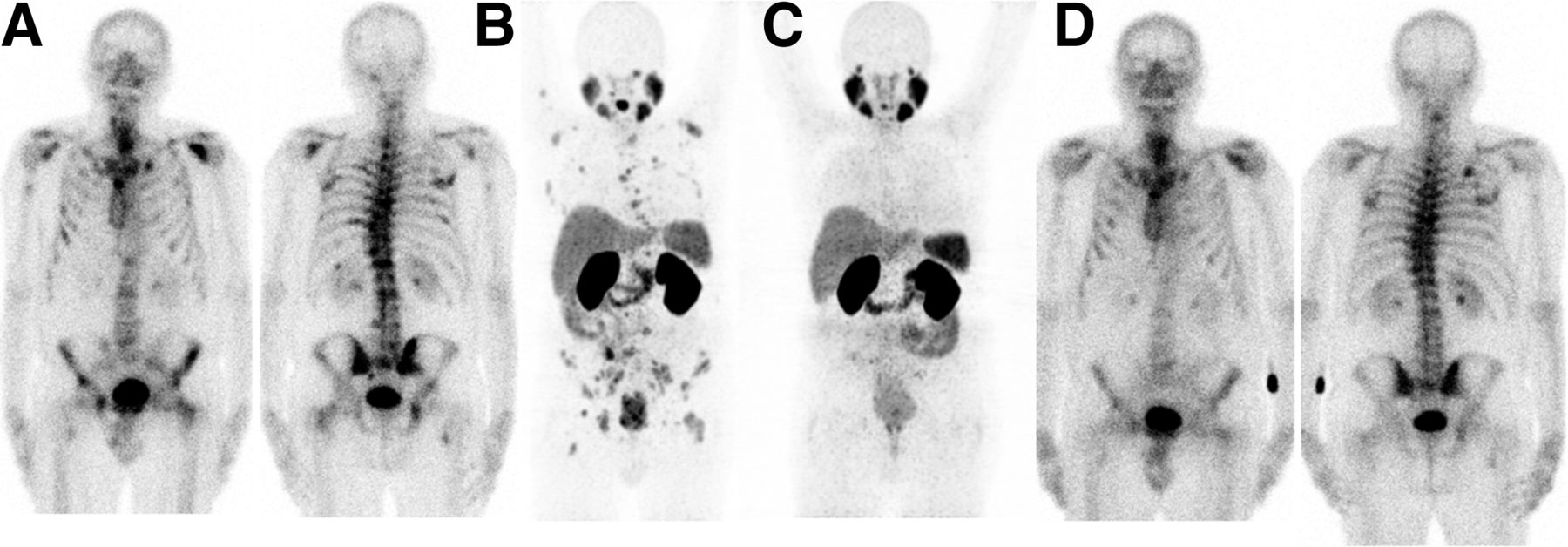
A 69-y-old patient with hormone-refractory PC (Gleason score, 8) from group 2 (PET ≤ bone scan) who underwent bone scintigraphy (A) was referred for 223Ra therapy. PSMA PET/CT (C) showed diffuse bone metastases concordant to bone scintigraphy. PSA level at time of PET imaging was 30 ng/mL, and ALP was 207 U/L. Patient underwent 6 cycles of therapy with 223Ra therapy and showed 4 wk later near-complete response in PET (C) and partial response in bone scintigraphy (D). PSA and ALP decreased to 2.95 ng/mL and 98 U/L, respectively.
Therapeutic Response According to ALP Changes in Patients with High ALP Levels
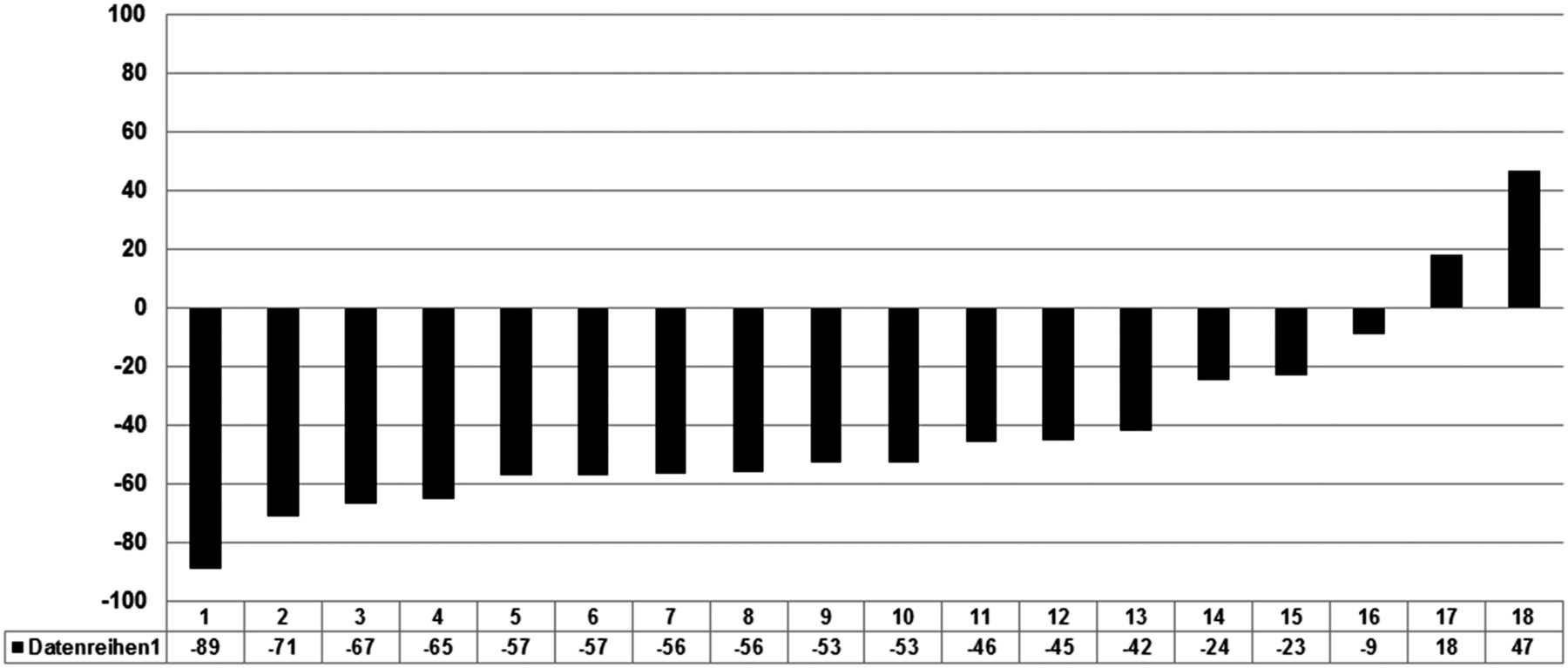
Thirty-seven patients had a high ALP level (19 in group 1 and 18 in group 2; P = nonsignificant). Twelve (63.2%) and 16 (88.9%) patients in group 1 and group 2, respectively, showed an ALP decline. This difference was not significant; however, 7 (36%) and 13 (72.2%) patients in group 1 and group 2, respectively, showed an ALP decline of >30% (P = 0.04) (Figs. 5 and 6). Considering any ALP decline as a response, no patient with increasing ALP showed a PSA response (P = 0.036), and considering an ALP decline of >30% as a response, only 1 patient (5.8%) showed a PSA response without an ALP decline of >30% (P = 0.01) (Table 2).
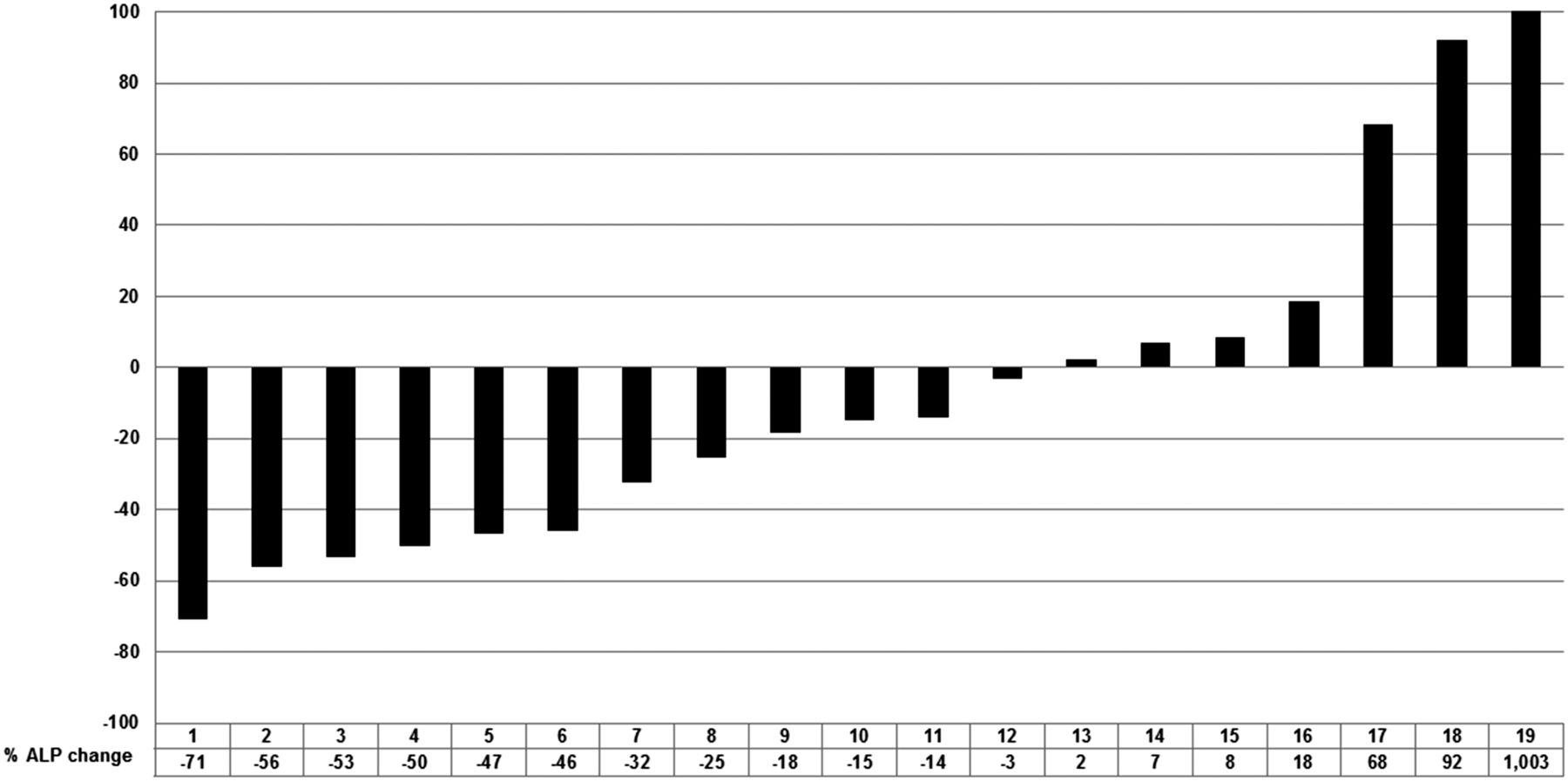
Waterfall plot showing percentage ALP change in group 1 from baseline at 4 wk after last cycle in 19 patients with high ALP level at baseline.

Waterfall plot showing percentage ALP change in group 2 from baseline at 4 wk after last cycle in 18 patients with high ALP level at baseline.
Therapeutic Response According to PSA and ALP Changes in Patients with High ALP Level at Baseline
Correlation Between PSMA PET and PSA Changes
Thirteen patients in group 2, who at the time of this study received a second PSMA PET scan, were evaluated to determine the significance of PSA changes as a follow-up marker. Eleven of them underwent a second PSMA PET scan 4 wk after the sixth cycle of 223Ra, and 2 patients underwent the second PSMA PET scan 4 wk after the third cycle because of a PSA increase and the request of the patient to discontinue therapy. According to PSMA PET, 8, 4, and 1 patients showed progressive disease, partial response, and stable disease, respectively, whereas 4 patients experienced a PSA decline and 9 a PSA increase. There was a significant correlation between PSA changes and the therapeutic response according to the follow-up PSMA PET (P = 0.002). Detailed information of these 13 patients with the reason for disease progression is provided in Table 3.
Thirteen Patients Who Underwent Second PSMA PET as Follow-up Scan
DISCUSSION
In addition to docetaxel, which until 2010 was the only drug with a positive impact on overall survival, in recent years, 223Ra and 4 other new drugs (abiraterone, enzalutamide, sipuleucel-T, and cabazitaxel) have shown efficacy in prolonging the survival of CRPC patients (10,13,22–25). 223Ra is recommended as a first-line treatment in metastatic CRPC (6–8).
Etchebehere et al. showed that concomitant use of abiraterone and 223Ra seems to have a beneficial effect (26). Currently, several clinical trials are evaluating the safety and efficacy of 223Ra combined with abiraterone (NCT02043678) and enzalutamide (NCT02194842). Apart from these approved therapies, radioligand therapy with 177Lu-PSMA has shown a high therapeutic response rate in CRPC patients in a salvage situation, and it may have a positive impact on overall survival as well (20,21,27–32). These therapeutic options raise the need for accurate therapy planning and selection of patients who are eligible for 1 therapy or a combination of some of them.
CT and bone scanning are the recommended imaging modalities to monitor the response to therapy in patients with skeletal metastases. The National Comprehensive Cancer Network recommends adding choline PET/CT to bone scanning or 18F-fluoride PET/CT (33). Skeletal imaging with 18F-fluoride PET/CT is superior to bone scintigraphy in metastatic PC patients because of greater sensitivity, specificity, and accuracy (26,34). Bone scintigraphy or 18F-fluoride PET/CT should precede therapy with 223Ra to determine active osteoblastic lesions, because the regional uptake of 223Ra correlates with the intensity of bone metabolism (35).
In contrast to the ALSYMPCA trial, in which the bone scan response to treatment with 223Ra was not evaluated, there are some studies that have focused on the utility of bone scans (scintigraphy and PET) to assess the response and toxicity associated with this therapy (36–38). In recent years, PSMA PET/CT has been making ground-breaking changes in the diagnosis and staging of PC patients, and this imaging modality is superior to choline PET (16,18,39,40). PSMA is a type II transmembrane protein with glutamate-carboxypeptidase activity. It is highly expressed on prostate epithelial cells and is strongly upregulated in PC. The levels of PSMA expression are directly correlated with metastases, androgen independence, and progression of PC (41). The detection rate of PSMA PET/CT depends on the PSA level and is 96.8%, 93.0%, 72.7%, and 57.9% for PSA levels of >2, 1 to <2, 0.5 to <1, and 0.2 to <0.5 ng/mL, respectively (19).
Although PSMA PET cannot replace bone scintigraphy or 18F-fluoride PET/CT for detecting active osteoblastic lesions, PSMA PET/CT may help with better treatment planning, that is, to rule out patients with small undetected visceral metastases and bone marrow involvement as well as for the planning of therapy combinations (e.g., enzalutamide + 223Ra in patients with bone and lymph node metastases). The concurrent use of 223Ra with chemotherapy is currently not recommended; however, the concomitant use of these treatments in selected patients seems to be safe and beneficial (36).
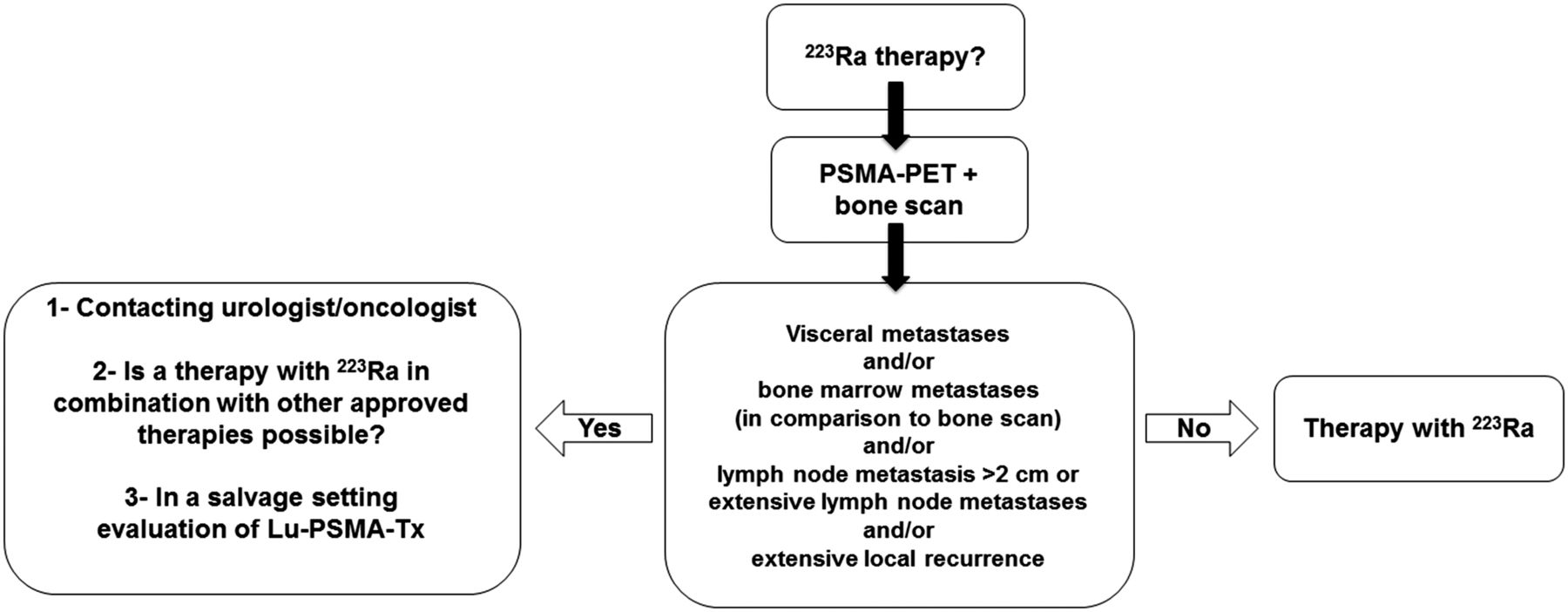
Our therapeutic approach using PSMA PET/CT as a gatekeeper for 223Ra is shown in Figure 7. However, because of reimbursement issues in Germany, it is not always possible to perform PSMA PET/CT on all patients in our department. In this study, to prove this concept, we compared 2 groups of PC patients who underwent 223Ra therapy. Patients in group 2 showed a significantly better response according to the decline in PSA levels 4 wk after the last cycle than patients in group 1. In a subgroup analysis of patients in group 2, 31.6% of patients who were classified in the subgroup PET > bone scan showed a PSA decline, whereas in the PET ≤ bone scan subgroup, 69.2% showed a PSA decline (P = 0.04). The main reason for a less favorable response in the PET > bone scan group is the progression of lymph node and bone (/marrow) metastases. The significant differences between these 2 groups and between the subgroups of group 2 demonstrate the benefit of PSMA PET/CT in terms of better patient selection. It demonstrates that, in well-selected patients, a PSA decline can be expected in patients with a therapeutic response.

Treatment planning approach in Department of Nuclear Medicine, University Hospital Bonn, for therapy with 223Ra according to results of PSMA PET and bone scintigraphy.
The Prostate Cancer Working Group pays little attention to PSA changes during and after therapy cycles; however, there was a significant correlation between PSA changes and the treatment response according to PSMA PET/CT images (P = 0.002) (Table 3), which increases the value of PSA as a reliable tumor marker for the follow-up of PC patients. According to our data, there is always an explanation for a rise in PSA. The ALSYMPCA trial was done at a time when PSMA PET/CT was not available in many countries or was not done routinely. We do not know what the outcome would have been regarding PSA results and overall survival if the patients in this study had been selected precisely by excluding patients with small visceral metastases, bone marrow involvement, and other soft-tissue metastases. We have to emphasize that, at the time of the ALSYMPCA study, 177Lu-PSMA therapy did not rank among the therapies used for metastatic PC. However, we now have this option.
Because therapy with 223Ra is recommended as a first-line therapy for symptomatic bone metastatic CRPC without visceral metastases, it could be indicated for patients with bone metastases and extensive lymph node metastases by combining radionuclide therapy with abiraterone or enzalutamide. In patients who should be evaluated for therapy with 223Ra in a salvage setting, therapy with 177Lu-PSMA in patients with soft-tissue metastases may be another alternative.
Changes in the ALP value are often used as a marker for treatment follow-up, because ALP may reflect the extent of bone disease more accurately than PSA levels (38). In the ALSYMPCA trial, a significantly higher proportion of patients showed a response according to the ALP level in the 223Ra group than in the placebo group (≥30% reduction, P < 0.001). In our study, 36% of the patients in group 1 and 72.2% of the patients in group 2 showed a significant ALP decline.
On the basis of the results of this retrospective study, we have observed a better therapeutic response in patients who underwent PSMA PET/CT as a gatekeeper for 223Ra therapy, which was because of better patient selection, mainly with the exclusion of patients with bone marrow involvement. These results should be confirmed by planning prospective studies with more patients. Future studies have to evaluate the importance and value of PSA and ALP as well as PSMA PET as follow-up markers in patients undergoing 223Ra therapy.
CONCLUSION
When PSMA PET is used as a gatekeeper, radionuclide therapy with 223Ra may be more effective and have more success regarding changes in the PSA level. An increase in the PSA level during therapy cycles likely occurs because of disease progression.
DISCLOSURE
Markus Essler received financial support to attend a DGN symposia from Bayer. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We are grateful to the nursing staff of the treatment ward in our department. We give special thanks to our study nurse, Ulrike Kuhn-Seifer (Department of Nuclear Medicine Bonn).
Footnotes
↵* Contributed equally to this work.
Published online Sep. 22, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 19, 2016.
- Accepted for publication August 29, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Impact of Baseline PSMA PET/CT Versus CT on Outcomes of 223Ra Therapy in Metastatic Castration-Resistant Prostate Cancer Patients
- 68Ga-PSMA PET/CT for Response Evaluation of 223Ra Treatment in Metastatic Prostate Cancer
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer
- Effect of External Cooling on 177Lu-PSMA Uptake by the Parotid Glands
- 223Ra Therapy of Advanced Metastatic Castration-Resistant Prostate Cancer: Quantitative Assessment of Skeletal Tumor Burden for Prognostication of Clinical Outcome and Hematologic Toxicity
- Reply: Regarding "18F-GP1, a Novel PET Tracer Designed for High-Sensitivity, Low-Background Detection of Thrombi"
- More {alpha} Than {beta} for Prostate Cancer?