


Abstract
68Ga-PSMA (prostate-specific membrane antigen) PET/CT is increasingly used in men with prostate-specific antigen (PSA) failure after radical prostatectomy (RP) to triage those who will benefit from salvage radiation treatment (SRT). This study examines the value of PSMA-informed SRT in improving treatment outcomes in the context of biochemical failure after RP. Methods: We analyzed men with rising PSA after RP with PSA readings between 0.05 and 1.0 ng/mL, considered eligible for SRT at the time of PSMA. For each patient, clinical and pathologic features as well as scan results, including site of PSMA-positive disease, number of lesions, and a certainty score, were documented. Subsequent management, including SRT, and most recent PSA were recorded using medical records. Treatment response was defined as both PSA ≤ 0.1 ng/mL and >50% reduction in PSA. Multivariate logistic regression analysis was performed for association of clinical variables and treatment response to SRT. Results: One hundred sixty-four men were included. PSMA was positive in 62% (n = 102/164): 38 of 102 in the prostatic fossa, 41 of 102 in pelvic nodes, and 23 of 102 distantly. Twenty-four patients received androgen-deprivation therapy (ADT) and were excluded for outcomes analysis. In total, 99 of 146 received SRT with a median follow-up after radiation treatment of 10.5 mo (interquartile range, 6–14 mo). Overall treatment response after SRT was 72% (n = 71/99). Forty-five percent (n = 27/60) of patients with a negative PSMA underwent SRT whereas 55% (33/60) did not. In men with a negative PSMA who received SRT, 85% (n = 23/27) demonstrated a treatment response, compared with a further PSA increase in 65% (22/34) in those not treated. In 36 of 99 patients with disease confined to the prostate fossa on PSMA, 81% (n = 29/36) responded to SRT. In total, 26 of 99 men had nodal disease on PSMA, of whom 61% (n = 16/26) had treatment response after SRT. On multivariate logistic regression analysis, PSMA and serum PSA significantly correlated with treatment response, whereas pT stage, Gleason score, and surgical margin status did not. Conclusion: PSMA PET is independently predictive of treatment response to SRT and stratifies men into a high treatment response to SRT (negative or fossa-confined PSMA) versus men with poor response to SRT (nodes or distant-disease PSMA). In particular, a negative PSMA PET result predicts a high response to salvage fossa radiotherapy.
- prostate specific membrane antigen
- PSMA
- PET/CT
- treatment outcome
- biochemical failure
- post radical prostatectomy
See an invited perspective on this article on page 1969.
Radical prostatectomy (RP) is the most widely used treatment for men with localized prostate cancer (PC). After surgery, patients are monitored with serial prostate-specific antigen (PSA) measurements. Approximately 20%–50% of pT2–3, node-negative PC patients treated with RP will experience biochemical recurrence, particularly those with poorly differentiated disease and positive surgical margins. Salvage radiation treatment (SRT) to the prostatic fossa (or fossa + pelvic nodes in higher risk patients) is the only potentially curative treatment option for patients with biochemical failure after RP. The 5-y progression-free survival rate in patients undergoing salvage radiation treatment (RT) is 56%, varying from 71% in men with pre-RT PSA level of less than 0.01–0.2 ng/mL, down to 18% in men with a PSA greater than 1.5 ng/mL undergoing SRT without androgen-deprivation therapy (ADT) (1–4). This indicates that men with low-volume recurrent PC benefit the most from SRT; and that there are a significant number of patients who do not show a lasting PSA response after salvage. Because SRT is only clinically useful in patients with local disease (disease confined to the fossa), and because SRT is related to significant disadvantages in treatment-related quality of life, patients with tumor spread outside the prostatic fossa should ideally be excluded when selecting patients for prostatic fossa–only SRT. Postoperative conventional imaging techniques such as transrectal ultrasound, MRI, CT, and bone scanning are neither sensitive nor specific enough to detect recurrent PC at an early stage where SRT may be curative. Recent publications have reported PSMA PET/CT identifying disease outside the prostate fossa in 28%–43% of men with a rising PSA after RP (5–7). These findings have led to significant changes in patient care, with many patients confirmed with metastatic disease on PSMA PET scans not proceeding to salvage fossa radiotherapy (8,9).
Currently, the treatment outcomes of the PSMA PET–guided change in disease management in this patient cohort are unknown. The aim of this study was to evaluate treatment outcomes from PSMA PET–informed SRT in men with rising PSA after RP.
MATERIALS AND METHODS
Between February 2015 and July 2016, PSMA PET/CT was performed in 657 consecutive patients at a single institution. Written informed consent was obtained from all patients included in the Prostate Cancer Imaging Database (ProCan-I). The Pro Can-I aims to prospectively collect clinical and imaging information on patients undergoing a PSMA PET scanning for PC and to assess the impact of the imaging results on clinical management and patient outcomes. The trial was approved by the St. Vincent’s Institutional Human Research and Ethics Committee.
Patient Population
Men who had undergone RP and were diagnosed with a rising PSA (PSA ≥ 0.05 and < 1.0 ng/mL) and suitable for SRT were selected for the present study (Fig. 1).
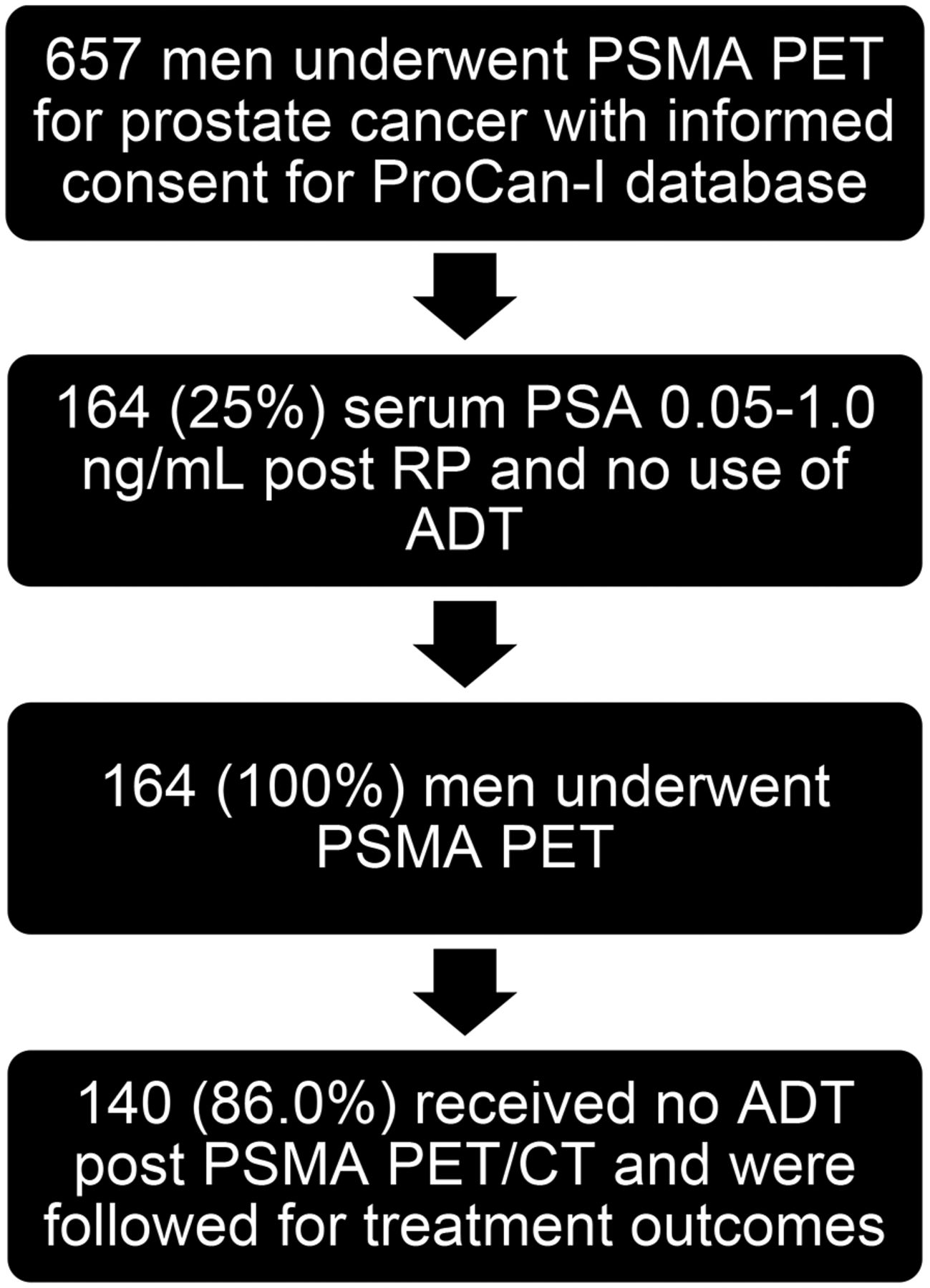
Flowchart for patient selection.
None of the patients had evidence of locoregional recurrence or metastatic disease on conventional clinical workup. Men who subsequently received any form of systemic treatment were excluded from analysis of treatment outcomes, but included in analysis on scan findings. Data to be collected at enrolment included age, previous therapy, time since RP, initial pathology (including T stage and Gleason score), surgical margin involvement, PSA at time of PSMA PET scanning, and prior imaging.
Imaging Protocol
PSMA was produced on-site compliant to the Good Laboratory Practices procedure using a TRASIS automated radiopharmacy cassette. Radiopharmacy quality control was undertaken using a high-pressure liquid chromatography method. Patients were injected with 68Ga-PSMA (2.0 MBq/kg) (H-BED CC). All PET/CT imaging was undertaken using a Phillips Ingenuity TOF–PET/64-slice CT scanner. For the PSMA PET/CT, a non–contrast-enhanced CT scan was obtained 45 min after tracer injection using the following CT parameters: slice thickness of 2 mm, with 2-mm slices, soft-tissue reconstruction kernel, 120 keV and 50 mAs, pitch of 0·828, 600 mm field of view, and a 512 matrix. Immediately after CT scanning, a whole-body PET scan was acquired for 2 min per bed position. The emission data were corrected for randoms, scatter, and decay using the Phillips Body-dynamic.xml and Body.xml reconstruction protocol. All images were viewed and reported using the Phillips Fusion Viewer.
Image Interpretation
All PET images were interpreted prospectively by credentialed nuclear medicine physicians with experience in reporting prostate PET images. Data for all PSMA scans were analyzed both visually and quantitatively. Visual analysis included a 4-point certainty scoring scale (definitely negative, equivocal probably negative, equivocal probably positive, definitely positive), as well as anatomic site and size of lesions. Semiquantitative analysis was undertaken using an automated SUVmax. For database purposes, each positive finding was coded according to anatomic site, SUVmax, number of lesions, and reporter certainty.
Follow-up and Treatment Outcomes
Management after the PSMA PET was documented for each patient, including date and type of treatment initiated (surveillance, systemic or local therapy). Any site of targeted treatment was documented. In the case of RT, treatment was divided into fossa-only RT, fossa + pelvic nodes, or stereotactic body radiation therapy external to the pelvis. The posttreatment PSA was the last PSA recorded for the patient before analysis of results. On the basis of previous literature demonstrating a post-SRT PSA of 0.10 ng/mL or less nadir as predictive of longer term outcome, treatment response was defined as both a PSA of 0.10 ng/mL or less and a greater than 50% reduction from pretreatment level (10). Follow-up time was defined as the interval (mo) between SRT and last recorded PSA.
Statistical Analysis
Pearson correlation and binary logistic regression analyses were used to identify determinants for differences between the patients with a positive scan and those with a negative scan considering pT stage, pLN stage, Gleason score, PSA level at the time of 68Ga-PSMA scanning, and time (mo) after RP. Uni- and multivariate binary logistic regression analyses were used to identify predictive determinants (PSMA PET results, serum PSA at PSMA PET, Gleason score at RP, and surgical margin status at RP) for treatment response in men who received SRT without ADT. P values of less than 0.05 were considered to indicate statistical significance. Statistical analysis was performed with IBM SPSS Statistics (version 22.0; SPSS Inc.).
RESULTS
Baseline Characteristics
Baseline characteristics are summarized in Table 1. One hundred sixty-four patients in total were included in this study. The median age at PSMA PET was 68 y (interquartile range, 62–71 y). The median time between RP and PSMA PET was 37 mo (interquartile range, 13–74 mo) and median PSA at PSMA PET 0.23 (interquartile range, 0.14–0.35).
Patient Characteristics
PSMA PET Results
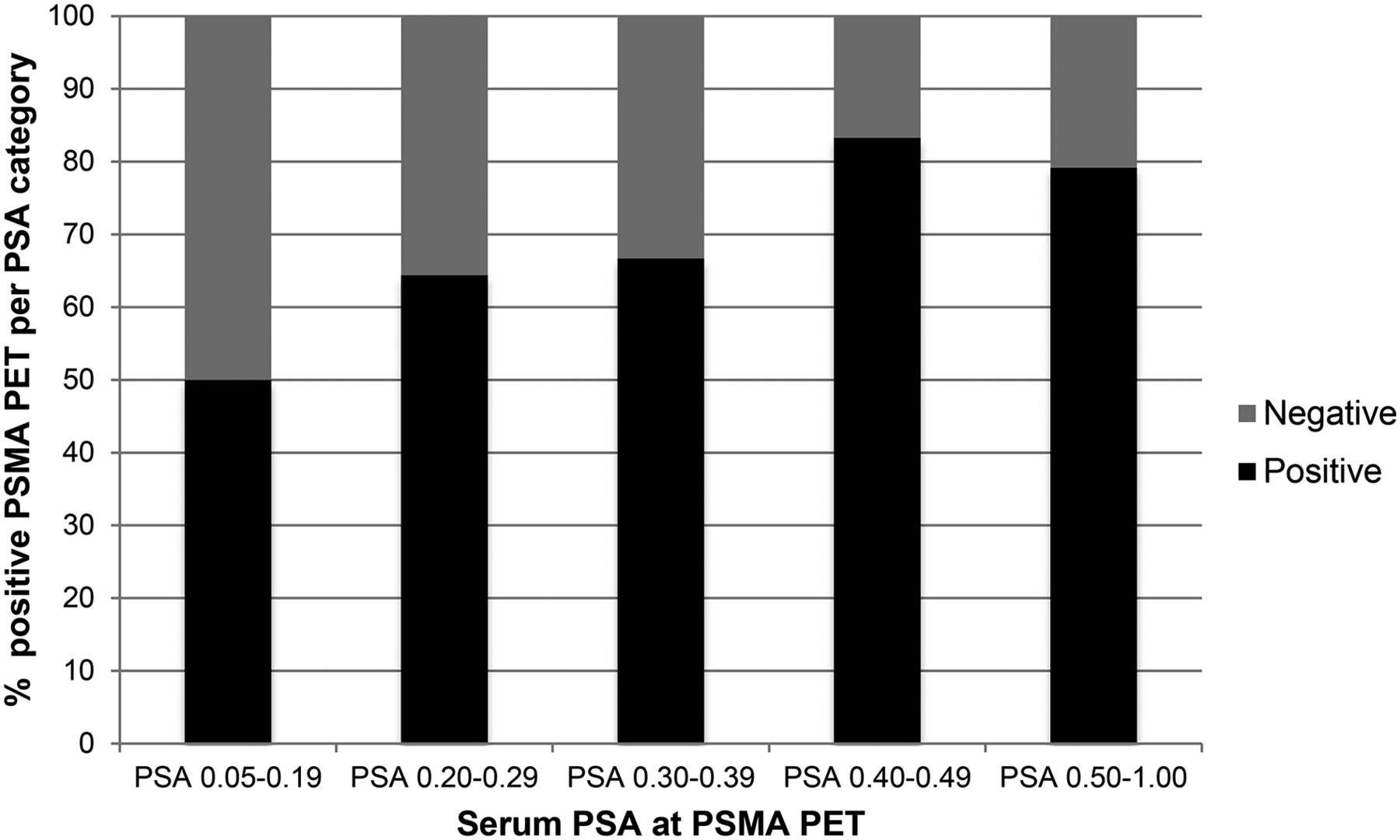
In 62% (n = 102/164) of the patients, PSMA PET/CT identified recurrent disease. The distribution of positive PSMA PET stratified by PSA levels is displayed in Figure 2. A positive PSMA PET/CT scan was reported in 50.0% (32/64) of the patients with a PSA of 0.01–0.19 ng/mL, 64.4% (29/45) with a PSA of 0.20–0.29 ng/mL, 66.7% (16/24) with a PSA of 0.30–0.39 ng/mL, 83.3% (10/12) with a PSA of 0.40–0.49 ng/mL, and 79.2% (19/24) with a PSA of 0.50–1.00 ng/mL.

PSMA PET positivity at incremental PSA levels in men with rising PSA after RP.
Of 102 men with a positive scan, 38 were positive in the prostatic fossa and 41 in pelvic nodes and 23 had distant metastasis on the PSMA PET/CT (Table 1).
PSMA PET/CT–Directed Treatments and Outcomes
A total of 24 of 164 (13.6%) patients received ADT after PSMA PET/CT and were excluded from outcome analysis. Of the 140 remaining men, 60 of 140 (43%) had negative and 80 of 140 (57%) had positive PSMA PET/CT scan findings. The median follow-up for these patients was 10.5 mo (interquartile range, 6–14 mo). Scan positivity and the sites of recurrence had an important impact on choice of subsequent management. Overall, the SRT rate was 70% (n = 99/140); this ranged from 100% (n = 36/36) for disease confined to the fossa to 87% (n = 26/30) for nodes, 71% (n = 10/14) for distant disease, and 45% (n = 27/60) for a negative PSMA PET finding.
Among the 99 patients receiving SRT, the overall treatment response rate was 72% (n = 71/99). This rose to 82.5% (52/63) in those with either a negative scan or a scan that was positive solely in the fossa, compared with a 53% (19/36) response rate in men with PSMA PET positivity for lymph nodes or distant disease (P < 0.002).
Compared with clinical predictors of response to SRT, the PSMA result was independently more predictive of a treatment response than PSA at imaging, Gleason score, pT stage, or surgical margins (Table 2). Results of the salvage treatments, stratified by PSMA PET findings and clinical parameters, are presented in the following sections and in Table 3.
Logistic Regression Analysis of Clinical Variables for Prediction of Treatment Response to SRT
Comparison of Clinical Variables Between Men with Treatment Response to SRT and Men Who Did Not Have PSA Response to SRT
Negative PSMA PET
Sixty of 140 men had a negative PSMA PET result. Of these, 45% (n = 27/60) of patients with a negative PSMA PET underwent SRT, whereas the remaining 55% (33/60) did not undergo treatment. There was no statistical difference in Gleason score, serum PSA, T stage, or surgical margins in those who underwent SRT compared with those who did not.
Of those with a negative scan who underwent SRT, 86% (n = 23/27) demonstrated a treatment response. Ten percent (3/29) had PSA failure with progressive rise in PSA despite fossa RT. In contrast, in men with a negative scan and no treatment, 65% (n = 22/34) demonstrated a further rise in PSA and 35% (12/34) a stable or declining PSA. In this cohort of men with a negative scan who underwent SRT, 20 of 27 (74%) received standard fossa RT and 7 of 27 (26%) both fossa and pelvic node field RT.
Disease Confined to Prostate Fossa
In the 36 of 99 men with disease confined to the prostate fossa on PSMA PET who underwent SRT and did not receive ADT, 81% (n = 29/36) had a significant treatment response. Nineteen percent (n = 7/36) demonstrated biochemical progression despite RT. In this cohort, 19 of 36 (53%) received standard fossa RT and 17 of 36 (47%) received fossa and pelvic node field RT.
Nodal Involvement on PSMA PET
Twenty of 99 men with nodal disease (+/− involving the prostate fossa) on PSMA PET received SRT without ADT. Of these, 61.5% (n = 16/26) had a significant treatment response after SRT. In this cohort, 38.5% (n = 10/26) demonstrated biochemical progression despite SRT. Men in this cohort all received SRT targeting PSMA, which identified nodal disease (fossa + node SRT).
Distant Disease
In the 15 men with distant metastasis on PSMA PET who did not receive ADT or systemic treatment, 10 of 15 (60%) received RT, of which 30% (n = 3/10) had a significant treatment response after RT whereas 70% (n = 7/10) demonstrated biochemical progression despite RT.
DISCUSSION
Salvage prostate fossa RT is the current standard of care in men with biochemical failure after radical prostatectomy. It remains the last chance for cure in these men, with around 56% of men achieving complete biochemical response at 5 y after RT (2,3,11). Studies have shown that low serum PSA values after RP are correlated to significantly better treatment outcomes, supporting early SRT at a serum PSA of less than 0.2 ng/mL or less than 0.5 ng/mL (3). Treatment response drops off dramatically once the PSA rises above 1.0 ng/mL (4). However, a significant number of men, even with low PSA levels, do not respond to this treatment, presumably because of disease beyond the prostatic bed at the time of salvage. In a previous study, we demonstrated that up to 29% of men in this patient cohort have disease outside the prostate fossa at the time of imaging with PSMA PET/CT (5). We know that there is a high management impact with PSMA PET/CT in this patient population (7–9,12,13). However, what has not yet been evaluated is whether a finding of disease outside the prostate fossa on PSMA PET affects treatment outcomes.
This study shows that, in the cohort of men for whom salvage fossa radiotherapy remains standard of care, PSMA PET effectively stratifies men into those with a high (82.5%) versus low response (53%) to salvage RT. High treatment responders were men with negative PSMA PET results or with disease confined to the fossa, whereas low responders had PSMA avidity in nodes or distantly. Furthermore, this difference in treatment response was evident despite the fact that the RT fields were predominately limited in the high-treatment-response cohort, and involved more extensive radiotherapy fields in the low-treatment-response group. A PSMA PET result proved to be more predictive of treatment response to SRT than established clinical predictors, such as PSA level, Gleason score, pT stage, and surgical margin status.
PSMA PET/CT is a sensitive technique for identifying sites of recurrence in the post-RP biochemical failure setting at low PSA levels (6). A significant proportion of men with a PSA of less than 1.0 ng/mL will have a positive PSMA PET scan, with the detection rate of the scan dependent on PSA at the time of imaging (5,7,14–17). Men imaged with a PSA of between 0.05 and 0.5 ng/mL can expect to have a positive scan approximately 60% of the time, rising to 80% in the PSA range of 0.5–1.0 ng/mL. By contrast, we also know that PSMA PET underestimates the extent of disease. PSMA PET does not detect small-volume nodal deposits, with sensitivity of the technique dropping off sharply at sizes below 4 mm because of the inherent physical limitations of PET imaging (16,18). The sensitivity is further reduced in the region of the prostate fossa because of adjacent excreted activity in the bladder (19,20). The results of this study confirm that the extent of local recurrence may be underestimated by PSMA PET, and that this must be taken into consideration in interpretation of scan results.
We have demonstrated that the group with the highest treatment response to salvage fossa radiotherapy is those men with a negative PSMA PET scan. This may reflect the ability of PSMA PET to differentiate between disease phenotypes. Negative scans may identify patients with less aggressive disease who will benefit from local salvage and targeted treatment. Of the more than 56% of men with a negative PSMA PET who did not proceed to SRT, with the clinician electing to watch the PSA, up to 67% progressed biochemically. There were no significant differences in risk factors found between the men treated or not treated (Gleason score, T stage, surgical margins, PSA) with the decision to treat likely influenced by the negative finding on the PET scan. This high treatment response to SRT in men with a negative scan confirms that PSMA PET is not sufficiently sensitive to exclude microscopic disease recurrence around the prostate fossa. More significantly, it demonstrates that a high proportion of men with a negative scan respond to local (potentially curative) treatment, with low-volume recurrent disease amenable to RT. This has important implications for the clinical management of men with prostate cancer and biochemical failure.
The study also confirms that a negative or fossa-confined pretreatment PSMA PET was the strongest independent determinant of treatment response after SRT, even when PSA level at the time of scan, pT stage, Gleason score, or surgical margins were included in the analysis, reinforcing the paradigm that clinicians should recommend SRT even in men with a negative PSMA PET/CT. Although median PSA was lower in the men with negative PSMA PET, there was no difference in PSA at imaging between men with disease confined to the fossa and those with positive nodes or distant disease. The question as to what PSA level is optimum for PSMA PET imaging of men with biochemical failure has not been addressed by this study and requires well-designed prospective trials.
PSMA PET is being increasingly used in men with rising PSA after RP. A positive scan may significantly alter RT intent, doses, and volume. This study describes a significantly reduced treatment response in men with nodal involvement on PET or distant disease compared with either a negative scan or disease confined to the fossa, despite the more complex RT plans in those with disease beyond the fossa on PSMA PET. This highlights 2 points. First, it demonstrates the ability of PSMA PET to stratify patients into those who will respond well to standard fossa RT, compared with those who may require more extensive treatment. Second it raises questions regarding optimum treatment for those men with PSMA PET–positive findings outside the prostate fossa, targeted or systemic. This study has insufficient patient numbers to analyze the treatment response based on variations in RT. Further, the short follow-up interval would make this type of analysis futile.
This study had an overall 75% early response rate to SRT in men with rising PSA (0.05–1.0 ng/mL) after RP. This is lower than expected from the literature for biochemical response at this median PSA level (3). There are several possible reasons for this. First, all those who were treated with concurrent ADT were excluded from analysis. Further, the PSA decline after SRT continues for more than 12 mo, and median time in this study between SRT and follow-up PSA was just 10.5 mo. Our definition of treatment response involves low PSA levels not previously measurable before the widespread use of supersensitive PSA assays. The criteria we used for defining early treatment response (PSA < 0.1 ng/mL and >50% decline in PSA) to SRT were based on recent data demonstrating that a PSA nadir after SRT less than 0.1 ng/mL has prognostic implications (10) and attempted to define men who had a significant decline in PSA (>50% reduction) due to accurate targeting of disease. Finally, more than half the men with a negative PSMA scan, which we have shown in this study as predictive of treatment response, did not in fact receive RT. This may well have reduced our overall treatment response, and raises questions regarding optimal current practice for men undergoing PSMA-informed management.
A major limitation of this study is the short follow-up after treatment. With a median of 10.5 mo in the treated cohort of patients, it is difficult to compare treatment response with larger studies of SRT (measuring biochemical failure) in this population. Although it is not possible to extrapolate long-term findings from early treatment responses, it is most likely that the nonresponders (those with PSA rise despite SRT) will not be cured, and further follow-up is not required. Although the ability of PSMA PET to stratify treatment responses and characterize men with early biochemical failure has been demonstrated in this interim study, further follow-up will be undertaken to determine whether the stratification in biochemical failure persists up to 5 y after therapy, and whether PSMA targeted treatment is appropriate.
A further limitation of the study is the relatively low numbers of patients enrolled. This limits the study’s ability to evaluate appropriate PSA levels for imaging. Larger prospective studies with longer follow-up are needed to confirm that the prognostic value of a PSMA PET adds additional value to the predictive clinical findings included in the Stephenson nomogram and other predictors of salvage RT failure.
CONCLUSION
PSMA PET is independently predictive of a treatment response to SRT and stratifies men into a high treatment response to SRT (negative or fossa-confined PSMA PET) versus men with a poor response to SRT (nodes or distant disease on PSMA PET). A negative PSMA PET predicts a high response to salvage fossa radiotherapy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 26, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 30, 2017.
- Accepted for publication July 5, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Association of Free-to-Total PSA Ratio and 18F-DCFPyL Prostate-Specific Membrane Antigen PET/CT Findings in Patients with Biochemical Recurrence After Radical Prostatectomy: A Prospective Single-Center Study
- Utility of 64Cu-Sarcophagine-Bombesin PET/CT in Men with Biochemically Recurrent Prostate Cancer and Negative or Equivocal Findings on 68Ga-PSMA-11 PET/CT
- Salvage Radiotherapy PSMA PET/CT-guided in Men With PSA Recurrence
- Changes in Management After 18F-DCFPyL PSMA PET in Patients Undergoing Postprostatectomy Radiotherapy, with Early Biochemical Response Outcomes
- Prostate-specific membrane antigen positron emission tomography compared to multiparametric MRI for prostate cancer diagnosis: a protocol for a systematic review and meta-analysis
- 3-Year Freedom from Progression After 68Ga-PSMA PET/CT-Triaged Management in Men with Biochemical Recurrence After Radical Prostatectomy: Results of a Prospective Multicenter Trial
- 18F-rhPSMA-7 PET for the Detection of Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy
- Lesion Detection and Interobserver Agreement with Advanced Image Reconstruction for 18F-DCFPyL PET/CT in Patients with Biochemically Recurrent Prostate Cancer
- Bridging the Imaging Gap: PSMA PET/CT Has a High Impact on Treatment Planning in Prostate Cancer Patients with Biochemical Recurrence--A Narrative Review of the Literature
- Prospective, Multisite, International Comparison of 18F-Fluoromethylcholine PET/CT, Multiparametric MRI, and 68Ga-HBED-CC PSMA-11 PET/CT in Men with High-Risk Features and Biochemical Failure After Radical Prostatectomy: Clinical Performance and Patient Outcomes
- Detection Efficacy of 18F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy
- 68Gallium-labelled PSMA-PET/CT as a diagnostic and clinical decision-making tool in Asian prostate cancer patients following prostatectomy
- Outcome After PSMA PET/CT-Based Salvage Radiotherapy in Patients with Biochemical Recurrence After Radical Prostatectomy: A 2-Institution Retrospective Analysis
- Seduction by Sensitivity: Reality, Illusion, or Delusion? The Challenge of Assessing Outcomes after PSMA Imaging Selection of Patients for Treatment