


Abstract
In preclinical trials, the recently developed tracer 2-methoxy-18F-DCFPyL (18F-JK-prostate-specific membrane antigen [PSMA]-7) has shown favorable properties regarding clinical performance and radiochemical accessibility. The aim of this study was to evaluate the clinical utility of 18F-JK-PSMA-7 for PET/CT imaging of patients with prostate cancer. Methods: In an Institutional Review Board–approved pilot study, the initial clinical utility of PET/CT imaging with 18F-JK-PSMA-7 was directly compared with 68Ga-PSMA-11 PET/CT in a group of 10 patients with prostate cancer. The 2 PSMA tracers were administered to each patient less than 3 wk apart. Next, we analyzed the data of 75 consecutive patients who had undergone clinical 18F-JK-PSMA-7 PET/CT imaging for tumor localization of biochemical recurrence (BCR). Results: The pilot study in 10 patients who were examined with both PSMA tracers demonstrated that 18F-JK-PSMA-7 was at least equivalent to 68Ga-PSMA-11. All unequivocally 68Ga-PSMA-11–positive lesions could be also detected using 18F-JK-PSMA-7, and in 4 patients additional suspected PSMA-positive lesions were identified (1 patient changed from PSMA-negative to PSMA-positive). In patients with BCR (after prostatectomy or radiotherapy), the capacity of 18F-JK-PSMA-7 PET/CT to detect at least one PSMA-positive lesion was 84.8%. The prostate-specific antigen (PSA)–stratified detection rate of 18F-JK-PSMA-7 after prostatectomy varied among 54.5% (6/11 patients; PSA < 0.5 μg/L), 87.5% (14/16 patients; PSA 0.5–2 μg/L), and 90.9% (20/22 patients; PSA > 2 μg/L). Conclusion: The tracer 18F-JK-PSMA-7 was found to be safe and clinically useful. We demonstrated that 18F-JK-PSMA-7 was not inferior when directly compared with 68Ga-PSMA-11 in a pilot study but indeed identified additional PSMA-avid suspected lesions in oligometastasized patients with BCR. In a subsequent analysis of a clinical cohort of BCR patients, 18F-JK-PSMA-7 was useful in tumor localization. 18F-JK-PSMA-7 is recommended for future prospective trials.
When a patient experiences a new increase in prostate-specific antigen (PSA) levels after surgery or radiation therapy for prostate cancer, commonly referred to as biochemical recurrence (BCR), sensitive imaging modalities are needed to decide on metastasis-directed therapy options (1,2). Over the past few years, radiolabeled PSMA–specific PET tracers have been increasingly used to localize prostate cancer (3–9). The rationale behind these tracers is the fact that tumor cells display an approximately 8- to 12-fold increased expression of folate hydrolase 1, better known as prostate-specific membrane antigen (PSMA), on their surface, compared with noncancerous prostate tissue (10,11). An additional advantage of PSMA-specific PET tracers is that they are not negatively affected by therapies targeting the signaling of the androgen receptor in castration-resistant prostate cancer (12).
Most PET tracers currently established for cancer detection are labeled with 18F because of its ideal decay properties regarding half-life, availability from a cyclotron, and high image resolution due to its low β+-emission energy (13,14). However, regarding PSMA ligands, 68Ga-labeled compounds were the first widely used in clinical studies (15). Advantages are that no access to a cyclotron is required and that 68Ga-labeled tracers can easily be obtained without complex radiosynthetic chemistry, since the 68Ga label can be introduced by simple complex formation with an appropriate chelator (16). In 2011, Chen et al. reported on synthesis of the 18F-labeled PSMA-specific tracer 2-(3-{1-carboxy-5-[(6-18F-fluoro-pyridine-3-carbonyl)-amino]-pentyl}-ureido)-pentanedioic acid (18F-DCFPyL) using a multistep protocol that involved radiofluorination of a prosthetic group (17). Clinical studies revealed that 18F-DCFPyL displayed at least noninferior sensitivity in detecting relapsed tumors in prostate cancer patients, compared with 68Ga-PSMA-11 (6,7,18,19). In some patients, these tracers even exhibited increased sensitivity, possibly due to the increased resolution of the 18F label for small anatomic structures such as small iliac lymph nodes.
When 18F-labeled PSMA ligands were introduced into the clinical setting, their synthesis was far more difficult than that of their 68Ga-labeled counterparts in routine clinical practice (17,20). Indeed, if the synthesis reaction of 18F-DCFPyL is not performed under optimal conditions, an unstable isomer is formed, which leads to rapid defluorination of the 18F-labeled PSMA-specific product (21,22).
Recently, our group introduced the PSMA-specific derivative 2-methoxy-18F-DCFPyL (18F-JK-PSMA-7), a new compound for PET imaging. This compound had been selected from a group of several candidates because of its favorable imaging properties (23). The abbreviation JK (J for Jülich and K for Köln [Cologne]) refers to the Forschungszentrum Jülich and the University Hospital of Cologne, which were involved in the development of this tracer. In addition, we recently reported on a minimalist approach that enables us to implement a robust and high-yielding process for synthesizing 18F-JK-PSMA-7, with minor variations in release specifications ideally suited for high-throughput production in a clinical setting (23).
Here, we present the first application of 18F-JK-PSMA-7 in a pilot study, demonstrating its noninferiority to the benchmark tracer 68Ga-PSMA-11. Furthermore, we report the results of the first routine clinical application of this tracer in a cohort of 75 prostate cancer patients with BCR.
MATERIALS AND METHODS
Study Design and Patient Selection Criteria
In brief, our study followed a 2-step approach. In the first step, we offered an additional 18F-JK-PSMA-7 PET/CT scan to 10 patients who had undergone 68Ga-PSMA-11 imaging. Nine of these 10 patients had recently experienced BCR of their disease, and 1 patient with known oligometastatic status showed a raised PSA level. The 68Ga-PSMA-11 scans were interpreted as negative or inconclusive in 5 patients; only a solitary PSMA lesion had been detected in the other 5 patients. To improve the certainty of the assumed tumor localization or to exclude any additional PSMA-positive metastases, we performed a second PET/CT scan with 18F-JK-PSMA-7 within 3 wk of the 68Ga-PSMA-11 scan. The rationale was our previous experience indicating a potentially superior detection rate for 18F-labeled PSMA-specific PET tracers (7,18). We did not observe any adverse side effects in any of those 10 patients during the entire examination procedure (up to 3 h after injection of 18F-JK-PSMA-7). Furthermore, in telephone counseling on therapeutic options some weeks later, none of the patients reported any new side effects.
In the second step, we used the novel 18F-JK-PSMA-7 tracer to examine a cohort of 75 prostate cancer patients with BCR who were referred to our institute for PET/CT imaging between March 2017 and December 2017. Of these patients, 49 presented with BCR after surgery, 47 of whom had a PSA level of at least 0.2 μg/L after nadir. The other 26 patients of the 75-patient cohort presented with BCR after radiotherapy (external-beam radiation therapy, brachytherapy, seed implantation). Seventeen of these patients had a PSA level of at least 2 μg/L after nadir. The other 9 patients had a PSA increase of less than 2 μg/L and did not fulfill the Phoenix criterion for BCR but nevertheless were referred for restaging because of continuously rising PSA values with no sign of intraprostatic inflammation.
The institutional review board approved this retrospective study, and all subjects gave written informed consent. All procedures were performed in compliance with the regulations of the responsible local authorities (District Administration of Cologne, Germany).
Imaging
Patients fasted for approximately 4 h before undergoing PET/CT to allow administration of contrast agent when neither CT scans nor MRI scans had been performed previously and to exclude any interference with the novel 18F-JK-PSMA-7. Data on 18F-DCFPyL had previously shown that fasting did not influence PSMA accumulation in metastases (24), but we had no data on the influence of fasting on 18F-JK-PSMA-7 uptake. In our pilot study, a mean dose of 141 ± 30 MBq of 68Ga-PSMA-11 and a mean dose of 358 ± 15 MBq of 18F-JK-PSMA-7 were injected. Following previously published protocols, 68Ga-PSMA-11 PET scans were acquired 1 h after injection (3–5). In patients with a PSA level below 2.0 μg/L, a second scan of the pelvis and lower abdomen was performed 3 h after injection, to guarantee maximal sensitivity for the 68Ga-PSMA-11 tracer (25–28). In parallel with previous studies using 18F-DCFPyL (6,7), 18F-JK-PSMA-7 PET scans were acquired 2 h after tracer injection. In the pilot study, we additionally generated a series of PET data between 10 and 230 min after injection in 9 of our 10 patients, to define the scans with the best visualization of the PSMA-positive tissue (29). All images were acquired on a Biograph mCT 128 Flow PET/CT scanner (Siemens Healthineers). The same filters and acquisition times (15 min from top of skull to mid thigh) were used for 68Ga-PSMA-11 1 h after the injection and for 18F-JK-PSMA-7. The second 68Ga-PSMA-11 PET scan had a FlowMotion (Siemens) bed speed of 0.7 mm/s instead of 1.5 mm/s to compensate for the decay of 68Ga-PSMA-11. Non–contrast-enhanced (low-dose) CT scans were conducted in parallel with PET imaging. Images were reconstructed using an ultrahigh-definition algorithm (13).
All PET scans were analyzed by a team of at least 2 specialists in nuclear medicine and 1 radiologist. A scan was scored as positive if focal tracer accumulation was detected in the prostate fossa, in a lymph node, or at a distant site. A focus of tracer accumulation was interpreted as a suspected lymph node if it showed a morphologic correlate on the corresponding CT scan consistent with a regional lymph node, even when the diameter was less than 8 mm. The PET/CT reading was performed according to the published criteria for harmonization of the PSMA PET/CT interpretation (30,31).
Tracer Preparation
All tracers were synthesized in accordance with applicable good manufacturing practices using a 2-step protocol. Additionally, extensive quality control measures, including radiochemical purity, endotoxin testing, pH, and determination of residual solvents such as acetonitrile, acetone, tertiary butanol, and tetraethylammonium hydrogen carbonate, were performed.
In brief, 18F-JK-PSMA-7 was prepared using a 2-step reaction. In the first step, the radiolabeled active ester was produced by the nucleophile reaction of 18F with 2-methoxy-N,N,N-trimethyl-5-((2,3,5,6-tetrafluoro-phenoxy) carbonyl) pyridine-2-aminium-trifluoromethanesulfonate to generate the ester 2,3,5,6-tetrafluorophenyl-6-(18F-fluoro)-4-methoxy-nicotinate (18F-FPy-OMe-TFP). In the second step, 4.6 ± 0.1 mg of (((S)-5-amino-1-carboxypentyl)-carbamoyl)-l-glutamic-acid was added to 18F-FPy-OMe-TFP and subsequently incubated at 45°C for 6 min. Then, the final product, 18F-JK-PSMA-7, was purified by solid-phase extraction (Oasis HLB; Waters) and formulated in saline. This reaction provided 18F-JK-PSMA-7 in a high radiochemical yield of up to 40% and a high radiochemical purity (>95%). The specific concentration of F-PSMA-7 was no more than 10 μg/mL. The upper limit of the injected volume was 10 mL; the activity of 18F-JK-PSMA-7 was at least 30 MBq/mL. Each week, we produced 2 batches of 18F-JK-PSMA-7. The detailed procedure for the radiosynthesis using the minimalist light protocol is described elsewhere (23). The activity produced and the radiochemical purity were analyzed for the 74 consecutive batches of 18F-JK-PSMA-7 synthesized within the first year of clinical application.
Synthesis of 68Ga-PSMA-11 was performed as described previously (32,33).
RESULTS
Robustness and Reliability of 18F-JK-PSMA-7 Production
We analyzed the quality of 74 consecutive synthesis batches of 18F-JK-PSMA-7 over the course of 12 mo. We found a high radiochemical activity per synthesis (mean activity, 6,660 MBq ± 2,869 MBq; interquartile range, 2,712 MBq) and a high radiochemical purity (mean purity, 98.6% ± 1.6%; interquartile range, 2.4%). In the course of this study, only 2 of 74 syntheses (2.7%) failed to reach a radiochemical purity of more than 95%.
Direct Comparison Between the Biodistribution Patterns of 18F-JK-PSMA-7 and 68Ga-PSMA-11
We next assessed the validity of 18F-JK-PSMA-7. For this purpose, we offered 10 patients who had just undergone PET/CT imaging with 68Ga-PSMA-11 an additional PET/CT scan with 18F-JK-PSMA-7. We performed the second PET/CT scan within less than 3 wk and found that all unequivocally 68Ga-PSMA-11–positive lesions could be validated using 18F-JK-PSMA-7. Moreover, 4 patients displayed at least 1 suspected PSMA-positive lesion on the 18F-JK-PSMA-7 scan that had been missed by 68Ga-PSMA-11 (Figs. 1–4). Intriguingly, in 3 of these 4 patients, the additional PSMA-positive lesions were located in locoregional lymph nodes (iliac lymph nodes: patients 2 and 4; retroperitoneal lymph nodes: patient 7). In 1 patient (patient 1), a PSMA-positive bone lesion that was revealed by 18F-JK-PSMA-7 had been known from the 18F-DCFPyL PET/CT scan 2 y before.
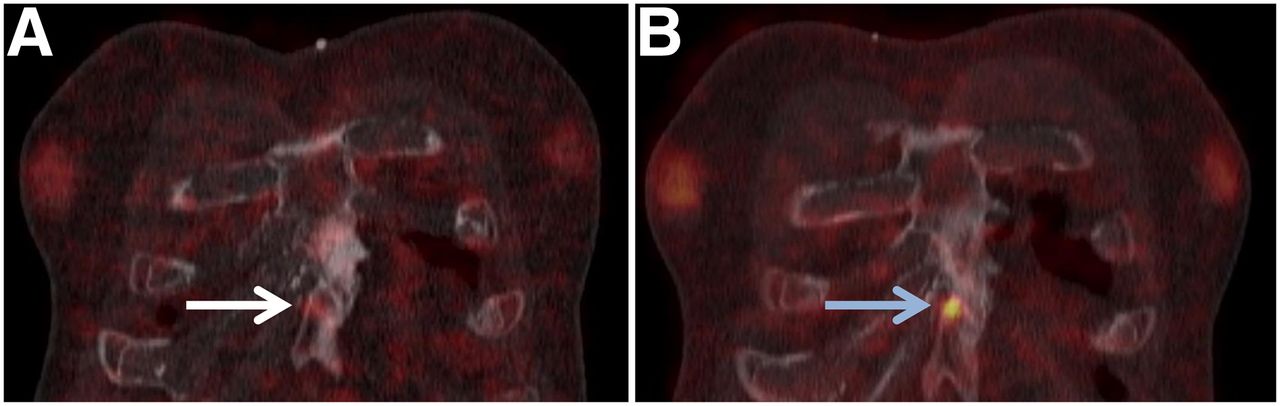
68Ga-PSMA-11 PET/CT (A) and 18F-JK-PSMA-7 PET/CT (B) of patient 1. Besides concordant PSMA-positive tissue within irradiated prostate (not shown), patient had previously proven bone metastases, appearing positive in sternum on 18F-JK-PSMA-7 scan (arrow) but only faintly positive on 68Ga-PSMA-11 scan (arrow).
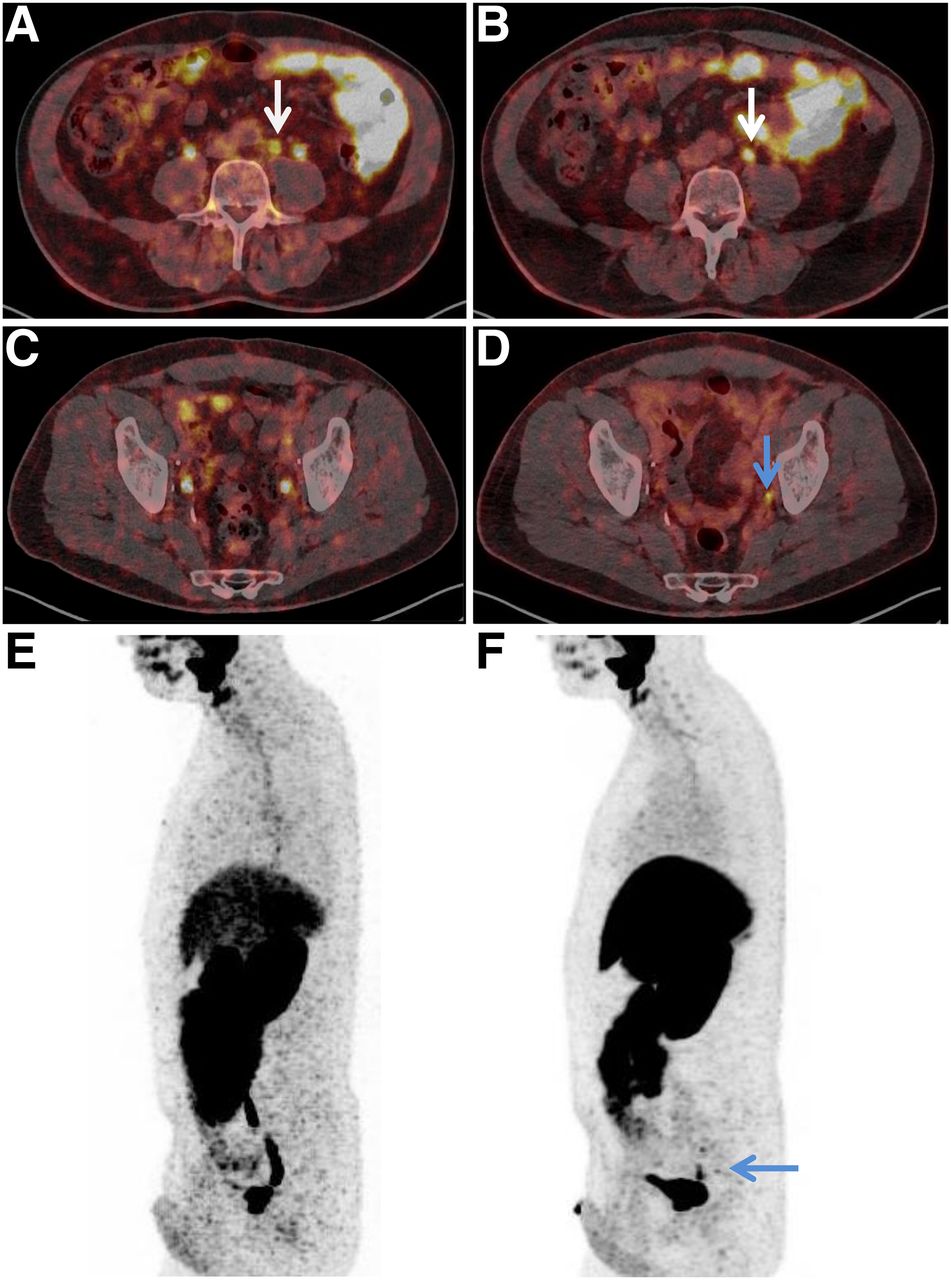
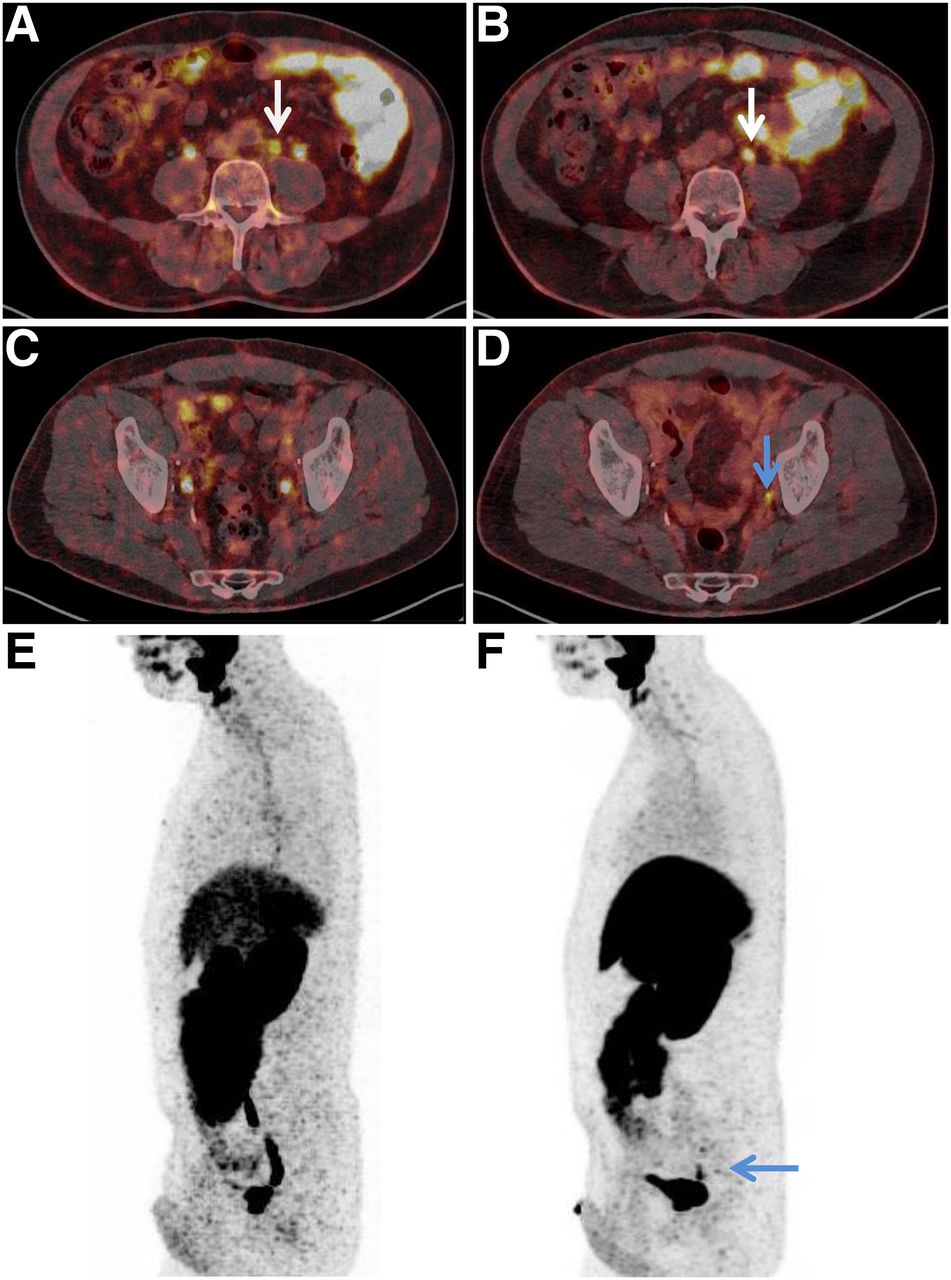
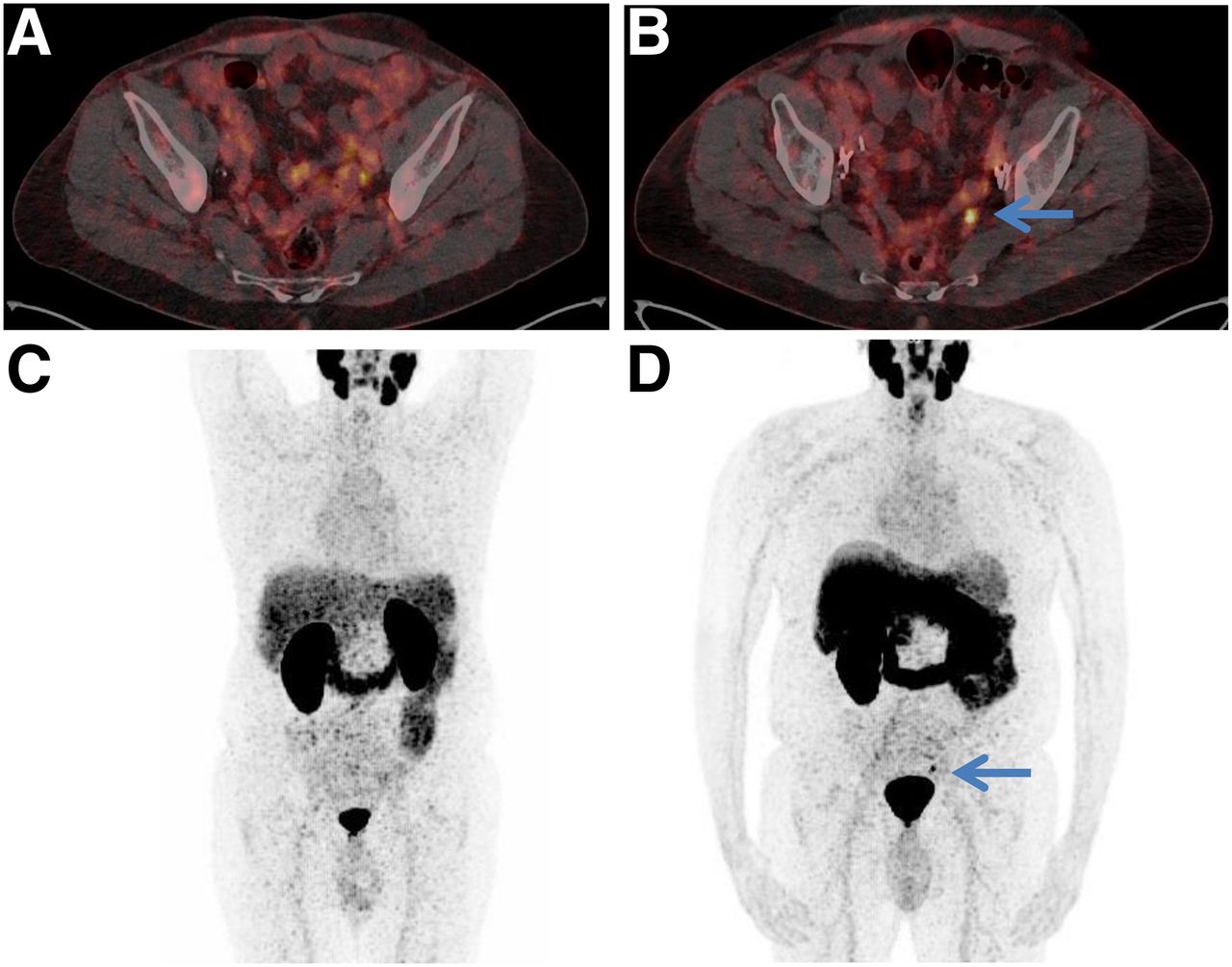
68Ga-PSMA-11 PET/CT (A, C, and E) and 18F-JK-PSMA-7 PET/CT (B, D, and F) of patient 2. Besides concordant PSMA-positive lymph node on left near bifurcation (arrows on A and B), 18F-JK-PSMA-7 in this patient revealed small PSMA-positive left iliac caudal lymph node dorsal to ureter (arrows on D and F).
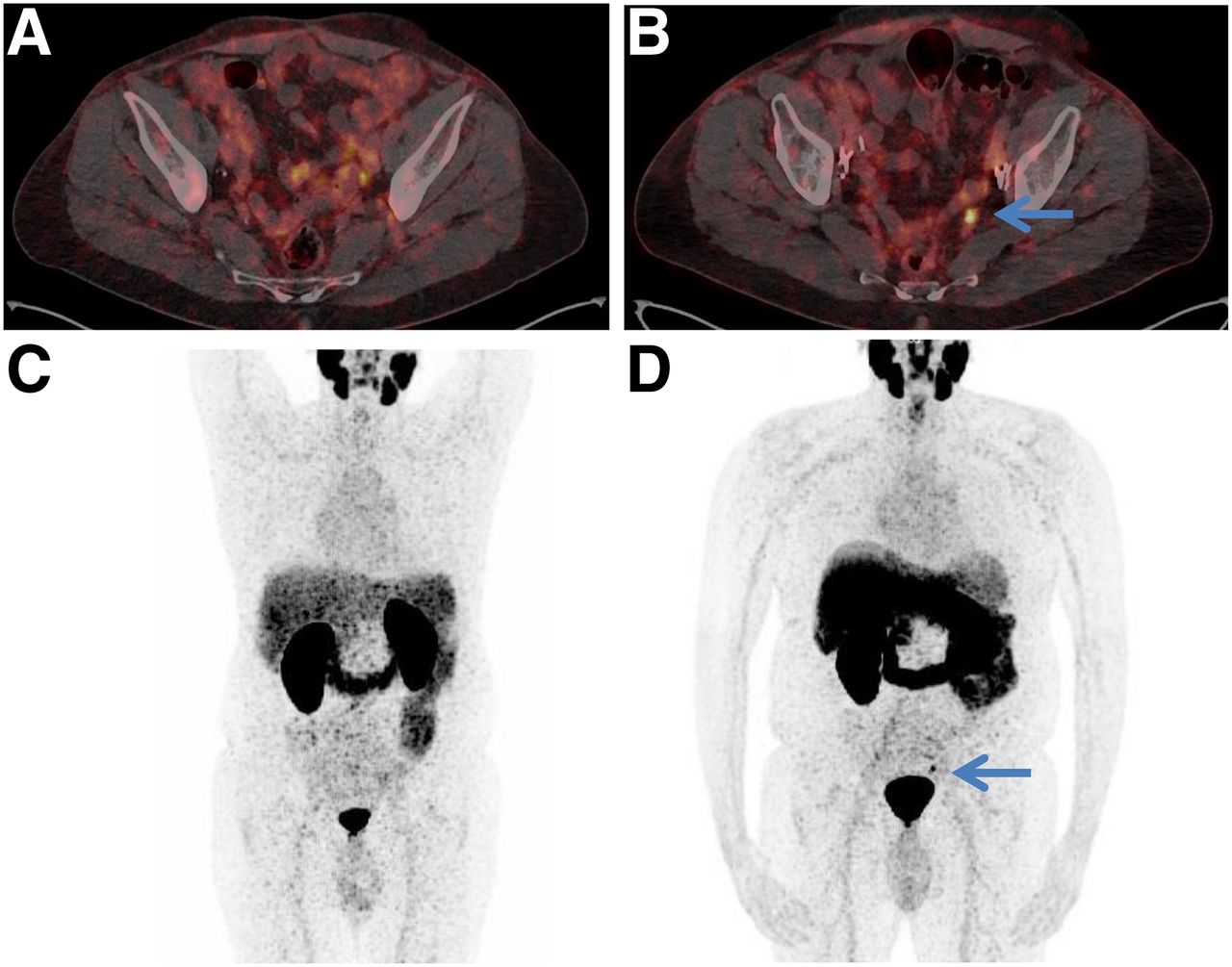
68Ga-PSMA-11 PET/CT (A and C) and 18F-JK-PSMA-7 PET/CT (B and D) of patient 4. PSMA-positive left iliac lymph node was visible on 18F-JK-PSMA-7 PET/CT (arrows).

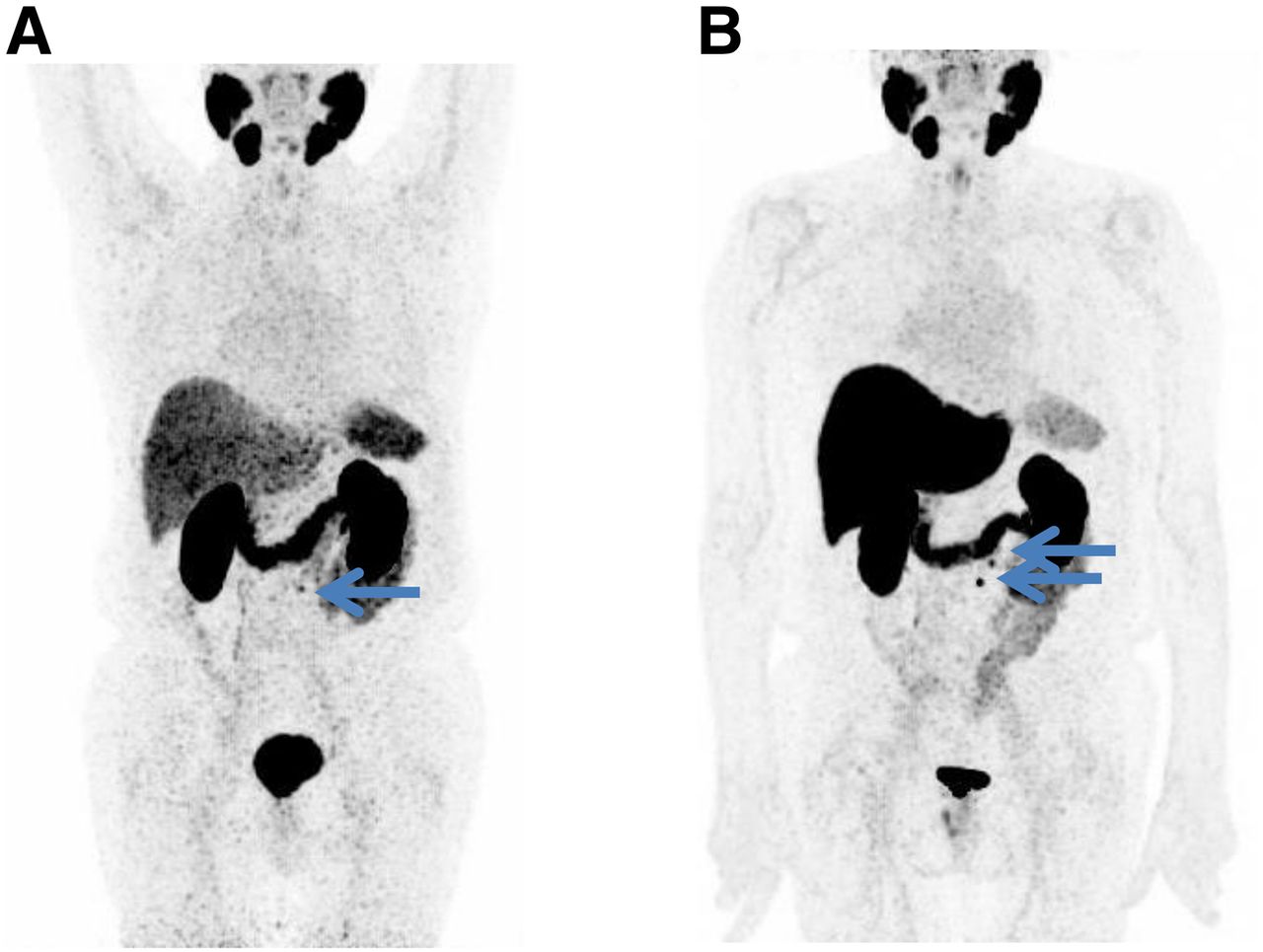
68Ga-PSMA-11 PET/CT (A) and 18F-JK-PSMA-7 PET/CT (B) maximum-intensity projections of patient 7. 68Ga-PSMA-11 PET/CT revealed only 1 PSMA-positive retroperitoneal paraaortic lymph node (arrow on A), whereas 18F-JK-PSMA-7 PET/CT showed 2 PSMA-positive retroperitoneal lymph nodes (arrows on B).
The follow-up data of the 10 patients are summarized in Tables 1 and 2. First, we report the details of the 4 patients with the different PET findings. In 1 of these patients (patient 4), the first PET/CT scan with 68Ga-PSMA-11 was interpreted as completely negative. The PSMA-positive left iliac lymph node that was detected by 18F-JK-PSMA-7 was a plausible explanation for the BCR in patient 4, with a PSA level of 1.1 ng/mL, and was finally confirmed by tumor growth seen on an externally performed 68Ga-PSMA-11 PET/CT examination 8 mo later. The salvage lymphadenectomy initially undertaken could not verify the PET finding. The PSMA-positive lymph nodes found additionally by the 18F-JK-PSMA-7 scan in 2 other patients (patients 2 and 7) were localized in the same lymph node area as that in which the 68Ga-PSMA-11 PET/CT had already depicted 1 PSMA-positive lymph node. Both patients received radiotherapy of the PSMA-positive lymph node area, and the PSA level dropped after the irradiation.
Patient Characteristics and Localization of Pathologic PSMA Uptake Detected by 68Ga-PSMA-11 PET/CT and 18F-JK-PSMA-7 PET/CT in Initial Cohort of 10 Patients (Patients 1–5)
Patient Characteristics and Localization of Pathologic PSMA Uptake Detected by 68Ga-PSMA-11 PET/CT and 18F-JK-PSMA-7 PET/CT in Initial Cohort of 10 Patients (Patients 7–11)
Second, we observed concordant findings using both PSMA tracers in 6 patients: concordantly positive in 2 patients (patients 5 and 11) and concordantly negative in 4 patients (patients 3, 7, 9, and 10). Both PSMA-positive patients showed PSMA-positive tissue within the prostate fossa and received salvage radiotherapy. One of the 4 PSMA-negative patients was subjected to salvage radiotherapy of the prostate fossa.
Benchmarking the Detection Rate of 18F-JK-PSMA-7 Across 75 Prostate Cancer Patients with BCR
Closing the pilot study, we examined 162 prostate cancer patients with 18F-JK-PSMA-7 (349 ± 53 MBq) within a year of the clinical application of 18F-JK-PSMA-7. Focusing on the localization of BCR as the main indication for PET/CT, we studied the detection rate of 18F-JK-PSMA-7 (347 ± 56 MBq) in 75 patients, aged 69.2 ± 8.1 y, with increasing PSA levels after initial curative treatment, for whom it was unclear whether they carried PSMA-positive lesions (Table 3). These patients did not receive androgen deprivation therapy. We analyzed the detection rate separately for patients after prostatectomy with or without salvage radiotherapy versus patients after radiotherapy alone.
Results of 18F-JK-PSMA-7 PET/CT in 75 Patients with BCR, Specified by Initial Therapy and PSA Level
Overall, 49 patients in our cohort had recently experienced BCR after prostatectomy with or without salvage radiotherapy. In 40 of these prostatectomy patients, we detected 18F-JK-PSMA-7–positive lesions, resulting in a detection rate of 81.6%. The PSA-stratified detection rate for 18F-JK-PSMA-7 varied among 54.5% (6/11 patients; PSA < 0.5 μg/L), 87.5% (14/16 patients; PSA 0.5–2 μg/L), and 90.9% (20/22 patients; PSA > 2 μg/L).
Our cohort contained a further group of 26 patients who presented with a PSA increase after radiotherapy. The detection rate for the 18F-JK-PSMA-7 tracer was 94.1% (16/17) in patients with BCR according to the Phoenix criterion (PSA level ≥ 2.0 μg/L above nadir). Some patients were referred for PSMA PET/CT when the PSA increase was repeatedly confirmed but remained below 2.0 μg/L and the Phoenix criterion defining the BCR had not yet been reached. In this constellation, the 18F-JK-PSMA-7 PET scan detected PSMA-positive tissue in 33.3% of patients (3/9).
Tumor relapse patterns substantially differed between BCR patients after surgery and BCR patients after radiotherapy. Although 19 of the 49 prostatectomy patients (38.8%) displayed PSMA positivity exclusively in lymph nodes, this pattern was rarely observed in the patients with a PSA increase after radiotherapy (3/26, 11.5%). Several of the radiotherapy patients, however, displayed PSMA-positive tissue exclusively within the prostate (8/26, 30.8%).
Verification
After the introduction of 18F-JK-PSMA-7 into our clinical care procedures, collection of data on verification became part of our quality assurance program. After an interval of 6–18 mo, we read all the written reports, which were sent to our institute. Additionally, we checked all our electronic patient files.
The PSMA-positive lesions in the 59 patients who underwent PET/CT for BCR were confirmed by histology in 6 patients, by follow-up in 17 patients, and by morphologic imaging in 20 patients. Further information was missing for 16 patients. The histologic verification resulted from salvage lymphadenectomies with PSMA-positive lymph node metastases. Verification by follow-up was based on a decrease in PSA level after radiotherapy (n = 9), progression of the PSMA-positive lesion after watchful waiting (n = 7), or regression of the PSMA-positive lesion after starting ADT (n = 1). One of these patients with progressive PSMA-positive nodal disease on a second PET exam had shown positive 18F-JK-PSMA-7 PET/CT findings but then negative histologic results (0/14 lymph nodes) after salvage lymphadenectomy. We therefore did not interpret this 18F-JK-PSMA-7 PET/CT finding as false-positive. The verification by morphologic imaging summarized patients in whom CT demonstrated an osteosclerotic or osteolytic lesion (n = 11), a suspected lymph node at least 8 mm in diameter within the pelvis (n = 7), or a suspected pulmonary lesion (n = 1) and patients in whom MRI had revealed a suggestive lesion within the prostate (n = 1).
DISCUSSION
Over the past 4 y, we have successfully introduced 18F-DCFPyL and later 18F-JK-PSMA-7 into our routine PET/CT imaging procedure for prostate cancer patients (7,18,34). We described the synthesis of 18F-JK-PSMA-7 and found that it could be produced with a consistently high radiochemical yield and purity (23). This robust synthesis substantially reduced the need to reschedule appointments at short notice in our institute. Furthermore, recent preclinical data have highlighted favorable properties of 18F-JK-PSMA-7 in comparison with other 18F-labeled PSMA tracers, such as high edge-contrast, resolution, and signal-to-noise ratio (23).
Here, we present the first clinical study with 18F-JK-PSMA-7 across 10 + 75 patients. As a first step, we showed that distribution patterns of 18F-JK-PSMA-7 and 68Ga-PSMA-11 are highly concordant in patients consecutively examined with the 2 tracers. Interestingly, 18F-JK-PSMA-7 increased the detection rate for suspected lesions in small anatomic structures, such as iliac and retroperitoneal lymph nodes. These lesions might have remained masked by the limited resolution of the 68Ga-emitting tracers, but the detection of such lesions with 18F-JK-PSMA-7 had a substantial impact on subsequent therapy in some of these patients. This finding corroborates our earlier observations on 18F-DCFPyL (7,18). In contrast to our previous studies, however, we were able to observe this improved sensitivity pattern of 18F-JK-PSMA-7 although the acquisition protocol for 68Ga-PSMA-11 had been amended by a second PET scan 3 h after injection for patients with PSA levels below 2.0 μg/L (25–28). This finding suggests that the ability of 18F-PSMA–specific ligands to visualize small anatomic structures reflects an intrinsic quality of the 18F label and does not result from differences in image acquisition protocols. It remains an intrinsic advantage of the 18F-labeled PSMA ligands that batches with high 18F activity were produced and that, on each application, the 18F activity injected was higher than the corresponding amount of 68Ga activity.
As a second step, we measured and compared the detection rate of 18F-JK-PSMA-7 in 75 patients with BCR and confirmed that its sensitivity and metastatic pattern also depended largely on the PSA level and type of previous therapy (surgery vs. radiotherapy). The PSA-stratified detection rates that we found for 18F-JK-PSMA-7 in this study were highly concordant with results reported for 68Ga-PSMA-11 by independent institutes with high expertise in this field (4). These observations suggest that the potential sensitivity of the new 18F-JK-PSMA-7 tracer is at least not inferior to previous PSMA tracers. Further, when combining the detection rate of 18F-JK-PSMA-7 across all BCR patients and excluding the patient subgroup with a PSA increase below the Phoenix criterion, we obtained a pooled localization rate of 84.8% (56/66 patients). At the same institute and with the same PET scanner, but in another cohort with the same patient characteristics, we had observed a pooled localization rate of 79.1% (102/129 patients) for 68Ga-PSMA-11 and 74.2% (46/62 patients) for 18F-DCFPyL 2 y ago (18). Indeed, as shown by Mannweiler et al. in immunohistochemical analyses (35), lack of PSMA expression intrinsically limits the sensitivity of PSMA tracers to about 84%, so that 18F-JK-PSMA-7 exploits the full sensitivity potential of PSMA tracers.
Dosimetric data on 18F-JK-PSMA-7 were based on animal studies (23) and then on a cohort of 10 patients (29). 18F-JK-PSMA-7 showed fast excretion via the blood and the kidneys in humans, similar to that seen with 18F-DCFPyL. The blood protein binding of 18F-JK-PSMA-7 was significantly lower than that of 18F-PSMA-1007 and 68Ga-PSMA-11 in animal studies (23). The PSMA-positive metastases in patients showed an increase in SUVmax and SUVpeak up to 3 h after the injection of 18F-JK-PSMA-7 (29).
Our head-to-head comparison between 68Ga-PSMA-11 and 18F-JK-PSMA-7 had some limitations. It was not designed as a prospective trial. The 18F-JK-PSMA-7 PET scans were clinically indicated by an equivocal or negative interpretation of the first PET scan with 68Ga-PSMA-11 or by an oligometastatic status before radiotherapy. It might be possible that the diagnostic accuracy of 68Ga-PSMA-11 PET/CT was underestimated in the initial cohort of 10 patients. Our working group did not set out to conduct the first-in-humans observational study based on animal studies (23) with testing of 18F-JK-PSMA-7 on healthy volunteers. It is a general advantage of all 18F-labeled PSMA ligands that the injected activities are usually higher than the injected activities of the 68Ga-labeled PSMA ligands. In our pilot study, we injected an activity of approximately 2 MBq of 68Ga-PSMA-11 per kilogram of body weight, which complies with the recommended range for 68Ga-PSMA (1.8–2.2 MBq/kg) in the international guidelines (36), but higher activities of 68Ga-PSMA-11 will have a positive impact on lesion detectability (37).
CONCLUSION
We have shown that 18F-JK-PSMA-7 is safe and that its sensitivity in prostate cancer patients is not inferior to that of 68Ga-PSMA-11. Further, in parallel with previous studies with 18F-DCFPyL, we observed even improved sensitivity for 18F-JK-PSMA-7, a modified version of 18F-DCFPyL, compared with 68Ga-PSMA-11 in a few selected patients with PSMA-positive lesions in small lymph nodes. Additionally, the simplicity, high radiochemical yield, and robustness of 18F-JK-PSMA-7 production propose use of this PSMA-specific agent for routine clinical diagnostics.
DISCLOSURE
Bernd Neumaier, Philipp Krapf, Boris Zlatopolskiy, and Alexander Drzezga have applied for a patent on 18F-JK-PSMA-7. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTIONS: Is 18F-JK-PSMA-7, a modified version of 18F-DCFPyL, helpful for PET/CT imaging of patients with prostate cancer?
PERTINENT FINDINGS: 18F-JK-PSMA-7 was directly compared with 68Ga-PSMA-11 PET/CT in a pilot study including 10 patients, and additional suspected PSMA-positive lesions were identified in 4 patients. During the first year of application, 18F-JK-PSMA-7 PET/CT detected at least 1 PSMA-positive lesion in 84.8% of the patients with BCR.
IMPLICATIONS FOR PATIENT CARE: We observed an improved detection rate for 18F-JK-PSMA-7 compared with 68Ga-PSMA-11 in a few selected patients with PSMA-positive lesions in small lymph nodes.
Footnotes
↵* Contributed equally to this work.
Published online Jul. 19, 2019.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 8, 2019.
- Accepted for publication July 6, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}