


Abstract
We evaluated 18F-fluciclovine uptake parameters that correlate with true positivity for local recurrence in non–prostatectomy-treated patients. Methods: Twenty-one patients (prostate-specific antigen level, 7.4 ± 6.8 ng/mL) with biochemical recurrence after nonprostatectomy local therapy (radiotherapy and cryotherapy) underwent dual–time-point 18F-fluciclovine (364.1 ± 37.7 MBq) PET/CT from pelvis to diaphragm. Prostatic uptake over background was delineated and coregistered to a prostate-biopsy–planning ultrasound. Transrectal biopsies of 18F-fluciclovine–defined targets were completed using a 3-dimensional visualization and navigation platform. Histologic analyses of lesions were completed. Lesion characteristics including SUVmax, target-to-background ratio (TBR), uptake pattern, and subjective reader’s suspicion level were compared between true-positive (malignant) and false-positive (benign) lesions. Univariate analysis was used to determine the association between PET and histologic findings. Receiver-operating-characteristic curves were plotted to determine discriminatory cutoffs for TBR. Statistical significance was set at a P value of less than 0.05. Results: Fifty lesions were identified in 21 patients on PET. Seventeen of 50 (34.0%) targeted lesions in 10 of 21 patients were positive for malignancy. True-positive lesions had a significantly higher SUVmax (6.62 ± 1.70 vs. 4.92 ± 1.27), marrow TBR (2.57 ± 0.81 vs. 1.69 ± 0.51), and blood-pool TBR (4.10 ± 1.17 vs. 2.99 ± 1.01) than false-positive lesions at the early time point (P < 0.01) and remained significant at the delayed time point, except for blood-pool TBR. Focal uptake (odds ratio, 12.07; 95% confidence interval, 2.98–48.80; P < 0.01) and subjective highest suspicion level (odds ratio, 10.91; 95% confidence interval, 1.19–99.69; P = 0.03) correlated with true positivity. Using the receiver-operating-characteristic curve, optimal cutoffs for marrow TBR were 1.9 (area under the curve, 0.82) and 1.8 (area under the curve, 0.85) at early and delayed imaging, respectively. With these cutoffs, 15 of 17 malignant lesions were identified at both time points; however, fewer false-positive lesions were detected at the delayed time point (5/33) than at the early time point (11/33). Conclusion: True positivity of 18F-fluciclovine–targeted prostate biopsy in non–prostatectomy-treated patients correlates with focal uptake, TBR (blood pool and marrow), and subjective highest suspicion level. A marrow TBR of 1.9 at the early time point and 1.8 at the delayed time point had optimal discriminating capabilities. Despite the relatively low intraprostate positive predictive value (34.0%) with 18F-fluciclovine, application of these parameters to interpretative criteria may improve true positivity in the treated prostate.
Biochemical recurrence (BCR) occurs in approximately 20%–60% of patients after treatment for localized prostate cancer (1–3). BCR is frequently detectable before clinical evidence of recurrent disease is seen. Diagnosis of recurrent prostate cancer after localized therapy is challenging because of significant changes in the prostate anatomy and the presence of artifacts from previous definitive treatment (4,5). Transrectal ultrasound (TRUS)–guided biopsy, the standard method for recurrent cancer detection in the prostate or prostate bed, has several limitations, including a low detection rate and low accuracy (6–8). Hence, TRUS-guided biopsy may miss clinically relevant disease, making treatment planning difficult.
Imaging has achieved a prominent role in the diagnosis of recurrent prostate cancer. MRI is of great value in the detection of primary prostate cancer yet has suboptimal diagnostic performance for recurrent prostate cancer detection (9–11), partly because of tissue changes from previous treatment (4,5). Molecular imaging using radiotracers such as 18F- and 11C-choline (12–14), 68Ga-prostate-specific membrane antigen (15,16), and 18F-fluciclovine (17–23) has also been applied for the detection and localization of recurrent prostate cancer. Multimodal imaging has recently been explored to improve detection of prostate cancer recurrence. The combination of PET with CT or MRI has shown improved efficacy in the detection of recurrent prostatic cancer (22,24).
18F-fluciclovine, a synthetic l-leucine analog, is approved by the U.S. Food and Drug Administration for imaging of suspected prostate cancer recurrence based on elevated blood prostate-specific antigen levels after prior treatment (23). PET using 18F-fluciclovine for detecting recurrent prostate cancer has yielded favorable results (17–20,22,25). Though with lower specificity in the unresected treated prostate, 18F-fluciclovine PET can provide localizing information to direct targeted biopsy. We have reported a significant increase in the detection rate of recurrence in the prostate with 18F-fluciclovine PET/CT–guided biopsy compared with standard TRUS (26). Despite the improved detection rate of fused 18F-fluciclovine PET/TRUS–targeted biopsy, the false positivity of 18F-fluciclovine in the treated prostate has remained high.
Our aim in this analysis was to explore 18F-fluciclovine uptake parameters that correlate with true positivity for local recurrence in patients with BCR after nonsurgical prostate cancer treatment. Understanding the uptake parameters that are characteristic of true prostate cancer recurrence in this group of patients may help develop optimized interpretative criteria for 18F-fluciclovine uptake and better guide targeted biopsy in the treated prostate.
MATERIALS AND METHODS
Patient Selection
This prospective clinical trial between November 2015 and April 2017 was approved by the institutional review board and complied with the Health Insurance Portability and Accountability Act. Inclusion criteria were BCR based on American Society for Radiation Oncology–Radiation Therapy Oncology Group Phoenix criteria (elevated prostate-specific antigen > nadir + 2.0 ng/mL) or the older American Society for Radiation Oncology criteria (3 consecutive rises of prostate-specific antigen or earlier if clinically appropriate; >1 y since cryotherapy, external-beam radiation, or high-intensity focused ultrasound or >2 y since brachytherapy; and >1 mo since prior prostate biopsy). All patients who met the inclusion criteria gave written informed consent.
PET/CT Imaging Protocol
18F-fluciclovine was prepared as previously reported, under Investigational New Drug Application 72,437 (27). Patients ingested oral contrast medium after at least 4 h of fasting. An initial CT scan (slice thickness, 3.75 mm; spacing, 3.25 mm) was completed for attenuation correction (∼100 mAs); afterward, 364.1 ± 37.7 MBq (9.84 ± 1.02 mCi) of intravenous 18F-fluciclovine were administered. At 5 min after injection, the patient underwent dual–time-point PET scanning from pelvis to diaphragm at 2.5 min/bed position at 4 table positions. Scanning was completed on a Discovery MV690 PET/CT scanner (GE Healthcare). Images were reconstructed with iterative technique (VUE Point Fx [GE Healthcare]; 3 iterations, 24 subsets, 6.4-mm filter cutoff) and transferred to an MIMVista workstation (MIM Software) for interpretation.
PET/CT Image Interpretation
Images were interpreted by a board-certified nuclear medicine physician (25 y of experience) per previously reported dual–time-point criteria (19). The nuclear medicine physician was masked to the patient’s clinical history and other imaging results to avoid interpretation bias. The SUVmax and SUVmean of the background (blood pool [aorta], prostate, and marrow [L3]) were recorded. On a workstation, the physician identified regions of focal 18F-fluciclovine activity in the prostate that were at least greater than the SUVmean of the marrow background on both early and delayed sequences. In addition to visual analysis, the subjective reader’s suspicion level was used to characterize the lesions, with a suspicion level of 1 being defined as definitively negative, 2 as probably negative, 3 as indeterminate, 4 as probably positive, and 5 as definitively positive. Prostate lesions with a suspicion level of at least 3 were exported to the biopsy planning system and targeted for biopsy.
Lesion uptake pattern, defined as focal (well defined) or nonfocal (amorphous); central or peripheral (prostate zone); and left or right apex, mid, or base (prostate region) were noted. The seminal vesicles were considered part of the prostate base. Target-to-background ratios (TBRs) (SUVmax of target/SUVmean of reference background) and retention fraction ([delayed SUVmax/early SUVmax] × 100) were calculated.
Fused PET/TRUS-Targeted Biopsy
PET/CT images with delineated lesions were coregistered to a previously obtained planning TRUS on a workstation with modified software as previously described (28,29). Transrectal biopsy of 18F-fluciclovine–defined targets was completed with the guidance of a 3-dimensional visualization and navigation platform (Artemis; Eigen). Standard TRUS-guided biopsy was performed on each patient before PET-targeted biopsy in the same session (28,29), and the detection rates were compared (26).
Fifty lesions (average, 2.38 per patient) with 125 cores (average, 2.5 per target) were sampled on targeted biopsy. All biopsied lesions were verified histologically. Gleason scores (grade groups) were reported in all cores that had no therapy-related changes.
Statistical Analysis
Descriptive statistical analysis was performed. Characteristics were compared between true-positive lesions and false-positive lesions using paired t testing and χ2 testing as appropriate. Univariate analysis was used to determine the association between PET and histologic findings. Receiver-operating-characteristic curves were plotted to determine the TBR cutoffs that best discriminated between benign and malignant lesions. The level of statistical significance was set at a P value of less than 0.05. Analysis was performed using Statistical Analysis Software (version 9.4; IBM).
RESULTS
Patient Characteristics
Twenty-one patients (mean age, 69.6 ± 7.4 y) with a mean prostate-specific antigen level of 7.4 ± 6.8 ng/mL met the inclusion criteria. The average interval between 18F-fluciclovine PET/CT and biopsy was 50.1 ± 22.4 d. Recurrent prostate cancer was detected in 10 of the 21 (47.6%) patients on targeted biopsy and 6 (28.6%) on TRUS-guided biopsy. Five patients had malignancy detected on both TRUS-guided and targeted biopsies, whereas 1 patient had malignancy detected on TRUS-guided biopsy only. For initial prostate cancer therapy, 3 of the 21 (14.3%) patients had cryotherapy alone, 2 (9.5%) brachytherapy alone, 1 (4.8%) intensity-modulation radiation therapy alone, 1 (4.8%) proton-beam therapy alone, 1 (4.8%) external-beam radiation therapy alone, and 13 (61.9%) mixed therapy (external-beam radiation/intensity-modulation radiation and/or brachytherapy and/or cryotherapy and/or hormonal therapy).
Lesion Characteristics
Of the 50 lesions targeted for biopsy, 17 (34.0%) were positive for recurrent prostate cancer (true-positives). Gleason scores and grade groups were reported for 12 of the 17 lesions. Median Gleason score and grade group were 7 (range, 6–9) and 3 (range, 1–5), respectively. In 5 of 17 lesions, Gleason scores and grade groups were not assigned because of significant therapy-related histologic changes. Of the 33 false-positive lesions, 16 (48.5%) had evidence of prostatitis or radiation changes and 17 (51.5%) were benign prostate tissue.
Compared with false-positive (benign) lesions, true-positive (malignant) lesions had a significantly higher SUVmax (respectively: 6.62 ± 1.70 vs. 4.92 ± 1.27; odds ratio [OR], 2.15; 95% confidence interval [CI], 1.33–3.50; P < 0.01, and 5.19 ± 1.22 vs. 4.10 ± 1.33; OR, 2.01; 95% CI, 1.12–3.62, P = 0.02) and marrow TBR (respectively: 2.57 ± 0.81 vs. 1.69 ± 0.51; OR, 8.58; 95% CI, 2.33–31.57; P < 0.01, and 2.16 ± 0.51 vs. 1.57 ± 0.56; OR, 7.13; 95% CI, 1.82–27.95; P < 0.01) at the early and delayed time points, respectively. Blood-pool TBR was significantly higher in true-positive than false-positive lesions at the early time point (4.10 ± 1.17 vs. 2.99 ± 1.01; OR, 2.40; 95% CI, 1.34–4.32; P < 0.01), but there was no significant difference at the delayed time point (3.56 ± 0.69 vs. 3.21 ± 1.42; OR, 1.26; 95% CI, 0.77–2.05; P = 0.36). There was no statistical difference in normal-prostate TBR between true-positive and false-positive lesions at the early and delayed time points (Table 1).
Differences in Mean Lesion Uptake and TBR
Focal uptake (OR, 12.07; 95% CI, 2.98–48.80; P < 0.01) and highest suspicion level (OR, 10.91; 95% CI, 1.19–99.69; P = 0.03) correlated with true positivity (Table 2). Prostate zone, region, and initial therapy did not significantly correlate with true positivity. Of the lesions biopsied, 17 had both focal uptake and highest suspicion level. Of these, 11 of 17 (64.7%) were confirmed to be malignant on histology.
Association Between Lesion Characteristics and Cancer Recurrence Detected by Targeted Biopsy
Receiver-Operating-Characteristic Curve Cutoffs
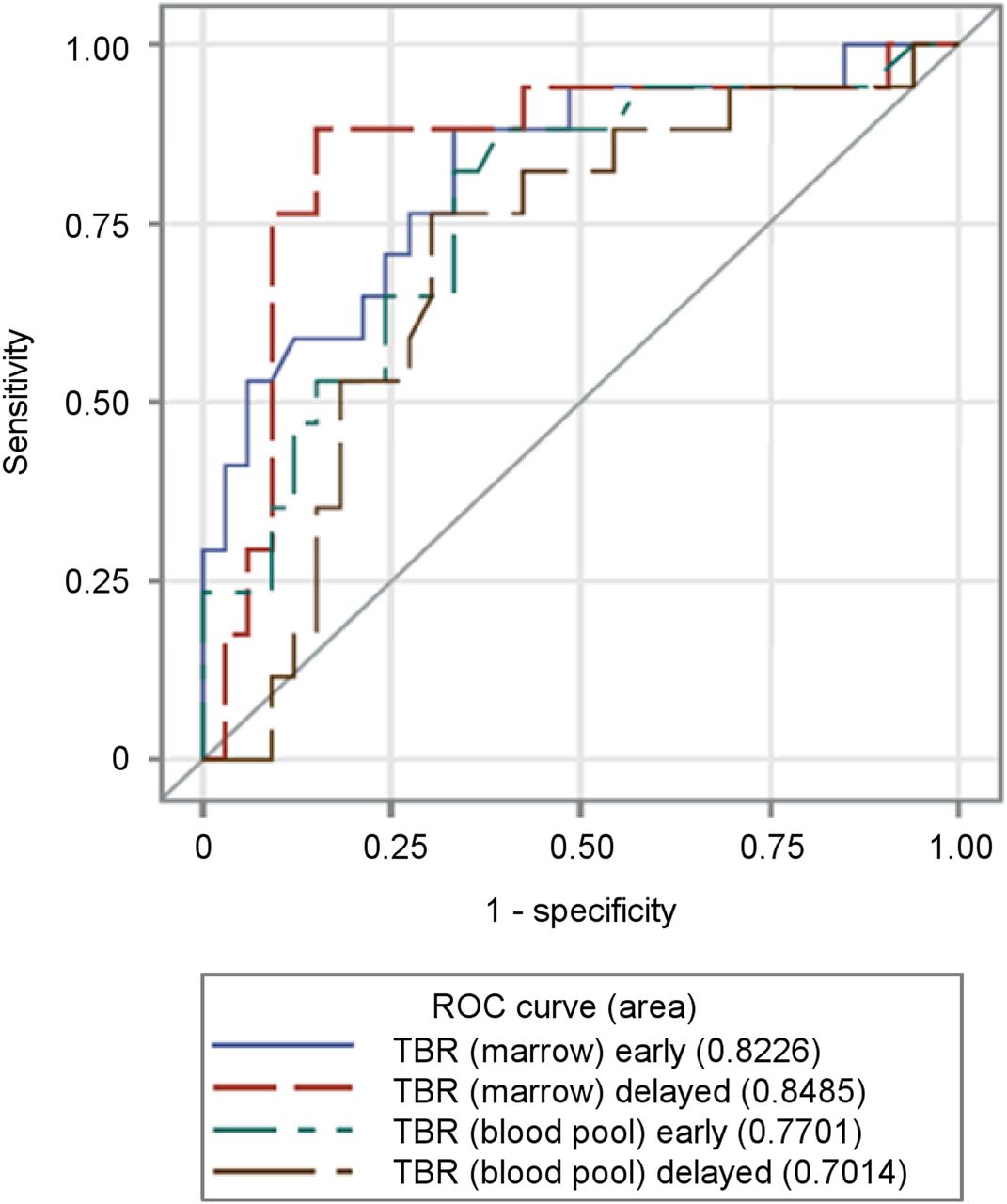
The receiver-operating-characteristic curves for uptake parameters were analyzed to explore optimal diagnostic performance (Fig. 1). At a cutoff of 1.9 for marrow TBR at the early time point, 15 of 17 malignancies would have been detected at the expense of 11 of 33 false-positives (area under the curve [AUC], 0.82) with a sensitivity of 88.2% and a specificity of 66.7%. Intriguingly, marrow TBR was more discriminating at the delayed time point than at the early time point. Using an optimal cutoff of 1.8 for marrow TBR at the delayed time point, 15 of 17 malignancies would have been detected at the expense of 5 of 33 false-positives (AUC, 0.85) with a sensitivity of 88.2% and a specificity of 84.8%. Blood-pool TBR, using an optimal cutoff of 3.0, was less discriminating at the early (AUC, 0.77) and delayed (AUC, 0.70) time points (Table 3). Figures 2 and 3 are examples of true-positive and false-positive lesions, respectively.
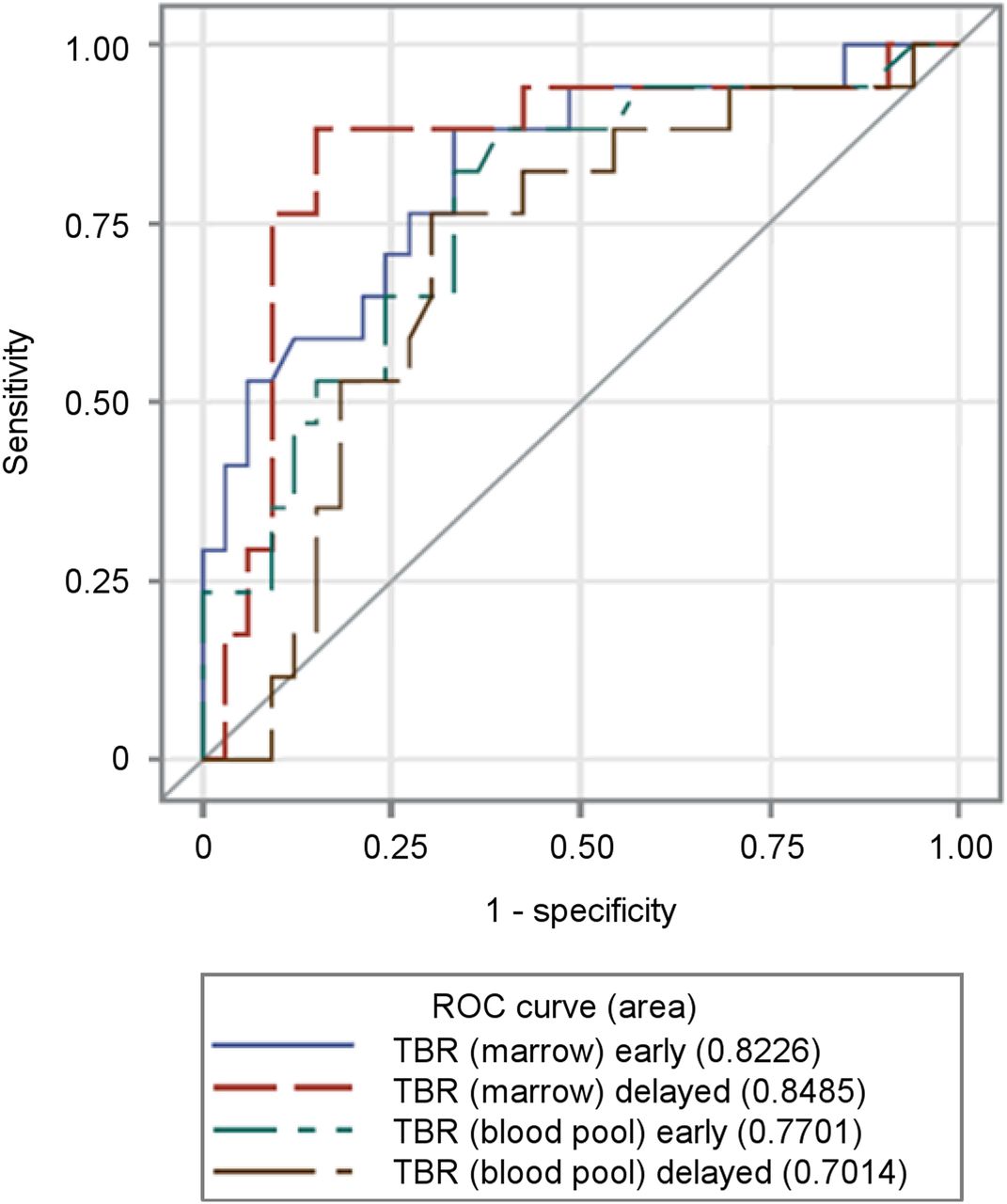
Receiver-operating-characteristic (ROC) curves for TBR marrow and blood pool at early and delayed time points. Better discrimination of true positivity is noted with marrow TBR at delayed time point.
Cutoffs for 18F-Fluciclovine Uptake Parameters

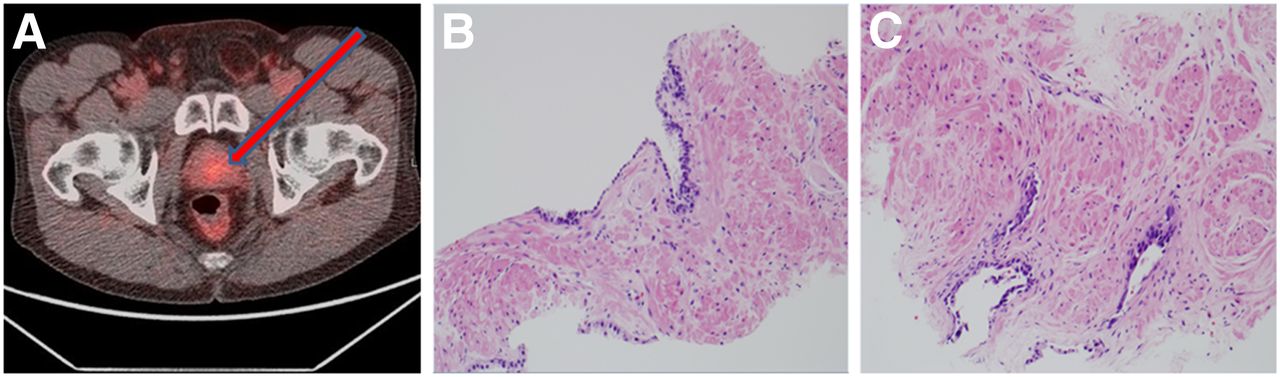
A 68-y-old patient (prostate-specific antigen level, 3.9 ng/mL) with BCR 4 y after intensity-modulated radiation therapy. (A) Left mid lesion (arrow) with focal uptake and highest suspicion level was detected on 18F-fluciclovine PET/CT. (B) Histologic examination revealed prostatic adenocarcinoma (true-positive) with radiation therapy effect (×20). Gleason score (grade group) was not assigned to lesion because of therapy-related changes.
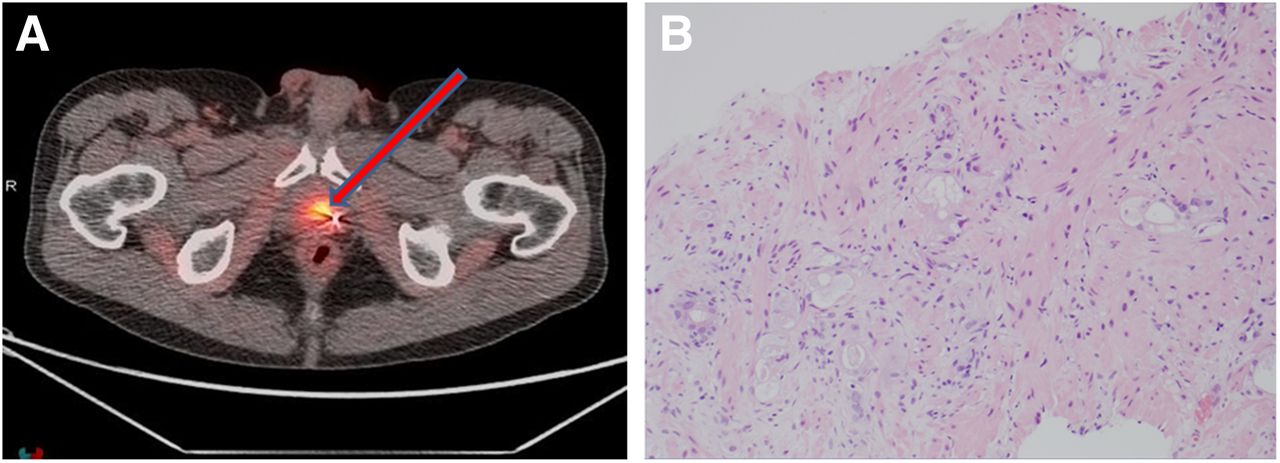
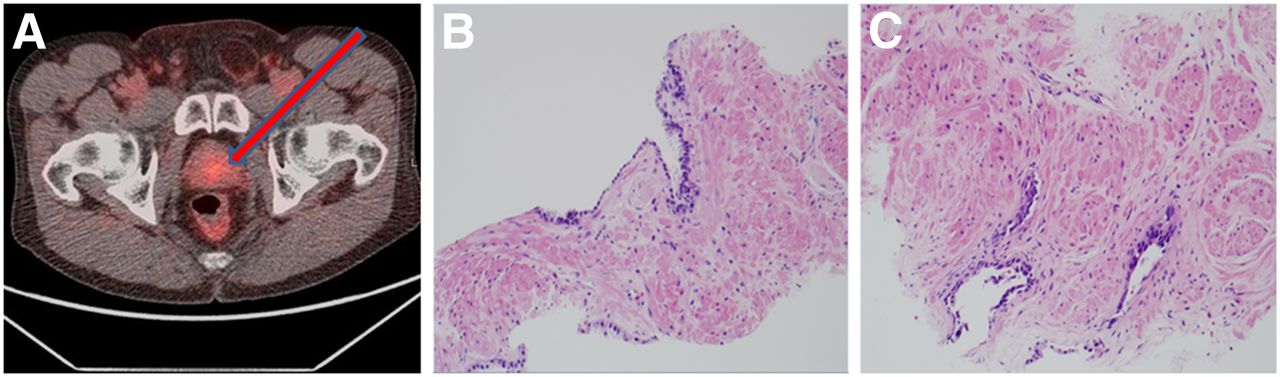
A 61-y-old patient (prostate-specific antigen level, 7.3 ng/mL) with BCR 6 y after external-beam radiation. (A) Left mid lesion (arrow) with nonfocal uptake and equivocal suspicion level was detected on 18F-fluciclovine PET/CT. (B and C) Histologic examination revealed benign prostatic glands (false-positive) with radiation therapy effect (×20).
DISCUSSION
We previously reported that 18F-fluciclovine PET–guided biopsy increased the detection rate of recurrent prostate cancer over standard TRUS in patients with non–prostatectomy-definitive treatment (26). We set out to determine the 18F-fluciclovine uptake parameters of the lesions that were associated with true positivity. We found recurrent prostate cancer in 17 of 50 (34%) lesions detected in 21 patients on 18F-fluciclovine PET–targeted biopsy. Focal uptake and subjective highest suspicion level correlated with true positivity. We found significantly higher 18F-fluciclovine uptake (SUVmax and marrow TBR) in true-positive lesions than in false-positive lesions. In addition, we found that the yields from targeted biopsy were optimal at set marrow TBR cutoffs of 1.9 and 1.8 at the early and delayed time points, respectively. The use of these cutoffs would result in a sensitivity of 88.2% and specificity of 66.7% using an early time point (5 min) and a sensitivity of 88.2% and specificity of 84.8% using a delayed time point (15 min).
The high false positivity in the treated prostate in this study is consistent with our prior reports (19,22). Although 18F-fluciclovine PET is approved for detection of prostate cancer recurrence (30), factors such as benign prostatic hyperplasia and inflammation have been associated with reduced specificity in both treated and untreated prostate (17,18,20,31,32). Among the lesions in our study with false-positive results, about half had evidence of prostatitis or radiation changes.
Few studies using fusion imaging–guided biopsy have reported lesion-based prostate cancer detection rates in a recurrence setting. A previous retrospective study evaluating the ability of multiparametric MRI/TRUS-guided biopsy to detect local recurrence of prostate cancer in 10 patients after prostatectomy reported a detection rate of 62.5% (10/16 lesions) (33). The reported detection rate in that study is superior to the positive predictive value, 34.0%, reported in our study. This difference may be related to the absence of confounding artifacts in the previous group of patients, who had primary surgical treatment. However, in our cohort of patients with previous local therapy, the presence of therapy-related artifacts may be responsible for the lower positive predictive value we found.
Our findings that lesions in recurrent prostate cancer had a significantly higher mean SUVmax and marrow TBR, and were more likely to have focal 18F-fluciclovine uptake, creates a framework to explore modified diagnostic interpretation criteria that may help maximize the detection rate of recurrent prostate cancer. This concept is similar to the study by Piert et al., who reported focal 11C-choline uptake within the prostate in patients with primary prostate cancer, compared with amorphous uptake in false-positive lesions (14). The same study reported a significantly higher mean SUVmax and TBR in true-positive lesions, although this analysis was done on patients with primary prostate cancer.
The importance of characterization and determination of optimal cutoffs for clinical interpretation in the setting of BCR has been highlighted in previous studies. Piert et al., in a different study, reported a higher cancer detection rate with 18F-choline at an optimal cutoff (AUC, 0.92) in the setting of PET/CT fused with MRI for guided biopsy for localizing prostate cancer (34). At the optimal threshold, 3 additional lesions otherwise missed were identified, and they were confirmed to be malignant on histology. This result is consistent with our finding better sensitivity and specificity for 18F-fluciclovine PET with optimal TBR thresholds.
Proper characterization of lesions seen on 18F-fluciclovine PET in the setting of BCR, and enhancement of interpretative criteria, are essential not only for diagnostic purposes but for guiding decisions on therapy. For example, when we used a marrow TBR of more than 1, which is clinically recommended, all cancers were identified at the expense of 31 of 33 false-positives (specificity, 6.1%). If we had used an optimal marrow TBR of 1.9 at the early time point, slightly fewer cancers would have been identified (15/17), yet with considerably fewer false-positives (11/33)—a common tradeoff of sensitivity for higher specificity. When compared with delayed imaging, a cutoff of 1.8 for marrow TBR yielded even fewer false-positives (5/33), with the same sensitivity. This increase in specificity at the delayed time point highlights the potential value of delayed imaging in identification of true malignant lesions with 18F-fluciclovine. Elschot et al. used 18F-fluciclovine PET/MRI in the setting of primary prostate cancer and found that delayed imaging improved the distinction between prostate cancer and benign lesions (31).
One limitation of our study is the relatively small sample size. However, its prospective nature and the availability of histologic proof make these findings relevant to current practice in this cohort of patients. Results would have to be confirmed in a larger series before firm recommendations can be made to alter interpretative criteria. Other limitations include the heterogeneity of initial focal therapy in our study population, the unavailability of a reference gold standard such as salvage prostatectomy, and the inability to determine specificity because targeted biopsy was performed only on 18F-fluciclovine–positive regions (no true-negatives). To address these limitations, each patient underwent standard 12-core template biopsy (masked to 18F-fluciclovine PET findings) immediately before the targeted biopsy, and detection rates for both biopsy techniques were compared and have been reported separately (26). Also, we acknowledge the possibility of sampling error during the biopsies due to the imperfect nature of prostate contouring using CT and the lesions from the PET data. We expect that the next generation of our technology will have automated thresholding and contouring and that the addition of PET/MR capabilities will further advance the field.
CONCLUSION
True positivity of 18F-fluciclovine–targeted prostate biopsy in non–prostatectomy-treated patients correlates with focal uptake, TBR (blood pool and marrow), and subjective highest suspicion level. The diagnostic performance of 18F-fluciclovine PET for recurrent cancer in the treated prostate of patients with nonprostatectomy local treatment can be optimized using marrow TBR thresholds of 1.9 and 1.8 at the early and delayed time points, respectively. Though we have reported a relatively low intraprostatic positive predictive value (34.0%) for recurrent prostate cancer using 18F-fluciclovine PET, application of these parameters to interpretative criteria may improve detection of lesions that are true-positive for malignancy. Larger prospective studies to evaluate the interpretation parameters of 18F-fluciclovine PET among patients with BCR are encouraged. The technology for PET/TRUS-guided biopsy that we used in our study may also be used for other radiotracers.
DISCLOSURE
This study was funded by National Institutes of Health grants R21CA176684, R01CA156775, and R01CA204254. Blue Earth Diagnostics Ltd. provided fluciclovine synthesis cassettes to Emory University, which is eligible for royalties derived from the sale of products related to the research described in this article. The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict-of-interest policies. Mark Goodman is entitled to royalties derived from the sale of products related to the research described in this article. The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict of interest policies. Olayinka Abiodun-Ojo, Akinyemi Akintayo, Oladunni Akin-Akintayo, Funmilayo Tade, and David Schuster are or have been receiving funding from Blue Earth Diagnostics Ltd. and Nihon Medi-Physics Co., Ltd., through the Emory University Office of Sponsored Projects for other clinical trials using fluciclovine. David Schuster participates, through the Emory Office of Sponsored Projects, in sponsored grants including those funded or partially funded by Telix Pharmaceuticals (US) Inc. and Advanced Accelerator Applications and is a consultant for Syncona and AIM Specialty Health. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can defining 18F-fluciclovine uptake parameters associated with true positivity improve the detection rate of PET/TRUS-targeted biopsy for recurrent prostate cancer in non–prostatectomy-treated patients?
PERTINENT FINDINGS: In this prospective clinical trial evaluating 18F-fluciclovine uptake parameters that correlate with true positivity on 18F-fluciclovine PET/TRUS-targeted biopsy in non–prostatectomy-treated patients, TBRs (marrow and blood pool), focal uptake, and subjective highest suspicion level correlated with true positivity of prostate cancer recurrence.
IMPLICATIONS FOR PATIENT CARE: Understanding the uptake parameters that are characteristic of true prostate cancer recurrence in this group of patients may be helpful to better guide targeted biopsy of the treated prostate.
Acknowledgments
We acknowledge Fielder Bridget, RN, Fenton G. Ingram, RT(R), CNMT, PET, Seraphinah Lawal, RT(R), CNMT, PET, Ronald J. Crowe, RPh, BCNP, and the cyclotron/synthesis team from the Emory University Center for Systems Imaging. This study is registered at ClinicalTrials.gov (https://clinicaltrials.gov/ct2/show/NCT02744534).
Footnotes
Published online Apr. 6, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 5, 2019.
- Accepted for publication March 29, 2019.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.