


Abstract
Prostate-specific membrane antigen (PSMA)–ligand PET imaging provides unprecedented accuracy for whole-body staging of prostate cancer. As PSMA-ligand PET/CT is increasingly adopted in clinical trials and routine practice worldwide, a unified language for image reporting is urgently needed. We propose a molecular imaging TNM system (miTNM, version 1.0) as a standardized reporting framework for PSMA-ligand PET/CT or PET/MRI. miTNM is designed to organize findings in comprehensible categories to promote the exchange of information among physicians and institutions. Additionally, flowcharts integrating findings of PSMA-ligand PET and morphologic imaging have been designed to guide image interpretation. Specific applications, such as assessment of prognosis or impact on management, should be evaluated in future trials. miTNM is a living framework that evolves with clinical experience and scientific data.
See an invited perspective on this article on page 466.
Prostate-specific membrane antigen (PSMA)–ligand PET/CT or PET/MRI provides high sensitivity and specificity for prostate cancer staging (1). The accuracy of PSMA-ligand hybrid imaging is superior to that of conventional imaging and tracers such as choline across a range of indications and disease extents (2–15). Level 2b evidence for superior detection rates at early biochemical recurrence after radical prostatectomy led to a grade A recommendation for PSMA-ligand PET/CT by the European Association of Urology (16). We anticipate increased adoption of PSMA-ligand PET/CT fueled by upcoming evidence and inclusion into guidelines. Thus, reporting standards must be created now to aid reproducibility, enhance communication, and ultimately support acceptance of this technology to the benefit of prostate cancer patients.
The Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE) criteria reported in this issue of The Journal of Nuclear Medicine summarize standards for study design and reporting of prostate cancer molecular imaging. We acknowledge that performance characteristics from different studies can be compared only if target regions are properly described and uniformly used. Therefore, PROMISE recommends that definition of anatomic regions be guided by reproducibility, general applicability, and clinical relevance. Uniform frameworks for image reporting have previously been proposed for pelvic multiparametric MRI (17), bone scintigraphy (18), and many other techniques and indications (19,20). Precise description and organized classification of PSMA-ligand PET/CT findings are needed to serve both clinical reporting (to help with defining tumor extent, tailoring therapy, assessing prognosis, and facilitating exchange of information between centers) and research (to help with validating findings, pooling data within multicenter trials, and performing metaanalyses of published data).
The clinicopathologic TNM system of the American Joint Committee on Cancer and Union Internationale Contre le Cancer is the most widely used prostate cancer staging system (21). In clinical practice, the TNM score is based on a patchwork of information: local, nodal, and distant involvement are categorized by histopathologic examination after surgery or other tissue sampling, as well as clinical findings and imaging. Combination of all modalities improves staging, as each single modality comes with limitations: in prostate cancer clinical examination, ultrasound, CT, and MRI have a low sensitivity for metastases (22), whereas surgery and biopsy with subsequent histopathologic examination can evaluate only the dissected tissue and, thus, often underdiagnose prostate cancer metastases at extrapelvic regions or locations outside the operating or sampling field (23).
Detection of prostate cancer with PSMA-ligand PET/CT depends on target expression. On the basis of the high and specific target expression level of most prostate cancer cells, PSMA-ligand PET/CT detects more than 50% of lymph node metastases with a short diameter of at least 2.3 mm and more than 90% of those with a short diameter of at least 4.5 mm in a salvage lymphadenectomy setting (24). Staging is provided for the entire field of view and for regions otherwise inaccessible by surgery or biopsy. In view of these unique characteristics, we propose a molecular imaging TNM (miTNM) framework for PSMA-ligand PET/CT prostate cancer staging. This framework may also be applied for PSMA-ligand PET/MRI, SPECT/CT, or similar approaches. miTNM serves to provide standardized reporting of the presence, location, and extent of local prostate cancer and its pelvic spread; the presence, location, extent, and distribution pattern of extrapelvic metastases; the PSMA expression level of tumor lesions; and diagnostic confidence about reported findings.
To support acceptance, implementation, and correlation, definitions for the PSMA-ligand PET/CT miTNM framework were designed in analogy with the clinicopathologic TNM framework when possible. Categories describing the PSMA expression level and pattern of bone involvement were added—for example, to aid the planning of PSMA-directed therapy or the estimation of patient prognosis.
PSMA-ligand PET/CT provides high accuracy at substantial to almost-perfect reproducibility for TNM staging among readers with various levels of experience (25). Precise and reproducible staging was achieved even without detailed criteria for lesion positivity (25). Nevertheless, for successful application of miTNM in prostate cancer staging, it is crucial to have criteria for performing and interpreting PSMA-ligand PET/CT (26–28), as recently recommended in a joint guideline by the European Association of Nuclear Medicine and the Society of Nuclear Medicine and Molecular Imaging (27). Therefore, we have designed flowcharts on morphologic and PSMA-ligand PET findings to guide standardized image interpretation.
An overview of miTNM, version 1.0, is given in Tables 1 through 6 and Figures 1 through 4. Anatomic regions and disease patterns are detailed in the following sections.
miPSMA Expression Score
miTNM Classification for PSMA-Ligand PET/CT or PET/MRI
Sextant Segmentation of Prostate Gland
Lymph Node Regions
Pattern of Bone Involvement
Certainty and Final Diagnosis

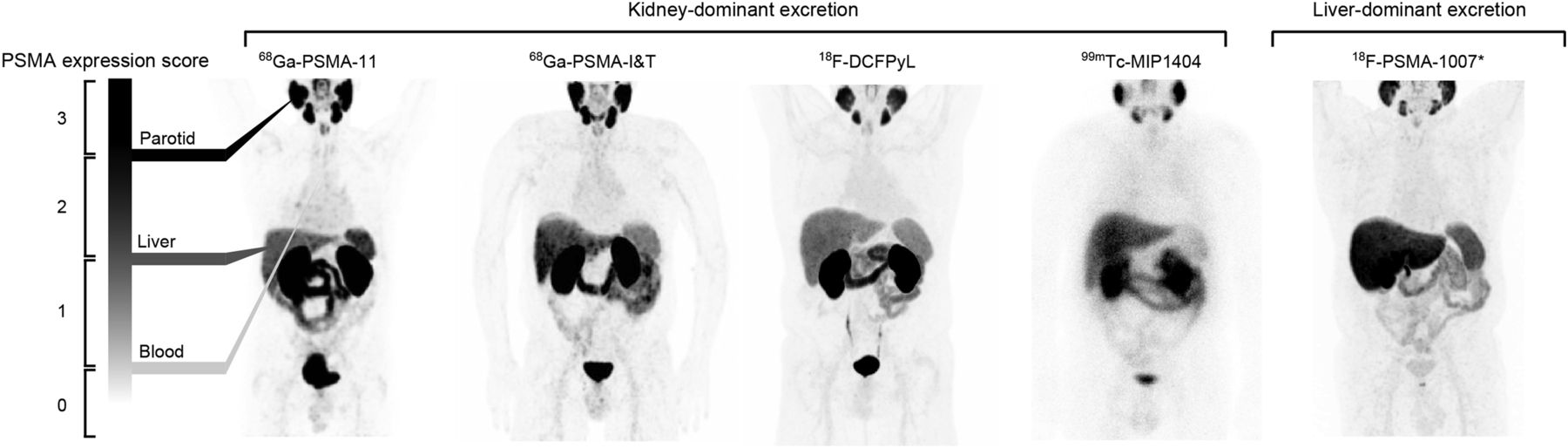
miPSMA expression score. Thresholds are demonstrated on 68Ga-PSMA11 PET maximum-intensity projection (left). For comparison, images are shown for 68Ga-PSMA-I&T scan, 18F-DCFPyL maximum-intensity projection at 1 h, 99mTc-MIP1404 planar scan at 3 h, and 18F-PSMA-1007 scan. *For PSMA ligands in which the ligand has liver-dominant excretion, spleen is recommended as reference organ instead of liver.
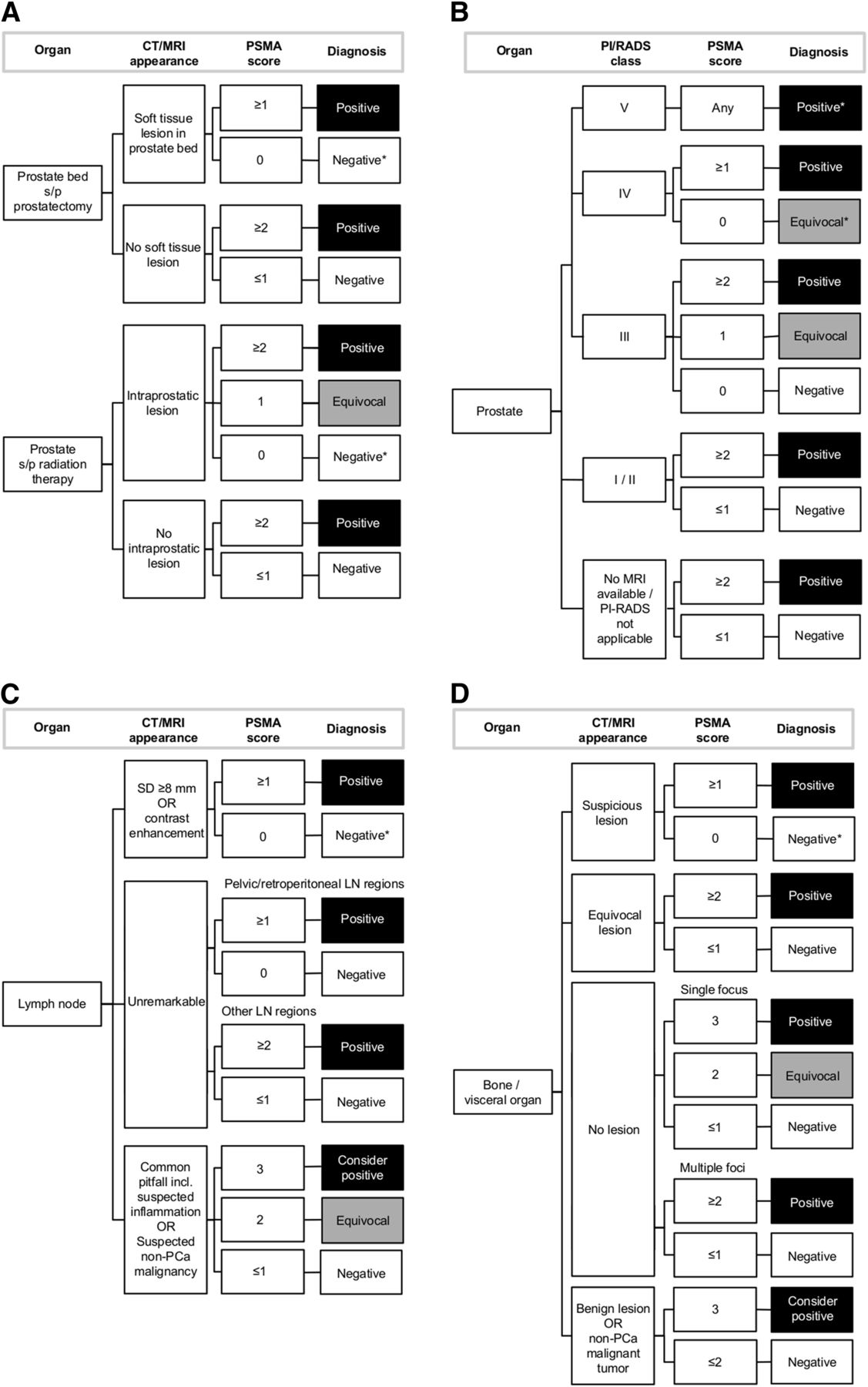
Guide for interpretation of PSMA-ligand PET/CT or PET/MRI. Criteria are given separately for imaging of prostate bed after prostatectomy or after radiation therapy (A), imaging of prostate for tumor detection or primary staging of cancer (B), imaging of lymph nodes (C), and imaging of bone or visceral organs (D). LN = lymph node; PCa = prostate cancer; SD = short-axis diameter; s/p = status post. *Consider PSMA-ligand–negative prostate cancer.
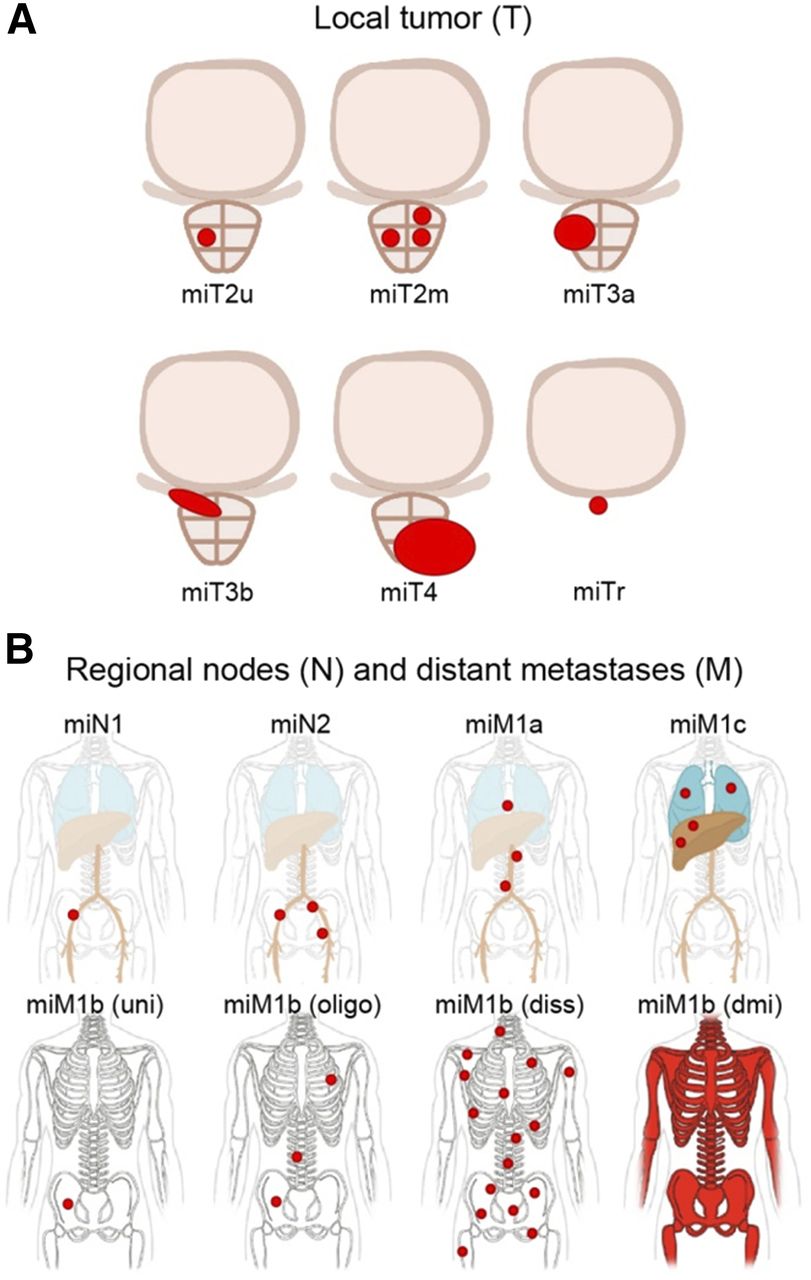
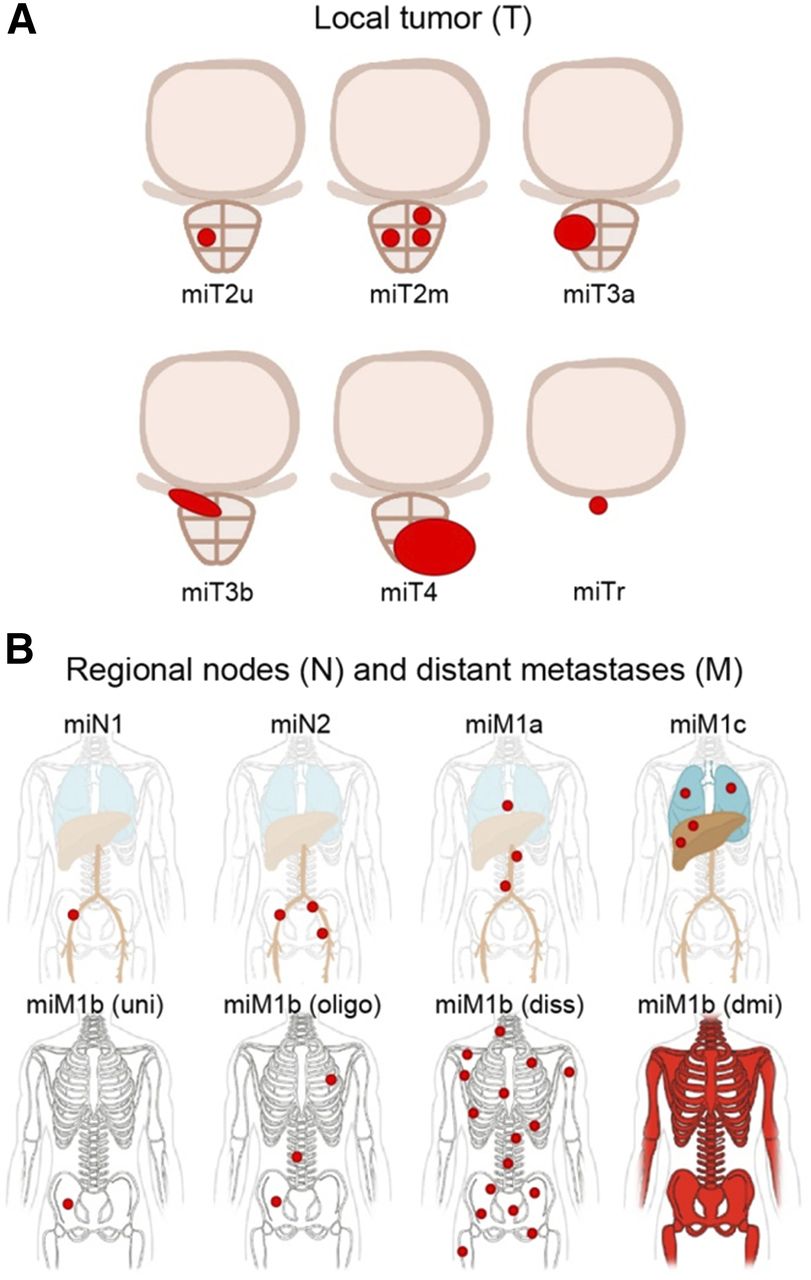
miTNM categories and pattern of bone involvement for reporting prostate cancer stage by PSMA-ligand PET/CT: local tumor extent (A) and pelvic node and distant metastases (B). Tumor involvement is delineated in red. Diss = disseminated; dmi = diffuse marrow involvement; oligo = oligometastatic; uni = unifocal.
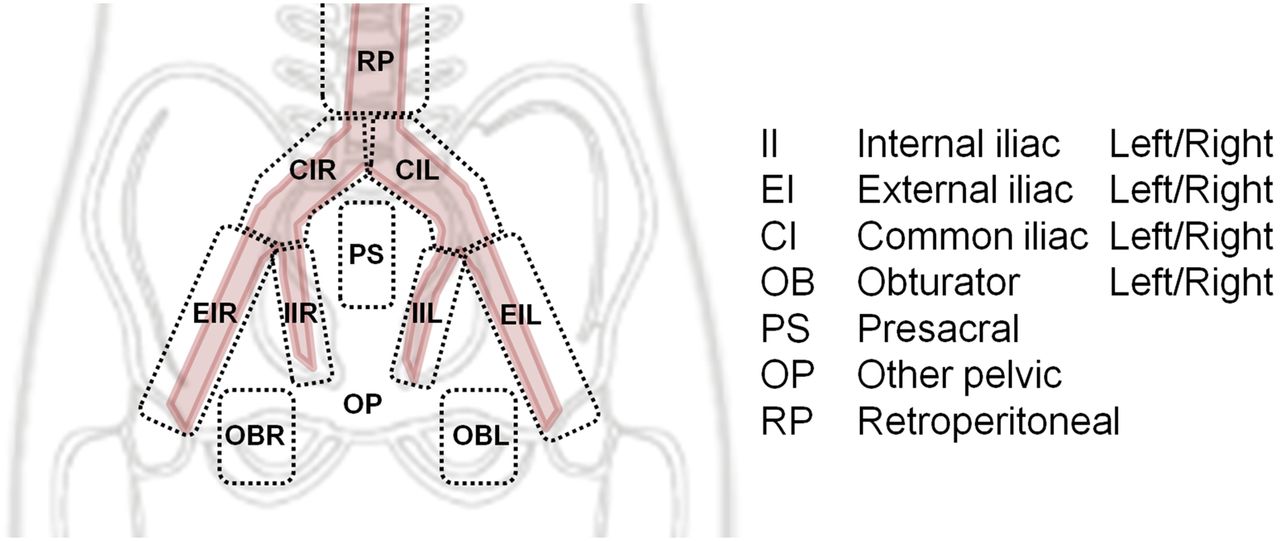
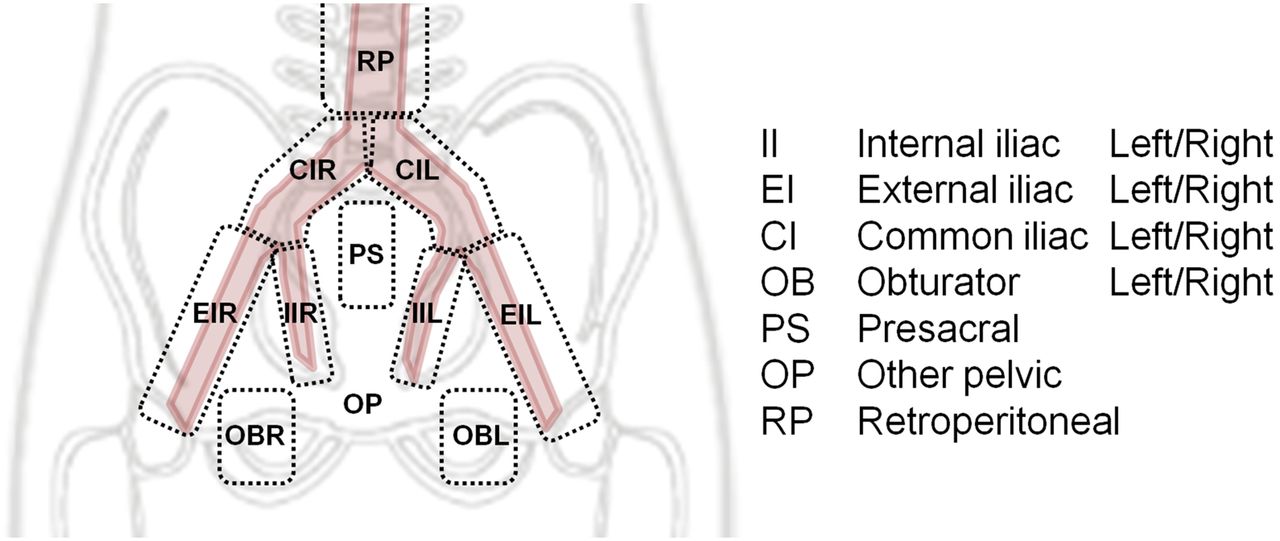
miTNM standard template for pelvic lymph node regions. Transition to retroperitoneal extrapelvic region is indicated.
PSMA EXPRESSION SCORE AND INTERPRETATION CRITERIA
Rationale
PSMA expression based on immunohistochemistry is known to correlate with tumor differentiation as well as prognosis (29–31). Loss of PSMA expression in metastases can indicate dedifferentiation and increasing tumor heterogeneity, leading to more aggressive phenotypes and a nonresponse to PSMA-directed therapy (32,33). In intraprostatic lesions, PSMA-ligand PET has been shown to correlate with tumor aggressiveness as defined by the Gleason score (6,34). Absence of PSMA expression as measured by PET in a primary tumor raises concerns about missed PSMA expression in its metastases and therefore provides important information for interpretation of PSMA-ligand PET results (5,35). Thus, information derived from noninvasive mapping of tumoral PSMA expression is valuable and should be reported for clinical and research PSMA-ligand PET.
miPSMA Score
We propose a miPSMA score that enables standardized reporting of PSMA expression as detected with PSMA-ligand PET. Expression categories are defined in relation to mean uptake in the blood pool, liver, and parotid gland (Table 1; Fig. 1). Results are reported as 0, 1, 2, or 3 for no, low, intermediate, or high PSMA expression, respectively. Scores 2 and 3 are empirically considered typical for prostate cancer lesions and favorable for PSMA-directed radioligand therapy. Expression level is determined visually, and we do not recommend uptake measurements on a regular basis. Occasionally, quantitative analyses might be necessary to correctly assign a specific miPSMA score.
On the basis of personal experience, we advise comparison of the mean SUVs of the respective lesions and the reference organ. The liver SUV can be measured by placing a 3-cm-diameter circular region of interest in the normal inferior right liver lobe in the axial plane; the blood pool, by centering a 2-cm-diameter circular region of interest in the aortic arch in the axial plane; the parotid gland, by centering a 1.5-cm-diameter circular region of interest in the right parotid gland in the axial plane; and a tumor lesion, by centering a 1-cm-diameter circular region of interest over the voxel with maximum uptake in the axial plane. Notably, SUV measurements in PSMA-ligand PET require further validation and investigation to clarify whether SUVmean, SUVmax, or SUVpeak is the most appropriate parameter.
Detailed comparative data are lacking on the biodistribution of various PSMA ligands. However, application of the miPSMA score for different PSMA ligands appears feasible because their biodistribution is grossly similar (Fig. 1). Known differences in biodistribution (e.g., higher blood-pool activity for 18F-DCFBC or higher liver uptake for 18F-PSMA1007) should be considered, especially when comparing studies using different ligands. For PSMA ligands with liver-dominant excretion (e.g., 18F-PSMA1007), the spleen is recommended instead of the liver for comparison against blood-pool and salivary gland uptake (36).
Interpretation
The miPSMA score alone is not suitable for diagnosing or excluding prostate cancer. Interpretation of miPSMA scores must be performed with consideration of the clinical context and other imaging findings and can vary for different tissue classes and even locations. A guide for the interpretation of PSMA-directed imaging based on CT, MRI, and PET findings is given in Figure 2. We designed flowcharts that are based on our clinical experience; however, interpretation critically depends on multiple factors, including indication, current therapy, prostate-specific antigen level, and prior clinical, imaging, or histopathologic findings. The criteria in Figure 2 are not to be taken as absolute definitions for positive, negative, or equivocal findings. Especially in patients with a rising, yet low, level of prostate-specific antigen and otherwise unremarkable imaging findings, even faint but focal uptake above the background level at a typical location may serve as an indicator of prostate cancer. The usability and potential further adoption of the miPSMA score is prone to prospective clinical validation. Definition of more detailed criteria for certain clinical situations, such as was recently proposed using a consensus reading with multiple Delphi rounds (28), is recommended.
The miPSMA score may become useful for selecting patients for targeted radiotherapy. At restaging, a decrease in the miPSMA score in conjunction with morphologic findings can help to identify dedifferentiation or response to therapy.
FINAL DIAGNOSIS AND CERTAINTY
The final diagnosis should ideally be either positive or negative for prostate cancer. Equivocal findings should be avoided and limited to certain settings, such as when other techniques may be able to clarify the findings. In addition, we recommend reporting diagnostic certainty using a 5-point scale (Table 6). Certainty will substantially vary depending on uptake, location, and CT or MRI findings. For instance, at biochemical recurrence, diagnostic certainty will be substantially higher when focal uptake is at a common location (e.g., internal iliac lymph node) than when at an uncommon location (e.g., rib). Certainty is further influenced by the specific clinical scenario; for example, faint uptake in the prostate gland after radiation therapy may often represent physiologic background activity, whereas any faint uptake in the former prostate bed after radical prostatectomy is highly suggestive.
Standardized wording for the final diagnosis and level of certainty will improve communication between the reader and the treating physician. Implementation into study protocols will allow identification of ambiguous judgments and potential pitfalls, aiding future improvement of PROMISE and miTNM. It will also be desirable to adjust the different categories with data based on studies using histopathologic correlation. This step will increase understanding between corresponding physicians and facilitate any potential consequences, such as a change in management.
LOCAL TUMOR (T)
Categorization of a local tumor is based on extent and organ confinement (Table 2; Fig. 3A). miT0 describes the absence of local recurrence in the pelvis both after radical prostatectomy and after radiation therapy. miT2 to miT4 categorize tumor extent with the prostate in place, either treated or untreated. Local-organ–confined tumor is defined as miT2u for unifocal involvement and miT2m for multifocal involvement. Extraprostatic extension is classified by 3 categories in accordance with the clinicopathologic TNM system: limited extraprostatic extension (miT3a), involvement of seminal vesicles (miT3b), and infiltration of external sphincter, rectum, bladder, levator muscles, or pelvic wall (miT4). Because of the low spatial resolution of PET, combination with appropriate cross-sectional imaging is needed to adequately judge extraprostatic extension. This is best achieved by complementing PSMA-ligand PET with multiparametric MRI either within a hybrid PET/MRI study or as a separate dataset available for image fusion. Notably, to avoid confusion with the clinicopathologic TNM system, in which T1 defines a tumor on histopathology with no correlation on palpation or any type of imaging, no miT1 category is used.
To describe the anatomic distribution of intraprostatic tumor extension and to facilitate a straightforward correlation between imaging and histopathology (6,37), information on prostate involvement is described on a sextant basis (Table 3). Sextant segments were chosen to provide information for biopsy, the common method of diagnosing prostate cancer. For ultrasound biopsy, image fusion encompassing both cognitive and software-based approaches is recommended (38–41). For traditional sextant segmentation, the craniocaudal extent of the prostate is divided into 3 equal-thickness volumes separated as falling to the left or right of the urethra: that is, left basal, right basal, left mid, right mid, left apical, and right apical segments (6,42). We are aware that more detailed descriptions of intraprostatic tumor involvement exist, such as the local template provided by PI-RADS (the Prostate Imaging and Reporting and Data System, version 2) (17). However, because our system is intended to harmonize image findings across PET/CT and PET/MRI, the sextant approach is most applicable. Outcome data, matched with the pathologic tumor stage, has indicated that tumor extent on a sextant basis or seminal vesicle infiltration is valuable prognostic information (43,44). Nevertheless, in dedicated studies using PET/MRI technology, further discrimination of the prostate gland in the peripheral, transition zone is recommended for reporting of intraprostatic tumor spread, such as by using the proposed template in PI-RADS.
Local recurrence after radical prostatectomy is categorized by miTr. Infiltration of pelvic structures should be detailed in the report. The probability of local tumor both after radical prostatectomy and after radiation therapy increases with focal uptake, higher miPSMA in the prostate (other than the bladder neck or urethra area), MRI showing a typical appearance of local tumor (diffusion restriction, contrast enhancement), or CT showing circumscribed contrast enhancement or signs of extraprostatic extension. A guide integrating the findings of PSMA-ligand PET and morphologic imaging is given in Figure 2A for local tumor after primary treatment and in Figure 2B for primary staging or tumor detection. PI-RADS is applicable only for detecting tumor in patients with an increased level of prostate-specific antigen; therefore, it should not be combined with interpretation of PSMA-ligand uptake for primary local staging after histologic confirmation (Fig. 2B). PSMA-ligand–positive pitfalls such as acute prostatitis and MRI-positive pitfalls such as postbiopsy changes and benign nodules must be ruled out. Notably, tumors with a low-Gleason-score pattern, and some rare entities such as intraductal carcinomas, tend to be negative on PSMA-ligand PET.
PELVIC NODES (N)
Pelvic node metastases are categorized as single involved nodal regions (miN1a) or multiple involved nodal regions (miN1b). Clinical data indicate that the number of metastatic lymph nodes on histopathology significantly affects disease progression and survival (e.g., recurrence-free survival at 10 y of >70% vs. 49% for patients with 1 or 2 vs. >5 positive lymph nodes) (45,46). In addition, it is generally accepted that histopathologic information from extended lymph node dissection is important for prognosis (47).
PSMA-ligand PET/CT is currently regarded as the most powerful application for providing a comprehensive overview of nodal involvement in the entire field of view. However, because PSMA-ligand PET/CT has failed to identify very small (<2 mm) lymph nodes, we feel that reporting based on traditional surgical templates is appropriate (24). A standardized template for pelvic lymph node regions provides anatomic information to facilitate comparison with surgery, histopathology, or other imaging findings (Table 4; Fig. 4). Such a template covers the different regions usually approached when extended lymph node dissection is performed (23). The anatomic structures delineating template regions for the pelvis, as adopted in two published reports (48,49), are described in Supplemental Table 1 (available at http://jnm.snmjournals.org). Each region is encoded by its initials, with bilateral regions further specified as left or right. Besides having prognostic value for determining disease extent, the specific location of lymph node metastases is critical for surgery and radiation therapy planning. For instance, the presacral and mesorectal regions, as well as the retroperitoneum, lie outside the typical surgical field.
The probability of nodal involvement increases not only with focal uptake and higher miPSMA score but also with lesion size, contrast enhancement, and location. A guide integrating findings in PSMA-ligand PET and morphologic imaging for pelvic N-staging is given in Figure 2C. CT and MRI abnormalities such as regional grouping, loss of fatty hilum, or focal necrosis may serve as additional morphologic criteria. PSMA-ligand–positive pitfalls such as focal uptake in the celiac ganglia or an adjacent ureter, inflammation, or lymphedema must be ruled out (7,25,50,51).
EXTRAPELVIC NODES AND DISTANT METASTASES (M)
PSMA-ligand PET/CT detects prostate cancer metastases with better sensitivity and specificity than conventional imaging (13–15). At biochemical recurrence, organ involvement can be diagnosed early (2,8,9) and the exact pattern of disease demonstrated. In accordance with the clinicopathologic TNM system, distant metastases are separated into 3 categories: extrapelvic lymph nodes (miM1a), bone metastases (miM1b), and organ metastases (miM1c) (Table 2; Fig. 3B). The location of miM1a nodes is categorized using a standard template (Table 4) as retroperitoneal, supradiaphragmatic, or other. Other lymph node regions or all affected organs in patients with organ involvement (miM1c) should be further specified in the final report.
PSMA-ligand PET/CT has been shown to be superior to bone scintigraphy in describing the extent of bone involvement (13). Bone disease is subcategorized as showing unifocal involvement, oligometastatic involvement, disseminated involvement, or diffuse marrow involvement (Table 5; Fig. 3B). Oligometastatic bone involvement is diagnosed when there are 3 or fewer bone lesions (52). When involvement is unifocal or oligometastatic, the involved bones should be specified. We acknowledge that the concept and final definition of oligometastatic disease are still under debate and that, for example, certain authors count all types of metastatic lesions up to a specific threshold (53). The pattern of bone involvement can have important implications for prognosis (52,54) and management (53). For instance, unifocal involvement may be targetable with curative intent by external-beam radiation therapy, and diffuse marrow involvement indicates elevated risk for hematotoxicity after radionuclide therapy (55–57).
The probability of bone or organ involvement increases with focal uptake, higher miPSMA score, and abnormalities on CT or MRI. For bone metastases, common CT findings include sclerotic, rarely lytic lesions with or without extraosseous extension, and common MRI findings include a low signal on unenhanced T1-weighted images. A guide integrating findings on PSMA-ligand PET and morphologic imaging for M-staging is given in Figure 2D. PSMA-ligand–positive pitfalls such as posttraumatic rib uptake and primary malignancies not related to prostate cancer must be ruled out (26). A comprehensive overview of the potential pitfalls for PSMA-ligand PET imaging has recently been published (51).
EXAMPLES
Figures 5– 7 provide 3 examples illustrating the use of miTNM in different clinical scenarios.
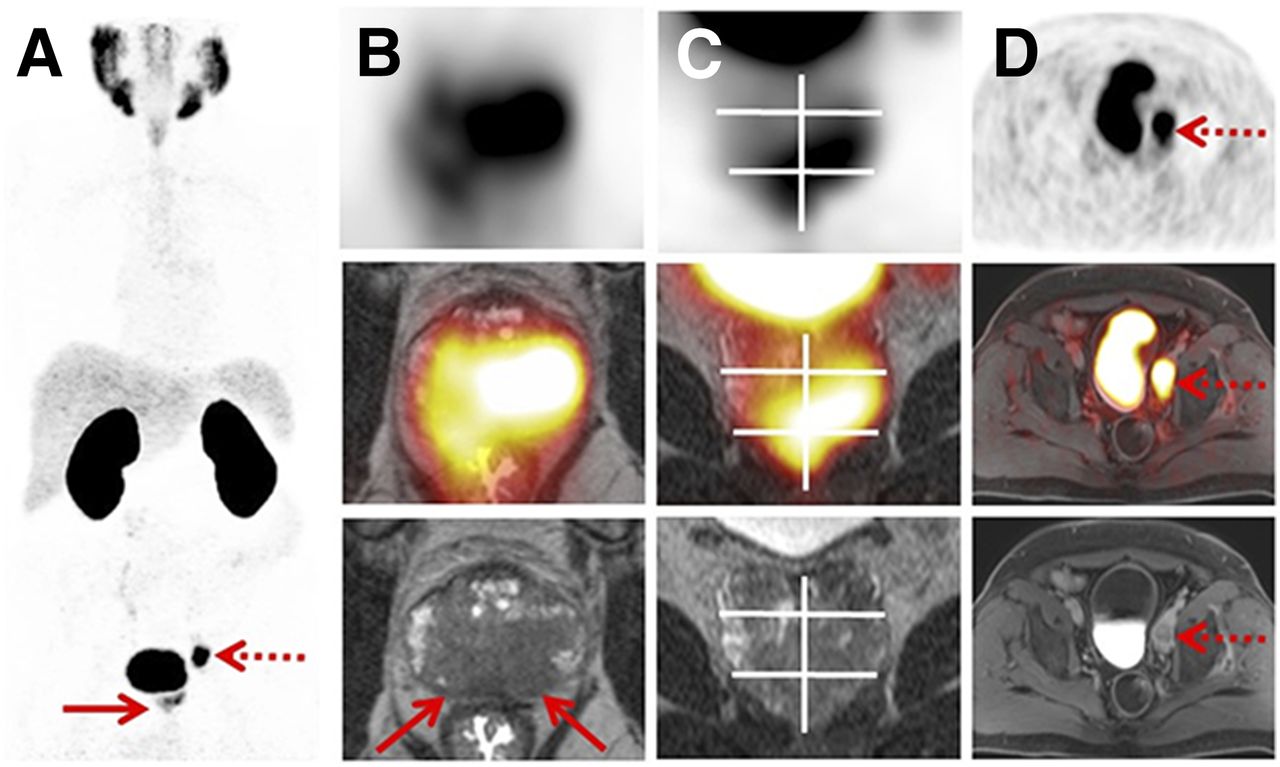
Primary staging using 68Ga-PSMA11 PET/high-resolution T2-weighted MRI of prostate in 65-y-old patient with histopathologically proven prostate cancer: PET maximum-intensity projection (A) and axial PET/MRI (B), coronal PET/MRI (C), and axial PET/MRI (PET at top, PET/MRI in middle, and MRI at bottom). Sextant segment boundaries are shown on coronal images in white. Maximum-intensity projection demonstrates intermediate PSMA expression (score 2) in prostate gland (solid arrow) and high PSMA expression (score 3) in regional pelvic lymph node (dotted arrow). Axial and coronal MRI show bilateral T2-hypointense lesions corresponding to uptake on PSMA-ligand PET and clearly exceeding prostate margins, indicative of extraprostatic extension (T3a; solid arrows). Axial and coronal PET/MRI show bilateral involvement of apical and mid segments and of left basal segment on MR images. Axial imaging shows single lymph node metastasis in left obturator region (dotted arrows). Final diagnosis was miT3aN1(OBL)M0. All findings were confirmed by postoperative histopathologic examination.

68Ga-PSMA11 PET/CT restaging in 62-y-old patient with biochemically recurrent prostate cancer and rising level of prostate-specific antigen: PET maximum-intensity projection (A) and 2 levels of axial PET/CT (B and C), with PET at top, PET/CT in middle, and CT at bottom. Maximum-intensity projection and axial images in B demonstrate multiple retroperitoneal and supradiaphragmatic lymph node metastases with intermediate PSMA expression (score 2, solid arrows). In total, 3 bone lesions (dotted arrows) define oligometastatic bone involvement. (C) Sclerotic bone metastasis in thoracic spine demonstrates low PSMA expression (score 1). Final diagnosis was miT0N0M1a(RP, SD)b(oligo).

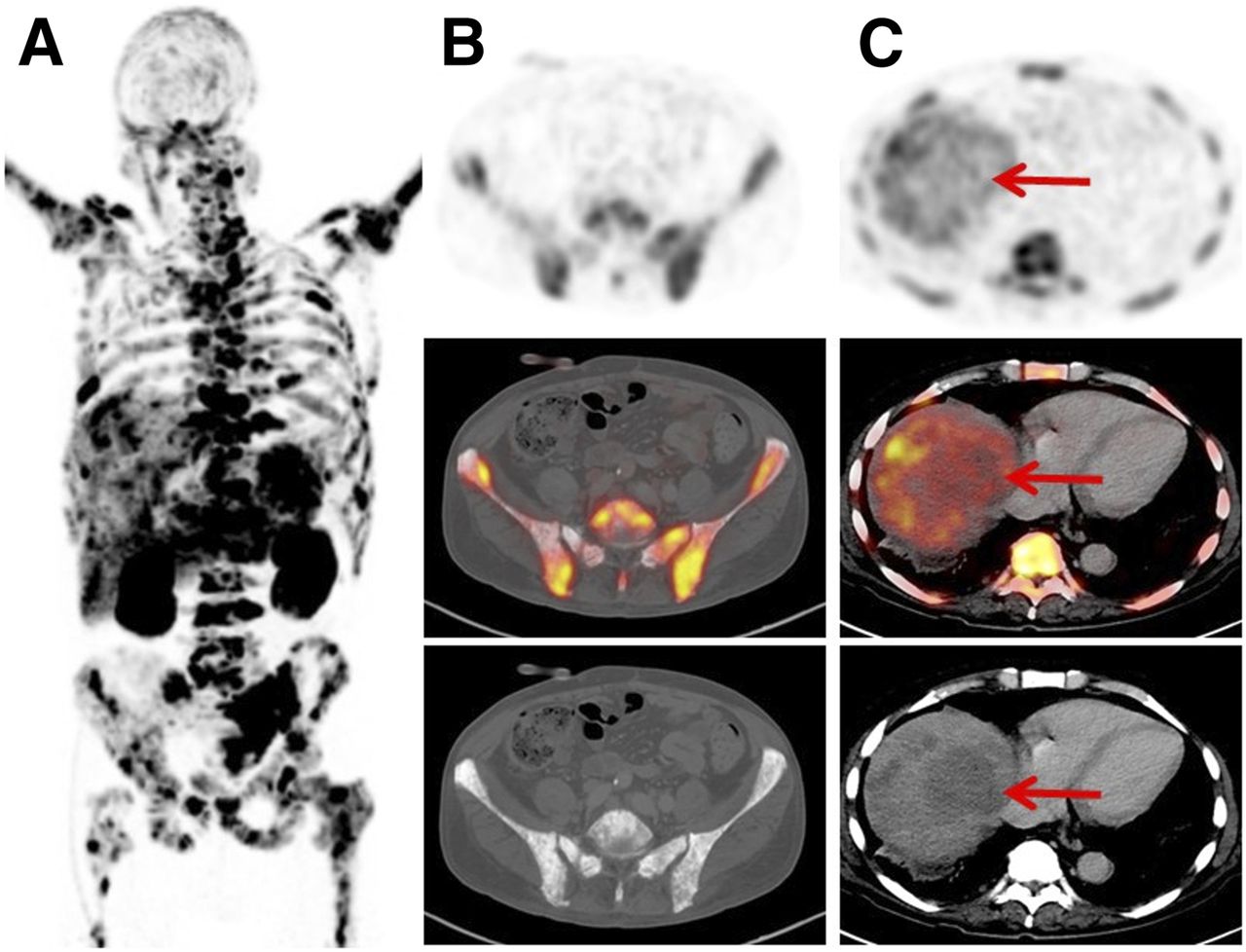
68Ga-PSMA11 PET/CT restaging in 76-y-old patient with advanced metastatic castration-resistant prostate cancer before potential PSMA-radioligand therapy: PET maximum-intensity projection (A) and 2 levels of axial PET/CT (B and C). PET/CT shows diffuse skeletal uptake with low to high PSMA expression (score 1–3). PET/CT shows multiple liver metastases with low PSMA expression (arrows, score 1). Final diagnosis was miT0N0M1b(dmi)c(liver). PSMA-radioligand therapy was omitted because of diffuse marrow involvement and low PSMA expression in liver metastases.
LIMITATIONS
The aim of miTNM is to create a framework for PSMA-ligand PET reporting. We realize that—like the first clinicopathologic TNM proposal and other image classification systems—initial definitions are arbitrary and not supported by strong clinical evidence. We admit that although our approach parallels the now extensively validated clinicopathologic TNM, miTNM is based only on our joint experience and the supporting evidence, with no prognostic validation having been performed. The historical development of classification systems for imaging (e.g., BI-RADS, PI-RADS, RECIST, and PERCIST) demonstrates that after an initial proposal with often a limited scientific basis, further sequential adjustments have been made to optimize applicability and clinical validity. We expect and desire a similar process for the miTNM system presented here. The system will evolve as more evidence becomes available for PSMA-ligand PET/CT and patient outcome. miTNM remains inclusive for other staging systems focusing on local staging or management decisions.
Currently, there are several different PSMA ligands in clinical use. Because comparative data on biodistribution and uptake in tumors are not currently available, caution is warranted when comparisons are made between studies applying different PSMA ligands. Therefore, we highly recommend that the specific PSMA ligand be disclosed and that the same ligand be used when follow-up imaging is performed. Notably, this proposal focuses on small ligands, because antibodies (e.g., J591), minibodies, and other, larger, molecules with affinity to PSMA demonstrate a substantially different biodistribution and currently lack data describing their clinical use (58).
FUTURE DEVELOPMENT
PSMA-ligand PET enables unprecedented delineation of whole-body tumor burden based on high target-to-background expression levels (Supplemental Fig. 1) (59). Introduction of tools for whole-body tumor volumetry based on a combination of molecular and morphologic techniques might overcome several limitations of solely morphology-based criteria, such as RECIST (60): lesions without distinct morphologic boundaries, such as bone metastases, could be included in the evaluation. Molecular imaging also offers the potential to acknowledge target expression as part of a quantitative imaging biomarker, and lesions can be subselected by certain target definitions, minimizing potential bias. Consequently, direct assessment of tumor volume, instead of assessment of lesion diameter sums, could be done. For PSMA-ligand PET, initial attempts have been made by introducing PSMA-derived tumor volume, total lesion PSMA, or bone PET indices (59,61). Further advances in the field of software-assisted tumor delineation will help to automatically delineate—separately for bone and soft tissue—total tumor volume, total tumor target expression, or a combination of these. Prospective clinical evaluation is mandatory to assess their potential for predicting prognosis and response in patients with PSMA-expressing prostate cancer.
SUMMARY
We propose miTNM, version 1.0, as a standardized framework for reporting the results of PSMA-ligand PET/CT or PET/MRI. miTNM organizes the staging of whole-body prostate cancer by including information on exact location, pattern of disease distribution, PSMA expression, and level of certainty. miTNM aims to aid information exchange by unifying clinical and research reporting of PSMA-ligand imaging. Prospective evaluation of miTNM needs to be performed and its impact on patient prognosis and management assessed.
DISCLOSURE
Wolfgang Fendler received a scholarship from the Deutsche Forschungsgemeinschaft (grant 807122). Jeremie Calais received a grant from the Fondation ARC pour la recherche sur le cancer (grant SAE20160604150). Matthias Eiber received funding from the Deutsche Forschungsgemeinschaft within Sonderforschungsbereich 824 (project B11). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Marie Bieth for contributing a case demonstrating software-algorithm–based automatic delineation of tumor volume. We thank Torsten Kuwert, Christian Schmidkonz, Thorsten Derlin, Steve Rowe, and Michael A. Gorin for contributing images outlining the biodistribution of 99mTc-MIP1404, 68Ga-PSMA I&T, and 18F-DCFPyL.
Footnotes
Guest Editor: David Mankoff, University of Pennsylvania.
Published online Nov. 9, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 23, 2017.
- Accepted for publication October 5, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 99mTc-MIP-1404 SPECT/CT Companion Diagnostic for 177Lu-PSMA Therapy in Metastatic Castration-Resistant Prostate Cancer
- Pattern of Failure in Patients with Biochemical Recurrence After PSMA Radioguided Surgery
- Perspective on Pattern of Failure in Patients with Biochemical Recurrence After PSMA Radioguided Surgery
- Association of Free-to-Total PSA Ratio and 18F-DCFPyL Prostate-Specific Membrane Antigen PET/CT Findings in Patients with Biochemical Recurrence After Radical Prostatectomy: A Prospective Single-Center Study
- Diagnostic Efficacy of Various Imaging Modalities Across Different Stages of Prostate Cancer: A Network Meta-Analysis of Diagnostic Studies
- Clinical Factors That Influence Repeat 68Ga-PSMA-11 PET/CT Scan Positivity in Patients with Recurrent Prostate Cancer Under Observation After a Negative 68Ga-PSMA-11 PET/CT Scan: A Single-Center Retrospective Study
- [68Ga]Ga-PSMA-11 PET and Prostate Cancer Bone Metastases: Diagnostic Performance of Available Standardized Criteria
- Current Status of Prostate-specific Membrane Antigen-targeted Alpha Radioligand Therapy in Prostate Cancer
- The Diagnostic Value of the Sentinel Node Procedure to Detect Occult Lymph Node Metastases in PSMA PET/CT Node-Negative Prostate Cancer Patients
- 68Ga-PSMA PET/CT-Based Atlas for Prostate Bed Recurrence After Radical Prostatectomy: Clinical Implications for Salvage Radiation Therapy Contouring Guidelines
- Prognostic Role of 68Ga-PSMA11 PET-Based Response in Patients with Prostate Cancer Undergoing Taxane-Based Chemotherapy
- Unspecific 18F-PSMA-1007 Bone Uptake Evaluated Through PSMA-11 PET, Bone Scanning, and MRI Triple Validation in Patients with Biochemical Recurrence of Prostate Cancer
- Is 18F-FDG PET Needed to Assess 177Lu-PSMA Therapy Eligibility? A VISION-like, Single-Center Analysis
- PSMA-Directed Imaging and Therapy of Salivary Gland Tumors: A Single-Center Retrospective Study
- Predicting Outcomes of Indeterminate Bone Lesions on 18F-DCFPyL PSMA PET/CT Scans in the Setting of High-Risk Primary or Recurrent Prostate Cancer
- Eligibility for 177Lu-PSMA Therapy Depends on the Choice of Companion Diagnostic Tracer: A Comparison of 68Ga-PSMA-11 and 99mTc-MIP-1404 in Metastatic Castration-Resistant Prostate Cancer
- Feasibility of 99mTc-MIP-1404 for SPECT/CT Imaging and Subsequent PSMA-Radioguided Surgery in Early Biochemically Recurrent Prostate Cancer: A Case Series of 9 Patients
- A 2022 International Survey on the Status of Prostate Cancer Theranostics
- 68Ga-PSMA-11 PET/MRI in Patients with Newly Diagnosed Intermediate- or High-Risk Prostate Adenocarcinoma: PET Findings Correlate with Outcomes After Definitive Treatment
- Reproducibility of PSMA PET/CT Imaging for Primary Staging of Treatment-Naive Prostate Cancer Patients Depends on the Applied Radiotracer: A Retrospective Study
- Utility of 18F-rhPSMA-7.3 PET for Imaging of Primary Prostate Cancer and Preoperative Efficacy in N-Staging of Unfavorable Intermediate- to Very High-Risk Patients Validated by Histopathology
- 18F-DCFPyL PET Acquisition, Interpretation, and Reporting: Suggestions After Food and Drug Administration Approval
- Repeatability of 68Ga-PSMA-HBED-CC PET/CT-Derived Total Molecular Tumor Volume
- An 89Zr-Labeled PSMA Tracer for PET/CT Imaging of Prostate Cancer Patients
- aPROMISE: A Novel Automated PROMISE Platform to Standardize Evaluation of Tumor Burden in 18F-DCFPyL Images of Veterans with Prostate Cancer
- PSMA PET Validates Higher Rates of Metastatic Disease for European Association of Urology Biochemical Recurrence Risk Groups: An International Multicenter Study
- The Added Value of 18F-FDG PET/CT Compared with 68Ga-PSMA PET/CT in Patients with Castration-Resistant Prostate Cancer
- PSMA PET for the Assessment of Metastatic Hormone-Sensitive Prostate Cancer Volume of Disease
- Assessing Response to 177Lu-PSMA Radioligand Therapy Using Modified PSMA PET Progression Criteria
- Detection Efficacy of 18F-rhPSMA-7.3 PET/CT and Impact on Management in Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy and Before Potential Salvage Treatment
- Prostate-specific membrane antigen is a biomarker for residual disease following neoadjuvant intense androgen deprivation therapy in prostate cancer
- Early Injection of Furosemide Increases Detection Rate of Local Recurrence in Prostate Cancer Patients with Biochemical Recurrence Referred for 68Ga-PSMA-11 PET/CT
- 68Ga-PSMA-11 PET/CT Improves Tumor Detection and Impacts Management in Patients with Hepatocellular Carcinoma
- Correlation of Lesional Uptake Parameters and Ratios with miPSMA Score and Estimating Normal Physiologic Concentration: An Exploratory Analysis in Metastatic Castration-Resistant Prostatic Carcinoma Patients with 68Ga-PSMA-11 PET/CT
- The Annual Journal Impact Factor Saga
- The Impact of Monosodium Glutamate on 68Ga-PSMA-11 Biodistribution in Men with Prostate Cancer: A Prospective Randomized, Controlled Imaging Study
- Radiation Dosimetry of 99mTc-PSMA I&S: A Single-Center Prospective Study
- Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study
- Positive Predictive Value and Correct Detection Rate of 18F-rhPSMA-7 PET in Biochemically Recurrent Prostate Cancer Validated by Composite Reference Standard
- Reply: The Importance of an Adequate Surgical Template During Salvage Lymph Node Dissection for Node-Recurrent Prostate Cancer
- Biochemical Persistence of Prostate-Specific Antigen After Robot-Assisted Laparoscopic Radical Prostatectomy: Tumor Localizations Using PSMA PET/CT Imaging
- Liver Enzyme Elevation After 177Lu-PSMA Radioligand Therapy for Metastasized Castration-Resistant Prostate Cancer
- Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer
- Identification of PCWG3 Target Populations Is More Accurate and Reproducible with PSMA PET Than with Conventional Imaging: A Multicenter Retrospective Study
- Automated analysis of PSMA-PET/CT studies using convolutional neural networks
- 68Ga-PSMA PET/CT for Primary Lymph Node and Distant Metastasis NM Staging of High-Risk Prostate Cancer
- PSMA-Ligand PET for Early Castration-Resistant Prostate Cancer: A Retrospective Single-Center Study
- Semiautomatically Quantified Tumor Volume Using 68Ga-PSMA-11 PET as a Biomarker for Survival in Patients with Advanced Prostate Cancer
- Factors Predicting Metastatic Disease in 68Ga-PSMA-11 PET-Positive Osseous Lesions in Prostate Cancer
- Impact of 68Ga-PSMA-11 PET on the Management of Recurrent Prostate Cancer in a Prospective Single-Arm Clinical Trial
- 18F-DCFPyL PET/CT in Patients with Subclinical Recurrence of Prostate Cancer: Effect of Lesion Size, Smoothing Filter, and Partial-Volume Correction on PROMISE Criteria
- 68Ga-PSMA PET/CT Combined with PET/Ultrasound-Guided Prostate Biopsy Can Diagnose Clinically Significant Prostate Cancer in Men with Previous Negative Biopsy Results
- Impact of 68Ga-PSMA-11 PET/CT on Staging and Management of Prostate Cancer Patients in Various Clinical Settings: A Prospective Single-Center Study
- Mapping Prostate Cancer Lesions Before and After Unsuccessful Salvage Lymph Node Dissection Using Repeat PSMA PET
- 11C-Choline PET/CT in Recurrent Prostate Cancer: Retrospective Analysis in a Large U.S. Patient Series
- Proposal for Systemic-Therapy Response-Assessment Criteria at the Time of PSMA PET/CT Imaging: The PSMA PET Progression Criteria
- Intraindividual Comparison of 18F-PSMA-1007 with Renally Excreted PSMA Ligands for PSMA PET Imaging in Patients with Relapsed Prostate Cancer
- Evaluation of an Automated Module Synthesis and a Sterile Cold Kit-Based Preparation of 68Ga-PSMA-11 in Patients with Prostate Cancer
- Comparison of 3 Interpretation Criteria for 68Ga-PSMA11 PET Based on Inter- and Intrareader Agreement
- Prostate-Specific Membrane Antigen PET/CT Combined with Sentinel Node Biopsy for Primary Lymph Node Staging in Prostate Cancer
- Total-Body 68Ga-PSMA-11 PET/CT for Bone Metastasis Detection in Prostate Cancer Patients: Potential Impact on Bone Scan Guidelines
- An 18F-Labeled PSMA Ligand for PET/CT of Prostate Cancer: First-in-Humans Observational Study and Clinical Experience with 18F-JK-PSMA-7 During the First Year of Application
- Lesion Detection and Interobserver Agreement with Advanced Image Reconstruction for 18F-DCFPyL PET/CT in Patients with Biochemically Recurrent Prostate Cancer
- Prostate-Specific Membrane Antigen Ligand Positron Emission Tomography in Men with Nonmetastatic Castration-Resistant Prostate Cancer
- Improving 68Ga-PSMA PET/MRI of the Prostate with Unrenormalized Absolute Scatter Correction
- Intention-to-Treat Analysis of 68Ga-PSMA and 11C-Choline PET/CT Versus CT for Prostate Cancer Recurrence After Surgery
- qPSMA: Semiautomatic Software for Whole-Body Tumor Burden Assessment in Prostate Cancer Using 68Ga-PSMA11 PET/CT
- Healthy Tissue Uptake of 68Ga-Prostate-Specific Membrane Antigen, 18F-DCFPyL, 18F-Fluoromethylcholine, and 18F-Dihydrotestosterone
- Combination of 68Ga-PSMA PET/CT and Multiparametric MRI Improves the Detection of Clinically Significant Prostate Cancer: A Lesion-by-Lesion Analysis
- Metaanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology
- Novel Structured Reporting Systems for Theranostic Radiotracers
- Follow-up of Lesions with Equivocal Radiotracer Uptake on PSMA-Targeted PET in Patients with Prostate Cancer: Predictive Values of the PSMA-RADS-3A and PSMA-RADS-3B Categories
- PSMA Ligand PET/MRI for Primary Prostate Cancer: Staging Performance and Clinical Impact
- Interobserver Agreement for the Standardized Reporting System PSMA-RADS 1.0 on 18F-DCFPyL PET/CT Imaging
- Potential Impact of 68Ga-PSMA-11 PET/CT on the Planning of Definitive Radiation Therapy for Prostate Cancer
- Detection Threshold and Reproducibility of 68Ga-PSMA11 PET/CT in a Mouse Model of Prostate Cancer