


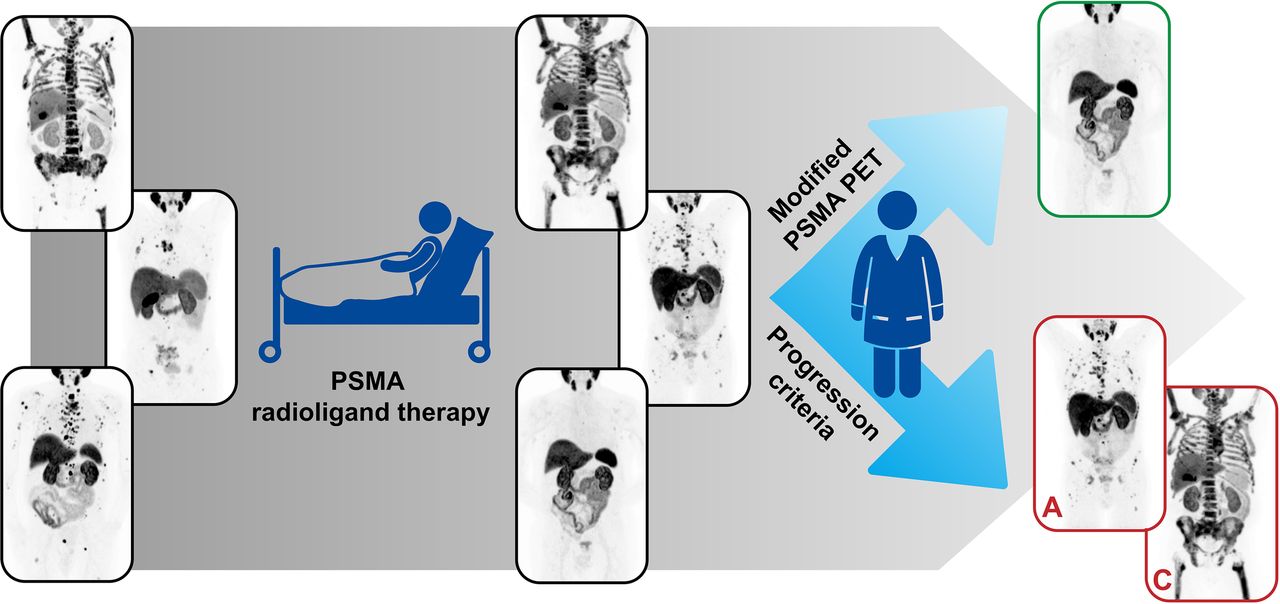
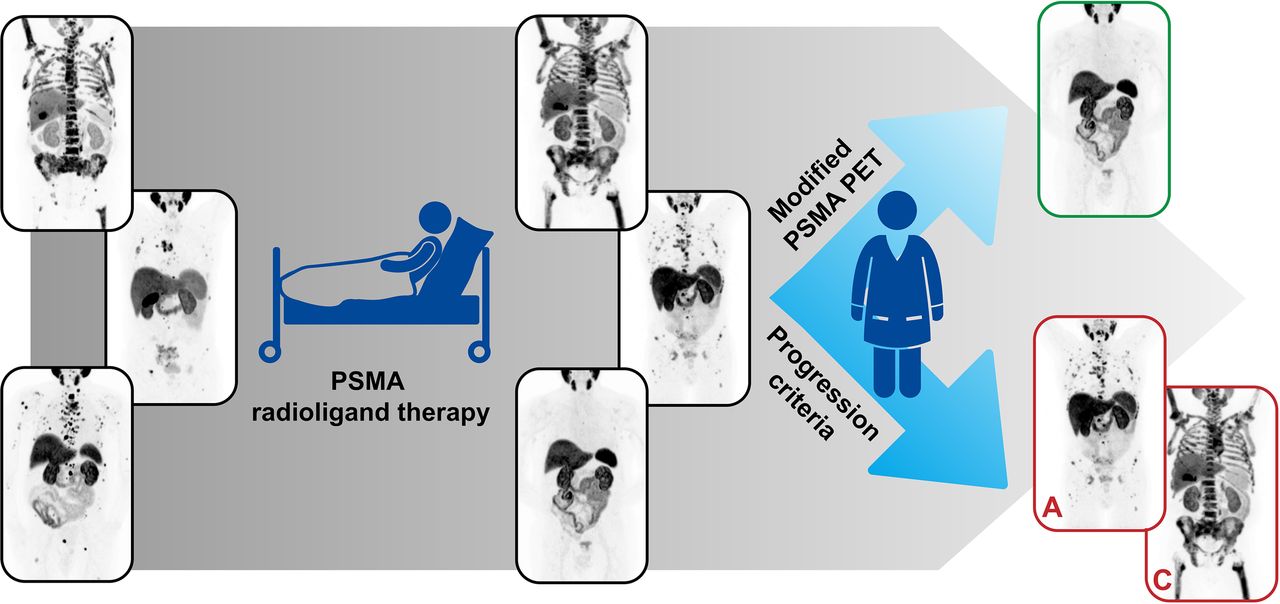
Visual Abstract
Abstract
PET/CT targeting the prostate-specific membrane antigen (PSMA) plays a key role in staging of patients with prostate cancer. Moreover, it is used not only for the assessment of adequate PSMA expression of prostate cancer cells before PSMA-targeting radioligand therapy (RLT) but also for restaging during the course of therapy to evaluate response to treatment. Whereas no established criteria exist for systematic response evaluation so far, recently proposed PSMA PET Progression (PPP) criteria might fill this gap. The aim of this study was to assess the feasibility of PPP criteria in patients undergoing PSMA RLT and their prognostic implications. Methods: In this retrospective analysis, PSMA PET/CT scans of 46 patients before and after completion of PSMA RLT were analyzed separately by 2 readers using modified PPP criteria. After interobserver agreement assessment, consensus results (progressive vs. nonprogressive disease) were compared in a multivariate Cox regression model (endpoint, overall survival [OS]). Results: Interobserver agreement using the modified PPP criteria was substantial (Cohen κ = 0.73), with a concordance in 87% of patients. The median OS of all patients after PSMA RLT (n = 46) was 9.0 mo (95% CI, 7.8–10.2 mo). Progression according to the modified PPP criteria was found in 32 patients and was a significant (P ≤ 0.001) prognostic marker for OS, with a hazard ratio of 15.5 (95% CI, 3.4–70.2). Conclusion: Response assessment in patients undergoing PSMA RLT using modified PPP criteria are reproducible and highly prognostic for OS. The modified PPP criteria should be validated in future prospective trials.
PET/CT targeting prostate-specific membrane antigen (PSMA) has become a key role in staging of patients with prostate cancer. To develop systematic and reproducible evaluation criteria, several proposals for assessing PSMA PET/CT have been made (1–3). However, no established criteria for therapy response assessment by PSMA PET/CT exist so far, and response assessment in patients with prostate cancer is still based on serum prostate-specific antigen (PSA) level and on bone scintigraphy and CT scans as recommended by, for example, the Prostate Cancer Working Group 3 (4).
Especially in the context of PSMA radioligand therapy (RLT), PSMA PET/CT is frequently used to assess adequate PSMA expression of prostate cancer cells not only before but also during the course of therapy to evaluate response to treatment (5). Therefore, an evaluation system that is easy to implement, simple to use, and reproducible is desirable not only for clinical routine but also for clinical trials. Although different approaches have already been suggested for assessing response to treatment in metastatic prostate cancer using RECIST 1.1 (6–8), adapted PERCIST (7–9), or the quantification of whole-body tumor burden (10–15), they have not yet been clinically implemented.
Obviously, there is a need for an easy, fast, and reproducible validation system to assess response to PSMA RLT. Fanti et al. recently published the PSMA PET Progression (PPP) criteria, which include PSMA PET/CT, biochemical response, and clinical parameters. They focused on disease progression as defined by 3 categories (16). Although promising, these response assessment criteria have not yet been tested for feasibility in patients with advanced prostate cancer receiving PSMA RLT.
The aim of this retrospective analysis was to evaluate the feasibility of PPP criteria in patients undergoing PSMA RLT and to assess the prognostic implications of these criteria. Therefore, PSMA PET/CT scans before and after completion of RLT were analyzed and the results were correlated to overall survival (OS).
MATERIALS AND METHODS
Patient Cohort
All patients treated on a compassionate-use basis with at least 1 cycle of PSMA RLT between February 2016 and April 2020 at our department were screened for eligibility. In suitable patients, both initial and follow-up PET/CT had to be performed with the same PSMA radioligand (68Ga-PSMA-11 or 18F-PSMA-1007) but not necessarily on the same PET/CT scanner. Other inclusion criteria were in-house assessment of imaging and laboratory data and the availability of survival data. Patients without a follow-up PET/CT scan (i.e., in cases of clinical progress) were excluded from the study. The time points of the PET/CT scans were before therapy and after the final cycle of PSMA RLT. The last follow-up was in October 2020, and 33 patients had died by that time point. The median time of follow-up in surviving patients was 14 mo (95% CI, 12.9–15.1 mo). The review board of the University of Freiburg (protocol 562/15) approved this study, and all subjects gave written informed consent.
Imaging and Treatment Protocol
At 1 h (68Ga-PSMA-11) or 2 h (18F-PSMA-1007) after injection of the respective tracer, whole-body PSMA PET scans were acquired from skull to mid thigh with a scan duration of 2 min per bed position. A contrast-enhanced diagnostic CT scan (120 kVp, 100–400 mAs) with dose modulation was performed for anatomic correlation and attenuation correction. Scanning was performed on a Vereos Digital PET/CT device, a Gemini TF 64 PET/CT device, or a Gemini TF 16 Big-Bore PET/CT device (all Philips Healthcare). All patients were asked to void before undergoing PET. Images were reconstructed with a vendor-specific reconstruction algorithm (blob ordered-subset time-of-flight) with 3 iterations and 9 subsets (relaxation parameter, 0.35) and a voxel size of 2 × 2 × 2 mm (Vereos Digital PET/CT) or with 3 iterations and 33 subsets (relaxation parameter, 0.35) and a voxel size of 2 × 2 × 2 mm (Gemini TF 64 PET/CT and Gemini TF 16 Big-Bore PET/CT). The spatial resolution of the reconstructed PET images is about 5 mm (Vereos) to 7 mm (both Gemini TF) in full width at half maximum.
A standardized institutional protocol for RLT was applied according to current guidelines (17). In-house labeling was performed for 177Lu-PSMA 617. The standard PSMA RLT protocol consisted of infusion of 6.0 GBq of the radioligand every 6–8 wk with up to a maximum of 4 cycles depending on response to treatment, as assessed by PSMA PET/CT and laboratory data 6–8 wk after every second cycle. In the case of only 3 treatment cycles, an additional PET/CT scan was performed 6–8 wk after the third cycle.
Response Assessment Using Modified PPP Criteria
PET/CT images were retrospectively analyzed by 2 readers (with 1 and 4 y of PSMA PET/CT reading experience) using the local PACS system IMPAX EE (Agfa HealthCare). For response assessment, 3 categories defining progression adapted from PPP criteria were used (Table 1) (16). Exclusion of these 3 categories was defined as nonprogressive. After the assessment of interobserver agreement, a final consensus was reached and used for further comparisons.
Progression on PSMA PET/CT in Accordance with Modified PPP Criteria
The original category C had to be changed from “increase in size or uptake of one or more lesions” to a “visually assessed distinct increase in the PSMA-positive tumor volume,” as the original category was not applicable in cases of diffuse bone marrow involvement and no validated quantification assessment of the whole-body tumor burden on 18F-PSMA-1007 PET/CT exists so far. However, recent studies report promising results for the manual and semiautomatic quantification of whole-body tumor burden on 68Ga-PSMA-11 PET/CT using a 50% threshold of local SUVmax (PSMATV50) (14,15). Hence, PSMATV50 was assessed in all patients without new lesions on PSMA PET/CT (e.g., category C and all patients rated nonprogressive) by 1 reader in order to test the suitability of category C. For this assessment, the Beth Israel plug-in for Fiji (18) from the Beth Israel Deaconess Medical Center was used. A relative threshold of 50% of SUVmax within a segmented volume was applied, and the volumes of the segmented lesions were summed to PSMATV50.
Since the increase in laboratory data is not defined by PPP criteria, an arbitrary cutoff of at least 25% (in analogy to the criteria of the Prostate Cancer Clinical Trials Working Group 3 (4)) was chosen for PSA, lactate dehydrogenase, and alkaline phosphatase according to results of Yordanova et al. (19). Changes in neuron-specific enolase were included in order to detect possible neuroendocrine dedifferentiation.
Response of Serum PSA Level
Response of serum PSA level was assessed in all patients, comparing PSA values from the time of first-cycle administration to the time of the last PET/CT examination (i.e., end of therapy). In analogy to the criteria of the Prostate Cancer Clinical Trials Working Group 3 (4), biochemical progression was defined as a rise in serum PSA level of at least 25%, and patients were dichotomously divided into progressive or nonprogressive accordingly.
Finally, the OS of progressive and nonprogressive patients as assessed with both categorization systems (PPP and PSA-level only) was compared in uni- and multivariate analysis with the following possible confounders: time since initial diagnosis, number of lines of therapy before PSMA RLT, total injected activity for PSMA RLT, number of therapy cycles, and serum PSA level before application of the first cycle.
Statistical Analysis
Statistical analyses were performed using SPSS software, version 27.0 (IBM). Descriptive data are presented as mean ± SD and range. Survival data are represented by Kaplan–Meier curves and analyzed via log-rank comparisons for univariate analysis and via Cox regression models for multivariate analysis. For comparison between 2 Cox models, the Gönen and Heller concordance probability estimate (20) was calculated using R software, version 4.0.3, with a probability of 0.5 indicating a random discrimination and 1 a perfect discrimination. A landmark analysis for OS was performed, starting with the time point of the final follow-up PSMA PET/CT study after RLT until death or last follow-up. OS is presented as median and 95% CI. The Cohen κ was used to assess interrater reliability (on the basis of Landis and Koch criteria (21)). For comparisons between subgroups in the volumetric analysis, a paired or unpaired t test was performed when indicated. A P value of less than 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
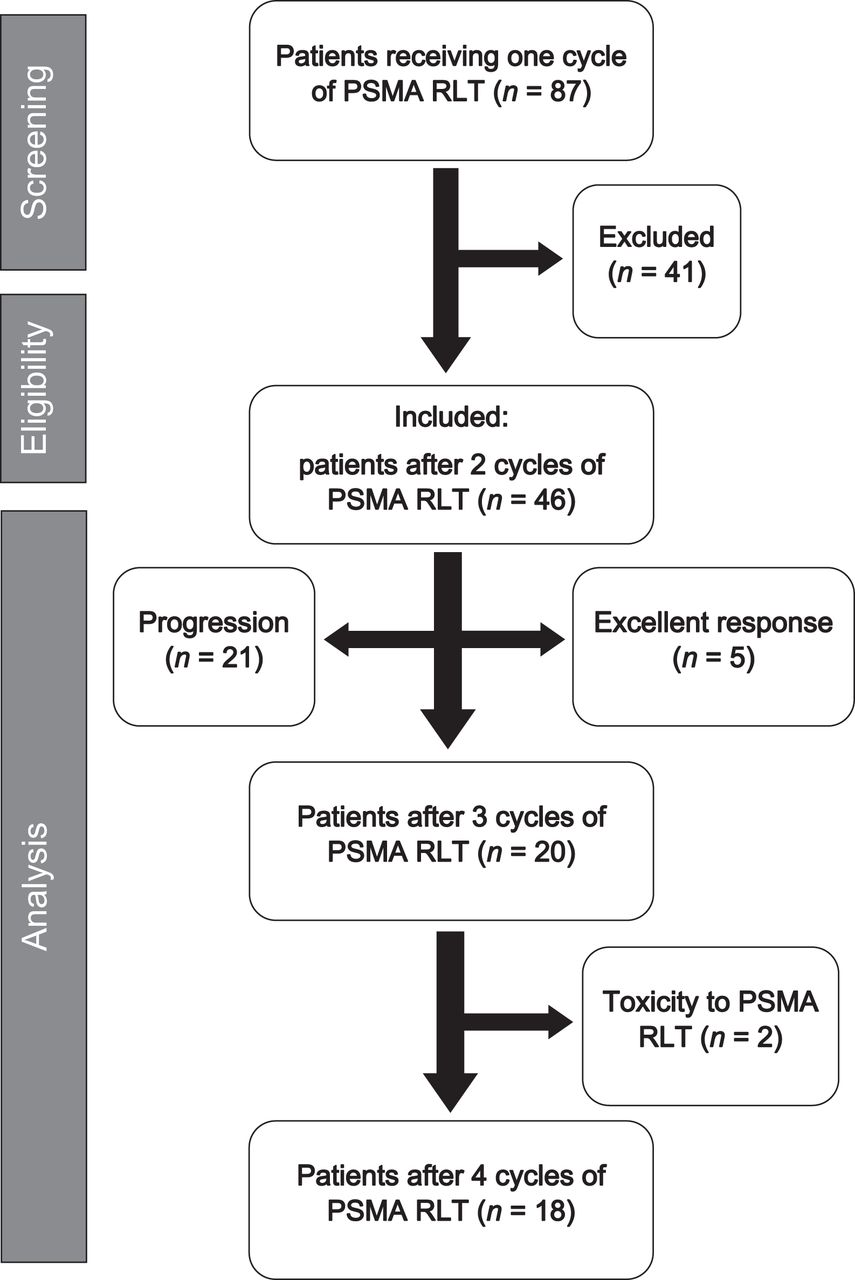
Of 87 patients receiving PSMA RLT, 46 were included in this analysis. Detailed characteristics are given in Table 2. In total, 129 cycles of RLT were administered, with a mean activity of 5.9 ± 0.7 GBq (range, 3.0–7.5 GBq). Eighteen patients received all 4 cycles of PSMA RLT. In 2 patients, PSMA RLT was limited to 3 cycles because of therapy-associated side effects (progression of preexisting renal insufficiency, xerostomia, and fatigue). In the remaining 26 patients, only 2 cycles of PSMA RLT were performed (Fig. 1), because of either a very good response (n = 5) or distinct progression (n = 21) as assessed by PSMA PET/CT and laboratory data (based on clinical decision). The intervals between initial PSMA PET/CT and the first cycle of PSMA RLT, and between the last cycle and restaging PSMA PET/CT, were 46 ± 26 d (range, 5–126 d) and 53 ± 12 d (range, 23–77 d), respectively. In 27 patients, RLT was monitored using 68Ga-PSMA-11 PET/CT, and 19 patients were examined with 18F-PSMA-1007 PET/CT.
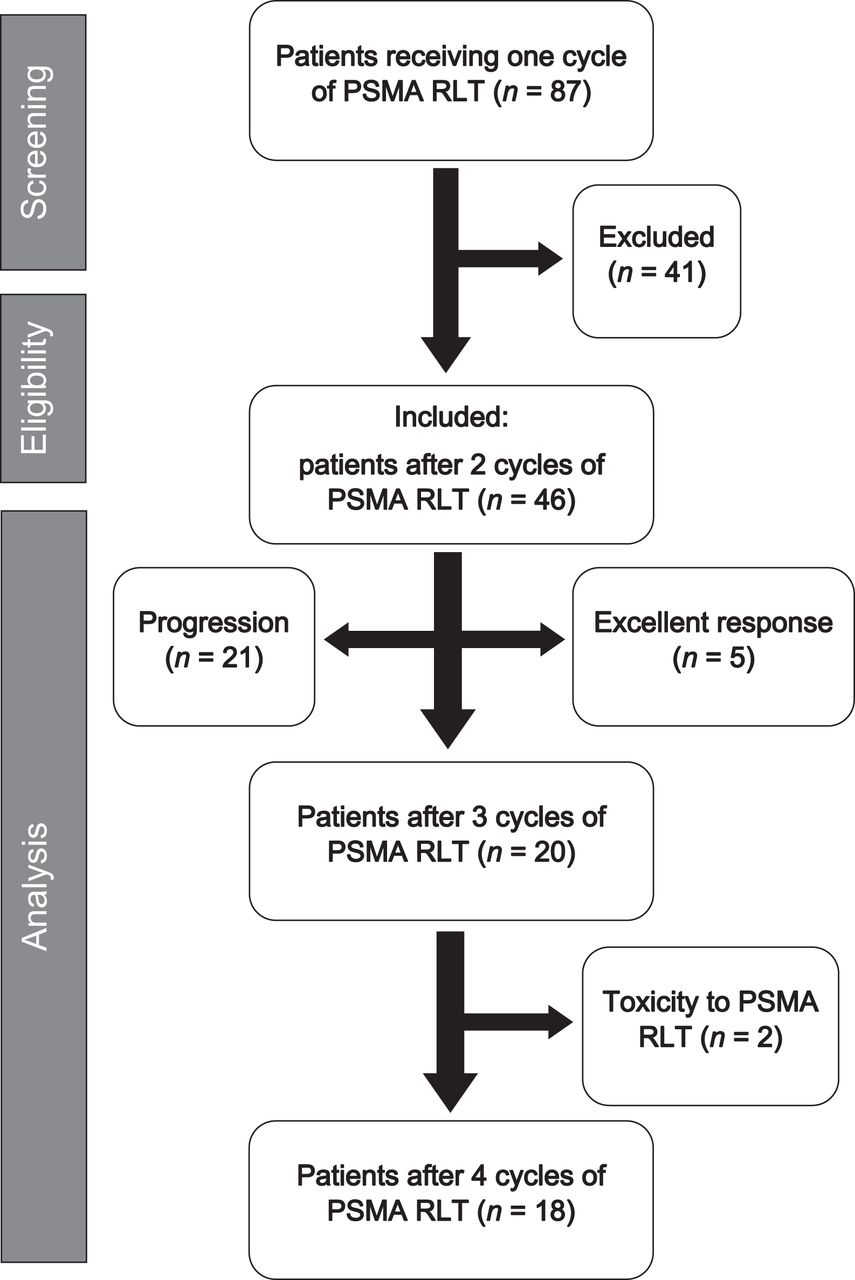
Flow diagram of patients included in this analysis undergoing PSMA RLT.
Patient Characteristics (n = 46)
Response Assessment
Response According to Modified PPP Criteria
According to the modified PPP criteria, 32 of 46 patients were considered progressive (70%). Of these patients, 21 had undergone 2 cycles of PSMA RLT, 2 had been treated with 3 cycles, and 9 had received 4 cycles. In most cases (27/32, 84%), progression was due to the appearance of 2 or more new metastases on PSMA PET (category A). In 4 patients, a distinct increase in tumor volume was seen in addition to a serum PSA level rising by at least 25% (category C), and in 1 patient a distinct increase in tumor volume was seen in addition to an alkaline phosphatase level rising by at least 25% (category C). Category B (1 new metastasis and rising laboratory values) did not occur in any patient. Interobserver agreement on categorization was substantial, as indicated by a Cohen κ of 0.73, with a concordance in 87% of patients. Examples for categories A and C are shown in Figure 2.

Maximum-intensity projections of 18F-PSMA-1007 PET scans of 2 patients with metastatic prostate cancer undergoing PSMA RLT. (A) A 75-y-old patient with disseminated bone metastases and multiple lymph node metastases before and after 4 cycles of PSMA RLT; restaging PET shows multiple new bone metastases (category A). (B) A 65-y-old patient with diffuse bone marrow involvement and multiple lymph node metastases before and after 2 cycles of PSMA RLT; restaging PET shows distinct increase in tumor volume (PSMATV50 increased by 50% in humerus, pelvis, and right femur), with corresponding 45% increase in serum alkaline phosphatase. In turn, serum PSA decreased by 52% (category C).
The volumetric assessment of the patients who were rated with category C (n = 5) or as nonprogressive (n = 14) showed a significant difference in the percentage change in PSMATV50 between the 2 groups (C: ΔPSMATV50, 96% ± 73% [range, 31%–200%], vs. nonprogressive: ΔPSMATV50, 51% ± 35% [range, −87%–16%]; P < 0.001). PSMATV50 decreased significantly in patients rated as nonprogressive (from 135.6 ± 172.1 mL to 81.2 ± 171.3 mL; P = 0.02), but no significant change in PSMATV50 was found in the 5 patients rated with category C (from 198.6 ± 271.5 mL to 325.3 ± 390.4 mL; P = 0.086).
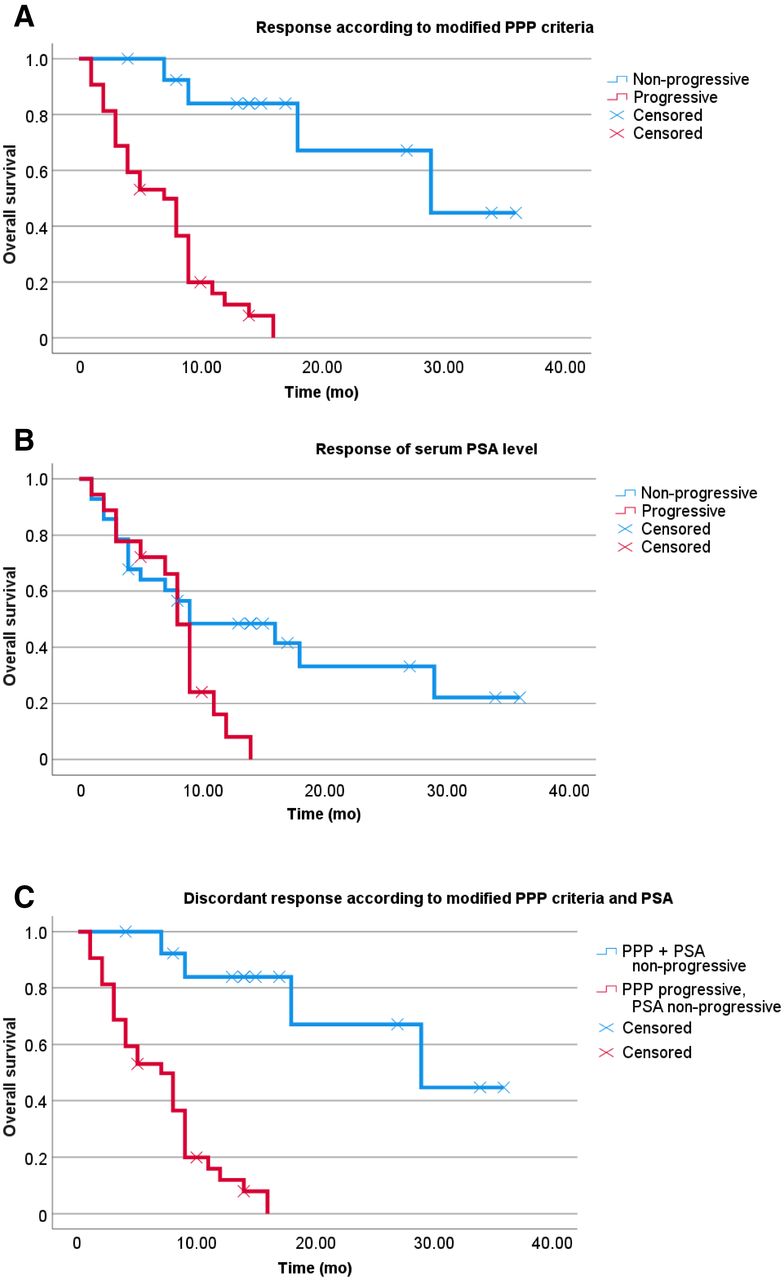
The median OS of all patients (n = 46) was 9.0 mo (95% CI, 7.8–10.2 mo). Patients with progression according to the modified PPP criteria (n = 32) had a median OS of 7.0 mo (95% CI, 4.0–10.0 mo) only. Those patients who were not progressive had a significantly longer median OS, at 29.0 mo (95% CI, 8.2–49.8 mo) (P ≤ 0.001; Fig. 3).
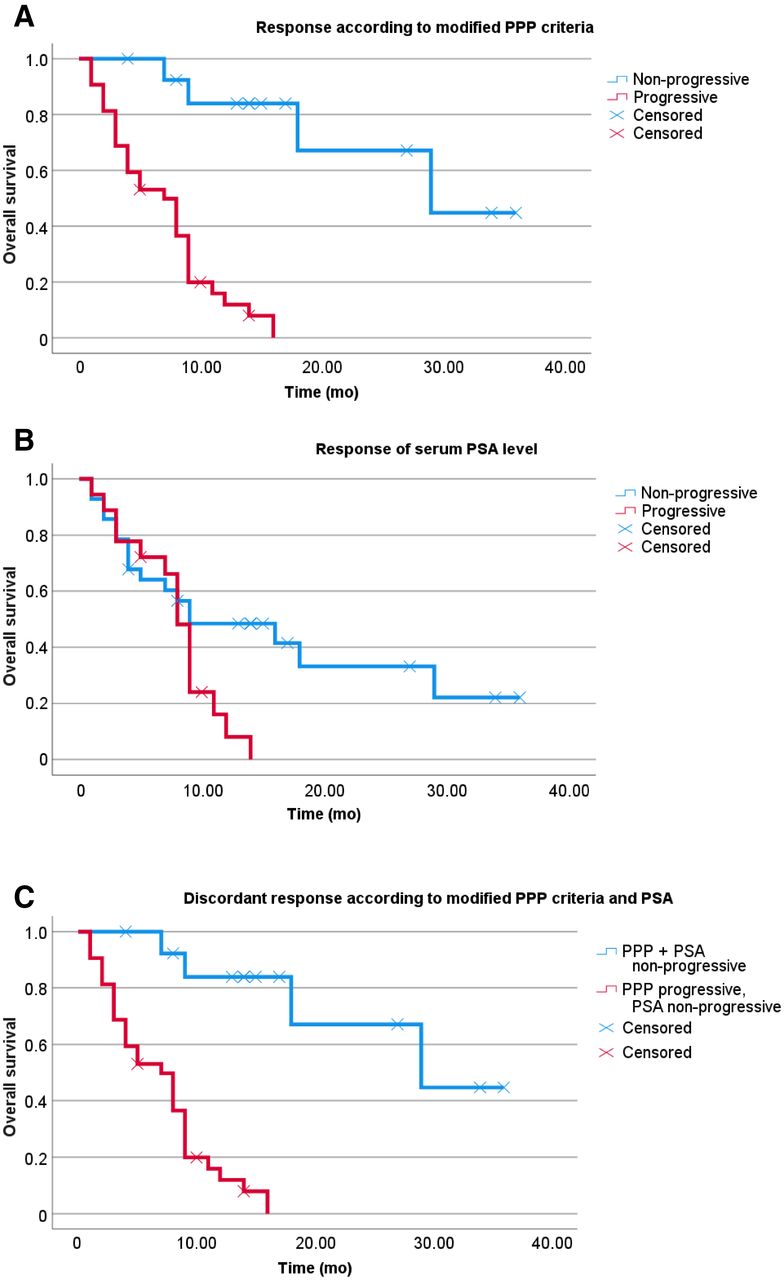
Kaplan–Meier curves of OS using log-rank comparison. (A) Patients with progression according to modified PPP criteria (n = 32) had short median OS of 7.0 mo (95% CI, 4.0–10.0 mo). Those patients who were not progressive (n = 14) had significantly longer OS, at 29.0 mo (95% CI, 8.2–49.8 mo) (P ≤ 0.001). (B) Patients with progression of serum PSA level (n = 18) had median OS of 8.0 mo (95% CI, 6.9–9.1 mo), compared with those patients with nonprogressive serum PSA level (n = 28), with OS of 9.0 mo (95% CI, 0–19.1 mo) (P = 0.046). (C) Patients rated as category A (modified PPP criteria) but with nonprogressive PSA value (n = 13) had significantly shorter median OS of 11.0 mo (95% CI, 8.2–13.8 mo) than patients with nonprogressive serum PSA level and corresponding response according to modified PPP criteria (n = 15, median OS was not reached at end of follow-up period; P ≤ 0.001).
Response of Serum PSA Level
Progression of the serum PSA level at the time of the final PET/CT examination was found in 18 of 46 patients (39%). Of these patients, 14 had been treated with 2 cycles of PSMA RLT and 4 with 4 cycles. These patients (n = 18) had a median OS of 8.0 mo (95% CI, 6.9–9.1 mo), compared with those patients (n = 28) with a nonprogressive serum PSA level, who had a median OS of 9.0 mo (95% CI, 0–19.1 mo) (P = 0.046; Fig. 3).
Comparison of Biochemical and Imaging Findings
Thirteen patients who were rated as category A did not show a progression of serum PSA level. The mean relative change in serum PSA in these patients was −33% ± 24% (−69%–5%). These patients had a significantly shorter median OS of 11.0 mo (95% CI, 8.2–13.8 mo) than did those with a nonprogressive serum PSA level (n = 15, median OS was not reached at the end of the follow-up period; P ≤ 0.001). Conversely, all patients with a progressive serum PSA also showed a progression on PSMA PET/CT (category A or C).
After PSMA RLT, 8 patients presented with new visceral sites of disease. Of these, 2 patients presented with new liver metastases, which were visible only on CT (apart from many progressive PSMA-positive bone and lymph node metastases). The other new visceral metastases were concordantly detectable on PET and CT (a detailed comparison of biochemical and imaging findings can be found in Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
In a multivariate analysis, progression according to the modified PPP criteria remained a significant prognostic marker (P ≤ 0.001), with a hazard ratio of 15.5 (95% CI, 3.4–70.2), in contrast to the response of serum PSA level, which was not significant after stratification (P = 0.12). The modified PPP criteria showed a better discriminatory power, with a concordance probability estimate of 0.76, compared with the response of PSA, with a concordance probability estimate of 0.66.
DISCUSSION
In our patient cohort, the median OS of all patients (n = 46) was 9.0 mo, which at first appears to be shorter than the OS reported in other published retrospective studies (11.0 mo) (22) and prospective studies (13.3 mo) (23) of patients receiving PSMA RLT. However, this discrepancy is not surprising, as we performed a landmark analysis starting with the follow-up PSMA PET/CT and not with the administration of the first cycle of therapy in order to assess the association of posttherapy PPP criteria and further patient survival. The binary categorization of patients into progressive and nonprogressive by modified PPP criteria was superior to the binary categorization of serum PSA level as judged by Gönen and Heller’s concordance probability estimate (20). This result was probably due to the 13 of 46 patients who had a nonprogressive serum PSA level but showed 2 or more new lesions on PSMA PET/CT (i.e., category A), which was associated with a significantly reduced median OS of 11.0 mo compared with patients with a corresponding biochemical and imaging response. In this respect, discrepant developments in PSA and PSMA PET have previously been observed after PSMA RLT (24) and might indicate the loss of adequate PSA expression and the transition to a more aggressive stage of disease (25). Moreover, none of the patients was in category B (1 new metastasis and rising laboratory values), probably because of the advanced disease stage of the patients with disseminated metastases or even diffuse bone marrow involvement.
A possible pitfall of PPP criteria is their assumption of a persistent PSMA expression throughout the course of disease. Neuroendocrine dedifferentiation and progression with a loss of PSMA expression (26) (which is more likely to occur in an advanced disease stage) are not defined, and progression without a finding on PSMA PET or CT is not included in the PPP criteria. In our patient cohort, 2 patients presented with new liver metastases after PSMA RLT, and these could be detected solely on CT. Unfortunately, CT-based criteria in advanced prostate cancer are known to be of limited value (7,8), especially since diffuse sclerotic bone lesions are difficult to measure and to quantify (27). In this sense, it is imaginable that the additional use of 18F-FDG PET might help to detect more aggressive tumor manifestations (28,29). Discordant 18F-FDG–positive but PSMA-negative lesions are a known negative prognostic marker before initiation of PSMA RLT (30). Neuroendocrine biomarkers have been shown not to be prognostic for OS before PSMA RLT (31). However, a distinctly elevated or rising neuron-specific enolase level during the course of PSMA RLT is reported to be associated with discordant 18F-FDG–positive lesions (32). If this association can be confirmed and a prognostic relation can be found for both parameters, neuron-specific enolase level might be implemented into PPP criteria to be evaluated even in the case of a nonprogressive PSMA PET/CT scan.
Because this analysis was retrospective, there were some limitations, which resulted in modified PPP criteria without confirmatory biopsy or correlative imaging within 3 mo. However, this situation affected only 11% (5/46) of the included patients, who were rated as category C, and is more likely in clinical routine. Second, in contrast to published PPP criteria, our evaluation was done primarily visually, as our analysis included PSMA PET scans with 2 different tracers (68Ga-PSMA-11 and 18F-PSMA-1007), and no validated quantification assessment of the whole-body tumor burden on 18F-PSMA-1007 PET/CT exists so far. In particular, a liver-based threshold as proposed for 68Ga-PSMA-11 PET (12) cannot be directly adapted to 18F-PSMA-1007 PET because of the hepatobiliary excretion of 18F-PSMA-1007 (33). However applying the recently proposed quantification of whole-body tumor burden on 68Ga-PSMA-11 PET/CT using PSMATV50 (14), we found a significant difference in the percentage change in PSMATV50 between patients rated as category C and those who did not show progression on PSMA PET/CT. Further research evaluating PSMATV50 in larger patient cohorts with 18F-PSMA-1007 PET scans might help to implement this approach into PPP criteria. Third, although the patients included in this study were not treated with the same number of therapy cycles, it must be emphasized that the aim of this analysis was to evaluate not the effectiveness of PSMA RLT but the assessment of progression using modified PPP criteria. Therefore, the number of therapy cycles was part of the multivariate analysis, with modified PPP criteria also showing a significant impact on OS after stratification, despite the admitted limitation of a rather small patient population. Fourth, an important limitation of modified PPP criteria is that they cannot be used in clinical trials for assessing radiographic-progression–free survival, as they also contain laboratory data. Fifth, even though the authors of the PPP criteria mentioned that a correlation between PPP assessment and OS might be of limited value because of the bias of further treatments (16), it has to be acknowledged that PSMA RLT often represents the last line of treatment, with restricted further therapeutic options. Thus, in our opinion there is no or only a little bias to our observation that PPP assessment accurately reflects response to PSMA RLT. Finally, a prospective validation of the present modified PPP scheme is warranted.
CONCLUSION
Response assessment in patients undergoing PSMA RLT using modified PPP criteria is reproducible and highly prognostic for OS. Modified PPP criteria should be validated in future prospective trials.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the feasibility of using PPP criteria in patients undergoing PSMA RLT, and what are the prognostic implications of these criteria?
PERTINENT FINDINGS: In this retrospective analysis, PSMA PET/CT scans of 46 patients before and after completion of PSMA RLT were analyzed separately by 2 readers using modified PPP criteria. Progression according to the modified PPP criteria was found in 32 patients and was a significant (P ≤ 0.001) prognostic marker for OS, with a hazard ratio of 15.5 (95% CI, 3.4–70.2).
IMPLICATIONS FOR PATIENT CARE: Response assessment in patients undergoing PSMA RLT using modified PPP criteria is reproducible and highly prognostic for OS.
Footnotes
Published online March 31, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 24, 2020.
- Revision received March 18, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Role of PSMA PET Parameters as Biomarkers for Response to PSMA-Targeted Radiopharmaceutical Therapy
- Assessing Response to PSMA Radiopharmaceutical Therapies with Single SPECT Imaging at 24 Hours After Injection
- PSMA PET/CT for Response Assessment and Overall Survival Prediction in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Androgen Receptor Pathway Inhibitors
- Prognostic Value of End-of-Treatment PSMA PET/CT in Patients Treated with 177Lu-PSMA Radioligand Therapy: A Retrospective, Single-Center Analysis
- 68Ga-PSMA PET/CT for Response Evaluation of 223Ra Treatment in Metastatic Prostate Cancer
- Prognostic Value of Tumor Volume Assessment on PSMA PET After 177Lu-PSMA Radioligand Therapy Evaluated by PSMA PET/CT Consensus Statement and RECIP 1.0
- A Single-Arm, Low-Dose, Prospective Study of 177Lu-EB-PSMA Radioligand Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer