


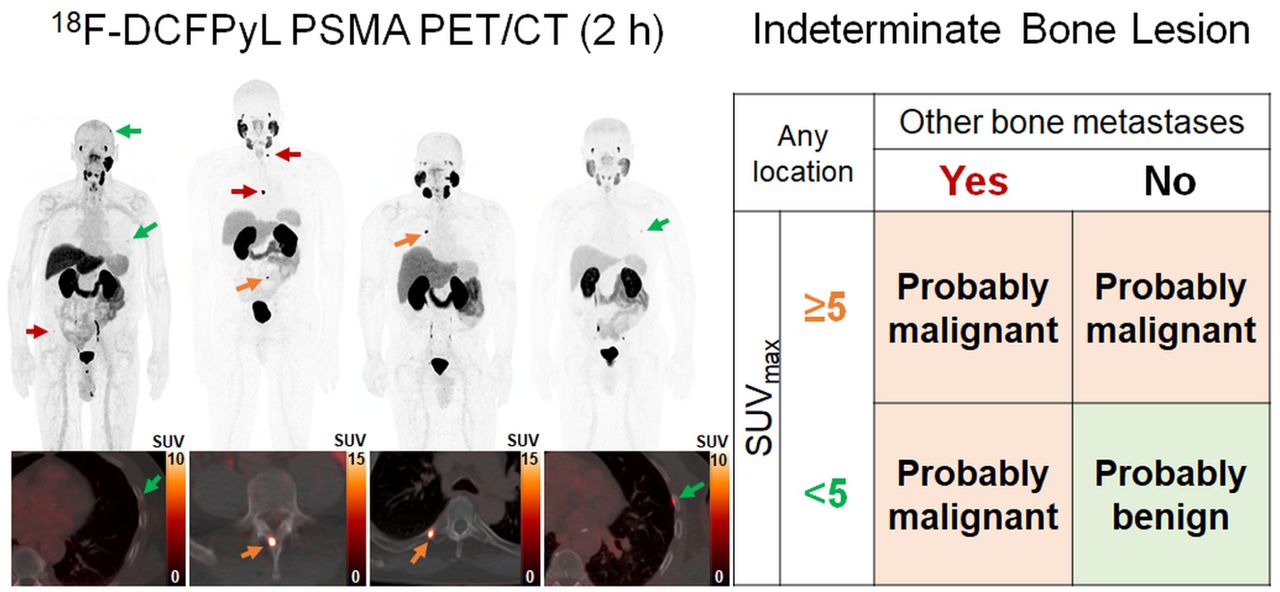
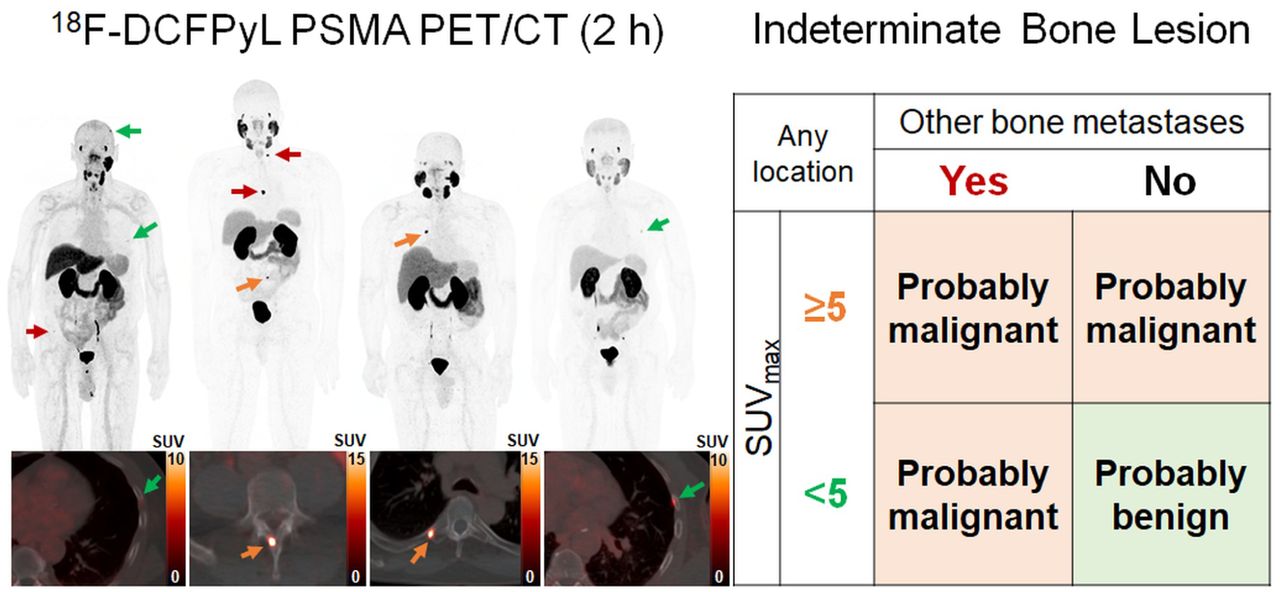
Visual Abstract
Abstract
Indeterminate bone lesions (IBLs) on prostate-specific membrane antigen (PSMA) PET/CT are common. This study aimed to define variables that predict whether such lesions are likely malignant or benign using features on PSMA PET/CT. Methods: 18F-DCFPyL PET/CT imaging was performed on 243 consecutive patients with high-risk primary or biochemically recurrent prostate cancer. IBLs identified on PSMA PET/CT could not definitively be interpreted as benign or malignant. Medical records of patients with IBLs were reviewed to determine the ultimate status of each lesion. IBLs were deemed malignant or benign on the basis of evidence of progression or stability at follow-up, respectively, or by biopsy results; IBLs were deemed equivocal when insufficient or unclear evidence existed. Post hoc patient, lesion, and scan variables accounting for clustered data were evaluated using Wilcoxon rank-sum and χ2 tests to determine features that favored benign or malignant interpretation. Results: Overall, 98 IBLs within 267 bone lesions (36.7%) were identified in 48 of 243 patients (19.8%). Thirty-seven of 98 IBLs were deemed benign, and 42 were deemed malignant, of which 8 had histologic verification; 19 remained equivocal. Location and SUVmax categorical variables were predictive of IBL interpretation (P = 0.0201 and P = 0.0230, respectively). For IBLs with new interpretations, 34 of 37 (91.9%) considered benign showed an SUVmax of less than 5 or exhibited focal uptake without coexisting bone metastases; 37 of 42 (88.1%) deemed malignant demonstrated an SUVmax of at least 5 or were present with coexisting bone metastases. Logistic regression predicted IBLs with a high SUVmax (univariable: odds ratio [OR], 9.29 [P = 0.0016]; multivariable: OR, 13.87 [P = 0.0089]) or present with other bone metastases (univariable: OR, 9.87 [P = 0.0112]; multivariable: OR, 11.35 [P = 0.003]) to be malignant. Conclusion: IBLs on PSMA PET/CT are concerning; however, characterizing their location, SUV, and additional scan findings can aid interpretation. IBLs displaying an SUVmax of at least 5 or present with other bone metastases favor malignancy. IBLs without accompanying bone metastases that exhibit an SUVmax of less than 5 and are observed only in atypical locations favor benign processes. These guidelines may assist in the interpretation of IBLs on PSMA PET/CT.
Prostate-specific membrane antigen (PSMA) PET/CT is a highly sensitive and specific diagnostic tool enabling early detection of primary and metastatic prostate cancer (PCa) (1). PSMA overexpression is observed in nearly 95% of all cases of primary PCa, and PSMA expression on histology correlates with tumor aggressiveness (2). The recent Food and Drug Administration approval of 18F-DCFPyL has increased the use of PSMA PET/CT in staging and in suspected early metastatic involvement of patients with high-risk PCa and biochemically recurrent (BCR) PCa (3). However, 18F-DCFPyL and other PSMA PET tracers commonly demonstrate nonspecific and indeterminate PSMA uptake in soft tissue or bones with unclear or no anatomic correlation on CT (4–6). To interpret lesions with PSMA uptake, several PSMA PET/CT reporting systems, including the European Association of Nuclear Medicine standardized reporting criteria (E-PSMA), the PSMA Reporting and Data System (PSMA-RADS), and the Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE), were developed with structured categories for lesions that are benign, likely benign, indeterminate or equivocal, likely malignant, and malignant (7–9). Lesion classification is based on location, size, SUVmax, relative uptake compared with expected physiologic uptake, number of lesions with PSMA uptake, and scan-based regional distribution (7); however, lesions classified as indeterminate require follow-up for definitive assessment. Since metastatic PCa commonly involves bones, PSMA uptake in indeterminate bone lesions (IBLs) that are benign processes, such as fibrous dysplasia, Paget disease, and hemangiomas, can easily be mistaken for bone metastases and lead to inappropriate changes in patient management (10–14). On the other hand, IBLs interpreted as benign when they are true metastases may delay necessary treatment. Recent PSMA PET/CT imaging studies using 18F-PSMA-1007 (5,15,16), 68Ga-PSMA-11 (6,16–18), and 18F-DCFPyL (4) tracers have investigated indeterminate PSMA-avid uptake in soft-tissue and bone lesions. Although these studies associate certain imaging features with IBLs that are usually benign—specifically, a single IBL located in the rib with subtle PSMA uptake and no additional metastases—there lacks consensus regarding features that predict which IBLs are likely malignant. In this study, we defined features of 18F-DCFPyL PET/CT that predict IBLs as benign or malignant.
MATERIALS AND METHODS
Patient Population
Between July 2017 and October 2021, 18F-DCFPyL PET/CT imaging was performed on 243 consecutive patients with histologically confirmed high-risk PCa or BCR PCa without prior evidence of metastatic disease. All patients gave written informed consent before participating in a prospective clinical trial (NCT03181867). In a post hoc subanalysis, patients included in this study had at least 1 IBL in the presence or absence of other soft-tissue or bone lesions suggestive of metastatic PCa on 18F-DCFPyL PET/CT. Patients without an IBL were excluded.
18F-DCFPyL PET/CT Imaging
18F-DCFPyL was synthesized under good manufacturing practices as previously described (19). Patients received an intravenous injection of 18F-DCFPyL (mean, 262.7 ± 37.9 MBq [7.10 ± 1.02 mCi]; range, 167.6–317.8 MBq [4.53–8.59 mCi]) and underwent whole-body PET/CT after a 2-h uptake period (3 min/bed position) using a 3-dimensional time-of-flight Discovery MI DR scanner (GE Healthcare) with a 20-cm coronal and a 70-cm axial field of view. Image reconstruction applied an attenuation-corrected 3-dimensional iterative maximum-likelihood expectation-maximization algorithm using 29 subsets, 3 iterations, time-of-flight, a point spread function regularization parameter of 6.0, and a gaussian postprocessing filter with a 4.1-cm kernel. A low-dose unenhanced CT scan (120 kV, 60 mAs) was acquired with each PET scan for attenuation correction and anatomic coregistration.
Assessment of PSMA-Avid IBLs
18F-DCFPyL PET/CT images were prospectively interpreted by 2 expert nuclear medicine physicians (both with 5 y of experience reading PSMA PET/CT images). Scans of patients with at least 1 PSMA-avid IBL, defined as focal radiotracer uptake in bone without correlative sclerotic or lytic features on CT, or not clearly benign—equivalent to the definition of the PSMA-RADS-3B category (9)—were further analyzed. Two different readers retrospectively reviewed each IBL using medical records until January 2022, including other pre-PSMA and post-PSMA follow-up imaging, therapeutic interventions, and laboratory or biopsy-based pathology, to provide an updated interpretation as benign, malignant, or equivocal based on the following criteria.
Benign findings were, first, no evidence of progression (i.e., a stable lesion without morphologic changes) between pre-PSMA and PSMA imaging for patients without follow-up or between pre-PSMA and post-PSMA imaging for patients with follow-up; second, PCa-negative biopsy findings for the lesion; or third, stable lesion uptake before therapeutic intervention at follow-up 18F-DCFPyL PET/CT.
Malignant findings were, first, evidence of progression (i.e., new lesions, sclerotic changes, or lytic changes) between pre-PSMA and PSMA imaging for patients without follow-up or between pre-PSMA and post-PSMA imaging for patients with follow-up; second, PCa-positive biopsy findings for the lesion; or third, evidence of lesion regression after therapeutic intervention based on a significantly reduced SUVmax at follow-up 18F-DCFPyL PET/CT imaging.
Equivocal findings were insufficient evidence for either a benign or a malignant interpretation due to a short follow-up duration or unclear imaging features.
Statistical Analysis
The association of IBL characteristics with an updated interpretation was evaluated using the Wilcoxon rank-sum test for clustered data (20) in continuous variables and the χ2 test for clustered data (21) in categorical variables to account for multiple lesions sampled per patient. The characteristics evaluated included SUVmax, anatomic location; CT features (including no CT abnormality in bone sclerotic, lytic, and mixed sclerotic and lytic bone morphologies; and the presence or absence of other suggestive findings on PSMA imaging (including lymph node or bone uptake). Tests were repeated considering distribution of benign versus malignant lesion assignments as well as benign versus malignant versus equivocal categorizations. Logistic regression analysis, using weighted generalized estimation equations with working independence correlation structure to account for the correlation of multiple lesions per patient, was performed to evaluate the association of IBL characteristics with a malignant interpretation. Lesions with an equivocal clinical or pathologic interpretation were excluded from logistic regression analysis. Weights were calculated as 100 × (1/Np), where Np is the number of lesions sampled per patient. P values of less than 0.05 were considered significant for all statistical analyses. Receiver-operating-characteristic curve and Youden index ([sensitivity + specificity − 1]) analyses were evaluated for the SUVmax of IBLs to be interpreted as benign or malignant. The SUVmax threshold with the highest sensitivity and lowest false positive rate was selected to differentiate lesions likely to be malignant.
RESULTS
Incidence and Interpretation of IBLs
Overall, 98 IBLs within 267 total bone lesions (36.7%) were identified in 48 of 243 patients (19.8%). Patient characteristics are shown in Table 1, and patient selection criteria with lesion-level follow-up and IBL interpretation based on review are shown in Figure 1. Median patient follow-up was 7.5 mo (range, 0.0–54.0 mo); median lesion follow-up was 4.8 mo (range, 1.1–54.0 mo) in patients with post-PSMA follow-up and 9.1 mo (range, 0.0–54.0 mo) in patients with prior imaging only. Detailed patient follow-up information was used to interpret each IBL as benign, malignant, or equivocal (Supplemental Fig. 1; Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
Clinical Characteristics of Patients with IBLs

Flowchart of patient selection criteria and lesion-level follow-up for patients with at least 1 IBL. Interpretations (benign, malignant, or equivocal) are shown for IBLs with no follow-up (prior imaging) and follow-up (imaging or biopsy).
The 98 IBLs had a median SUVmax of 3.6 (interquartile range, 2.3–9.8) and were identified in the pelvis (28.6%), spine (21.4%), ribs (39.8%), or other atypical locations including the scapula, clavicle, skull, sternum, and extremities (10.2%). Only 8 of 98 (8.2%) IBLs had biopsy confirmation—3 were malignant (metastatic prostate adenocarcinoma) and 5 were benign (Table 2). At the lesion level, 42 of 98 (42.9%) IBLs were considered malignant, 37 (37.7%) were benign, and 19 (19.4%) remained equivocal. Most IBLs were assessed as equivocal (18/19, 94.7%) because of short follow-up (<7 mo). At the patient-level, 11 of 48 (22.9%) had a malignant IBL, 24 (50.0%) had a benign IBL, and 13 (27.1%) had equivocal findings; 1 patient with multiple IBLs had mixed determinations. Examples are given of patients with IBLs on 18F-DCFPyL PET/CT which demonstrate benign (Figs. 2 and 3) or malignant (Fig. 4; Supplemental Fig. 2) characteristics based on their location, SUVmax, and CT morphology. PSMA PET/CT features in the pelvis (Fig. 3) and spine (Fig. 4) can show similarity but have different interpretations; thus, additional follow-up may assist with assessment.
Histopathologic Assessment of IBL Biopsy Specimens

A 63-y-old patient with BCR PCa and PSA of 0.46 ng/mL. Axial 18F-DCFPyL PET (left), 18F-DCFPyL PET/CT (middle), and CT (right) images show a single area of subtle PSMA-avid uptake with SUVmax of 2.4 in the right fifth rib and no CT correlate (arrows). This IBL was determined to be benign based on negative 17-mo follow-up bone scintigraphy findings.

A 60-y-old patient with BCR PCa and PSA of 3.9 ng/mL. Axial 18F-DCFPyL PET (left), 18F-DCFPyL PET/CT (middle), and CT (right) images show a single area of subtle PSMA-avid uptake with SUVmax of 3.9 in left iliac bone and mixed sclerotic and lytic CT features (arrows). This IBL was stable for 4 mo and negative on 4 other staging modalities; thus, the IBL was interpreted as benign.

A 73-y-old patient with BCR PCa and PSA of 4.9 ng/mL. Axial 18F-DCFPyL PET (A), 18F-DCFPyL PET/CT (B), CT (C), pre-PSMA MRI (D), and follow-up MRI (E) images show a single area of subtle PSMA-avid uptake with SUVmax of 3.3 in left T8 lamina and subtle sclerotic CT features (arrows). This IBL became more prominent and enhanced over a 3-y period between retrospective MRI (D) and follow-up MRI (E) and was determined to be malignant.
Imaging Features of IBLs That Predict for Malignancy or Benignancy
Two lesion-based categorical variables were predictors for malignancy or benignancy: lesion location (P = 0.0201)—categorized as spine, pelvis, ribs, and other regions (e.g., skull, sternum, and scapula)—and lesion SUVmax (P = 0.0230)—categorized as less than 5 versus 5 or more (Table 3). No other 18F-DCFPyL PET/CT–based continuous and categorical variables were predictive (Supplemental Table 2). Logistic regression analysis for benign versus malignant findings (n = 79) revealed that a high SUVmax (univariable: odds radio [OR], 9.29 [95% CI, 3.19–24.75; P = 0.0016]; multivariable: OR, 13.87 [95% CI, 1.91–100.9; P = 0.0089]) and the presence of additional bone metastases on the PSMA PET/CT scan (univariable: OR, 9.87 [95% CI, 2.00–48.82; P = 0.0112]; multivariable: OR, 11.35 [95% CI, 3.05–42.25; P = 0.0030]) were associated with malignancy (Table 4). Selection of an SUVmax threshold of at least 5 was based on receiver-operating-characteristic curve and Youden index analyses that maximized the sensitivity (71.4%, 30/42) for predicting IBLs as malignant with the fewest false positives (2.7%, 1/37) (Supplemental Fig. 3). Although this SUVmax threshold missed 12 of 42 (28.6%) IBLs with an SUVmax of less than 5 that were deemed malignant, 7 of these 12 IBLs were identified in the presence of other bone metastases. Therefore, a model incorporating all 3 18F-DCFPyL PET/CT imaging variables that predicted for malignancy or benignancy (n = 79) was developed to assess the likelihood that an IBL would be benign or malignant based on a single PSMA PET/CT scan (Fig. 5). Overall, 89.9% of the model’s predictions agreed with our assessment, but 10.1% disagreed, including 5 false negatives and 3 false positives (Table 5). Although our model suggests that a single IBL located in the pelvis or spine with an SUVmax of less than 5 is probably benign, these are common sites for PCa bone metastases and represented a greater number of false negatives, such as the example in Figure 4. Ultimately, the relationship of these predictive variables may improve IBL interpretation on PSMA PET/CT scans (Fig. 6).
18F-DCFPyL PSMA PET/CT-Based Variables That Predict IBL Interpretation (n = 98)
Logistic Regression Analysis Showing OR at 95% CI for Clinically Relevant 18F-DCFPyL PET/CT-Based Features That Predict IBLs as Benign vs. Malignant (n = 79)

Model assessing the likelihood that an IBL is benign or malignant based on 18F-DCFPyL PET/CT imaging variables that predicted for benignancy or malignancy (n = 79).
Model Predicting the Likelihood That IBLs Identified on 18F-DCFPyL PET/CT at 2 Hour of Uptake Are Benign or Malignant (n = 79)

Sankey diagram showing the relationship of multiple predictive 18F-DCFPyL features (n = 98). Specifically, lesion location, lesion SUVmax, and type of bone findings on a PSMA PET/CT scan are more likely associated with a particular lesion interpretation (right). Pathways with 1 lesion have been removed for clarity.
DISCUSSION
PSMA PET/CT can impact management decisions in patients with high-risk primary and BCR PCa, and multiple studies have demonstrated that up to 68% of predetermined interventions can change after PSMA PET/CT (22,23). Although the PSMA-RADS, PROMISE, and E-PSMA structured PSMA PET/CT reporting systems have improved lesion classification and interpretation based on particular imaging features, several lesions with PSMA uptake categorized as indeterminate or equivocal have been shown to be false positives (11–13) whereas some have been shown to be true positives at follow-up (4,18). A particular issue with PSMA PET/CT is the incidence of indeterminate lesions with mild focal uptake in bone and unclear or negative anatomic features; currently, these lesions require biopsy or follow-up imaging for definitive assessment. Interpreting such lesions as metastatic without sufficient evidence can have far-reaching implications for patients and lead to unnecessary interventions that alter a patient’s quality of life. Understanding specific features that increase the certainty of interpreting IBLs as probably benign or probably malignant is, therefore, of great clinical importance.
Our study demonstrated that 3 PSMA PET/CT–based features predict IBL interpretation: the presence or absence of other bone metastases on the scan, IBL SUVmax, and IBL location. Prior studies investigating IBLs using a variety of PSMA PET tracers have mentioned that these particular features may predict interpretation or are important. Specifically, a follow-up 18F-PSMA-1007 PET/CT study by Arnfield et al. monitoring 159 IBLs for more than 12 mo in 77 patients suggested that IBLs were likely benign when showing an SUVmax of less than 7.2 in the absence of other definite bone metastases (15). In contrast, a multicenter 18F-PSMA-1007 PET/CT study analyzing 351 IBLs with an SUVmax of less than 10 determined that SUVmax did not predict interpretation (5). Moreover, a follow-up 68Ga-PSMA-11 PET/CT study by Chen et al. reported that 61 of 62 patients with primary PCa and a single rib IBL with a mean SUVmax of 3.0 were benign; however, 1 lesion showing an SUVmax of 2.2 later proved to be a metastasis (18). Lastly, a 18F-DCFPyL PET/CT longitudinal follow-up study found that 3 of 14 IBLs showed changes indicative of malignancy (4). These prior studies collectively demonstrate that a single IBL in an atypical location in the absence of metastases is meaningful for predicting IBLs as benign but that SUVmax is not reliable. In addition, our findings agree with previous studies that no patient variables (including age, primary PCa, Gleason grade group, TNM stage, and serum prostate-specific antigen [PSA]) predict IBL interpretation.
There are some similarities between these prior studies and our findings regarding which IBLs favor benign outcomes; however, we expand on the current understanding of imaging features that predict IBLs for malignancy. First, we suggest that IBLs are likely malignant in the presence of other bone metastases, independent of SUVmax and location, but not necessarily with accompanying soft-tissue metastases. In our cohort, 7 of 48 patients with an IBL had no more than 3 other bone metastases, of which 3 of 7 also had lymph node involvement and 4 of 7 had no PSMA-avid lymph nodes. On the basis of our predictive model, 3 of the 4 patients with no PSMA-avid lymph nodes could be classified as oligometastatic and might have had the option to undergo local PCa interventions. Second, IBLs with an SUVmax of at least 5 after 2 h of 18F-DCFPyL uptake increased the likelihood of malignancy. Of the 34 IBLs showing an SUVmax of at least 5, 30 of 34 (88.2%) were deemed malignant, and only 1 of 34 (2.9%) was a false positive lesion deemed benign whereas 3 of 34 (8.8%) were equivocal because of insufficient evidence. However, IBLs with an increased SUVmax can result from inflammatory events such as trauma or hemangiomas (13), as well as from benign bone remodeling processes such as fibrous dysplasia (10) or Paget disease (24). Although the SUVmax threshold of at least 5 after 2 h of uptake was feasible to classify 88.2% of IBLs as malignant for our cohort, this SUVmax threshold requires validation in separate cohorts receiving 18F-DCFPyL PET/CT. Third, IBLs in typical locations were more commonly malignant based on follow-up review, but the association of lesion location with SUVmax and other PSMA scan bone findings, particularly whether lesions are solitary, multifocal, or present with other bone metastases, can improve assessment as displayed in Figures 5 and 6.
Although these predictors can guide interpretation, follow-up imaging may be necessary when insufficient evidence is available or conflicting imaging features are present on other studies. In this scenario, equivocal interpretation avoids misdiagnosis, and follow-up imaging can assist with assessment. Of the 19 of 98 (19.4%) IBLs that remained equivocal in our study, 16 had no available post-PSMA follow-up records, 2 had short follow-up (<3 mo), and 1 had sufficient follow-up (12 mo) but CT changes were not clear enough for a definitive interpretation. Overall, most IBLs that were determined to be equivocal (14/19, 74%) showed an SUVmax of less than 5 and were located in the ribs without other bone metastases.
IBLs showing subtle PSMA uptake only outside the pelvis or spine in the absence of definite bone metastases are likely benign; however, malignancy is always possible. For example, in the 68Ga-PSMA-11 PET/CT study mentioned earlier, 1 of 62 (1.6%) single rib IBLs with an SUVmax of 2.2 in the absence of other metastases demonstrated evidence of malignancy on follow-up imaging (18). In our study, only 1 of 42 (2.3%) IBLs was a single atypical lesion in the scapula that had a subtle SUVmax of 1.0 and no coexisting metastases but that nonetheless showed sclerotic progression consistent with malignancy. Considering common PSMA pitfalls, the SUVmax threshold of at least 5 minimized false positives in our study. However, among PET imaging protocols that use different uptake times or different PSMA tracers, there may be significant variation in SUVmax measurements, such as a higher lesion uptake on delayed scans (19) or a higher SUVmax for 18F-PSMA-1007 versus 68Ga-PSMA-11 (17). For instance, a recent 18F-PSMA-1007 PET–guided biopsy study after 1.5 h of uptake demonstrated that 10 of 11 IBLs with a mean SUVmax of 12.5 (range, 5.1–26.0) were benign, indicating that several lesions were not clinically concerning despite exceeding a prior proposed SUVmax threshold of 7.2–11.1 after 2 h of uptake (15,25). Thus, standardized imaging protocols for each class of PSMA tracer are necessary before SUVmax can reliably serve as a predictor of risk of malignancy. Ultimately, pairing detailed patient history with these predictive imaging features may increase the predictive value of IBL categorization among different PSMA agents and scanning conditions.
Our study had 3 main limitations. First, the follow-up time for our patients was short (mean, 7.5 mo; range, 0.0–54.0 mo); thus, nearly 20% of the IBLs remained equivocal because of insufficient evidence. Second, only a minority of IBLs were biopsied (8%, 8/98) since biopsy was not always safe to obtain or accepted by patients; however, all biopsy results supported our predictive model. Despite careful analysis of imaging and clinical findings, the lack of pathology confirmation may misrepresent the true nature of some IBLs deemed benign or malignant. Third, our results are limited to one type of PSMA-targeted PET tracer, 18F-DCFPyL, after 2 h of uptake, and quantitative SUVmax PET findings may not apply to other tracers scanned under different conditions. However, other variables such as location and additional bone findings may still be relevant with other tracers.
CONCLUSION
IBLs on PSMA PET/CT are concerning in patients with high-risk primary and BCR PCa; however, IBL location, SUV, and additional scan findings can aid interpretation. IBLs in any location with an SUVmax of at least 5 or with coexisting bone metastases irrespective of location and SUVmax have an increased risk for malignancy. Conversely, IBLs with an SUVmax of less than 5 that are present only in atypical locations such as the ribs without accompanying bone metastases are likely benign. These predictors may assist in decreasing the number of bone lesions on PSMA PET/CT that are truly indeterminate.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can imaging-based features on PSMA PET/CT predict the likelihood that an IBL is benign or malignant?
PERTINENT FINDINGS: Categorizing IBL location and SUVmax can predict for malignancy versus benignancy in 18F-DCFPyL PET/CT scans. An IBL with coexisting bone metastases or an IBL with an SUVmax of at least 5 after 2 h of uptake, independent of location, is suggestive of malignancy. An IBL in an atypical location such as the rib with an SUVmax of less than 5 after 2 h of uptake and without accompanying bone metastases is usually benign.
IMPLICATIONS FOR PATIENT CARE: Considering the location and SUVmax of IBLs and other findings on PSMA PET/CT scans can reduce the number of patients with an IBL by reassigning such lesions to either the benign or malignant category.
Footnotes
Published online Oct. 20, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 25, 2022.
- Revision received September 13, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.