


Visual Abstract

Abstract
In up to two thirds of prostate-specific membrane antigen (PSMA) PET scans, unspecific bone uptake has been described. The aim of this study was to estimate the diagnostic accuracy of [68Ga]Ga-PSMA-11 PET/CT for bone metastases and the occurrence of equivocal lesions. Methods: We analyzed retrospectively 118 patients who underwent a [68Ga]Ga-PSMA-11 PET/CT for initial staging or recurrence evaluation. Lesions were interpreted according to the PSMA reporting and data system (PSMA-RADS) and the prostate cancer molecular imaging standardized evaluation (PROMISE) criteria. The SUVmax and the localization of each lesion were recorded. A combination of prior or follow-up examinations was used as a reference standard to categorize benign and malignant lesions. Correlation between the final diagnosis and imaging or clinicobiochemical parameters was tested. The diagnostic accuracy was calculated for different cutoffs of PSMA-RADS criteria, for PROMISE criteria, and the sequential combination of both. Results: In total, 265 bone abnormalities were identified in 70 of 118 patients. Among these, 148 (55.8%) lesions in 50 (42.4%) patients were classified as PSMA-RADS-3B. There were no PSMA-RADS-3D lesions in our cohort. Equivocal lesions were more frequent on the ribs (30.6%) followed by the pelvis (26.5%), but in the ribs, such an uptake was malignant in 33.3% of cases versus 66.7% in the pelvis. A significant association was found between the final diagnosis and the SUVmax, prostate-specific antigen (PSA), PSA doubling time, International Society of Urological Pathology score, and the number of foci. The sensitivity and specificity were 100% and 63.6% for the PSMA-RADS-3B cutoff, respectively; 40.5% and 100% for the PSMA-RADS-4 cutoff, respectively; and 89.3% and 96.6% for both the PROMISE criteria and the sequential PSMA-RADS/PROMISE strategy, respectively. In the sequential method, the number of equivocal lesions was reduced from 147 to 2. We found that 53% of PSMA-RADS-3B lesions were malignant; 95.5% of lesions classified positive by the sequential method were true positives, whereas 32.6% were false negatives. Conclusion: [68Ga]Ga-PSMA-11 PET/CT has high accuracy for the diagnosis of bone metastases. Equivocal lesions constitute nearly half of the lesions seen on PSMA PET. The sequential combination of PSMA-RADS and PROMISE criteria reduces the number of lesions classified as equivocal. PSMA-RADS-3B lesions which are positive according to the PROMISE criteria should be considered highly suggestive of malignancy.
Prostate cancer (PCa) is often associated with bone metastases, with 3% presenting at initial diagnosis and 12% developing within 2 y, escalating to 80% at advanced stages (1,2). Bone metastases significantly impact prognosis; patients face a 1.52 times higher risk of fatal disease compared with those with nodal metastases (3). Three-year and 5-y survival rates for patients with bone metastases stand at 47.7% and 32.42%, respectively, markedly inferior (P < 0.001) to those without bone involvement (98.43% and 97.28%, respectively) (4).
Prostate-specific membrane antigen (PSMA), a glycoprotein highly expressed in PCa cells, can be imaged using PET radiopharmaceuticals. PSMA PET exhibits superior diagnostic accuracy in initial staging (5) and biochemical recurrence (6) compared with conventional imaging. It enhances lesion detectability even at low disease volumes, with pooled estimates of PET positivity reaching 33% (95% CI, 16%–51%) at PSA values below 0.2 ng/mL and 45% (95% CI, 39%–52%) for PSA values between 0.2 and 0.49 ng/mL (6). Nevertheless, PSMA is not PCa-specific, and false-positive uptake in benign bone lesions or unspecific bone uptake complicates interpretation (7,8), translating in an inherent risk of under- or overdiagnosis.
Standardized criteria, such as PSMA reporting and data system (PSMA-RADS) (9,10), the prostate cancer molecular imaging standardized evaluation (PROMISE) criteria (11,12), the European Association of Nuclear Medicine criteria (13), and E-PSMA criteria (14), aim to harmonize interpretation across readers and institutions. PSMA-RADS classifies lesions into 5 groups on the basis of morphology and uptake, subcategorizing equivocal lesions according to their type (e.g., bone, lymph node) and to their imaging characteristics. Note that PSMA-RADS does not provide a reference tissue to clearly define intense uptake. In this regard, PROMISE introduces a 4-level intensity-scoring scale. The European Association of Nuclear Medicine criteria incorporate a 2-step analysis, classifying uptake as abnormal and pathologic on the basis of intensity and pattern. E-PSMA criteria, discarding the subcategorization of lesions, including those in bone, categorize lesions into 5 groups and recommend using a 4-point scale of uptake intensity as well.
Despite these criteria refinements, equivocal lesions persist as a diagnostic challenge. This study seeks to evaluate the accuracy of [68Ga]Ga-PSMA-11 for the diagnosis of PCa bone metastases and to propose an approach to enhance differential diagnosis from other lesions. The investigation aims to contribute valuable insights into refining diagnostic protocols and ultimately improving patient outcomes in the management of PCa with bone involvement.
MATERIALS AND METHODS
Population
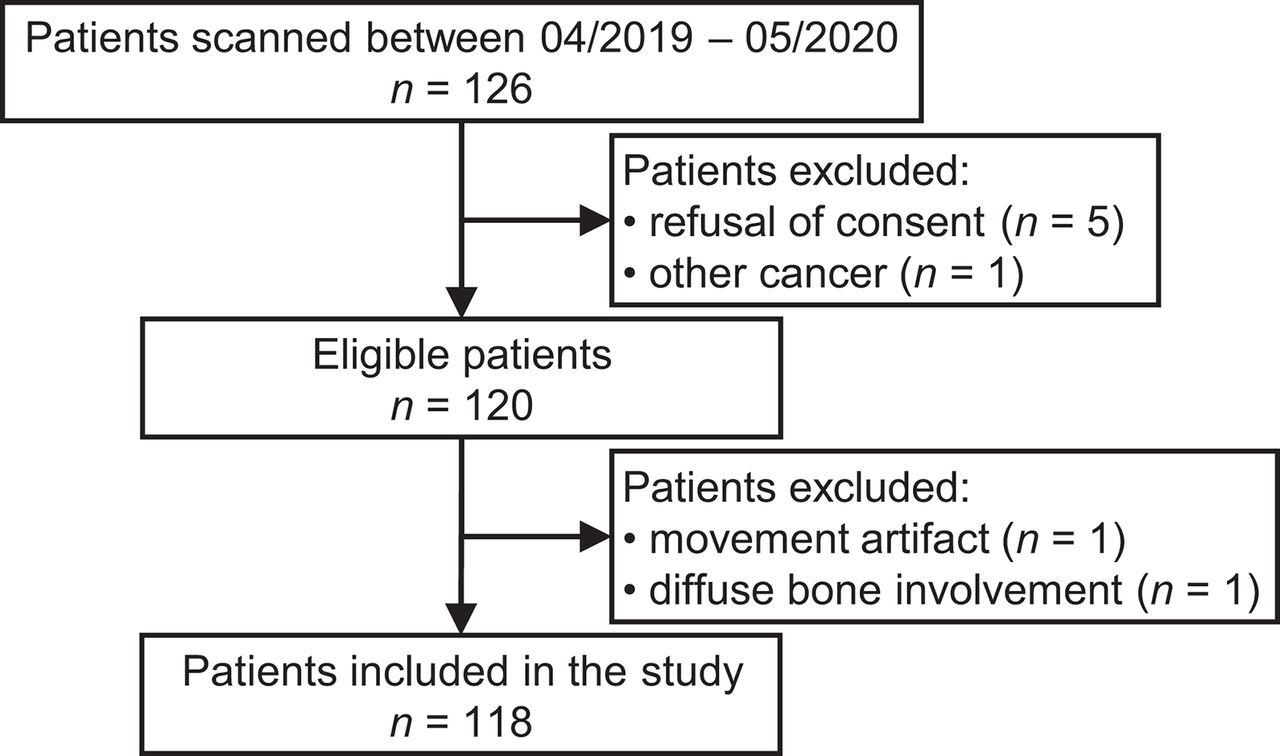
We retrospectively analyzed all consecutive [68Ga]Ga-PSMA-11 PET/CT scans acquired in our institution between April 2019 and May 2020. All participants had histology-proven prostate adenocarcinoma. The study protocol was approved by the institutional ethics committee (CCER ID: 2020-02500) with a waiver of signed informed consent, unless there was documented refusal of consent. A total of 126 patients underwent [68Ga]Ga-PSMA-11 PET/CT during this period. After application of exclusion criteria, 118 patients were included in the analysis (Fig. 1).

Flowchart of patient inclusion and exclusion.
Image Acquisition
All patients underwent [68Ga]Ga-PSMA-11 PET/CT: 44 patients on Biograph 128 Edge mCT Flow and 74 patients on digital Biograph 128 Vision (Siemens Healthineers). Sixty minutes after intravenous administration of [68Ga]Ga-PSMA-11 (2 MBq/kg, mean injected activity, 170 ± 22 MBq), the PET/CT image was acquired. First, CT was performed (reference 80 mAs, 120 kV, CareDose4D, CarekV; Siemens Healthineers) followed by PET acquisition with a speed of 0.5 mm/s (continuous bed motion) equivalent to 4.2 and 4.5 min per bed position, respectively, scanning from the proximal thighs to the vertex (a total of 5 to 6 bed positions). PET image reconstruction was performed using an attenuation-weighted ordered-subset expectation maximization iterative reconstruction algorithm with a matrix size of 400 for the mCT and 440 for the Vision and a slice thickness of 5 mm. The reconstruction parameters were set to the default values.
Image Data Analysis
Interpretation was performed on a diagnostic quality platform equipped with DICOM viewing software (OsirixMD). One nuclear medicine physician with 11 y of experience and 1 radiologist expert on osteoarticular imaging with 15 y of experience reviewed the PET/CT scans, masked to all other imaging and clinical information. The skeleton was divided into 9 regions: pelvis, lumbar spine, thoracic spine, cervical spine, lower extremities, upper extremities, ribs, clavicles/scapula/sternum, and head. For each lesion, the SUVmax and the location was noted. The radiologist analyzed the morphologic aspect on CT as no correlation, benign, equivocal, or malignant. If malignant, the aspect of the lesion (osteoblastic, lytic, or mixed) was noted.
PSMA-RADS Version 2.0
Lesions were classified according to the PSMA-RADS version 2.0 criteria, first without and then with reassignment and upgrade of PSMA-RADS-3B lesions to PSMA-RADS-4, in patients with more than 5 PSMA-RADS-4 or PSMA-RADS-5 lesions. In the absence of a clear definition, the threshold for intense activity (PSMA-RADS-4 and PSMA-RADS-5) was set at the parotid uptake level (10).
PROMISE Criteria
Lesions were classified according to the PROMISE criteria, using a morphologic correlate, the number of lesions, and the intensity of uptake compared with those of reference organs, as published (11,12).
Sequential Application of PSMA-RADS/PROMISE
First, lesions were classified according to PSMA-RADS version 2.0, without lesion reassignment. Then, the PROMISE criteria were applied for further characterization of PSMA-RADS-3B lesions.
Reference Standard
After completion of the [68Ga]Ga-PSMA-11 PET/CT analysis, lesions were compared with a composite reference standard, taking into account prior or follow-up examinations, including CT, MRI, bone scintigraphy, and serum PSA levels (Supplemental Table). A lesion was deemed to be a metastasis if biopsy confirmed the diagnosis, if PSMA focal uptake corresponded to a new lesion on CT compared with the most recent prior imaging, if follow-up imaging showed a new lesion or an increase in size or density corresponding to the PSMA focus, or if PSA dropped to zero after targeted treatment (e.g., radiotherapy). Conversely, a lesion was considered benign if CT revealed a benign lesion (e.g., enchondroma), if there was morphologic stability of at least 1 y without treatment, or if PSA dropped to zero after treatment unrelated to the lesion. Lesions which remained indeterminate despite a follow-up period of at least 1 y were labeled inconclusive on final diagnosis. Lesions without follow-up of at least 1 y that could not be characterized otherwise were labeled lost on follow-up.
Statistical Analyses
Descriptive statistics (median and interquartile range) were used for continuous data. Absolute numbers and percentages were used for ordinal and categoric data. All continuous variables were tested for normal distribution with the Shapiro–Wilk test, and normality was rejected with a P value of less than 0.05, indicating the use of a nonparametric test. Continuous and ordinal data were compared with the Mann–Whitney test. Categoric data were compared with the Pearson χ2 test. After exclusion of lesions already treated, lesions without follow-up, and lesions that remained inconclusive, we calculated the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of PSMA-RADS and PROMISE criteria. We used first the PSMA-RADS-3 as the cutoff and then the PSMA-RADS-4, and last we combined the 2 criteria using first the PSMA-RADS classification and then applied the PROMISE criteria on PSMA-RADS-3 lesions. Sensitivity and specificity between the different criteria were compared using the McNemar test. A P value of less than 0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 25 software (IBM). The Sankey diagram was created using sankeyMATIC.
RESULTS
In total, 118 patients were analyzed (Table 1). Most of these participants underwent [68Ga]Ga-PSMA-11 PET/CT in the context of biochemical recurrence or progression (40 with first recurrence, 61 for disease evaluation, including multiple recurrences and metastatic disease). Only 17 participants were scanned for initial staging, because at that period the [68Ga]Ga-PSMA-11 PET/CT was not yet in the clinically reimbursed indications.
Patient Demographic Characteristics
In total, 265 bone abnormalities were identified in 70 patients. Among these uptake regions, 119 foci (44.9%) in 45 patients (38.1%) either did not have a morphologic correlation on the CT (n = 90) or this was of indeterminate origin (n = 29) according to the radiology expert’s reading. In addition, after applying the PSMA-RADS criteria (Fig. 2), we identified 148 (55.8%) PSMA-RADS-3B lesions in 50 patients (42.4%), meaning equivocal lesions for which further work-up is proposed (Table 2).

PSMA-RADS examples. First row: PSMA-RADS-1, aligned rib fractures (SUVmax, 2.9 and 3) showing consolidation on follow-up. Second row: PSMA-RADS-2, degenerative vertebral alterations (SUVmax, 4.7) classified as benign. Third row: PSMA-RADS-3B, moderate focal uptake on left iliac bone (SUVmax, 6.2) without CT substrate, confirmed on follow-up by appearance of dense lesion. Fourth row: PSMA-RADS-4, intense focal uptake on D10 vertebral body (SUVmax, 62.3) without morphologic correlation, confirmed on follow-up. Fifth row: PSMA-RADS-5, intense focal uptake of dense lesion on D9 vertebral body (SUVmax, 23.9), showing extension to whole vertebral body and posterior elements on follow-up.
PSMA-RADS Results
Compared with the reference standard, there were in total 88 benign and 131 malignant lesions, which will be the focus of subsequent accuracy analyses. Additionally, 16 lesions remained equivocal despite follow-up; 8 lesions were already treated by radiation therapy and still presented a moderate uptake (1–3 y after treatment). For 21 lesions, no prior or follow-up work-up was available. One foci of abnormally increased uptake, initially considered to be a bone lesion, was proven on evaluation by MRI to be a schwannoma, misinterpreted because of its proximity to the bone (scapula) and excluded from further analysis.
The most common location of PSMA-RADS-3B lesions was the ribs (30.6%; mean SUVmax, 4.6), followed by the pelvis (26.5%; mean SUVmax, 6.5), the thoracic spine (16.3%; mean SUVmax, 5.3), the lumbar spine (9.5%; mean SUVmax, 7.1), the lower extremities (7.5%; mean SUVmax, 9.2), the scapula/clavicle and sternum together counting for 4.8% of total equivocal lesions with a mean SUVmax of 4.1, the head (2.7%; mean SUVmax, 8.8), the upper extremities (1.4%; mean SUVmax, 13.2), and the cervical spine (0.7%; SUVmax, 13.8). In the ribs, 44.4% of these lesions proved to be benign, 33.3% malignant, and 20% remained equivocal, whereas in the pelvis, 66.7% were malignant, 15.4% benign, and 5.1% equivocal (Fig. 3).

Histogram of PSMA-RADS-3B lesions according to location and diagnosis. Most common location was ribs, followed by pelvis. In ribs, 44.4% of lesions proved to be benign and 33.3% malignant, whereas in pelvis, 66.7% were malignant. FU = follow-up; RT = radiation therapy.
The normality of the distribution of the SUVmax, PSA, PSA doubling time, and years after diagnosis was rejected with the Shapiro–Wilk test (P < 0.05). The SUVmax was significantly higher in PSMA-RADS-3B lesions positive for malignancy on follow-up than in the negative ones (Mann–Whitney U test of 381.00, P < 0.0001) (Table 3). In patients presenting PSMA-RADS-3 lesions, the PSA value was significantly higher (U = 81.500, P = 0.002), the PSA doubling time was significantly shorter (U = 74.500, P = 0.010), the International Society of Urological Pathology score was significantly higher (U = 117.00, P = 0.030), and the number of foci was significantly higher (U = 73.00, P < 0.0001) when at least 1 of the lesions was malignant compared with the lesions of other patients that were benign.
Association of SUVmax, Clinicobiologic Parameters, and Diagnosis of PSMA-RADS-3B Lesions
With reassignment and upgrade of PSMA-RADS-3B lesions to PSMA-RADS-4, in multimetastatic patients, the number of equivocal lesions reduced from 147 to 113. With the sequential application of PSMA-RADS and PROMISE criteria (Fig. 4), the number of equivocal lesions decreased from 147 to 2. These 2 equivocal results in 2 patients corresponded to single bone lesions with an uptake score of 2 (higher than that in the liver and lower than that in the parotids; SUVmax, 15.7 and 12.1) both localized on a rib without any morphologic abnormality visible on the CT image.

Sankey diagram demonstrating sequential combination of PSMA-RADS and PROMISE criteria. Number of equivocal lesions decreased from 147 to 2. Of PSMA-RADS-3B lesions, 14 categorized negative by PROMISE were malignant and 3 categorized positive by PROMISE were benign. RT = radiation therapy.
Using the PSMA-RADS without lesion reassignment and a cutoff at PSMA-RADS-3B, the sensitivity was 100% with 32 false positives (FPs), whereas we set the cutoff at PSMA-RADS-4, there was a specificity of 100% with 78 false negatives (FNs). Upgrading PSMA-RADS-3B to PSMA-RADS-4 in multimetastatic patients and a cutoff at PSMA-RADS-4, the specificity remained 100% with 53 FNs. With the PROMISE criteria, the sensitivity was 89.3% and the specificity 96.6% with 3 FPs and 14 FNs, and the same results were obtained with sequential application of PSMA-RADS and PROMISE criteria (Table 4).
Diagnostic Performance of the Different Criteria
Interestingly, all FPs and FNs of PROMISE criteria were PSMA-RADS-3B lesions. In a total of 43 PSMA-RADS-3B lesions classified negative by PROMISE criteria, 14 were malignant on follow-up (32.6%). In a total of 67 PSMA-RADS-3B lesions categorized positive with PROMISE criteria, only 3 were benign on follow-up (4.5%).
The McNemar test yielded a statistically higher sensitivity for the PSMA-RADS cutoff of 3, followed by the PROMISE and sequential PSMA-RADS/PROMISE criteria (difference, 10.7%; P < 0.001), the PSMA-RADS-4 with lesion reassignment (40.5%; P < 0.001), and the PSMA-RADS-4 (59.5%; P < 0.001). The PSMA-RADS cutoff of 4 with or without lesion reassignment had higher specificity than the PROMISE and sequential PSMA-RADS/PROMISE criteria, but the difference was not significant (difference, 3.4%; P = 0.125), but the difference was significant compared with PSMA-RADS-3 (difference, 36.4%; P < 0.001).
Among the 21 lesions lost on follow-up, 13 were classified as PSMA-RADS-3B and 8 as PSMA-RADS-4 and PSMA-RADS-5. Based on the PROMISE criteria, the 8 PSMA-RADS-4 and PSMA-RADS-5 lesions would be positive, and for PSMA-RADS-3B lesions, 5 would be negative and 8 would be positive. To control whether lesions lost on follow-up would have changed the results, we compared the area under the receiver-operating-characteristic curve after including and considering equivocal lesions falsely classified by the PROMISE criteria. The change in the diagnostic accuracy was not significant (area under the curve of 0.877 vs. 0.928 for PROMISE with confirmed lesions; P = 0.068).
DISCUSSION
The primary objective of this retrospective study was to evaluate the diagnostic accuracy of [68Ga]Ga-PSMA-11 PET/CT in identifying bone metastases of PCa and to propose a diagnostic algorithm suitable for routine clinical application, facilitating the diagnostic process. After the introduction of PSMA PET tracers into clinical practice, physicians were confronted with focal bone uptake of uncertain origin. To obtain a balance between the higher diagnostic yield of these tracers and the unusual frequency of these findings, setting the diagnosis became challenging. Some of these indeed represent the PSMA tracers’ ability to detect metastases before visible morphologic changes (15), others are benign lesions, historically not posing diagnostic challenges (8), and some remain of indeterminate origin (7,16,17).
In our study, more than half of the [68Ga]Ga-PSMA-11 bone uptake lesions were categorized as PSMA-RADS-3B, indicating equivocal bone lesions requiring further investigation. Similar to previous reports (7,18), these lesions were most commonly located in the ribs (30.6%), followed by the pelvis (26.5%). Although rib lesions were mostly nonmalignant, as observed in prior studies (7,18,19), 66.7% of pelvic lesions in our study were malignant based on the reference standard. Discrepancies with a study by Chiu et al. (20), which did not find significant differences in FPs based on skeletal location, might be attributed to the fact that, contrary to our study, their analysis did not focus on equivocal lesions. Additionally, although 18F-labeling is associated with notable advantages, namely a lower positron energy resulting in higher spatial resolution, a longer half-life allowing centralized production and a wider distribution, facilitating clinical workflow, and eventually improving availability for patients, the presence of unspecific bone uptake is more common with [18F]F-PSMA-1007 than with [68Ga]Ga-PSMA-11 (16), occurring in up to two thirds of patients (7). A small retrospective study of PET image-guided biopsy found only 9.1% of such lesions to be metastatic, with the rest being benign without PSMA expression on immunohistochemistry (17). In our cohort, 8.7% of these bone uptake areas could be characterized on the basis of prior imaging, eventually available in the context of biochemical recurrence but not necessarily for primary staging. In our study, we excluded the index test from the reference standard. However, in clinical practice, follow-up PSMA PET could help characterize equivocal lesions by evaluating changes in uptake intensity, as suggested by Yin et al. and PSMA-RADS version 2.0 (10,18). Consistent with previous studies, malignant lesions exhibited a significantly higher median SUV than the benign ones (18,19). However, we refrained from deriving an SUV cutoff because of concerns about their generalizability. The use of SUV thresholds is problematic as the values of SUV are subject to machine, reconstruction, and acquisition delay variability.
The establishment of standardized interpretation criteria is crucial for providing harmonized and objective guidelines in clinical practice. Studies have demonstrated high interreader and intrareader reproducibility of various interpretation criteria (21,22). Notably, the lowest diagnostic confidence was associated with bone disease across different criteria. Our study proposes a combination of PSMA-RADS and PROMISE criteria to reduce the number of equivocal lesions based on the PSMA-RADS classification and to mitigate falsely classified PROMISE binary results. The number of equivocal lesions decreased from 147 with PSMA-RADS criteria to 2 with PROMISE and the sequential PSMA-RADS/PROMISE criteria. Moreover, incorporating PROMISE criteria for PSMA-RADS-3B lesions revealed that PSMA-RADS-3B lesions which are categorized positive with PROMISE criteria were indeed malignant in over 95% of cases, whereas PSMA-RADS-3B lesions classified as negative with PROMISE criteria were malignant in 32.6% of cases.
PSMA PET exhibits high diagnostic performance in detecting bone metastases, outperforming other modalities such as [18F]fluorocholine PET/CT, [18F]NaF PET/CT, MRI, and bone scintigraphy (23). Compared with bone scintigraphy, which suffers from FP results particularly at initial staging (24), [68Ga]Ga-PSMA-11 has demonstrated higher sensitivity (97%) and specificity (100%) (25). In our study, PROMISE or sequential PSMA-RADS/PROMISE criteria achieved a diagnostic accuracy of 92.2% for bone lesion characterization, with sensitivity, specificity, positive predictive value, and negative predictive value of 89.3%, 96.6%, 97.5%, and 85.9%, respectively. Relying solely on PSMA-RADS criteria would yield either high sensitivity or high specificity, depending on the chosen cutoff. Chiu et al., in a retrospective study, found a specificity of 73% and a positive predictive value of 95% using PSMA-RADS-4 as the cutoff for malignancy, in contrast to 100% for both in our study, potentially due to the higher cutoff in our classification, as this is not clearly defined in the criteria.
Nevertheless, our study has limitations. It is a retrospective monocentric study and lacks histopathologic confirmation of lesions. Instead, we used a reference standard including biopsy, imaging, and biochemical response. The exclusion of 21 lesions with unavailable follow-up did not impact the results significantly. Furthermore, in our cohort, there were no PSMA-RADS-3D lesions, a type of lesion that is managed differently by the PSMA-RADS and PROMISE criteria. These lesions would have been classified as benign by PROMISE criteria and could have increased the FN rate. Last, our study focused solely on bone lesions, and the generalizability of the results to soft-tissue equivocal lesions remains uncertain.
CONCLUSION
Over half of the bone lesions detected on PSMA PET/CT are equivocal, presenting challenges in diagnostic assessment due to the lack of morphologic substrate or low to moderate radiotracer uptake. Malignancy risk varies by location, with pelvic lesions more likely to be malignant than rib lesions. A sequential application of PSMA-RADS and PROMISE criteria reduces the number of equivocal lesions. Of the PSMA-RADS-3B lesions, 53% were malignant, and by the sequential method, 95.5% of lesions classified as positive were true positives. On the other hand, 32.6% were FNs, indicating that PSMA-RADS-3B lesions classified as negative with the sequential method still warrant follow-up.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can a combination of interpretation criteria improve the evaluation of equivocal bone lesions on [68Ga]Ga-PSMA-11 PET/CT?
PERTINENT FINDINGS: In this retrospective study, 55.8% of abnormal bone findings on [68Ga]Ga-PSMA-11 PET/CT were categorized PSMA-RADS-3B. PROMISE criteria alone or alongside PSMA-RADS reduced equivocal lesions from 147 to 2. Although the sequential use of these criteria did not enhance the accuracy beyond PROMISE alone, it could help identify lesions prone to misclassification by PROMISE interpretation.
IMPLICATIONS FOR PATIENT CARE: PSMA-RADS-3B lesions, classified as positive by the PROMISE criteria, should be considered highly suggestive of malignancy, as over 95% of lesions were indeed malignant. PSMA-RADS-3B lesions, classified as negative by PROMISE, still warrant follow-up, as at least 32.6% of them proved to be malignant on follow-up.
Footnotes
Published online Aug. 8, 2024.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 15, 2024.
- Accepted for publication July 4, 2024.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.