


Abstract
In prostate cancer with biochemical failure after therapy, current imaging techniques have a low detection rate at the prostate-specific antigen (PSA) levels at which targeted salvage therapy is effective. 11C-choline and 18F-fluoromethylcholine, though widely used, have poor sensitivity at low PSA levels. 68Ga-PSMA (Glu-NH-CO-NH-Lys-(Ahx)-[68Ga-N,N′-bis[2-hydroxy-5-(carboxyethyl)benzyl]ethylenediamine-N,N′-diacetic acid]) has shown promising results in retrospective trials. Our aim was to prospectively compare the detection rates of 68Ga-PSMA versus 18F-fluoromethylcholine PET/CT in men who were initially managed with radical prostatectomy, radiation treatment, or both and were being considered for targeted therapy. Methods: A sample of men with a rising PSA level after treatment, eligible for targeted treatment, was prospectively included. Patients on systemic treatment were excluded. 68Ga-PSMA, 18F-fluoromethylcholine PET/CT, and diagnostic CT were performed sequentially on all patients between January and April 2015, and the images were assessed by masked, experienced interpreters. The findings and their impact on management were documented, together with the results of histologic follow-up when feasible. Results: In total, 38 patients were enrolled. Of these, 34 (89%) had undergone radical prostatectomy and 4 (11%) had undergone radiation treatment. Twelve (32%) had undergone salvage radiation treatment after primary radical prostatectomy. The mean PSA level was 1.74 ± 2.54 ng/mL. The scan results were positive in 26 patients (68%) and negative with both tracers in 12 patients (32%). Of the 26 positive scans, 14 (54%) were positive with 68Ga-PSMA alone, 11 (42%) with both 18F-fluoromethylcholine and 68Ga-PSMA, and only 1 (4%) with 18F-fluoromethylcholine alone. When PSA was below 0.5 ng/mL, the detection rate was 50% for 68Ga-PSMA versus 12.5% for 18F-fluoromethylcholine. When PSA was 0.5–2.0 ng/mL, the detection rate was 69% for 68Ga-PSMA versus 31% for 18F-fluoromethylcholine, and when PSA was above 2.0, the detection rate was 86% for 68Ga-PSMA versus 57% for 18F-fluoromethylcholine. On lesion-based analysis, 68Ga-PSMA detected more lesions than 18F-fluoromethylcholine (59 vs. 29, P < 0.001). The tumor-to-background ratio in positive scans was higher for 68Ga-PSMA than for 18F-fluoromethylcholine (28.6 for 68Ga-PSMA vs. 9.4 for 18F-fluoromethylcholine, P < 0.001). There was a 63% (24/38 patients) management impact, with 54% (13/24 patients) being due to 68Ga-PSMA imaging alone. Histologic follow-up was available for 9 of 38 patients (24%), and 9 of 9 68Ga-PSMA–positive lesions were consistent with prostate cancer (68Ga-PSMA was true-positive). The lesion positive on 18F-fluoromethylcholine imaging and negative on 68Ga-PSMA imaging was shown at biopsy to be a false-positive 18F-fluoromethylcholine finding (68Ga-PSMA was true-negative). Conclusion: In patients with biochemical failure and a low PSA level, 68Ga-PSMA demonstrated a significantly higher detection rate than 18F-fluoromethylcholine and a high overall impact on management.
- 18F-fluoromethylcholine
- 68Ga-PSMA
- molecular imaging
- PET/CT
- prostate cancer
- prostate-specific membrane antigen
Despite advances in surgical technique and radiotherapeutic delivery, initial curative therapy will fail in a significant proportion of men with prostate cancer (1). In those men with biochemical failure after initial therapy, the currently available imaging techniques (2,3) have a low detection rate at the levels of prostate-specific antigen (PSA) at which targeted salvage therapy has optimal effect. With regard to PET/CT, whereas 18F-fluoromethylcholine (4) and 11C-choline (5) remain the best validated tracers for detection of recurrent prostate cancer (6,7), they have significant limitations that preclude their effectiveness in patients with a low PSA level (8). Recent retrospective data on the novel PET tracer 68Ga-PSMA (Glu-NH-CO-NH-Lys-(Ahx)-[68Ga-N,N′-bis[2-hydroxy-5-(carboxyethyl)benzyl]ethylenediamine-N,N′-diacetic acid]) have demonstrated promising sensitivity and specificity for the detection of prostate cancer in the setting of biochemical recurrence (9) and suggest that this agent is likely to be more sensitive than 18F-fluoromethylcholine or 11C-choline for the assessment of systemic spread (10,11). This promising tracer relies on overexpression of prostate-specific membrane antigen (a transmembrane folate hydrolase) on the surface of prostate cancer cells. This overexpression has been demonstrated both locally and in metastatic lesions within bone, lymph nodes, and soft tissue (12,13).
The aim of this study was to prospectively compare the detection rates and management impact of 68Ga-PSMA PET/CT and 18F-fluoromethylcholine PET/CT in patients with prostate cancer and a low but detectable PSA relapse after curative therapy.
MATERIALS AND METHODS
Study Design and Data Collection
Thirty-eight prostate cancer patients with a rising PSA level after radical prostatectomy, radiotherapy (external beam or other), or both, who were not yet on systemic therapy and were actively being considered for further targeted therapy, were enrolled in the trial. No target had been identified for treatment through clinical examination or imaging. Patients on hormonal or systemic treatment were excluded. Data on age, previous therapy, time since therapy, initial pathologic findings (including T stage and Gleason score), PSA doubling time, PSA at the time of scanning, and prior imaging results were collected at enrollment. The trial was approved by the Institutional Human Research and Ethics Committee, and informed consent was obtained from all participants.
Scan Acquisition
Both the 18F-fluoromethylcholine and the 68Ga-PSMA were produced onsite with good-laboratory-practice–compliant procedures using an automated radiopharmacy cassette (Trasis S.A.). Radiopharmacy quality control was undertaken using a high-pressure liquid chromatography method.
18F-fluoromethylcholine PET/CT and then 68Ga-PSMA PET/CT plus diagnostic contrast-enhanced abdominopelvic CT were performed within 30 d. The diagnostic CT scan was embedded within the attenuation-correction CT scan for the clinically indicated 18F-fluoromethylcholine scan but was separately reconstructed by standard CT methods and separately interpreted for the purposes of the study.
The routine clinical protocol was followed (for 18F-fluoromethylcholine, a 3.5 MBq/kg dose and a 10-min dynamic pelvic acquisition plus a 20-min static whole-body acquisition; for 68Ga-PSMA, a 2.0 MBq/kg dose and whole-body scanning 45 min after injection). Whole-body images were acquired from the vertex to the knees.
PET/CT was performed using an Ingenuity time-of-flight PET/64-slice CT scanner (Philips). For 68Ga-PSMA, unenhanced CT was performed 45 min after tracer injection using the following CT parameters: 2-mm slice thickness, 2-mm increment, soft-tissue reconstruction kernel, 120 keV and 50 mAs, 0.828 pitch, 600-mm field of view, and 512 matrix. Immediately after CT scanning, a whole-body PET scan was acquired for 2 min per bed position. For 18F-fluoromethylcholine PET/CT scans, low-dose and modulated diagnostic CT with intravenous contrast material was performed. The initial low-dose CT scan was acquired immediately before injection of 18F-fluoromethylcholine using the following parameters: 2-mm slice thickness, 2-mm increment, soft-tissue reconstruction kernel, 120 keV and 50 mAs, 0.828 pitch, 600-mm field of view, and 512 matrix. 18F-fluoromethylcholine was injected simultaneously with the PET acquisition of 1 bed position for 10 min, acquired in list mode to obtain dynamic reconstruction. Immediately afterward, modulated diagnostic whole-body CT with intravenous contrast material (vertex to midthigh) was performed with the following parameters: 2-mm slice thickness, 2-mm increment, soft-tissue reconstruction kernel, 120 keV and 50–350 mAs, 0.828 pitch, 600-mm field of view, and 512 matrix. The whole-body PET scan was then acquired for 2 min per bed position. For both 68Ga-PSMA and 18F-fluoromethylcholine scans, the emission data were corrected for randoms, scatter, and decay using the body-dynamic.xml and body.xml reconstruction protocols (Philips). All images were viewed and reported using Fusion Viewer (Philips).
Image Interpretation
The PET images were interpreted by 2 experienced nuclear medicine physicians who did not know the clinical or imaging results. Data for both the 18F-fluoromethylcholine and the 68Ga-PSMA scans were analyzed visually and semiquantitatively. Visual analysis included a 4-point certainty scoring scale, as well as site and size of lesions. Semiquantitative analysis was performed using an automated maximum standardized uptake value for both 18F-fluoromethylcholine and 68Ga-PSMA. No direct comparison was attempted. Instead, tumor-to-background ratios (TBRs) were determined for each lesion on both the 68Ga-PSMA and the 18F-fluoromethylcholine images. TBR was established by placing a 2-dimensional region of interest in the pelvis and measuring the maximum standardized uptake value of background fat within the area. This value was then used as the denominator for the maximum standardized uptake value of the lesion, resulting in TBR. The diagnostic CT results were interpreted separately by an experienced radiologist who did not know the PET results or clinical information.
Follow-up and Patient Management
Treating physicians were asked to report on the management plan prior to and subsequent to each PET scan. Changes in management after the 18F-fluoromethylcholine and 68Ga-PSMA results became known were classified as none, minor (change in delivery or site of selected treatment), or major (change in selected treatment). Detailed questions were posed on the type of management undertaken on the basis of the imaging results and whether 68Ga-PSMA had an added impact over 18F-fluoromethylcholine on management. All clinical data, along with any added value of imaging, were considered by treating physicians in defining further treatment. Histopathologic follow-up results were gathered when available.
Statistical Analysis
McNemar testing was used to analyze scan positivity at different PSA levels (0–0.5, 0.5–2.0, and 2.0–12.0 ng/mL). Pearson correlation and stepwise regression analysis were used to identify the determinants of scan positivity. PSA at the time of scanning, PSA doubling time, Gleason score, age, initial treatment, and years from treatment were included in the analysis. Wilcoxon signed-rank testing was used for lesion-based analysis and management-impact analysis. Two-tailed, paired t testing assuming unequal variance was used to analyze and compare TBR ratios between scans. PSA doubling time was calculated only for patients with a PSA level above 0.2 according to standard formulas, based on at least 2 PSA values separated by at least 3 mo within 1 y after recurrence and no adjuvant radiation or hormonal therapy before recurrence. Statistical analysis was performed with SPSS, version 21 (IBM).
RESULTS
The characteristics of the 38 patients are presented in Table 1. The primary treatment was radical prostatectomy in 34 patients (89%) and radiotherapy in 4 patients (11%). Twelve patients (32%) had undergone salvage radiotherapy after radical prostatectomy. The mean PSA level was 1.72 ng/mL (range, 0.04–12 ng/mL), and 30 patients (79%) had a PSA level of 2.0 ng/mL or less at the time of imaging. The mean PSA doubling time was 15.6 mo (range, 2.6–111.2 mo) and was calculated in 31 patients (insufficient data or low absolute PSA levels in the other 7 patients).
Patient Characteristics and Preimaging Data
Overall, 26 patients (68%) had positive scan results. Of these 26, 14 (54%) were positive with 68Ga-PSMA alone, 11 (42%) with both 18F-fluoromethylcholine and 68Ga-PSMA, and only 1 (4%) with 18F-fluoromethylcholine alone (subsequently confirmed as false-positive on biopsy). Overall, 12 of the 38 scans (32%) were negative with both tracers.
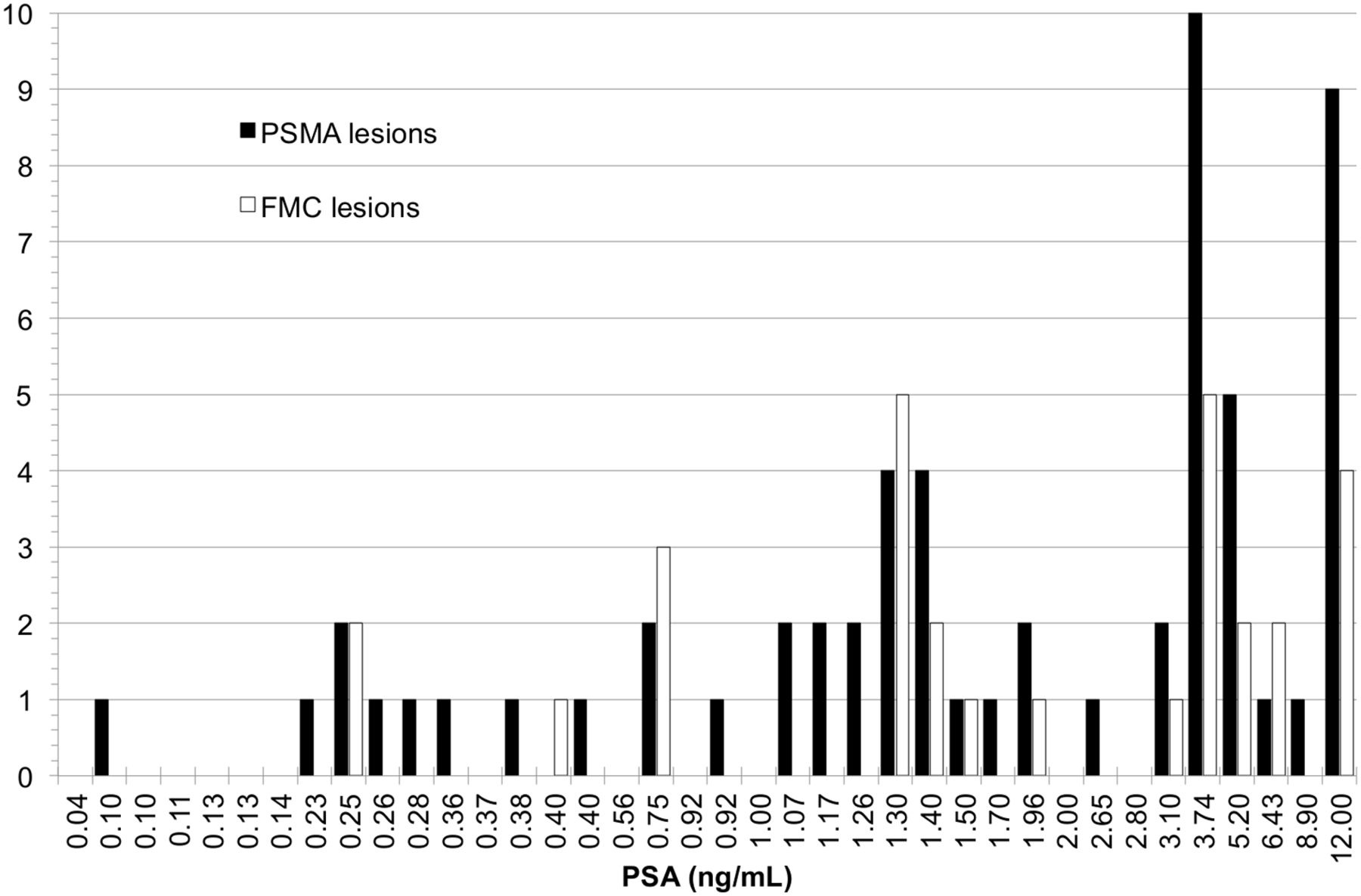
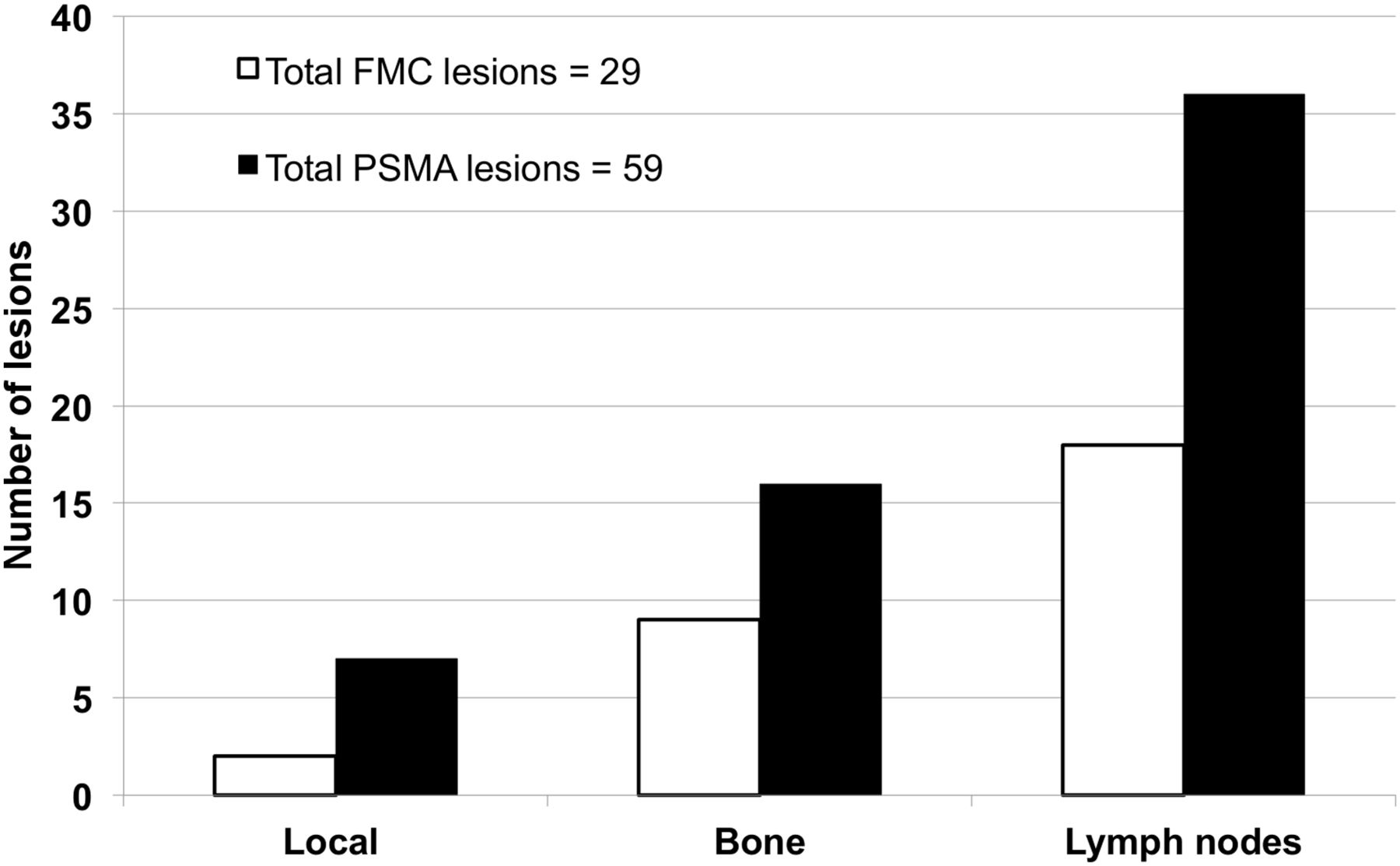
The most significant predictor of a positive PET result for both 18F-fluoromethylcholine and 68Ga-PSMA was PSA at the time of imaging (P < 0.001). In men with a PSA level below 0.5 ng/mL, 50% of scans were positive with 68Ga-PSMA versus 12.5% with 18F-fluoromethylcholine (P = 0.03). When PSA was 0.5–2.0 ng/mL, 71% were 68Ga-PSMA–positive and 36% were 18F-fluoromethylcholine–positive (P = 0.02). When PSA was above 2.0 ng/mL, 88% were 68Ga-PSMA–positive and 63% were 18F-fluoromethylcholine–positive (Table 2). Additionally, 68Ga-PSMA identified a higher number of lesions in every PSA cohort than did 18F-fluoromethylcholine (Fig. 1). Overall, 68Ga-PSMA detected more lesions than 18F-fluoromethylcholine (59 vs. 29, P < 0.001). More lesions (Fig. 2) were identified locoregionally, in lymph nodes and bone, with 68Ga-PSMA. Local lesions occurred both in radiotherapy patients (Fig. 3) and in radical prostatectomy patients. Uptake in residual radiotreated prostate tissue was detected on a single 18F-fluoromethylcholine scan and on three 68Ga-PSMA scans. For radical prostatectomy patients, seminal vesicle uptake was detected in 3 scans on solely 68Ga-PSMA (18F-fluoromethylcholine–negative, 68Ga-PSMA–positive). Finally, in a radical prostatectomy patient, the prostate bed was positive with 68Ga-PSMA but negative with 18F-fluoromethylcholine. Qualitative evaluation of the PET scan and the 2-mm-thick enhanced-CT slices was used to differentiate between activity within the urine and activity within the pelvis. With lesion-based analysis, only PSA at the time of scanning correlated significantly with total number of lesions on 68Ga-PSMA (P < 0.001) or 18F-fluoromethylcholine (P = 0.002). There was no significant correlation between PSA doubling time or Gleason score and the detection rate of either 18F-fluoromethylcholine or 68Ga-PSMA. On diagnostic enhanced CT, no lesions were considered definitely positive.
Detection Rates of 18F-Fluoromethylcholine and 68Ga-PSMA
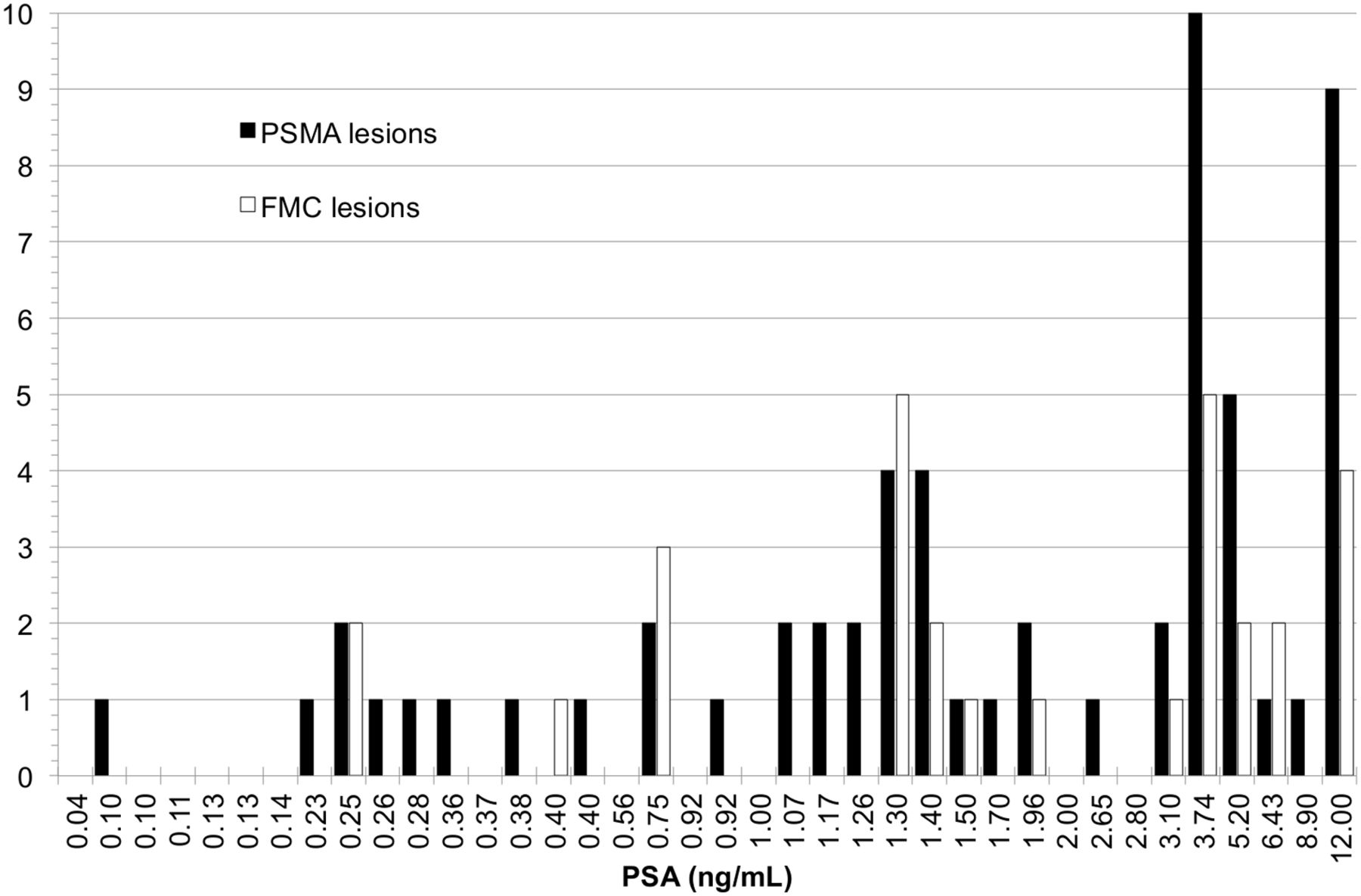
Total number of lesions detected for each patient with 18F-fluoromethylcholine (FMC) and 68Ga-PSMA, ranked by ascending PSA value.
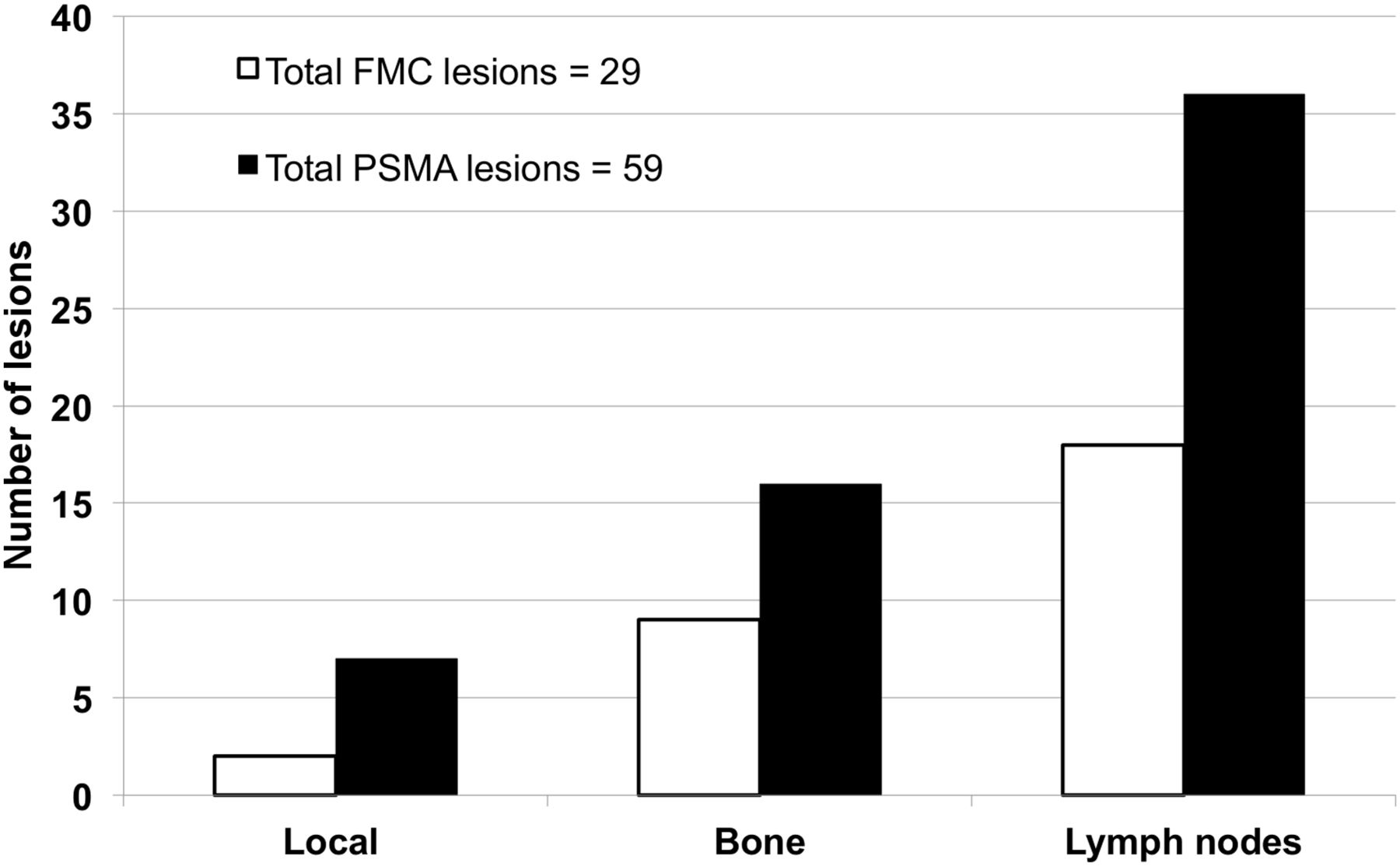
Total number of 18F-fluoromethylcholine (FMC) and 68Ga-PSMA–positive lesions per anatomic site, including prostate bed or seminal vesicles (local), bone, or lymph nodes.

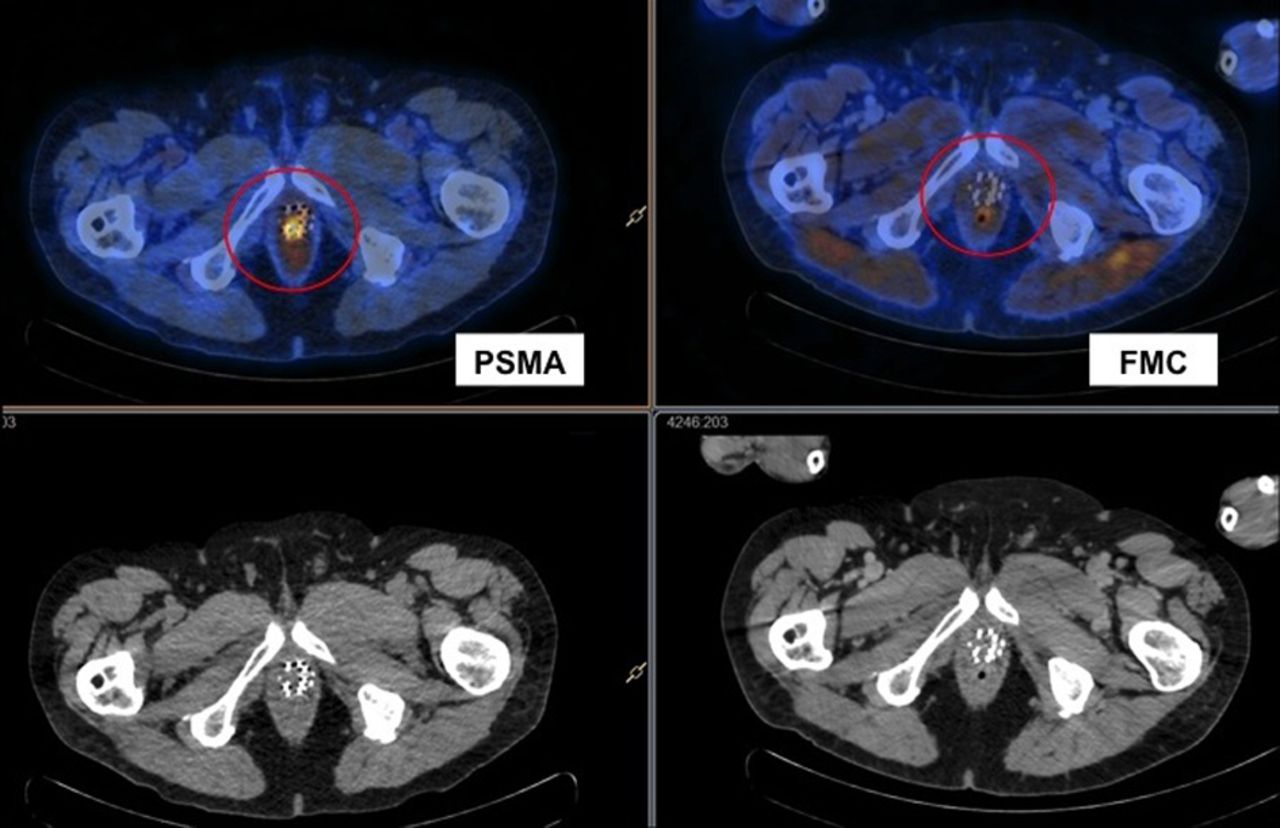
A 70-y-old man with Gleason 7 prostate cancer treated with radiation therapy who presented with rising PSA level (8.9) and PSA doubling time of 9.5 mo. 18F-fluoromethylcholine (FMC) scan was negative, whereas 68Ga-PSMA scan demonstrated intense uptake in prostate (maximum standardized uptake value, 4.5). Subsequent biopsy confirmed local recurrence.
After imaging, there was a major or moderate impact on management in 24 cases (63%) (Fig. 4), 54% (13/24) of which were attributable to the findings on 68Ga-PSMA imaging alone (Fig. 5). In the 11 of 24 patients (46%) for whom both 18F-fluoromethylcholine and 68Ga-PSMA had an impact, the 68Ga-PSMA results caused an additional change in management for 4 (36%). In no case was management changed on the basis of the results of 18F-fluoromethylcholine alone. In summary, 68Ga-PSMA imaging accounted (either alone or in concordance with 18F-fluoromethylcholine) for the entire impact on management in our patient cohort (24/38 for 68Ga-PSMA vs. 11/38 for 18F-fluoromethylcholine, P < 0.001). 68Ga-PSMA TBR was higher than 18F-fluoromethylcholine TBR in scans with positive findings (Fig. 6). The mean TBR was 9.4 for 18F-fluoromethylcholine but 28.6 for 68Ga-PSMA (P < 0.001). Mean uptake in fat was similar between the two types of scan (maximum standardized uptake values of 0.3 for 18F-fluoromethylcholine and 0.26 for 68Ga-PSMA).
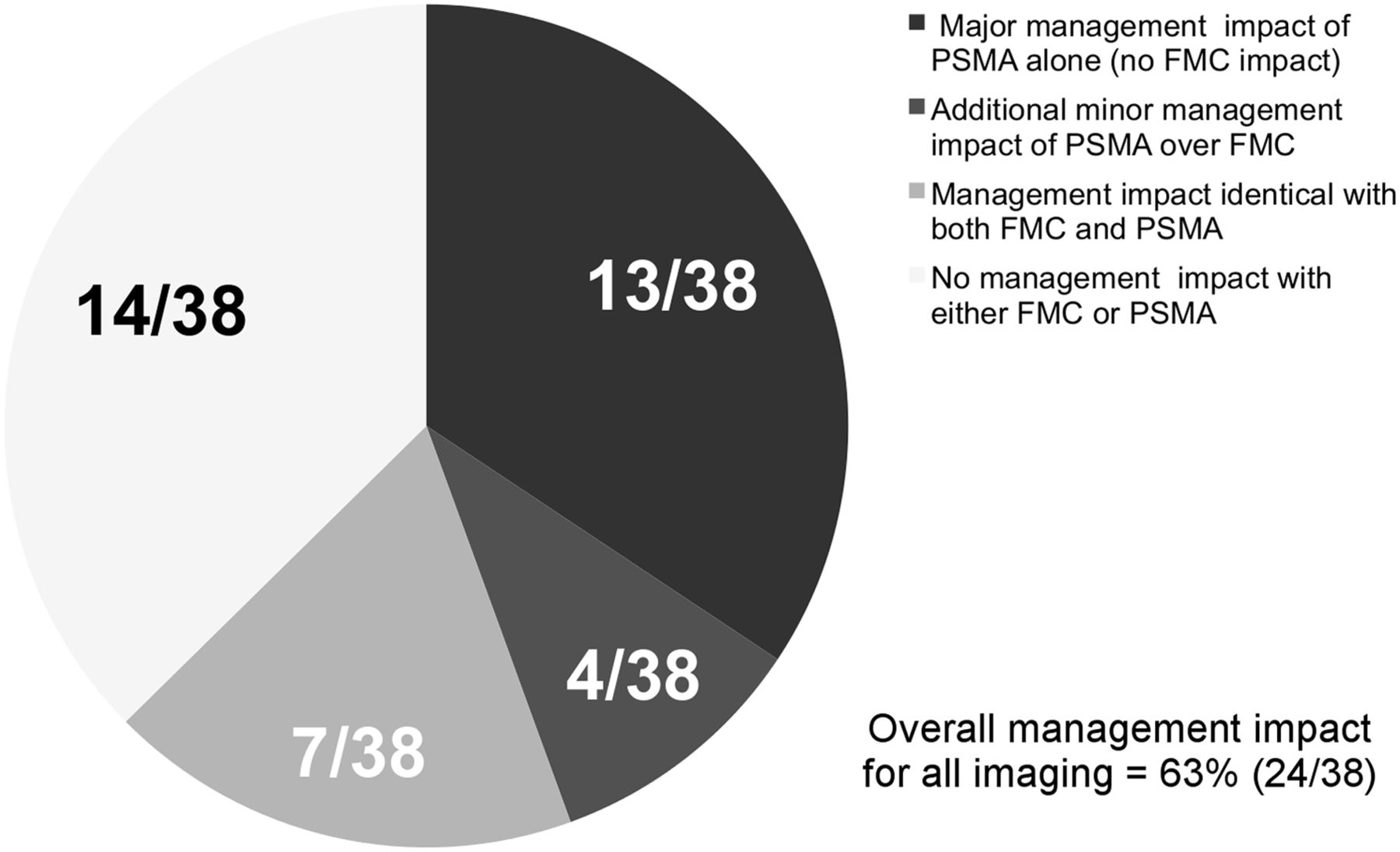
Impact on management. FMC = 18F-fluoromethylcholine.
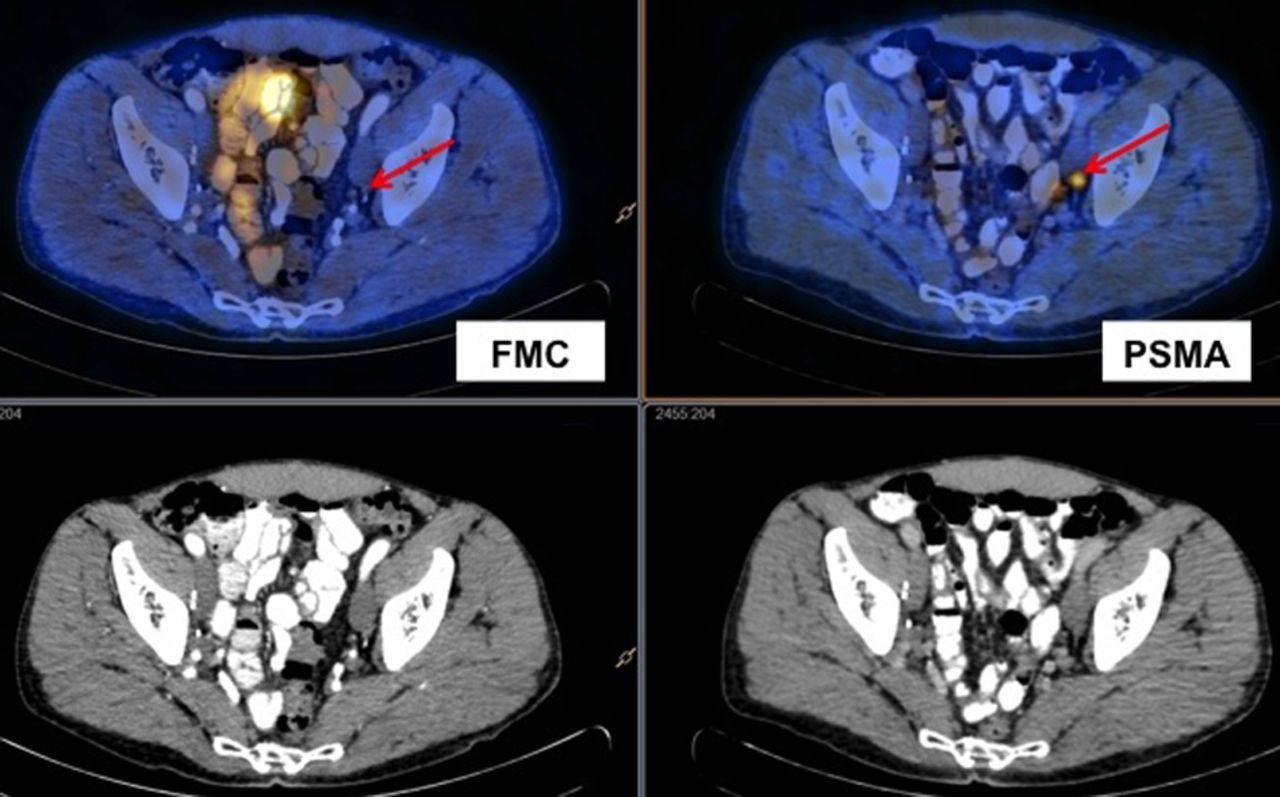
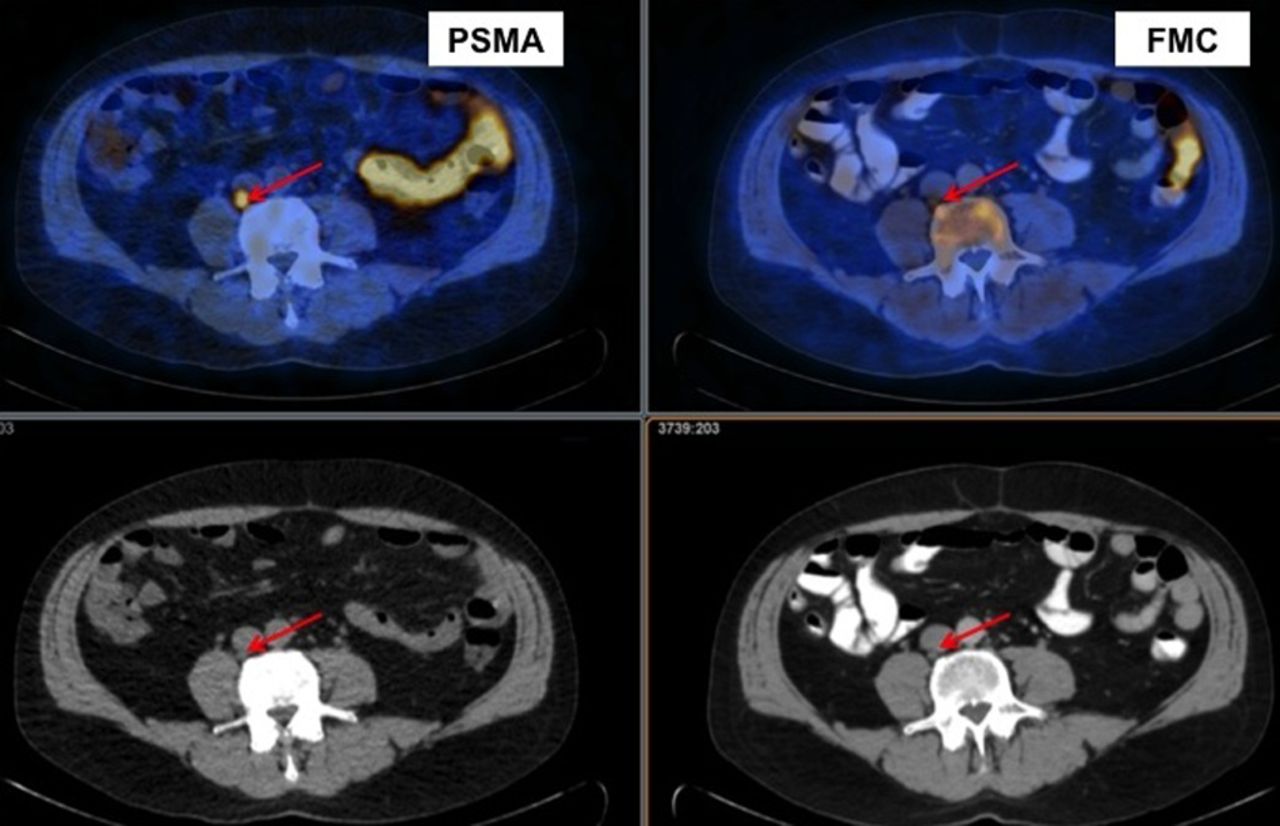
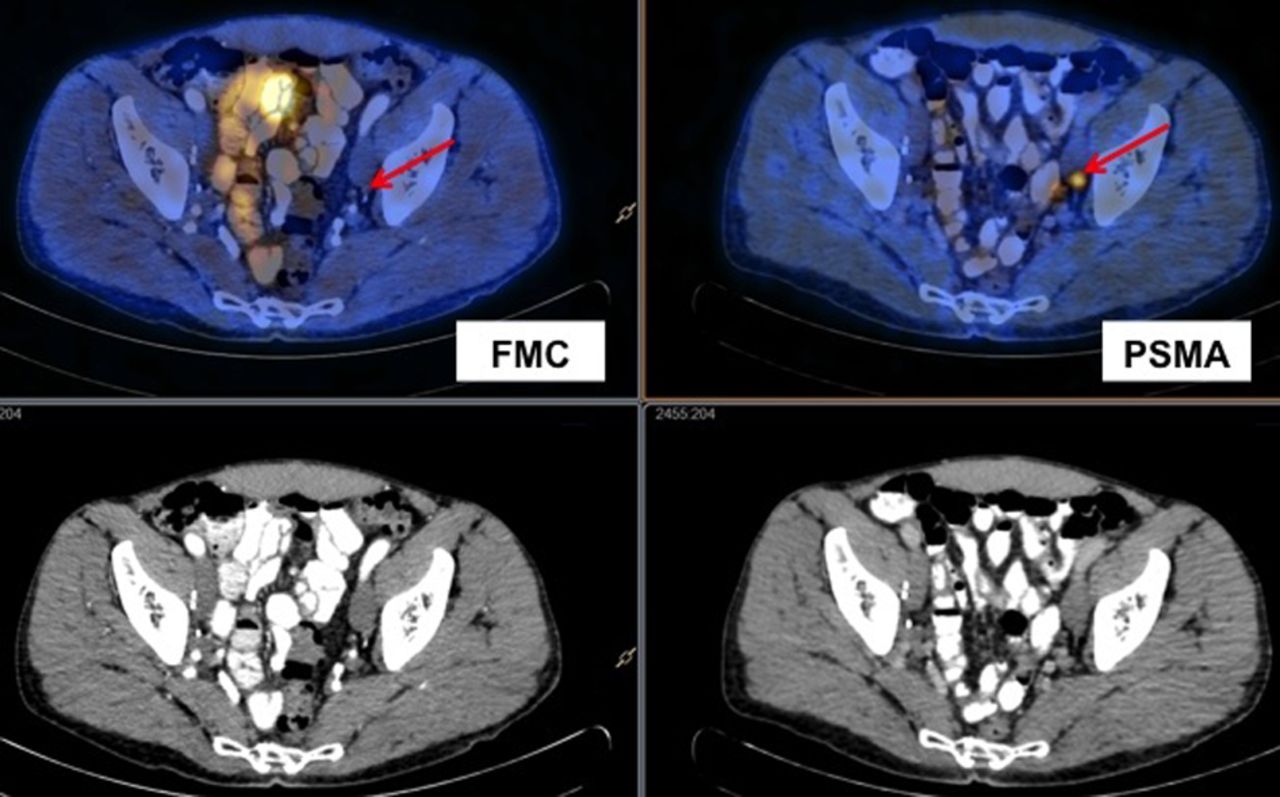
A 62-y-old man with Gleason 7 prostate cancer treated with radical prostatectomy and salvage radiation who presented with rising PSA level (0.4) and PSA doubling time of 8 mo. 18F-fluoromethylcholine (FMC) PET/CT findings were negative, whereas 68Ga-PSMA PET/CT scan demonstrated single positive left obturator lymph node (maximum standardized uptake value, 3.7). Subsequent biopsy confirmed prostate cancer recurrence.
A 70-y-old man with Gleason 7 prostate cancer treated with radical prostatectomy who presented with rising PSA (12.0) and PSA doubling time of 5.8 mo. Both 18F-fluoromethylcholine (FMC) PET/CT and 68Ga-PSMA PET/CT were positive for nodal disease (4 lesions positive on 18F-fluoromethylcholine imaging and 9 on 68Ga-PSMA). However, TBR was higher for 68Ga-PSMA than for 18F-fluoromethylcholine (25.0 vs. 7.0 in this image of positive paracaval lymph node). Biopsy confirmed nodal recurrence of prostate cancer.
Histopathologic confirmation was possible for 9 (24%) of the 38 patients with positive findings on 68Ga-PSMA or 18F-fluoromethylcholine imaging. All 9 of the 68Ga-PSMA–positive lesions that underwent biopsy were confirmed to be true-positive. Of the 2 lesions that were 18F-fluoromethylcholine–positive, one was true-positive. The other was false-positive with 18F-fluoromethylcholine (and on MR imaging) and true-negative with 68Ga-PSMA.
DISCUSSION
Our key finding was that in patients with rising PSA after curative treatment, 68Ga-PSMA has a higher detection rate than 18F-fluoromethylcholine regardless of PSA level. This finding was most evident in patients with low PSA levels (<0.5 ng/mL), with 50% of such patients having positive 68Ga-PSMA results. The high sensitivity at low PSA levels has important implications for the management of patients in whom PSA is rising after therapy with curative intent (radical prostatectomy or radiation) (14). There is a paucity of published literature on 68Ga-PSMA in humans. Although 3 retrospective studies (9,11,15) demonstrated promising results, to our knowledge no prospective studies have been published. The diagnostic value of 11C-choline and 18F-fluoromethylcholine is well documented (6,16), and the use of these agents in the setting of biochemical relapse is increasing (17). However, both tracers lack sensitivity at low PSA levels (8), and neither is yet standardized (18). Our results reinforce the limited sensitivity of 18F-fluoromethylcholine at low PSA levels and suggest that 68Ga-PSMA may more effectively detect recurrent disease at low PSA levels. The value of treating recurrent prostate cancer at low PSA levels has recently been outlined in European guidelines (14) and is associated with a reduced incidence of biochemical failure (19).
Currently, men with low PSA levels who experience biochemical relapse after radical prostatectomy often undergo salvage radiotherapy to the prostatic bed even when there are no significant imaging findings. Hence, it is no surprise that, per the nomogram of Stephenson et al. (20), only about half these men are currently cured. Furthermore, in a few men salvage radiation treatment may be harmful. Therefore, the high detection rate of 68Ga-PSMA at low PSA levels—demonstrated in this trial—may benefit management in patients with an early rise in PSA level after initial treatment. On the basis of our findings, disease outside the prostate bed is identified on 68Ga-PSMA alone in up to 75% (6/8) of 68Ga-PSMA–positive patients who would be eligible for salvage radiotherapy of the prostate bed (those patients with a PSA level of <1.0 ng/mL). The current clinical paradigm of either 18F-fluoromethylcholine–guided or unguided salvage radiotherapy of the prostate bed would have failed in these patients.
The superior sensitivity of 68Ga-PSMA compared with 18F-fluoromethylcholine was previously demonstrated in a single retrospective study (11), but there were important differences between that study population and ours. Most patients in our study had a PSA level below 2.0 ng/mL, whereas the previous study had a mean PSA level of 11.1 ng/mL and therefore was less able to demonstrate an added benefit for 68Ga-PSMA over 18F-fluoromethylcholine at low PSA levels. However, despite the difference in patient cohorts, both studies demonstrated a statistically higher total number of lesions detected with 68Ga-PSMA than with 18F-fluoromethylcholine in all positive patients.
Our study found that when 68Ga-PSMA was performed at low absolute PSA levels, the impact on management was exceptionally high. There are several reasons for this. First, when tumor recurred in the prostate bed, potentially curative and directed salvage radiation was delivered. Second, when oligometastatic disease was present, targeted treatments such as stereotactic body radiotherapy or lymph node dissection were used. Finally, when metastatic disease was found with 68Ga-PSMA (or less likely, with 18F-fluoromethylcholine), systemic treatment was begun and the patient was spared from undergoing salvage radiation to the prostatic fossa.
This study demonstrated a significantly higher TBR with 68Ga-PSMA than with 18F-fluoromethylcholine. Lesions detected with 68Ga-PSMA were more than twice the intensity of those detected with 18F-fluoromethylcholine, compared with background tissue. The significantly higher TBR with 68Ga-PSMA allows easier identification of even very small lesions.
The major limitation of this trial was that not all positive findings were confirmed histopathologically. Confirmation was impaired by the small volume of individual lesions and the high number of biopsy-inaccessible lymph node and bone recurrences. In patients whose biopsy was successful, we could confirm all 68Ga-PSMA findings as true-positive. At biopsy, one 18F-fluoromethylcholine–positive (and MR imaging–positive) lymph node that had been negative on 68Ga-PSMA was found. The aim of this trial was not to determine diagnostic accuracy but to assess the detection rate of the 2 tracers at low PSA levels. Many of these patients with disease identified on PET/CT will be undergoing targeted therapy as part of their routine clinical care. We intend to continue long-term follow-up of this cohort to document response to therapy and confirm diagnostic accuracy.
Histopathologic confirmation was obtained in only 24% of patients. However, it is remarkable that 100% of the 68Ga-PSMA–positive lesions that underwent biopsy were true-positive and that the single lesion positive with 18F-fluoromethylcholine and negative with 68Ga-PSMA was of a reactive nature. Although this study confirmed a high detection rate for 68Ga-PSMA at low PSA levels, further prospective trials addressing sensitivity and specificity are urgently needed.
A further limitation of this trial was the small number of men enrolled. Nevertheless, it is impressive that with such a small cohort there was a statistically significant difference in detection rates between 68Ga-PSMA and 18F-fluoromethylcholine on both a patient basis and a lesion basis. However, large, adequately powered prospective trials are needed to better evaluate 68Ga-PSMA.
Though previously reported in publications on 11C-choline (8,21) and more recently 68Ga-PSMA (22), a statistically significant correlation between PSA doubling time, Gleason score, and 18F-fluoromethylcholine or 68Ga-PSMA positivity was not found in our study. This discrepancy is probably related to the low mean PSA values of this patient cohort (<2.0 ng/mL) and the small number of men enrolled. Calculation of the PSA doubling time was possible for only 31 patients, therefore limiting statistical analysis of this variable.
The development of 68Ga-PSMA is at an early stage. Currently, there are several different 68Ga-PSMA ligands in clinical use and under research (23), making extrapolation of these data across all clinical sites problematic. Further product development, comparative trials, and harmonization of tracer use are urgently needed.
CONCLUSION
In patients who have a low, rising PSA level and are being evaluated for therapy with curative intent, 68Ga-PSMA PET/CT demonstrated a significantly higher detection rate for recurrent disease than 18F-fluoromethylcholine and had an impact on management in many patients. Although these findings need to be confirmed in larger trials, this prospective trial suggests that 68Ga-PSMA PET/CT will be an effective imaging tool for early detection of prostate cancer recurrence.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Funding was provided by St. Vincent’s Prostate Cancer Centre and the Australian Department of Health and Ageing through the Australian Prostate Cancer Research Centre—New South Wales (APCRC-NSW). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 25, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 4, 2015.
- Accepted for publication June 17, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic Efficacy of Various Imaging Modalities Across Different Stages of Prostate Cancer: A Network Meta-Analysis of Diagnostic Studies
- Prospective Comparison of 68Ga-NeoB and 68Ga-PSMA-R2 PET/MRI in Patients with Biochemically Recurrent Prostate Cancer
- Strong Correlation Between SUVmax on PSMA PET/CT and Numeric Drop-In {gamma}-Probe Signal for Intraoperative Identification of Prostate Cancer Lesions
- An Analysis of the Distribution of PSMA PET/CT-Positive Lymph Nodes and Their Coverage by Different Elective Nodal Radiation Volumes in Postoperative Prostate Cancer Patients
- Phase III Study of 18F-PSMA-1007 Versus 18F-Fluorocholine PET/CT for Localization of Prostate Cancer Biochemical Recurrence: A Prospective, Randomized, Crossover Multicenter Study
- Biology of Cancer and PET Imaging: Pictorial Review
- Diagnostic Performance and Clinical Impact of 68Ga-PSMA-11 PET/CT Imaging in Early Relapsed Prostate Cancer After Radical Therapy: A Prospective Multicenter Study (IAEA-PSMA Study)
- Detection Efficacy of 18F-rhPSMA-7.3 PET/CT and Impact on Management in Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy and Before Potential Salvage Treatment
- Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer
- Impact of 68Ga-PSMA-11 PET on the Management of Recurrent Prostate Cancer in a Prospective Single-Arm Clinical Trial
- 11C-Choline PET/CT in Recurrent Prostate Cancer: Retrospective Analysis in a Large U.S. Patient Series
- 3-Year Freedom from Progression After 68Ga-PSMA PET/CT-Triaged Management in Men with Biochemical Recurrence After Radical Prostatectomy: Results of a Prospective Multicenter Trial
- [18F]DCFPyL PET-MRI/CT for unveiling a molecularly defined oligorecurrent prostate cancer state amenable for curative-intent ablative therapy: study protocol for a phase II trial
- Appropriate Use Criteria for Imaging Evaluation of Biochemical Recurrence of Prostate Cancer After Definitive Primary Treatment
- Head-to-Head Comparison of 68Ga-PSMA-11 with 18F-PSMA-1007 PET/CT in Staging Prostate Cancer Using Histopathology and Immunohistochemical Analysis as a Reference Standard
- Detection Rate and Localization of Prostate Cancer Recurrence Using 68Ga-PSMA-11 PET/MRI in Patients with Low PSA Values <= 0.5 ng/mL
- Prostate-Specific Membrane Antigen-Guided Surgery
- Prospective Evaluation of PSMA-Targeted 18F-DCFPyL PET/CT in Men with Biochemical Failure After Radical Prostatectomy for Prostate Cancer
- Thyroid and androgen receptor signaling are antagonized by CRYM in prostate cancer
- Healthy Tissue Uptake of 68Ga-Prostate-Specific Membrane Antigen, 18F-DCFPyL, 18F-Fluoromethylcholine, and 18F-Dihydrotestosterone
- Phase I Study of CTT1057, an 18F-Labeled Imaging Agent with Phosphoramidate Core Targeting Prostate-Specific Membrane Antigen in Prostate Cancer
- Detection Rate of 18F-Choline PET/CT and 68Ga-PSMA-HBED-CC PET/CT for Prostate Cancer Lymph Node Metastases with Direct Link from PET to Histopathology: Dependence on the Size of Tumor Deposits in Lymph Nodes
- Impact of 68Ga-PSMA PET/CT on the Radiotherapeutic Approach to Prostate Cancer in Comparison to CT: A Retrospective Analysis
- Metaanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology
- Proceedings: Pathways for Successful Translation of New Imaging Agents and Modalities--Phase III Studies
- Prospective, Multisite, International Comparison of 18F-Fluoromethylcholine PET/CT, Multiparametric MRI, and 68Ga-HBED-CC PSMA-11 PET/CT in Men with High-Risk Features and Biochemical Failure After Radical Prostatectomy: Clinical Performance and Patient Outcomes
- Follow-up of Lesions with Equivocal Radiotracer Uptake on PSMA-Targeted PET in Patients with Prostate Cancer: Predictive Values of the PSMA-RADS-3A and PSMA-RADS-3B Categories
- Dosimetry of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: Correlations Between Pretherapeutic Imaging and Whole-Body Tumor Dosimetry with Treatment Outcomes
- Detection Efficacy of 18F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy
- 68Gallium-labelled PSMA-PET/CT as a diagnostic and clinical decision-making tool in Asian prostate cancer patients following prostatectomy
- Biochemical Recurrence of Prostate Cancer: Initial Results with [18F]PSMA-1007 PET/CT
- 64CuCl2 PET/CT in Prostate Cancer Relapse
- Impact of 68Ga-PSMA-11 PET/CT on the Management of Prostate Cancer Patients with Biochemical Recurrence
- Proposal for a Structured Reporting System for Prostate-Specific Membrane Antigen-Targeted PET Imaging: PSMA-RADS Version 1.0
- 68Ga-PSMA-11 PET/CT Mapping of Prostate Cancer Biochemical Recurrence After Radical Prostatectomy in 270 Patients with a PSA Level of Less Than 1.0 ng/mL: Impact on Salvage Radiotherapy Planning
- Impact of 68Ga-Prostate-Specific Membrane Antigen PET/CT on Prostate Cancer Management
- The Impact of 68Ga-PSMA PET/CT on Management Intent in Prostate Cancer: Results of an Australian Prospective Multicenter Study
- Impact of 68Ga-PSMA-11 PET on Management in Patients with Biochemically Recurrent Prostate Cancer
- Treatment Outcomes from 68Ga-PSMA PET/CT-Informed Salvage Radiation Treatment in Men with Rising PSA After Radical Prostatectomy: Prognostic Value of a Negative PSMA PET
- Seduction by Sensitivity: Reality, Illusion, or Delusion? The Challenge of Assessing Outcomes after PSMA Imaging Selection of Patients for Treatment
- PSMA Ligands for PET Imaging of Prostate Cancer
- Molecular radiotheragnostics in prostate cancer
- 68Ga-PSMA-11 PET/CT Interobserver Agreement for Prostate Cancer Assessments: An International Multicenter Prospective Study
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- Acceleration of PSMA-Targeted Theranostics to the Clinic: Can Common Sense Prevail?
- Detection Efficacy of Hybrid 68Ga-PSMA Ligand PET/CT in Prostate Cancer Patients with Biochemical Recurrence After Primary Radiation Therapy Defined by Phoenix Criteria
- 68Ga-PSMA-PET/CT Has a Role in Detecting Prostate Cancer Lesions in Patients with Recurrent Disease
- The Clinical Impact of Additional Late PET/CT Imaging with 68Ga-PSMA-11 (HBED-CC) in the Diagnosis of Prostate Cancer
- 68Ga-PSMA-11 PET Imaging of Response to Androgen Receptor Inhibition: First Human Experience
- The Rise of PSMA Ligands for Diagnosis and Therapy of Prostate Cancer
- What Medical, Urologic, and Radiation Oncologists Want from Molecular Imaging of Prostate Cancer
- Prostate-Specific Membrane Antigen-Targeted Radiohalogenated PET and Therapeutic Agents for Prostate Cancer
- Pilot Comparison of 68Ga-RM2 PET and 68Ga-PSMA-11 PET in Patients with Biochemically Recurrent Prostate Cancer
- 18F-Fluoride PET in the Assessment of Malignant Bone Disease