


Abstract
177Lu-prostate-specific membrane antigen (PSMA)–617 enables targeted delivery of β-particle radiation to prostate cancer. We determined its radiation dosimetry and relationships to pretherapeutic imaging and outcomes. Methods: Thirty patients with prostate cancer receiving 177Lu-PSMA-617 within a prospective clinical trial (ACTRN12615000912583) were studied. Screening 68Ga-PSMA-11 PET/CT demonstrated high PSMA expression in all patients. After therapy, patients underwent quantitative SPECT/CT at 4, 24, and 96 h. Pharmacokinetic uptake and clearance at a voxel level were calculated and translated into absorbed dose using voxel S values. Volumes of interest were drawn on normal tissues and tumor to assess radiation dose, and a whole-body tumor dose was defined. Correlations between PSMA PET/CT parameters, dosimetry, and biochemical and therapeutic response were analyzed to identify relationships between absorbed dose, tumor burden, and patient physiology. Results: Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%. On screening PSMA PET, whole-body tumor SUVmean correlated with mean absorbed dose (r = 0.62), and SUVmax of the parotids correlated with absorbed dose (r = 0.67). There was an inverse correlation between tumor volume and mean dose to the parotids (r = −0.41) and kidneys (r = −0.43). The mean parotid dose was also reduced with increasing body mass (r = −0.41) and body surface area (r = −0.37). Conclusion: 177Lu-PSMA-617 delivers high absorbed doses to tumor, with a significant correlation between whole-body tumor dose and PSA response. Patients receiving less than 10 Gy were unlikely to achieve a fall in PSA of at least 50%. Significant correlations between aspects of screening 68Ga-PET/CT and tumor and normal tissue dose were observed, providing a rationale for patient-specific dosing. Reduced salivary and kidney doses were observed in patients with a higher tumor burden. The parotid dose also reduced with increasing body mass and body surface area.
Prostate-specific membrane antigen (PSMA) is a type II transmembrane protein expressed in most clinically significant prostate cancers. Its expression increases in higher-grade, metastatic, and androgen-insensitive tumors (1–5), whereas expression is largely absent in benign or hyperplastic prostate tissue (6). Lower PSMA expression occurs in proximal small bowel, kidneys, and salivary and lacrimal glands (7,8). PSMA is a favorable target for molecular imaging (9–14) and therapy (15–21) of prostate cancer labeled with positron and β-emitting radionuclides, respectively
Radiolabeled small-molecule inhibitors of PSMA show promise as therapeutic agents in advanced prostate cancer (22), and understanding their radiation dosimetry is key to their development. 177Lu has favorable decay characteristics for radionuclide therapy, possessing both a short-range cytotoxic β-particle and a small γ-emission–enabling biodistribution to be quantified using scintigraphy.
Dosimetric estimates from retrospective series with β-labeled small molecules suggest that the normal tissues receiving the highest absorbed doses are small intestine, kidneys, and salivary glands (15,23–28).
Tumor dose may be an important predictor of clinical response, but estimation of a clinically relevant tumor-absorbed dose is challenging in patients with multiple sites of disease, often with variable uptake and retention of the therapeutic agent. It is difficult to envisage how index lesion dosimetry, as is commonly performed, can reflect this heterogeneity. In a novel approach we have estimated mean “total-body” tumor dose, alongside lesional tumor dosimetry, postulating that this may be more clinically relevant.
The primary aim of this study was to perform radiation dosimetry in men with advanced prostate cancer treated in a prospective clinical trial (29) using an automated voxelized dosimetry tool (30). We evaluated whether pretherapeutic 68Ga-PSMA PET is a predictor of absorbed dose, whether a “sink effect” was evident, and whether dose in normal tissues and tumor can predict toxicity and clinical response.
MATERIALS AND METHODS
Study Design and Patient Population
Between August 2015 and December 2016, 30 patients with PSMA-avid metastatic castration-resistant prostate cancer were enrolled and underwent up to 4 cycles of 177Lu-PSMA-617. Sufficient PSMA avidity for therapy was defined on 68Ga-PSMA-11 PET/CT as at least 1 site of metastatic disease with intensity significantly greater than normal liver (SUVmax at least 1.5 times SUV of normal liver). 18F-FDG PET/CT scans excluded patients if sites of 18F-FDG–positive disease without high PSMA expression were identified. Disease progression, either radiologically or clinically, was mandated before entry into the trial. The study protocol was approved by the institutional ethics board and was conducted in accordance with the declaration of Helsinki and good clinical practice. The trial was registered with the Australian New Zealand Clinical Trials Registry (ANZCTR12615000912583), and all patients gave written informed consent before study entry.
The 177Lu-PSMA-617 preparation, study design, and procedures have been previously described (29). The administered radioactivity (GBq) was adjusted according to tumor burden, patient weight, and renal function adapted from our practice using 177Lu-DOTATATE as follows. Activity was increased by 1 GBq if there were more than 20 sites of disease, decreased by 1 GBq if fewer than 10 sites, increased by 0.5 GBq per factor if weight was more than 90 kg or glomerular filtration rate more than 90 mL/min, and decreased by 0.5 GBq if weight was less than 70 kg or glomerular filtration rate less than 60 mL/min. Up to 4 cycles of therapy were administered at 6 weekly intervals.
Image Acquisition and Dosimetry
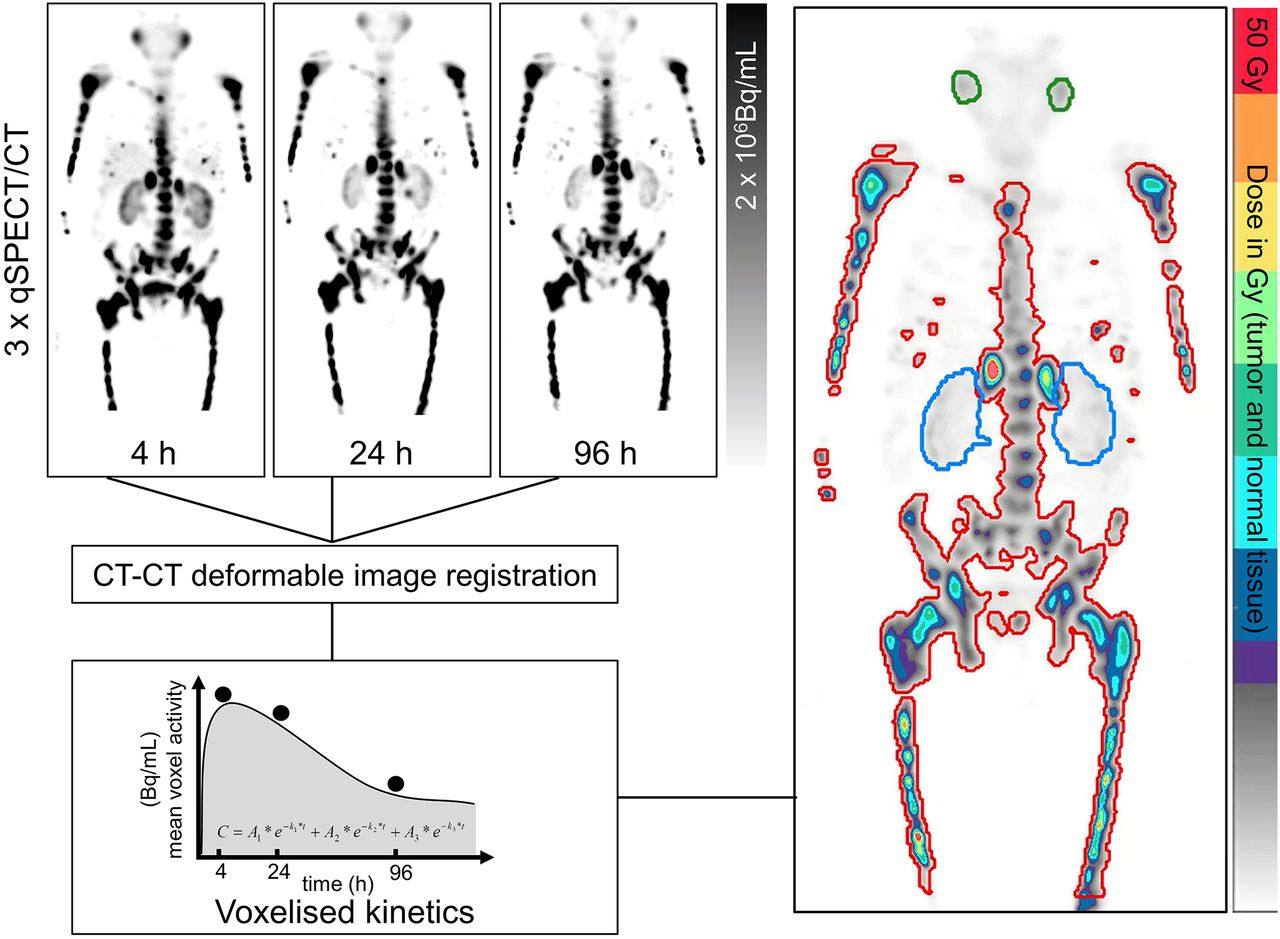
Thirty dosimetric image sets were obtained after initial therapy with serial quantitative SPECT/CT (2- or 3-bed-position acquisition) encompassing neck to pelvis performed 4, 24, and 96 h after injection (Symbia T6 or Intevo 16; Siemens A.G.) (Fig. 1).

Schematic of voxel-based dosimetry workflow, showing regions of interest for whole-body tumor volume (red), kidneys (blue), and salivary glands (green). qSPECT/CT = quantitative SPECT/CT.
SPECT voxels were acquired with dimensions of 4.8 × 4.8 × 4.8 mm, and 177Lu activity was quantified by conversion of voxel counts per seconds to activity per unit volume using attenuation, scatter, and dead-time corrections according to the protocol described by Beauregard et al. (31). Serial quantitative SPECT images were converted into voxel dose maps using a modified methodology described previously (30). Images were aligned by sequential rigid and B-spline deformable registration with Elastix (version 4.8) (32) using a weighted normalized correlation metric (80%) with transform bending energy penalty (20%). CT-to-CT registration was used to compute deformation fields for alignment of fused SPECT volumes. Images were resampled to 3 × 3 × 3 mm3 voxels to assist with voxel S-value convolution. Time–activity curves were independently calculated in each voxel based on a 3-phase exponential clearance model yielding 3-dimensional cumulated activity maps (30). Dose conversion was performed by convolving GATE-derived voxel dose kernel (maximum range, 40 mm) based on decay of 177Lu in ICRP soft tissue (33). Dose volumes were saved in DICOM format and contoured on clinical workstations. Regions of interest were drawn in normal tissues and tumor to determine absorbed dose. Mean “whole-body” tumor volume was determined by applying a 5-Gy threshold to the voxel dose volumes and then removing regions of physiologic uptake.
For normal tissues with a small size, namely the salivary and lacrimal glands, expanded contours encompassing the organs plus a 1- to 2-cm margin were also determined. Lacrimal dosimetry could not be obtained in 15 patients, as they were not included in the SPECT field of view at all 3 of the time points. These volumes were used to compute regional activity at each time point, and cumulated activity was converted to absorbed dose using the OLINDA sphere model S values, adjusted for patient-specific volumes defined on pretreatment 68Ga-PSMA PET scans (34–36). The duodenum presents a logistic challenge for our automated system because of its motile nature, and dosimetry for this organ has not been determined.
68Ga-PSMA PET/CT Analyses
Baseline 68Ga-PSMA-11 PET/CT was used to assess eligibility for treatment. “Whole-body” tumor volume was determined using an automated threshold encompassing activity with an SUV greater than 3, with removal of areas of physiologic uptake (MIM Software). This tumor volume was further subdivided into bone and soft tissue using subthresholding to 100 Hounsfield units and visual adjustment of the contours. Salivary glands were contoured on the PET sequence using an edge detection algorithm (PET Edge; MIM Software). For each volume of interest, the SUVmax, SUVmean, and volume were calculated.
Statistical Analysis
All continuous data are expressed as the median, SD, and range and R-statistics. We calculated correlations between parameters of PSMA PET/CT and dosimetric results estimated using our voxel-based method. We computed Spearman r and P values for each correlation and tested for difference in absorbed doses to tumor in patients achieving a prostate-specific antigen (PSA) response greater than 50% using a Wilcoxon–Mann–Whitney test. All analyses were conducted with R (R Development Team, 2018), and P values of less than 0.05 were considered statistically significant.
RESULTS
Baseline characteristics of patients and administered activities were documented (Supplemental Appendix 1). The median age of subjects was 70.5 y (interquartile range, 67–75 y), and patients had a median PSA doubling time of 2.4 mo. All patients were heavily pretreated, with 87% receiving prior systemic chemotherapy; 47% had also received second-line chemotherapy. Eighty-three percent had received second-generation antiandrogens, and more than 90% had more than 20 sites of disease. The mean administered activity was 7.8 GBq (range, 5.7–8.7 GBq).
Normal-Organ Dosimetry
Dosimetric estimates in parotid and submandibular glands, kidneys, spleen, liver, and noninfiltrated bone marrow are summarized in Tables 1 and 2. Salivary glands, lacrimal glands, and kidneys received the highest absorbed doses. For lacrimal glands, the application of MIRD yielded doses higher by a factor of 10 than the voxel technique; these are shown in Table 2.
Absorbed Doses in Normal Tissues (Gy) and Dose per Administered Activity (Gy/GBq) Following First Cycle of Therapy (Voxelized Technique)
Absorbed Dose Estimates in Absolute Dose (Gy) and Dose per Administered Activity (Gy/GBq) Estimated by Voxelized and MIRD Techniques
SUVmax of parotid glands on 68Ga-PSMA-11 PET correlated with mean absorbed dose (Gy/GBq) from voxel-based dosimetry (r = 0.68, P < 0.01) and is shown in Figure 2. There was an inverse correlation between tumor volume (defined on PSMA PET) and mean dose to the parotid glands (r = −0.41, P = 0.03) and kidneys (r = −0.43; P = 0.02). Mean parotid absorbed dose decreased with increasing body mass (r = −0.41, P < 0.01) and body surface area (r = −0.37, P < 0.05) and is shown in Figure 3. There was no significant correlation between parotid dose and glomerular filtration rate (r = 0.13, P = 0.5).
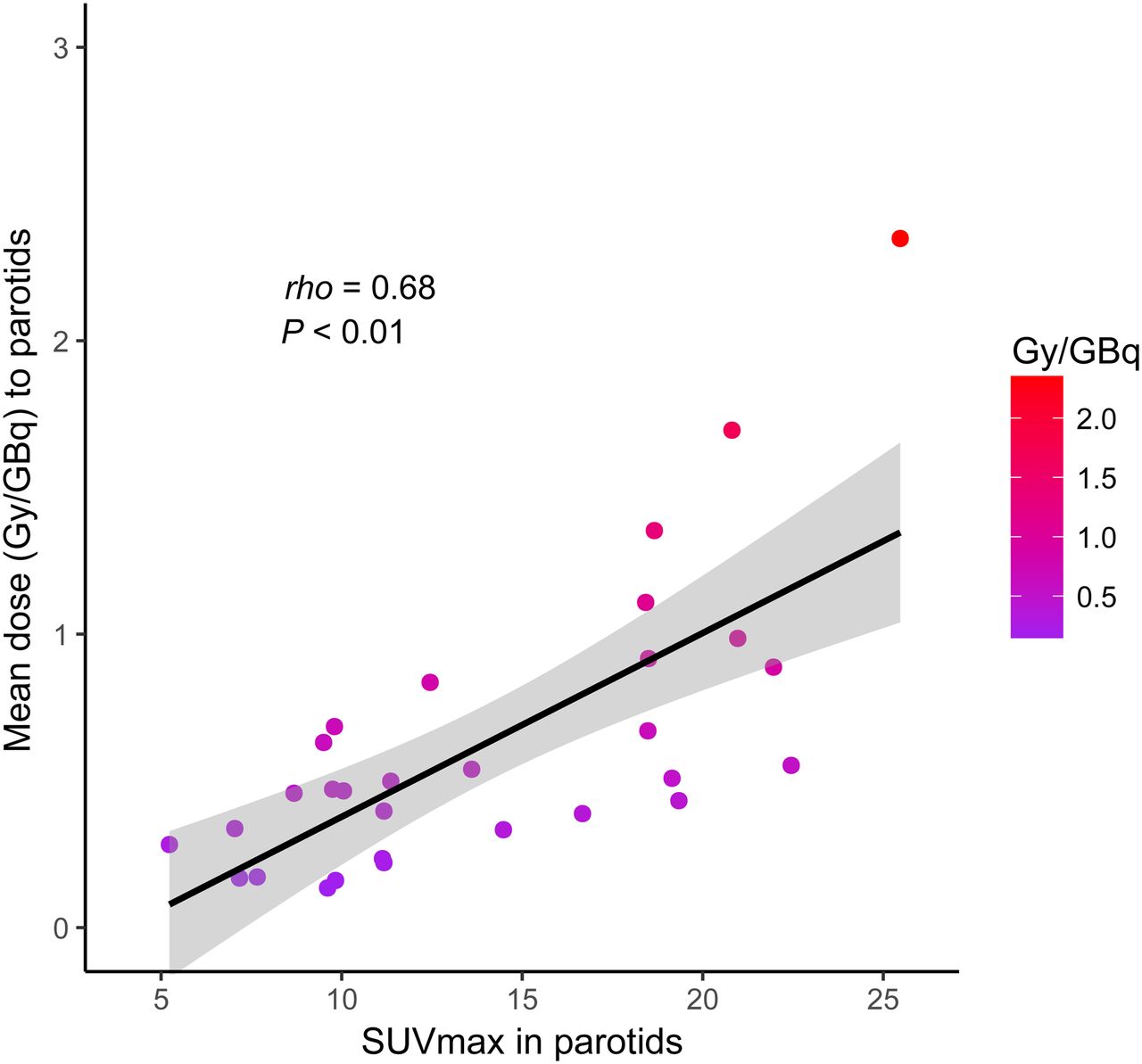
Correlation between SUVmax in parotid glands on screening 68Ga-PSMA PET and absorbed dose.

(A) Correlation between tumor volume on screening 68Ga-PSMA PET and mean parotid absorbed dose. (B) Correlation between body mass and mean parotid absorbed dose. (C) Correlation between body surface area and mean parotid absorbed dose.
Tumor Dosimetry
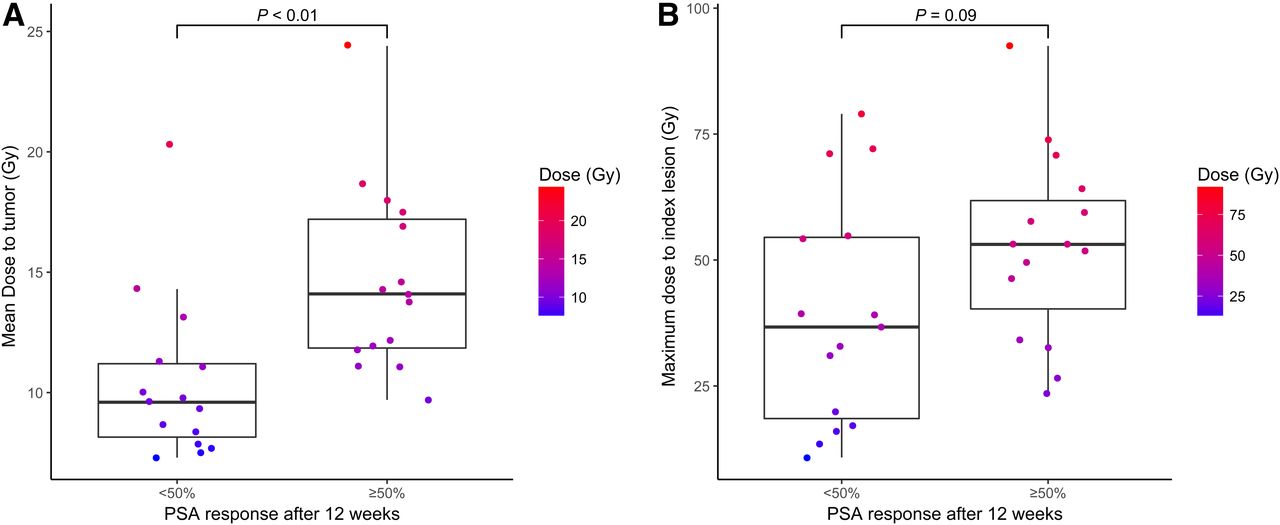
Absorbed whole-body tumor doses are shown in Table 3 and further divided into tumor-bearing bone and lymph/visceral regions. “Whole-body” tumor dose was associated with PSA response at 12 wk, with a median dose of 14.1 Gy (mean, 14.7 Gy; SD, 3.9 Gy; range, 9.7–24.4 Gy) in patients achieving a PSA decline of at least 50%, versus 9.6 Gy (mean, 10.4 Gy; SD, 3.4 Gy; range, 7.3–20.3 Gy) for those achieving a PSA decline of less than 50% (P < 0.01), and is shown in Figure 4A. With a tumor dose of less than 10 Gy, only 1 patient achieved a PSA decline of at least 50% and 10 patients had a PSA decline of less than 50%. Nonresponding patients achieved a significantly lower tumor dose than responders (P < 0.01) (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). Maximum tumor-absorbed dose in index lesions did not correlate with PSA response at 12 wk and is shown in Figure 4B.
Maximum Absorbed Dose (Gy) and Dose per Administered Activity (Gy/GBq) in Tumor-Bearing Bone, Lymph Nodes, and Mean Whole-Body Tumor Doses Above 5 Gy

(A) Mean whole-body tumor-absorbed dose was significantly higher in patients achieving greater than 50% fall in serum PSA at 12 wk. (B) Maximum tumor-absorbed dose in index lesions was not significantly different in patients achieving greater than 50% fall in serum PSA at 12 wk.
We found a significant correlation between the SUVmean of “whole-body” tumor on screening 68Ga-PSMA PET and the “whole-body dose” (Gy/GBq) (r = 0.62, P < 0.01); these correlations are shown in Figure 5. Both soft-tissue and bone metastases separately showed a significant correlation between SUVmean and mean absorbed dose (r = 0.55, P < 0.01, and r = 0.60, P < 0.01), respectively. There was a trend for a higher SUVmean to be associated with a PSA response at 12 wk, with a median SUVmean of 8.9 (mean, 9.2; SD, 2.8; range, 5.3–15.6) in patients achieving a decline of at least 50%, versus 7.0 (mean, 7.3; SD, 1.9; range, 5.1–12.1) in those who did not (P = 0.056) (Supplemental Fig. 2).
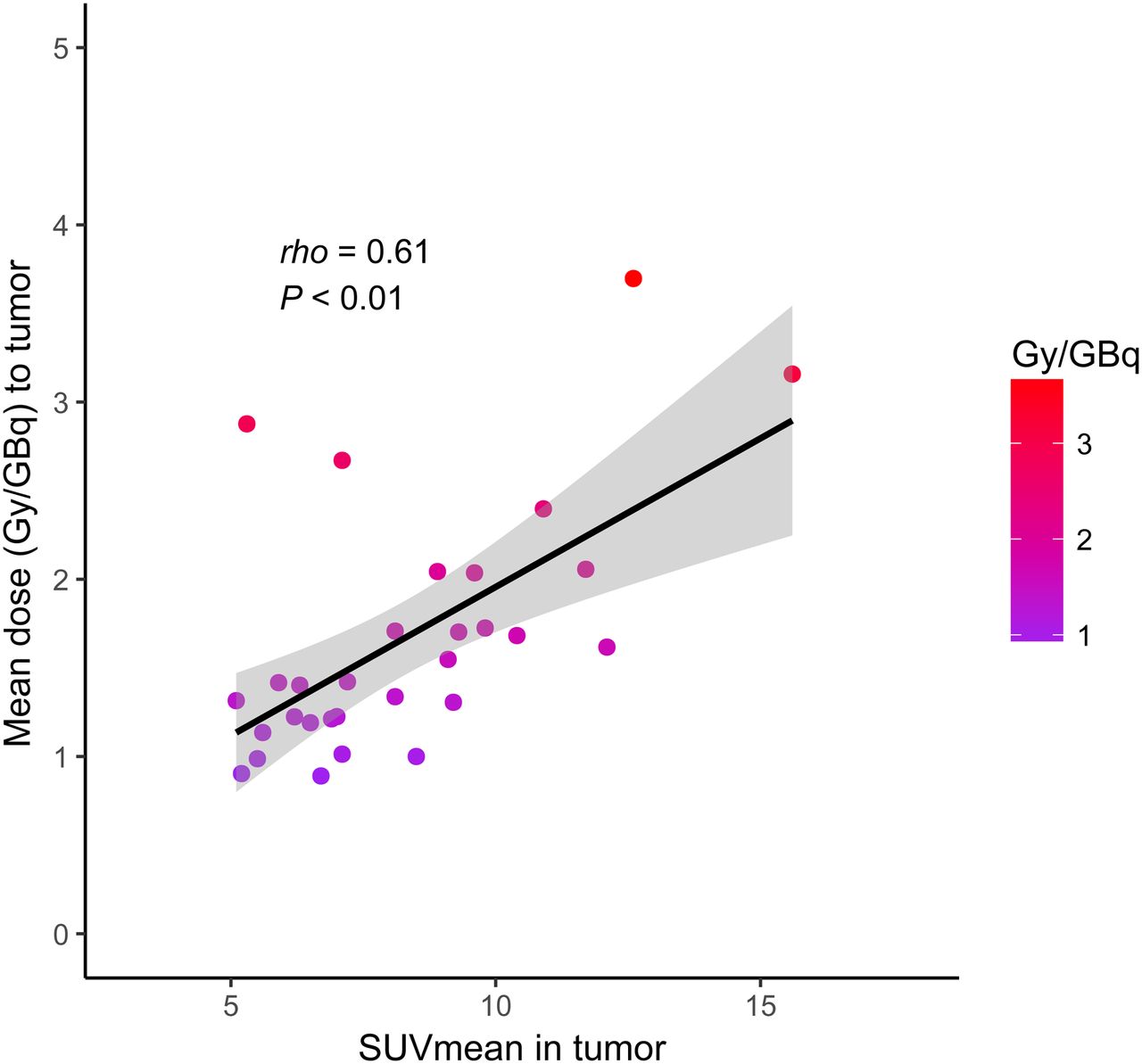
Correlation between SUVmean on screening 68Ga-PSMA PET and mean whole-body tumor dose calculated using 5-Gy dose cutoff.
DISCUSSION
We have demonstrated high tumor–to–normal-tissue uptake with prolonged retention of radionuclide in tumor-bearing areas in men with metastatic prostate cancer treated with 177Lu-PSMA-617.
Previous studies have generally used whole-body planar scintigraphy to measure activity (Supplemental Appendix 2) and may overestimate activity, particularly if significant activity overlies organs or tumor-bearing regions of interest. This overestimation has been well described in renal dosimetry after therapy using radiolabeled somatostatin analogs (37,38) and is relevant in PSMA radionuclide therapy, where bowel and liver may overlie kidneys and bone metastases may overlie salivary and lacrimal glands (13,24). The drawing of regions of interest on multiple sequential planar images is also time-consuming and subject to interobserver variation.
Although widely used, MIRD has several limitations as a dosimetry tool. Developed for population-based dosimetry, it assumes that organ masses and shapes conform to those of a standard man. Furthermore, it does not provide conversion factors for tumor or all organs, with no S factors for lacrimal or salivary glands. To assess dose in these organs using MIRD, we applied the OLINDA sphere model using volumes taken from pretreatment 68Ga-PSMA PET scans (36). These structures also present challenges for our voxelized dosimetry technique because of partial-volume effects and a greater likelihood of potential misregistration. The latter is most notable in the head and neck, where head rotation may occur between scans (35–39), and is of particular concern defining very small ROIs, such as lacrimal glands.
Absorbed dose estimates using both the voxel-based technique and MIRD show broad agreement for salivary tissues (24–27). For lacrimal glands, however, MIRD dose was higher by a factor of 10 than the voxel dose. Because of their small size, which presents challenges for both methods, the actual absorbed dose likely lies somewhere between their respective estimates. Some dosimetry studies suggest that lacrimal glands may be dose-limiting (23,26), whereas in clinical practice significant lacrimal toxicity is rare (29).
In our study, the highest doses occurred in salivary glands, lacrimal glands, and kidneys. Median renal doses were slightly lower than those predicted by others, perhaps reflecting overlying bowel or liver activity. Salivary gland doses are in the lower range of the published series, perhaps relating to overlying activity in bone or partial-volume effects of the voxelized technique. Liver and spleen doses are similar to those reported by Delker et al., who also used SPECT/CT to derive their activity maps (24). Regardless, all the available SPECT data suggest that these organs are not dose-limiting.
Our dosimetry suggests it is safe to deliver multiple cycles of therapy before exceeding the tolerance of salivary glands and kidneys. Assuming average biodistribution after 4 cycles of therapy at an administered activity of 8 GBq, doses to kidneys are 12.5 Gy, lacrimal glands 11.5 Gy, parotid glands 18.6 Gy, and submandibular glands 14.1 Gy. These doses meet accepted standards used in external-beam radiotherapy of 15–18 Gy (40), 34 Gy (41), and 20–25 Gy (salivary tissues) (42). It is well known that normal tissues can tolerate higher absorbed doses following radionuclide therapy than external beam (43) and is explained by the linear-quadratic formula developed following years of use in fractionated external-beam radiotherapy (44). Radiobiologic modeling, for example, suggests that renal tolerance following radionuclide therapy will be almost twice that expected following external beam (15).
Following 4 × 8 GBq, we would predict a marrow dose of 3.5 Gy, a value that exceeds the normally accepted 2 Gy tolerance of marrow (45) and is higher than previous studies of marrow dosimetry that have generally used blood sampling to determine dose (Supplemental Appendix 2). This estimate, however, is subject to several limitations as evidenced by the wide variation in absorbed dose (0.01–3.4 Gy/GBq) between patients. This is explained by the heterogeneity in the metastatic burden in the axial skeleton; although we attempted to define the marrow ROI using noninfiltrated bone, this was almost certainly confounded by measuring tumor rather than marrow dose. In patients with extensive metastases, bone marrow distribution is often expanded in the appendicular skeleton and discordant with tumor location (46). Thus, our marrow estimates are almost certainly overestimates as supported by the low incidence of grade 3/4 acute hematologic toxicity (29).
We found a significant correlation between pretherapeutic 68Ga-PSMA PET and estimated dose to tumor, salivary glands, and bone marrow. In the treatment of neuroendocrine tumor, it is reported that the SUVmax of 68Ga-DOTATOC PET/CT may predict response to radionuclide therapy (47). In our study, we were unable to determine an SUVmean below which patients are unlikely to respond, though there was a trend for a higher SUVmean to be associated with a PSA response at 12 wk (P = 0.056).
In the treatment of neuroendocrine tumors using radiolabeled somatostatin analogs, we have observed that uptake of radionuclide in normal tissues is lower in patients with a high tumor burden because of a tumor-sink effect (48). Recently, Gaertner at el. described reduced uptake of 68Ga-PSMA-11 in salivary glands in patients with high, medium, or low tumor burdens (49). We observed that SUVmax and absorbed dose in salivary glands and kidneys decreased significantly with a greater disease burden and a larger physical size. Such findings may be relevant in predicting salivary gland and renal toxicity (50). These data suggest that it may be optimal to deliver higher administered activities to patients with a larger burden of disease and size and, conversely, to reduce activity in patients with a lower disease burden. In contrast to neuroendocrine tumors treated with radiolabeled somatostatin analogs, however, we found no correlation between absorbed dose and renal function.
An association between predicted dose and either therapeutic response or normal-tissue toxicity would provide powerful supportive evidence for the validity and clinical relevance of the dosimetry methods being used. We have observed that an increasing whole-body tumor-absorbed dose occurs in men with a biochemical response, defined by a PSA decline of at least 50%. This parameter accounts for heterogeneity in tumor dose and is perhaps a more relevant estimate of clinical effect than index-lesion dosimetry, noting that the latter did not correlate with a PSA response (P = 0.09). However, we also acknowledge the considerable overlap in whole-body tumor dose between individual patients who responded to therapy and those who did not (Fig. 4A), and we would not regard routine dosimetry as mandatory in the clinical application of 177Lu-PSMA therapy.
The relationship between absorbed dose and acute toxicity cannot be evaluated comprehensively in this study, as significant treatment-related adverse events were uncommon (29). We observed no episodes of acute renal toxicity, and the mild xerostomia (all Common Terminology Criteria grade 1) reported by most patients on specific questioning tended to recover with time. The lack of higher-grade xerostomia makes it difficult to assess whether this will be dose-limiting. The results of studies using a higher administered radioactivity and a longer-term follow-up may provide insight into dose-limiting toxicities.
CONCLUSION
In a prospective study reporting the outcomes of 177Lu-PSMA-617 therapy in men with advanced prostate cancer, we observed low normal-organ toxicity with repeated cycles of effective therapy. Mean whole-tumor dose correlates with biochemical response and appears superior to conventional index-lesion dosimetry. Whole-tumor parameters correlated with screening 68Ga-PSMA PET findings. Low doses to salivary glands and kidneys are consistent with the lack of clinically apparent grade 3 or higher toxicity (28). We observed a tumor-sink effect, and this observation may provide a rationale for personalized treatment dosing.
DISCLOSURE
Michael Hofman is supported by a clinical fellowship award from the Peter MacCallum Foundation and a Movember clinical trials award from the Prostate Cancer Foundation of Australia. Shahneen Sandhu is supported by a clinical fellowship from the Peter MacCallum Foundation and by the John Mills Young Investigator Award from the Prostate Cancer Foundation of Australia. Rodney Hicks is supported by a practitioner fellowship from the National Health and Medical Research Foundation of Australia. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the nuclear medicine and nursing staff at the Peter MacCallum Cancer Center and all the patients who agreed to participate in the study. 177Lu (no carrier added) was supplied by the Australian Nuclear Science and Technology Organisation (ANSTO; Sydney, Australia). PSMA-617 was supplied by Advanced Biochemical Compounds (ABX; Radeberg, Germany).
Footnotes
Published online Oct. 5, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication August 20, 2018.
- Accepted for publication September 17, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Rethinking Dosimetry: A European Perspective
- Direct Correlation of Tumor Absorbed Dose with Overall Survival in Metastatic Castration-Resistant Prostate Cancer Treated with 177Lu Prostate-Specific Membrane Antigen
- Are FAP Theranostics Really Happening? Will Radiochemistry or Biology Win?
- Preclinical Evaluation of 177Lu-rhPSMA-10.1, a Radiopharmaceutical for Prostate Cancer: Biodistribution and Therapeutic Efficacy
- Computational Nuclear Oncology Toward Precision Radiopharmaceutical Therapies: Current Tools, Techniques, and Uncharted Territories
- An International Study of Factors Affecting Variability of Dosimetry Calculations, Part 4: Impact of Fitting Functions in Estimated Absorbed Doses
- The Role of PSMA PET Parameters as Biomarkers for Response to PSMA-Targeted Radiopharmaceutical Therapy
- Localized In Vivo Prodrug Activation Using Radionuclides
- Best Patient Care Practices for Administering PSMA-Targeted Radiopharmaceutical Therapy
- [177Lu]Lu-Prostate-Specific Membrane Antigen-617 in a Patient with Metastatic Castration-Resistant Prostate Cancer and Status After Bilateral Nephrectomy
- Single Chelator-Minibody Theranostic Agents for 89Zr PET Imaging and 177Lu Radiopharmaceutical Therapy of PSMA-Expressing Prostate Cancer
- First-Strike Rapid Predictive Dosimetry and Dose Response for 177Lu-PSMA Therapy in Metastatic Castration-Resistant Prostate Cancer
- Impact of Posttreatment SPECT/CT on Patient Management During 177Lu-PSMA-617 Radiopharmaceutical Therapy
- Localized in vivo prodrug activation using radionuclides
- Dosimetry of [177Lu]Lu-PSMA-Targeted Radiopharmaceutical Therapies in Patients with Prostate Cancer: A Comparative Systematic Review and Metaanalysis
- Assessing Response to PSMA Radiopharmaceutical Therapies with Single SPECT Imaging at 24 Hours After Injection
- Clinical Management of Advanced Prostate Cancer: Where Does Radiopharmaceutical Therapy Fit in the Treatment Algorithm?
- Real-World Experience with 177Lu-PSMA-617 Radioligand Therapy After Food and Drug Administration Approval
- First Safety and Efficacy Data with the Radiohybrid 177Lu-rhPSMA-10.1 for the Treatment of Metastatic Prostate Cancer
- Rethinking Dosimetry: The Perils of Extrapolated External-Beam Radiotherapy Constraints to Radionuclide Therapy
- Renal and Multiorgan Safety of 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer in the VISION Dosimetry Substudy
- The Hierarchy of SUVs: From Diagnostics to Therapeutics and the Pathway to Effective Theranostics
- An Intrapatient Dosimetry Comparison of 177Lu-rhPSMA-10.1 and 177Lu-PSMA-I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- Antihormonal-Treatment Status Affects 68Ga-PSMA-HBED-CC PET Biodistribution in Patients with Prostate Cancer
- Tandem Isotope Therapy with 225Ac- and 177Lu-PSMA-617 in a Murine Model of Prostate Cancer
- Prediction of Response to 177Lu-PSMA Therapy Based on Tumor-to-Kidney Ratio on Pretherapeutic PSMA PET/CT and Posttherapeutic Tumor-Dose Evaluation in mCRPC
- Lesion Dosimetry for [177Lu]Lu-PSMA-617 Radiopharmaceutical Therapy Combined with Stereotactic Body Radiotherapy in Patients with Oligometastatic Castration-Sensitive Prostate Cancer
- Analysing the tumor transcriptome of prostate cancer to predict efficacy of Lu-PSMA therapy
- Dual-Time-Point Posttherapy 177Lu-PSMA-617 SPECT/CT Describes the Uptake Kinetics of mCRPC Lesions and Prognosticates Patients Outcome
- The Impact of PSMA PET-Based Eligibility Criteria Used in the Prospective Phase II TheraP Trial in Metastatic Castration-Resistant Prostate Cancer Patients Undergoing Prostate-Specific Membrane Antigen-Targeted Radioligand Therapy
- [177Lu]Lu-PSMA-Radioligand Therapy Efficacy Outcomes in Taxane-Naive Versus Taxane-Treated Patients with Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Metaanalysis
- The Impact of PSMA PET-Based Eligibility Criteria Used in the Prospective Phase II TheraP Trial in Metastatic Castration-Resistant Prostate Cancer Patients Undergoing Prostate-Specific Membrane Antigen-Targeted Radioligand Therapy
- [177Lu]Lu-PSMA-Radioligand Therapy Efficacy Outcomes in Taxane-Naive Versus Taxane-Treated Patients with Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Metaanalysis
- Is 18F-FDG PET Needed to Assess 177Lu-PSMA Therapy Eligibility? A VISION-like, Single-Center Analysis
- Toward Single-Time-Point Image-Based Dosimetry of 177Lu-PSMA-617 Therapy
- A Single-Arm, Low-Dose, Prospective Study of 177Lu-EB-PSMA Radioligand Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer
- Evaluation of 177Lu-PSMA-617 SPECT/CT Quantitation as a Response Biomarker Within a Prospective 177Lu-PSMA-617 and NOX66 Combination Trial (LuPIN)
- Evolution of Models of Prostate Cancer: Their Contribution to Current Therapies
- Using 68Ga-PSMA-11 PET/CT for Therapy Response Assessment in Patients with Metastatic Castration-Resistant Prostate Cancer: Application of EAU/EANM Recommendations in Clinical Practice
- Combined Targeted Radiopharmaceutical Therapy and Immune Checkpoint Blockade: From Preclinical Advances to the Clinic
- Synthesis and Preclinical Evaluation of 177Lu-Labeled Radiohybrid PSMA Ligands for Endoradiotherapy of Prostate Cancer
- Dosimetry in Radiopharmaceutical Therapy
- 177Lu-PSMA Therapy
- Antitumor efficacy of 90Y-NM600 targeted radionuclide therapy and PD-1 blockade is limited by regulatory T cells in murine prostate tumors
- Prostate-Specific Membrane Antigen Radioligand Therapy Using 177Lu-PSMA I&T and 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer: Comparison of Safety, Biodistribution, and Dosimetry
- Thoughts on "Tumor Sink Effect in 68Ga-PSMA-11 PET: Myth or Reality?"
- Tumor Sink Effect: Myth or Reality?
- Pretherapeutic Comparative Dosimetry of 177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- 177Lu-PSMA-617 and Idronoxil in Men with End-Stage Metastatic Castration-Resistant Prostate Cancer (LuPIN): Patient Outcomes and Predictors of Treatment Response in a Phase I/II Trial
- Feasibility, Biodistribution, and Preliminary Dosimetry in Peptide-Targeted Radionuclide Therapy of Diverse Adenocarcinomas Using 177Lu-FAP-2286: First-in-Humans Results
- Assessing the Correlation Between 68Ga-PSMA-11 Renal PET Parameters and Renal Function Tests
- PSMA-Hornet: fully-automated, multi-target segmentation of healthy organs in PSMA PET/CT images
- Kidney Doses in 177Lu-Based Radioligand Therapy in Prostate Cancer: Is Dose Estimation Based on Reduced Dosimetry Measurements Feasible?
- Tumor Sink Effect in 68Ga-PSMA-11 PET: Myth or Reality?
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- Bringing VISION to Nuclear Medicine: Accelerating Evidence and Changing Paradigms with Theranostics
- Tumor Response to Radiopharmaceutical Therapies: The Knowns and the Unknowns
- Reimbursement Approaches for Radiopharmaceutical Dosimetry: Current Status and Future Opportunities
- Radionuclide Therapy in Prostate Cancer: From Standalone to Combination PSMA Theranostics
- Normal-Tissue Tolerance to Radiopharmaceutical Therapies, the Knowns and the Unknowns
- PSMA Expression Assessed by PET Imaging Is a Required Biomarker for Selecting Patients for Any PSMA-Targeted Therapy
- RESIST-PC: U.S. Academic Foray into PSMA Theranostic Trials
- Comparative Preclinical Biodistribution, Dosimetry, and Endoradiotherapy in Metastatic Castration-Resistant Prostate Cancer Using 19F/177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T
- Lutetium-177-PSMA-617 in Low-Volume Hormone-Sensitive Metastatic Prostate Cancer: A Prospective Pilot Study
- Deep-Learning Generation of Synthetic Intermediate Projections Improves 177Lu SPECT Images Reconstructed with Sparsely Acquired Projections
- 177Lu-Labeled Albumin-Binder-Conjugated PSMA-Targeting Agents with Extremely High Tumor Uptake and Enhanced Tumor-to-Kidney Absorbed Dose Ratio
- Dissimilar DNA Damage to Blood Lymphocytes After 177Lu-Labeled DOTATOC or Prostate-Specific Membrane Antigen Therapy
- John Violet: radiation oncologist and physician scientist who pioneered targeted radionuclide therapy for prostate cancer
- Neuroendocrine Differentiation and Response to PSMA-Targeted Radioligand Therapy in Advanced Metastatic Castration-Resistant Prostate Cancer: A Single-Center Retrospective Study
- Radiation Dosimetry in 177Lu-PSMA-617 Therapy Using a Single Posttreatment SPECT/CT Scan: A Novel Methodology to Generate Time- and Tissue-Specific Dose Factors
- Investigating PSMA-Targeted Radioligand Therapy Efficacy as a Function of Cellular PSMA Levels and Intratumoral PSMA Heterogeneity
- Mechanistic Insights for Optimizing PSMA Radioligand Therapy
- Long-Term Follow-up and Outcomes of Retreatment in an Expanded 50-Patient Single-Center Phase II Prospective Trial of 177Lu-PSMA-617 Theranostics in Metastatic Castration-Resistant Prostate Cancer
- Response Prediction of 177Lu-PSMA-617 Radioligand Therapy Using Prostate-Specific Antigen, Chromogranin A, and Lactate Dehydrogenase
- Patients Resistant Against PSMA-Targeting {alpha}-Radiation Therapy Often Harbor Mutations in DNA Damage-Repair-Associated Genes
- FAP: The Next Billion Dollar Nuclear Theranostics Target?